
Abstract
Background:
Several lines of evidence suggest that breast cancer (BC) and thyroid cancer (TC) occur together in the same female patients more frequently than would be expected by chance. This study investigated the prevalence and clinicopathological characteristics of second primary BC in TC patients and second primary TC in BC patients.
Methods:
A retrospective case-controlled study was performed in 4243 patients with differentiated TC and 6833 patients with BC. Age-matched control groups without second malignancies were selected.
Results:
Of the 4243 patients with TC, 55 patients developed subsequent BC during a five-year follow-up (range 2–40 years); the standardized incidence ratio (SIR) was 2.45 [confidence interval (CI) 1.83–2.96]. Among the 6833 patients with BC, 81 patients developed subsequent TC during a 6.2-year follow-up (range 2–40 years); the SIR was 2.18 [CI 1.43–2.82]. Subsequent second BC or TC diagnosed within five years of the initial primary malignancy showed more clinical characteristics consistent with early-stage cancer than did control BC or TC patients. Notably, the expression of both the estrogen and progesterone receptors was significantly higher in the tissues of BC patients with coexisting TC compared with those with BC alone.
Conclusions:
The overall risk of second primary TC or BC is increased in patients with prior BC or TC, respectively. The early detection of second cancer might have contributed to these findings. However, BC that coexisted with TC had a higher expression of hormone receptors, suggesting an association between the molecular pathogenesis of TC and BC.
Introduction
T
The increased incidence and excellent prognosis for longevity after both TC and BC have led to concern regarding the development of subsequent primary malignancies (3,10). It is important to identify how much the risk of additional tumors increases after a primary tumor, as well as how differences in the clinical, pathological, and treatment characteristics affect the risk profiles for developing subsequent primary TC or BC.
A retrospective case-controlled study was performed to assess the incidence of, and risk factors for, subsequent primary BC or TC in TC and BC patients, respectively.
Patients and Methods
Study patients
A retrospective case-controlled study was performed at a single tertiary referral center at Seoul National University Hospital. The Institutional Review Board approved the study protocol (numbers H-0912-009-302 and H 1204-077-406). Female patients with the first primary TC (papillary or follicular type) who underwent total thyroidectomy (n = 4234), or the first primary BC who underwent curative surgery (n = 6822) between January 1970 and December 2009 were included. The first cancer is defined as the cancer the patient experienced for the first time in life. Patients with medullary or anaplastic type of TC, those with cancers in organs other than thyroid and breast at the time of enrollment, and those with follow-up of less than two years were excluded. Second primary cancer was defined as that diagnosed at least two years after the first primary cancer; BC after TC (TC1 → BC2 group) and TC after BC (BC1 → TC2 group). Diagnoses made within two years of the first primary tumor were considered to be concomitant disease. Treatment and follow-up strategies for TC and BC were the same as previously described (11,12).
To compare the characteristics of TCs between the primary TC and BC1 → TC2 and TC1 → BC2 groups, 1:3-matched control groups were selected from the TC patients who were not diagnosed with prior or subsequent BC during the follow-up period, that is, TC2 controls for the BC1 → TC2 group, or TC1 controls for the TC1 → BC2 group. Controls, who were matched for both age at diagnosis (± 2 years) and time of surgery (± 2 years), were selected on a case-by-case basis from among the TC cohort: TC1 control (n = 165) and TC2 control (n = 243; Fig. 1). To compare the characteristics of BC between the primary BC and TC1 → BC2 groups or BC1 → TC2 groups, the 1:3-matched control groups were selected using the same criteria as the TC1 and TC2 controls: BC1 controls (n = 165) and BC2 controls (n = 243; Fig. 1).
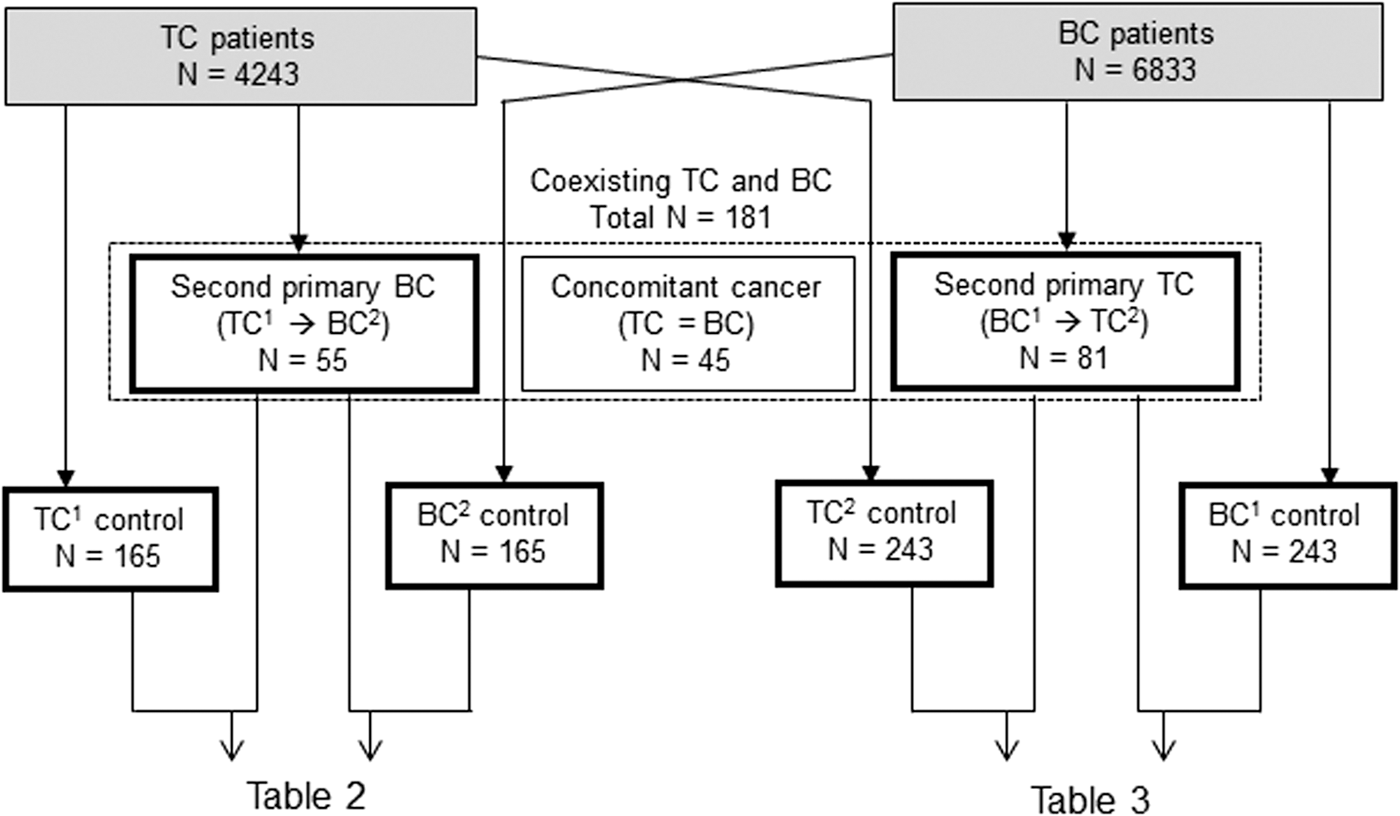
Study design. A retrospective case-controlled study was performed to investigate the incidence and characteristics of second primary breast cancer (BC) or thyroid cancer (TC). Second primary was defined as cancer diagnoses made at least two years after the first primary tumor. Among the total of 4243 TC and 6833 BC patients, 181 were diagnosed with coexisting TC and BC during the 40-year recruitment period. Of those, 55 (30.4%) had first primary TC with subsequent BC (TC1 → BC2 group), 81 patients (44.8%) had first primary BC with subsequent TC (BC1 → TC2 group), and 45 patients (24.9%) had concomitant disease (group TC = BC) within two years of their first diagnosis. Three controls matched by age at diagnosis (± 2 years) and time of surgery (± 2 years), who were not diagnosed with subsequent or previous cancer, were selected per case from each cohort.
Clinicopathological characteristics
Clinical characteristics of TC and BC were obtained, which include age at diagnosis, follow-up duration, family history, recurrence rate, and proportion of subjects who underwent RT for BC or RAI for TC. Pathological characteristics include histological type (papillary or follicular), tumor size, multifocality, extrathyroidal extension, and lymph node (LN) metastasis in TC, and histological type (infiltrative ductal carcinoma [IDC], ductal carcinoma in situ [DCIS], or others), tumor size, and LN metastasis in BC. Immunohistochemistry was performed to assess the expression of the estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) in BC specimens, and was scored as previously described (13).
Statistical analysis
The risk of second primary TC and BC was estimated by compiling the person-years (PY) of observations according to age and calendar year periods from the date of the initial TC or BC diagnosis to the date of diagnosis of the second primary cancer, the date of last follow-up evaluation, or the end of the study (December, 2009), whichever occurred first. The standardized incidence ratio (SIR) was calculated to assess the risk of second primary malignancies by comparing the number of patients with subsequent cancer to the number of cancers that would be expected based on incidence rates for the general Korean population (14). The cancer incidence rates specific for five-year age groups and calendar-year intervals were multiplied by the accumulated PY at risk to estimate the number of expected cancer cases. The observed and expected numbers of second cancers were then combined, and the SIR was expressed as the ratio of observed-to-expected cases.
To compare the clinicopathological characteristics of patients with second primary BC or TC with the control groups, chi square or Fisher's exact tests were used for dichotomous variables, as appropriate. The Mann–Whitney U-test was used to compare continuous variables. A p-value of <0.05 was considered statistically significant. All analyses were performed using SPSS v17.0 (SPSS, Inc., Chicago, IL).
Results
Frequency of co-existing TC and BC
Among the 4243 TC and 6833 BC patients, 181 were diagnosed with co-existing TC and BC over the 40-year recruitment period: 4.3% of the TC and 2.6% of the BC patients. A total of 55 patients (30.4%) had first primary TC followed by subsequent BC (TC1 → BC2 group), 81 (44.8%) had first primary BC and subsequent TC (BC1 → TC2 group), and 45 (24.9%) had concomitant disease within two years of initial diagnosis (group TC = BC; Fig. 1). The clinicopathological characteristics of these three groups of patients are summarized in Table 1.
Data are M ± SD or median (IQR) unless otherwise indicated.
p < 0.05 compared with TC1 → BC2; †p < 0.05 compared with TC = BC.
TC, thyroid cancer; BC, breast cancer; TC1 → BC2, primary TC followed by metachronous second primary BC; TC = BC, synchronous TC and BC; BC1 → TC2, primary BC followed by metachronous second primary TC; IDC, infiltrative ductal carcinoma; DCIS, ductal carcinoma in situ; ER, estrogen receptor; PR, progesterone receptor; PTC, papillary thyroid carcinoma; FTC, follicular thyroid carcinoma.
IDC was relatively infrequent, but DCIS was common in the TC1 → BC2 group compared with the TC = BC and BC1 →TC2 groups (p < 0.05). It is noteworthy that tumor size in BC was relatively small compared with TC tumors. The characteristics of BC or TC in the TC = BC group, in which the majority of TC cases were identified incidentally during BC diagnosis, were similar to those in the BC1 → TC2 group, although the ER-positive rate for BC was lower in the BC1 →TC2 group. The detection routes of subsequent cancer after first cancer are shown in Supplementary Figure S1 (Supplementary Data are available online at
Development of second primary BC in TC patients (TC1 → BC2)
The estimated incidence of BC was 148.7 per 100,000 PY, and the SIR was 2.45 [confidence interval (CI) 1.83–2.96] (14). The SIR was 2.16 [CI 1.67–2.65] after excluding incidentally detected cases (4/55) by imaging modalities performed during medical follow-up of TC. The mean latency from diagnosis with TC to the development of BC was 5.2 (3.1–11.0) years. The incidence of second primary BC was significantly higher, especially within the first five years of TC diagnosis, and then decreased rapidly according to the latency period (p < 0.01; Fig. 2A).
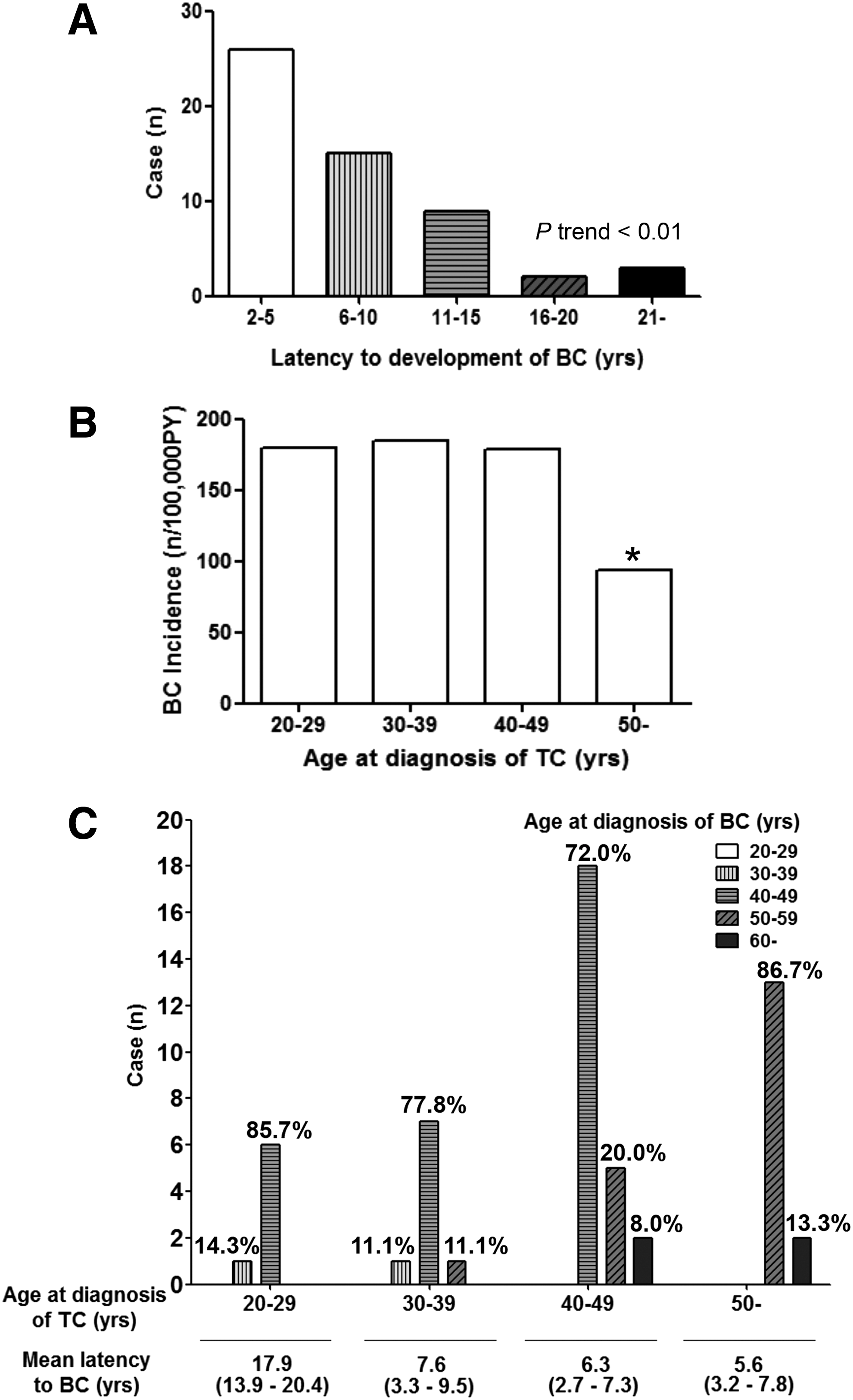
Association between age at diagnosis with TC and the latency to developing second primary BC.
When the data were analyzed according to the age at diagnosis with TC, the incidence of BC was similar in patients aged 20–50 years old. However, the incidence declined significantly after 50 years of age (p < 0.01; Fig. 2B). In patients who experience TC at a younger age (i.e., in their 20s or 30s), the mean latency to the development of BC was longer, so that the average age of TC development was the 40s and 50s, which is similar to the general population (Fig. 2C and Fig. 3). Only 2/55 (3.6%) patients were diagnosed with second primary BC before the 40 years of age.
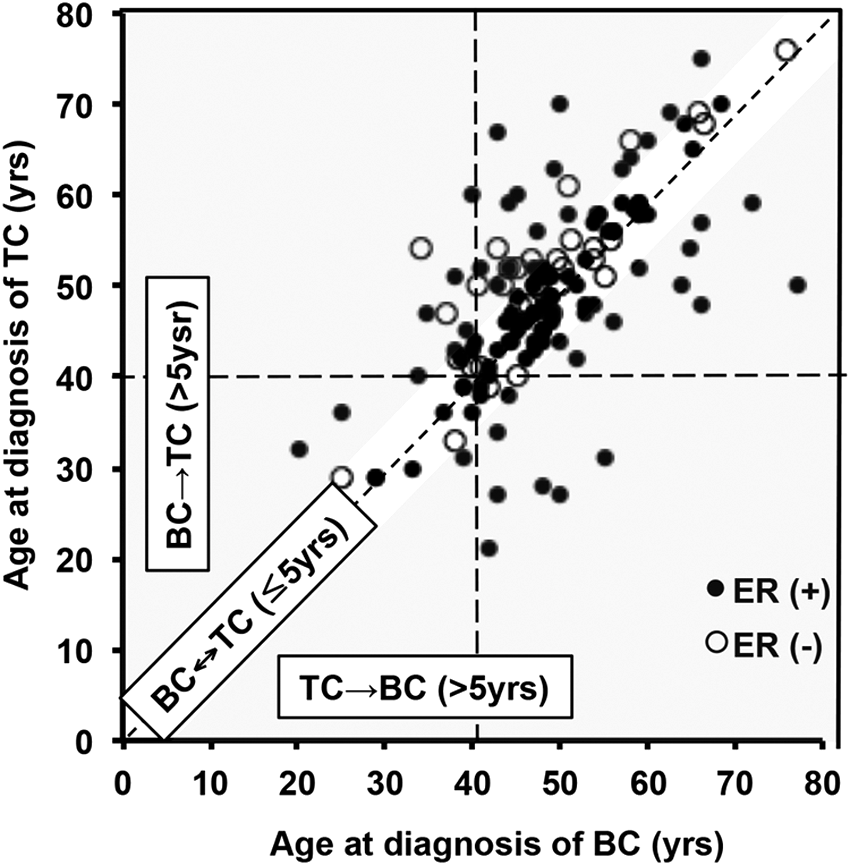
Association between the age at diagnosis of BC and TC within the same patients in accordance with ER positivity. All patients with coexisting TC and BC were included in the graph in accordance with their ER status. Gray zones denote patients diagnosed with second primary malignancy within five years of the first primary malignancy. White zones denote a BC↔TC of ≤5 years, including the BC1 → TC2-within-five-years, TC1 → BC2-within-five-years, and TC = BC groups. Closed circles denote ER (+) patients; open circles denote ER (−) patients.
Clinicopathological characteristics of BC in TC1 → BC2 patients
The clinicopathological characteristics of BC were compared between the 55 patients in the TC1 → BC2 group and the 165 matched controls in the BC2 control group (Table 2). The respective mean age at diagnosis of BC, median duration of follow-up after diagnosis with BC, and family history of BC were similar between the two groups. In the TC1 → BC2 group, the percentage of DCIS was significantly higher (29.1% vs. 8.5%, p < 0.05), and tumor size was smaller (1.7 ± 0.9 cm vs. 2.5 ± 1.6 cm, p < 0.05). The prevalence of LN metastasis (23.%s. 38.8%, p = 0.12) and BC recurrence (7.3% vs. 11.2%, p = 0.18) was lower compared with the BC2 control group, but not significantly. The expression of both the ER and PR was significantly higher in the tumors from individuals in the TC1 → BC2 group compared with those from the BC2 control group (ER 89.1% vs. 66.1%; PR 67.2% vs. 54.0%; p < 0.05).
Data shown are M ± SD or median (IQR) unless indicated otherwise.
p1 for the comparison between group TC1 → BC2 All and BC2 control; p2 for the comparison between BC2 within five years and after five years. * p < 0.05 compared to BC2 control.
p3 for the comparison between group TC1 → BC2 All and TC1 control; p4 for the comparison between BC2 within five years and after five years.
RAI, radioactive iodine.
As shown in Supplementary Figure S1, the detection rate of BC2 in the process of medical check-up and health screening was relatively higher within five years after the diagnosis of TC1. While this rate is not as high after five years, the patients were divided according to the latency to detection after TC1. Patients who were diagnosed with BC2 within five years of TC1 (n = 26) had significantly smaller-sized tumors than both those diagnosed with BC2 more than five years after TC1 diagnosis (n = 29; 1.5 ± 0.8 cm vs. 2.6 ± 1.7 cm, p < 0.05) and the BC2 control group (1.5 ± 0.8 cm vs. 2.5 ± 1.6 cm, p < 0.05). There were no significant differences in tumor size between the BC2 five years after TC and the BC2 control groups. The prevalence of LN and distant metastasis and the recurrence rate were lower, but not significantly, in the BC2 within and after five years of TC groups. The expression of ER and PR were not different between the BC2 within and after five years of TC groups (ER 84.6% vs. 93.7%, p = 0.67; PR 65.3% vs. 68.5%, p = 0.92, respectively), but were significantly higher in both subgroups compared with the BC2 control group (ER 66.3%, p < 0.05; PR 54.0%, p < 0.05). Figure 3 also illustrates that BC at five years post-TC exhibited very high ER positivity, regardless of age at the time of the BC diagnosis. The odds ratio of ER positivity for the diagnosis of previous TC in second primary BC (TC1 → BC2) was 4.20 ([CI 1.69–8.39]; p < 0.05), 2.83 ([CI 1.03–7.65]; p < 0.05), and 6.94 ([CI 1.68–14.8]; p < 0.05) for BC2 within and after five years, respectively.
Clinicopathological characteristics of TC in TC1 → BC2 patients
To evaluate factors that can facilitate risk prediction of second BC in TC patients, the clinicopathological characteristics of TC in the TC1 → BC2 group were compared with the TC1 control group (Table 2). The mean age at diagnosis of TC and median duration of follow-up after TC diagnosis were matched as described. There were no differences in family history of TC, histological type, tumor size, LN and distant metastasis, multifocality, extrathyroidal extension, tumor recurrence, and RAI therapy, regardless of the latency to detection of BC.
Development of second primary TC in BC patients (BC1 → TC2)
The estimated incidence of TC was 152.6 per 100,000 PY, and the SIR was 2.18 [CI 1.83–2.96] (14). The SIR was 1.73 [CI 1.25–2.16] after excluding incidentally detected cases (13/81) by imaging modalities performed during medical follow-up of BC. The mean latency from BC to the development of TC was 5.9 years (range 3.4–12.7 years). The incidence of second primary TC was significantly higher within the first five years of BC diagnosis, and then decreased over time (p < 0.01; Fig. 4A). The incidence of TC was similar in patients who were diagnosed when aged 20–50 years, but then declined significantly in patients aged >50 years (p < 0.05; Fig. 4B). In patients who experience BC at a younger age (i.e., in their 20s or 30s), the mean latency to the development of TC was longer, so that the average age of TC development was in the 40s and 50s, which is similar to the general population (Fig. 3 and Fig. 4C). Only 4/81 (4.9%) patients were diagnosed with second primary TC before 40 years of age.
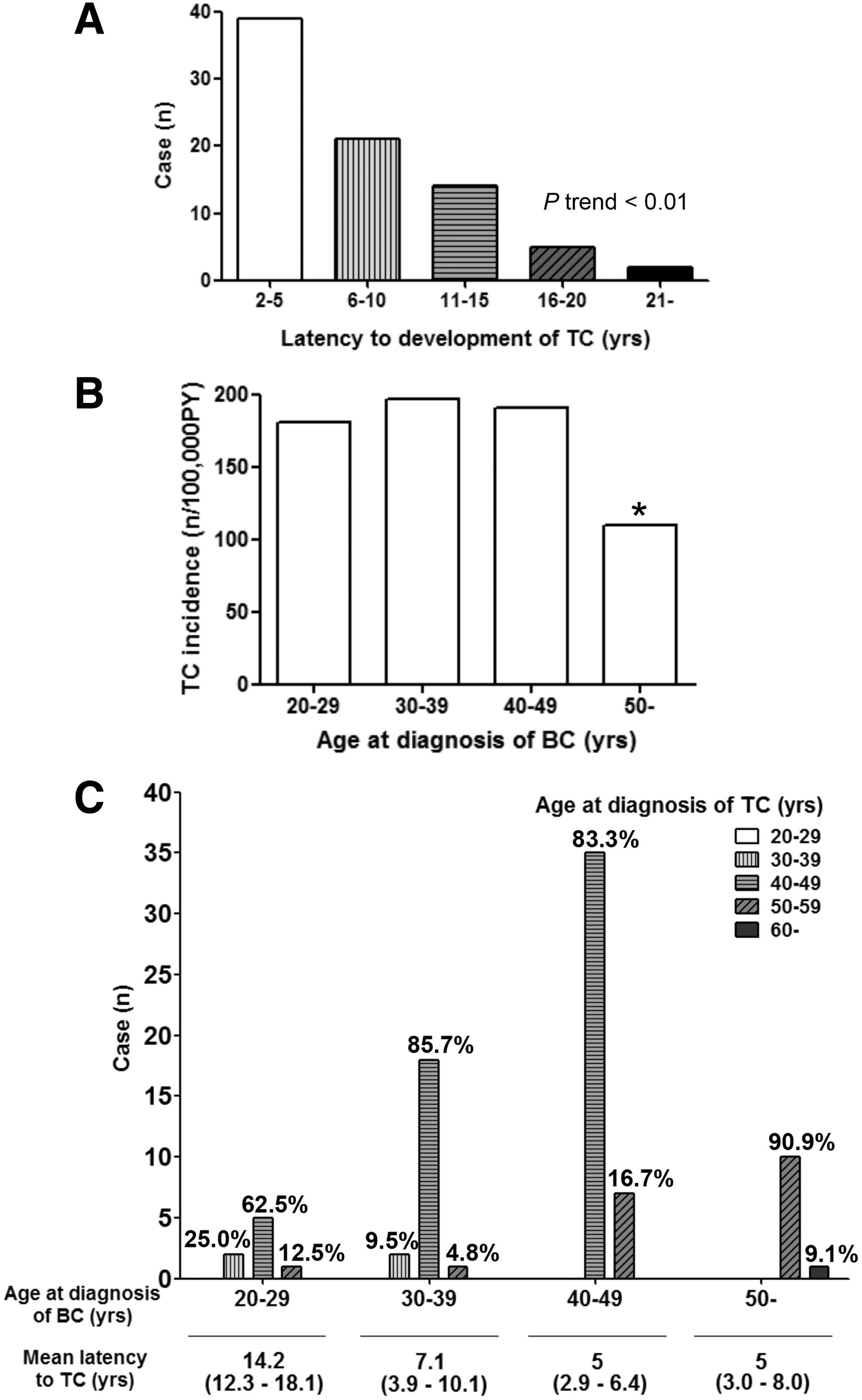
Association between age at diagnosis with BC and the latency to developing second primary TC.
Clinicopathological characteristics of TC in BC1 → TC2 patients
When the clinicopathological characteristics of TC were compared between the BC1 → TC2 group (n = 81) and the TC2 control group (n = 243; Table 3), the mean age at diagnosis with TC and the median duration of follow-up after TC were comparable. Other TC characteristics such as histological type (PTC 92.8% vs. 91.1%), tumor size (1.7 ± 0.9 cm vs. 2.0 ± 1.1 cm), LN (30.9% vs. 33.3%) and distant metastasis (2.5% vs. 3.3%), multifocality (34.6% vs. 37.9%), extrathyroidal extension (24.7% vs. 28.0%), and recurrence rate (4.9% vs. 6.2%) were also comparable between groups (p > 0.05). Similar to the TC1 → BC2 group, the detection rate of TC2 in the process of a medical check-up and health screening was relatively higher within five years after the diagnosis of BC1 (Supplementary Fig. S1). TC2 tumors diagnosed within five years after BC (n = 39) were smaller in size (1.5 ± 0.8 cm vs. 2.0 ± 1.11 cm, p < 0.05), but the prevalence of LN and distant metastasis, multifocality, extrathyroidal extension, and recurrence rate were comparable with the TC2 group after five years (n = 42).
Data shown are M ± SD or median (IQR) unless otherwise indicated.
p1 for the comparison between group BC1 → TC2 All and TC2 control; p2 for the comparison between TC2 within five years and after five years. * p < 0.05 compared with TC2 control.
p3 for the comparison between group BC1 → TC2 All and BC1 control; p4 for the comparison between BC2 within five years and after five years.
Clinicopathological characteristics of BC in BC1 → TC2 patients
To evaluate the factors that can facilitate risk prediction of second TC in BC patients, the clinicopathological characteristics of BC in the BC1 → TC2 group were compared with the BC1 control group (Table 3). The age at diagnosis, family history, pathological characteristics of BC, including histological type, tumor size, LN and distant metastasis, and recurrence rate were comparable between the two groups. The proportion of the patients who received RT for BC in the BC1 → TC2 and BC1 control groups was not different. There was also no significant difference in the characteristics of BC in patients who developed TC within (n = 39) and after (n = 42) five years of BC diagnosis. Notably, the expression of both ER and PR were significantly higher in the BC1 →TC2 group than the BC1 control group (ER 67.9% vs. 55.2%; PR 59.3% vs. 46.1%; p < 0.05). These results were similar, regardless of the latency to the development of second primary TC and the age at the time of BC diagnosis (Table 3 and Fig. 3). The odds ratios of ER positivity for the development of TC2 in BC1 patients was 1.72 ([CI 1.01–2.93]; p < 0.05), 1.74 ([CI 1.01–3.11]; p < 0.05), and 1.82 ([CI 1.02–3.15]; p < 0.05) for TC2 within and after five years, respectively.
Discussion
This study revealed that patients with TC or BC have a higher risk of developing second primary BC or TC, respectively. In this study, 4.3% of the TC and 2.6% of the BC patients were diagnosed with second primary or concomitant BC and TC, respectively. The expression of ER and PR was significantly higher in BC patients with co-existing TC compared with those without, suggesting the possibility that ER or PR signaling might represent common etiological factors in the development of TC and BC.
In patients with TC, the incidence of BC development was increased compared with the general population: the SIR for developing second primary BC was 2.45. These SIR values are high compared with previous studies, in which values ranged between 1.2 and 1.6 (2,3,15). The increased incidence of BC following TC might be attributable to the incidental detection of BC during follow-up of TC or to frequent health check-ups following TC, especially in the cases detected within five years (Supplementary Fig. S1), potentially resulting in high SIR values. To address this issue, SIR was calculated after excluding incidentally detected cases by imaging modalities performed during medical follow-up of TC. This reduced the SIR to 2.16, but it remained significantly high, even after excluding the incidentally identified cases. However, excluding these cases in the analysis should produce another bias because the possibility cannot be eliminated that these cases were detected by medical services other than the active follow-up of TC. Recent report regarding metachronous primary cancer after treatment of TC based on a nationwide registry in Korea showed that the SIR of second primary BC after TC (n = 178,844) is 1.20 [CI 1.11–1.30], which is much lower than that in the present study (16). However, it cannot be compared directly with the current result, since the nationwide study included all subtypes of TC, including anaplastic and medullary carcinomas, both of which are associated with a shorter life expectancy, and therefore the subjects are expected to have a lower chance of developing a second cancer. Another point is related to different patient characteristics. The latency between second primary BC after TC was longer in the present study compared with the nationwide registry-based study, in which the authors demonstrated that the SIR becomes significantly higher as the latency becomes longer. These differences in study design and population may have contributed to producing different SIRs in these two studies.
Patients in the BC2-within-five-years group were characterized by smaller tumor sizes, a higher proportion of DCIS, and a lower recurrence rate compared with the BC2-after-five-years group. It is speculated that this difference simply results from earlier diagnosis during the disease process rather than from the presence of tumors with different biological characteristics. Early detection of BC might have resulted in higher ER- and PR-positive rates compared with the BC control group. However, rates were also significantly higher in the BC2-after-five-years group, which exhibited other similar tumor characteristics to the BC control group, regardless of age at the time of BC diagnosis. These results imply that ER/PR signaling might contribute to high SIR values, in addition to the effects of early detection.
A tendency for favorable histopathological findings and prognosis of BC in TC1 → BC2 patients with a latency period within five years suggests that close monitoring for the detection of BC development might be beneficial in patients with TC. However, the peak age of BC development was between 40 and 50 years of age, irrespective of the age at the time of TC diagnosis. Indeed, patients who suffered from TC in their 20s and 30s exhibited longer latencies compared with those aged >40 years. The diagnosis of BC in these patients predominantly occurred in their 40s and 50s, which is similar to the general population; a very small proportion developed BC before the age of 40 years. Therefore, early screening tests for BC in younger TC patients would not be recommended, although regular mammography is advised for BC screening in women >40 or 50 years of age, according to several guidelines (17 –19).
Patients with BC also had a higher risk of developing TC; the SIR for developing second primary BC was 2.18. These SIR values are comparable with those of previous studies, in which values ranged between 1.7 and 3.7 (4,5,20,21). A recent report from Korea showed that the relative risk of second primary TC after BC (n = 2657) is 1.95 [CI 1.37–2.79], which is not significantly different from the present results (22). However, it is more difficult to demonstrate an association between BC and the subsequent development of TC. In addition to the effects of more active surveillance of other malignancies following the detection of BC, the incidental detection of TC during positron emission tomography or chest computed tomography during BC follow-up was reported frequently (Supplementary Fig. S1), and might have contributed to the increased rate of TC diagnosis. The SIR of BC in TC patients becomes 1.73 after excluding incidentally detected cases (7/45) by imaging modalities performed during follow-up of BC, although these SIR values should also be affected by bias as previously discussed for SIR of second primary BC in TC patients.
Except for the size of tumors diagnosed within five years, all of the histopathological findings pertaining to TC in BC1 → TC2 patients were similar to those in TC2 control patients without previous BC, suggesting no clinical predictors for TC development. Because there was no evidence of an improved prognosis for TC diagnosed early, and given that the peak age at TC diagnosis was similar to that of the general population, screening for TC in BC patients cannot be recommended, irrespective of the patient's age at BC diagnosis.
Several previous studies also suggest an association between TC and BC. However, most of these focused on epidemiological trends (3,15,23,24). The present study found that ER and PR expression increased significantly in a series of BC patients who also had TC, suggesting a role for ER/PR in this association. These findings were consistent, regardless of the sequence of TC or BC, the latent period to the development of the second malignancy, or the age at BC diagnosis. This suggests that a common molecular mechanism might play a role in the development of concurrent TC and BC, rather than an incidental association, including detection bias.
In accordance with the present observation, previous studies have also suggested a role for hormone receptors in the molecular pathogenesis of TC. Sex steroid receptors are present in human thyroid tissue and several TC cell lines, and ER levels are significantly higher in TC compared with normal thyroid tissue (25,26). Moreover, estrogen has direct pathophysiological effects on thyroid tissue via the ER (1,3,27). Other studies have shown that estrogen upregulates the expression of cell cycle-related genes and proto-oncogenes in thyroid cells, which might influence the pathogenesis of TC (6,7).
Alternatively, it could be that specific treatment for each cancer may be associated with the development of the second cancer, that is, RT after BC as a risk for subsequent TC, or RAI therapy in TC as a risk for the development of BC. However, this possibility could not be excluded because the proportion of patients who received RAI was not different between TC1 → BC2 and TC1 control groups, as was the proportion patients who received RT between BC1 → TC2 and BC1 control groups. The lack of effects of RAI on BC development have already been reported (28). It has been also reported that thyrotropin (29,30) or common environmental risk factors including exposure to ionizing radiation (9,31) may contribute to the co-occurrence of BC and TC. Further studies are needed to evaluate the etiological role of these factors in linking TC and BC, and to support the epidemiological data by understanding the pathogenic mechanisms.
In conclusion, this study has identified that the overall risk of second primary TC or BC is increased in patients with BC or TC, respectively. Although the increased incidence appears to be principally due to increased detection rates, the greater expression of ER and PR in BC in patients with co-existing TC suggests that a specific molecular pathogenesis might underlie this association. Regular breast examination, as recommended by several guidelines (17 –19) for the general population, should be emphasized in TC patients. However, for BC patients, no recommendations concerning TC screening can be proposed based upon the present results.
Footnotes
Acknowledgments
This work was supported by the SK Telecom Research Fund (grant number 2013-0545).
Author Disclosure Statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.