
Abstract
Background:
Most benign thyroid nodules found on fine-needle aspiration cytology (FNAC) can be followed with periodic ultrasonography. During follow-up, when nodules grow, re-aspiration or surgical resection for a histologic diagnosis is recommended. However, there is little evidence regarding the malignancy risk associated with nodule growth.
Method:
We retrospectively reviewed the records of 542 patients with FNAC-diagnosed adenomatous nodules (ANs) who underwent surgery in 2011–2012 at Kuma Hospital. Among them, 196 patients had surgical resection because of nodule volume growth (median, 1.94 times; range, 1.21–27.60) during the observation period (mean, 45.9 months). Excluding nodule growth, the remaining 346 patients underwent surgery for various reasons including the large size of nodules or the appearance of undefined ultrasound features suspicious for malignancy during follow-up. For comparison, we reviewed 409 patients with FNAC-diagnosed follicular neoplasms (FNs) operated on in 2011–2013. Most (n=327) underwent surgery shortly after the FNAC diagnosis, while 82 patients were observed for a period of time and had a late operation due to nodule volume growth (median, 2.70 times; range, 1.27–15.82).
Results:
The histologic diagnoses of the 196 growing FNAC-diagnosed ANs were 158 ANs, 32 follicular adenomas (FAs), 4 follicular tumors of uncertain malignant potential (FT-UMP; 2%), and 2 malignancies (1%). The 346 patients who underwent surgery for reasons other than nodular growth had 16 FT-UMP (4.6%) and 16 malignancies (4.6%). This suggests that nodule growth itself is not a risk factor for malignancy. On the other hand, there were 23 FT-UMP (28%) and 15 malignancies (18.3%) in the 82 growing FNAC-diagnosed FNs, while 44 FT-UMP (13.5%) and 54 malignancies (16.5%) in the 327 FNAC-diagnosed FN patients who underwent immediate surgery. The malignant potential was significantly higher in the growing-FN group than the immediate-surgery FN group (p<0.05). No significant difference was found in the volume change between the benign and the FT-UMP plus malignant group in the growing FNs, suggesting that a growth rate does not correlate with malignant potential.
Conclusion:
This is the first demonstration that the malignancy risk is low in FNAC-diagnosed ANs, even if the nodules grow significantly, whereas FNs have a higher risk when they grow.
Introduction
T
Adenomatous nodules (ANs) are the most common benign nodules. They are a form of benign hyperplasia but it is known that some ANs grow gradually. Because of this, it is essential to establish whether benign nodule growth is a risk factor for malignancy or not. In the present study, we addressed this issue by reviewing the records of 196 patients with FNAC-diagnosed ANs who had surgery because of increasing nodule volume.
Conversely, when a nodule is diagnosed as follicular neoplasm (FN) on FNAC, a diagnostic lobectomy is recommended (5 –8), because this category includes follicular adenoma (FA) and follicular cancer (FC), both of which are difficult to distinguish by preoperative examinations. Although most patients with FNs undergo surgical resection, some patients were observed without having immediate surgery at our institution, as described later. We also reviewed 82 patients with FNAC-diagnosed FNs who underwent late surgery because of nodule growth.
Materials and Methods
Patient series
All patients with thyroid nodule(s) referred to Kuma Hospital for their evaluation undergo a US examination. We classified thyroid nodules into classes 1 to 5 according to our US classification system (9). Briefly, class 1, round or oval anechoic lesion; class 2, regular-shaped nodule with cystic change (the echo level of solid lesion is similar to that of normal thyroid); class 3, solid and regular-shaped nodule (internal echo is homogeneous or may have strong echoes internally or at the capsule); class 4, solid and irregular-shaped nodule (internal echo is usually low and may have fine strong echoes internally); class 5, solid and irregular-shaped nodule with extrathyroid extension. Intermediate classes between class 2 and 3 (designated as class 2.5) and class 3 and 4 (designated as class 3.5) were also used. Nodules judged to be class 2.5 or lower were categorized as benign (typically cyst and AN are contained). Nodules with class 3 were categorized as borderline (FA, minimally invasive FC and sometimes AN). Nodules classified as 3.5 or higher were categorized as suspicious for malignancy or diagnosed as malignant. This US classification can evaluate nodules with high accuracy, as previously described (9 –11). Except for small nodules in US class 1 or 2, we conducted a US-guided FNA biopsy for thyroid nodules. We evaluated each nodule for management based on US findings and FNAC results in addition to clinical factors. When a patient had more than one nodule, we used the nodule with the highest US class and FNAC results to decide the management strategy. Most benign nodules were observed with periodic US monitoring once per year, whereas the management of FNAC-diagnosed FNs was not necessarily uniform.
We recommended immediate surgery for patients with FNs when they had at least one of the following clinicopathologic features: (1) US features suspicious for malignancy, (2) a tumor showing solid content measuring >4 cm in diameter, (3) serum thyroglobulin >1000 ng/mL, (4) a tumor compressing the trachea or esophagus, (5) a tumor expanding into the mediastinum, (6) autonomously functioning thyroid nodules, (7) a tumor presenting a cosmetic problem, and (8) the patient's desire to have it removed (10,11). Although most patients with FNs underwent surgical resection, some patients without any of these features were observed with careful US monitoring, if they desired.
We retrospectively reviewed the records of 542 patients with ANs categorized as benign based on FNAC who underwent surgery between January 2011 and December 2012 at Kuma Hospital. Every nodule resected in these 542 patients was larger than 10 mm in diameter and none had US features suspicious for malignancy (US class <3). Approximately half of the patients had a single nodule and the remaining half had more than one nodule >5 mm in diameter (the number of patients with single nodule versus multiple nodules: 270 versus 272). Among them, 196 patients had lobectomy because of nodule volume growth during the observation period. Thirty-five of these patients had been monitored by other hospitals and referred to Kuma Hospital for surgery. For every patient referral, US and FNA biopsy were re-performed and the US classification and FNA diagnosis were established independently at our hospital. The mean observation period in patients followed up at Kuma Hospital was 45.9 months. The remaining 346 patients underwent surgery for various reasons including the large size of the nodules, the appearance of some undefined US features suspicious for malignancy during the observation periods, or the patient's desire to have a nodule removed.
For comparison, we also studied the records of 409 patients with FNAC-diagnosed FNs (including suspicious for FNs) operated on between January 2011 and December 2013 (single nodule versus multiple nodules: 238 versus 171). Most of these patients (n=327) underwent surgery shortly after the FNAC diagnosis, while 82 patients were observed for some time and thereafter had a late operation due to nodule growth.
Lobectomy was performed for almost all cases, either AN or FN. Total thyroidectomy was done for a few cases of a very large nodule compressing the trachea, multiple large nodules in both lobes, or nodules with some undefined but undeniable US findings of suspicious for malignancy.
We analyzed all of the patients' final histologic diagnoses and nodule growth rates. Incidental occult papillary microcarcinomas (found in 6 patients during surgery) were excluded from the analysis. In the analysis regarding nodule growth rates between the benign group and the malignant plus FT-UMP (follicular tumor of uncertain malignant potential) group in the growing FNs, we excluded 18 patients who had been followed up at other hospitals before surgery because no accurate data regarding the size of the nodules were available.
Measurement of nodule growth rate
A high-resolution US examination was performed for each patient by well-trained ultrasonographers using a Toshiba Aplio SSA-770A ultrasound system (Toshiba American Medical Systems, Tustin, CA) with PLT-1204AX (7–14 MHz) and PLT-805AT (5–12 MHz) linear probes. Every targeted nodule for resection was larger than 10 mm in diameter and the volume of each nodule was calculated according to the ellipsoid formula (length [cm]×width [cm]×depth [cm]×3.14/6). The nodule growth is expressed as the number of times the baseline volume (initial examination) or the percent ratio of the final volume (right before the operation)/the baseline volume. Because the follow-up period varied between individuals, the growth rate is also shown per year of the observation period.
Interobserver variation
Because 13 different ultrasonographers evaluated nodular volume at our institution, we also investigated interobserver variation in a prospective study of 50 patients (8 males, 53.1±12.6 years old, 42 females, 52.7±13.3 years old). The volume of each nodule of each patient was measured by 3 different ultrasonographers successively in the same day. The 3 examiners were selected at random from the 13 ultrasonographers and each examiner was randomly assigned to group A, B, or C (each group finally consisted of unfixed 50 examiners). The data for the 50 nodules (10.4±11.4 g, mean±standard deviation [SD]) obtained by the 3 unfixed examiners were statistically analyzed. The intraclass correlation coefficient was 0.983 (95% confidence interval [CI]: 0.973–0.990, p<0.001). This result indicates that the interobserver variation among the 13 ultrasonographers at Kuma Hospital can be considered almost negligible. The coefficient of variance (CV) in each nodule was 9.6% and that for the 3 ultrasonographers (the CV of groups A, B, and C) was 20.0%. We decided that a >20% change in the nodule volume is significant as the consensus of Kuma Hospital.
Thyroid cytology
The original reporting system of thyroid cytology at our institution was based on the recently published Japan Thyroid Association (JTA) Reporting System (12) that modified the Papanicolaou Society's 1996 recommendation (13). After patients with nonmalignant nodules who underwent surgery between January 2011 and December 2013 were extracted, the FNAC samples of nodules of the patients to be analyzed in this study were re-evaluated using the Bethesda System for Reporting Thyroid Cytopathology (7,8). Descriptive comments and explanatory notes to subclassify the interpretation are provided in each case. For example, when AN is considered in the benign category, the supporting findings are described in the FNAC report. The FNAC morphologic criteria of AN at Kuma Hospital were principally based on those of nodular goiter described in the Bethesda System for Reporting Thyroid Cytopathology (7); AN is characterized by abundant watery colloid; small, round to oval follicular cells with dark nuclei, arranged in monolayer sheets or groups with follicle formation; and macrophages usually filled with hemosiderin granules. The group of FNs contained nodules diagnosed as also suspicious for FNs.
Statistical analysis
Categorical variables were compared by the χ2 test, and continuous variables were compared by the unpaired t-test. We calculated the intraclass correlation coefficient with SPSS version 20.0 (SPSS, Chicago, IL). Statistical significance was defined as p<0.05.
Results
Nodules of FNAC-diagnosed adenomatous nodule
One hundred ninety-six patients who had an FNAC-based diagnosis of AN underwent lobectomy because of an increase in nodule volume (median, 1.94 times; range, 1.21–27.60 times for the patients followed up at Kuma Hospital) after a period of observation (45.9±22.8 months). The final histologic diagnoses of these nodules evaluated as AN on FNAC are shown in Table 1A. There was 1 papillary cancer (PC), 1 FC, and 4 FT-UMP. The FNAC specimen of both PC and FC contained colloid but no or very few follicular epithelial cells, which might have been unsatisfactory for correct FNAC diagnosis. FT-UMP is a borderline lesion between benign and malignant nodules but it can be considered as a candidate for surgery. Therefore, in the 196 preoperative FNAC-diagnosed ANs that were resected because of increased nodule volume, there were only 2 cancers (1%) and only 6 nodules (3%) belonged to the category of candidates for surgery (Fig. 1A).
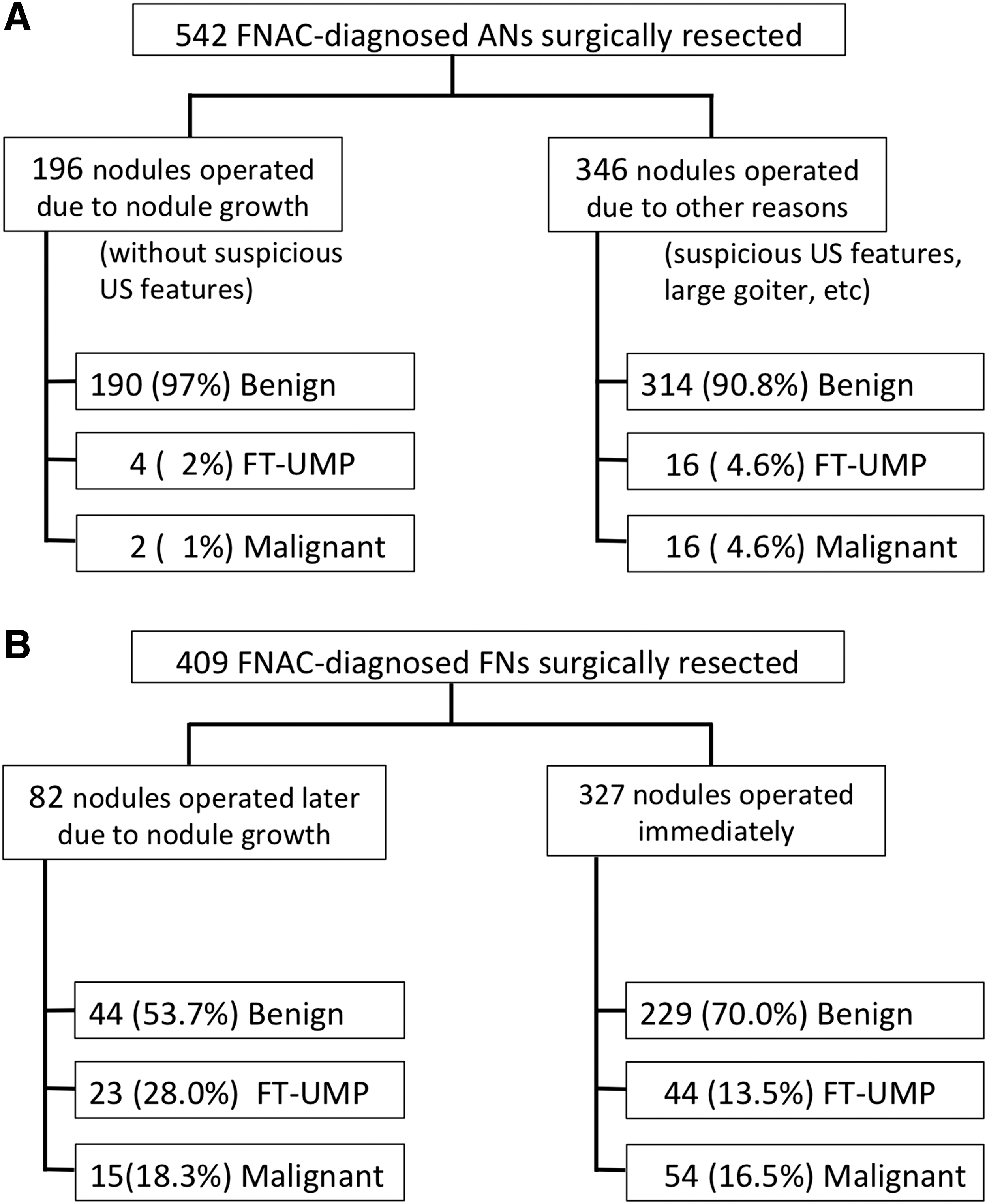
Flowchart representing breakdown of nodules according to the reasons for surgery (nodule growth or other reasons) and histologic diagnoses in the surgical specimen.
For the 346 patients who underwent surgery for various reasons other than nodular growth, the histologic diagnoses revealed 16 FT-UMP (4.6%) and 16 malignancies (4.6%; Table 1B, Fig. 1A). Because the reasons for surgery included some undefined US features suspicious for malignancy or the large size of the nodule, it is not surprising that this group showed a higher ratio of malignancy than the growing nodule group (16/346 [4.6%] versus 2/196 [1%], p<0.05).
The reasons for surgery were: appearance of suspicious US features for malignancy during observation, the large size of tumor compressing the trachea or esophagus, cosmetic problems with patient's desire to have it removed.
Malignant lymphoma.
AN, adenomatous nodule; FA, follicular adenoma; FT-UMP, follicular tumor of uncertain malignant potential; PC, papillary cancer; FC, follicular cancer.
Nodules of FNAC-diagnosed follicular neoplasm
There were 409 FNs determined by FNAC. Most (80%) were resected shortly after FNAC diagnosis, but 82 patients were observed for some time (mean, 49.6 months) and had a late operation after nodule volume growth (median, 2.70 times; range, 1.27–15.82). Table 2 shows their histologic diagnoses. For the 82 FNAC-diagnosed FNs operated on because of increased nodule volume during the observation period (the growing-FN group), the malignancies (14 FCs plus 1 PC) and FT-UMP accounted for 18.3% and 28%, respectively (Table 2A, Fig. 1B). In contrast, in the immediate-surgery FN group resected soon after FNAC (n=327), 16.5% were malignant and 13.5% were FT-UMP (Table 2B, Fig. 1B). The frequency of benign, FT-UMP, or malignancy was significantly different between the growing-FN group and the immediate-surgery FN group (p<0.05), suggesting a higher malignancy risk in the former compared with the latter group.
The reasons for surgery were: suspicious US features for malignancy, tumor showing solid content >4 cm in diameter, serum thyroglobulin >1000 ng/mL, tumor compressing the trachea or esophagus, tumor expanding into the mediastinum, autonomously functioning thyroid nodules, and tumor presenting cosmetic problems with patient's desire to have it removed.
Hashimoto's thyroiditis.
Metastatic cancer from renal cell carcinoma.
AN, adenomatous nodule; FA, follicular adenoma; FT-UMP, follicular tumor of uncertain malignant potential; PC, papillary cancer; FC, follicular cancer; PDC, poorly differentiated cancer; US, ultrasonography.
Sixty-four of 82 patients with growing FNs had been followed up at Kuma Hospital. Among them, 37 were proven to be benign (AN plus FA) and 27 were malignant plus FT-UMP. No significant difference was found in the initial nodule volume, the final nodule volume or the growth rate—whether we used the absolute percent ratio (final nodule volume/initial nodule volume) or the ratio per year of observation periods—between the benign group and the FT-UMP plus malignant group (Table 3).
Eighteen patients with follicular tumors (FT) who had been followed up at other hospitals before surgery were excluded because accurate nodule size data were not available.
Discussion
The aim of this study was to clarify whether surgical resection should be considered when benign nodules are growing. Several factors have been proposed as surgical indications for benign nodules, including the presence of local pressure symptoms associated with the nodules, external irradiation in childhood, cosmetic issues, and US features suggesting malignancy (4). Nodule size is controversial; some studies suggest that large nodules have a higher risk of malignancy (14 –17), while others do not support this (18 –20). Nodule growth is another important issue to be considered. When nodules become enlarged, the guidelines recommend re-aspiration or even surgical resection (5 –8). However, it is unclear whether nodule volume growth is a true risk for malignancy, because some benign nodules are in fact growing. Alexander et al. (21) observed that the proportion of thyroid nodules with an increase in volume of 15% or greater after 5 years was 89%. Similarly, Quadbeck et al. (22) followed 109 patients with benign thyroid nodules for at least 3 years and found that one-half of the benign nodules increased their volume by at least 30%. There has been no study confirming that progressive nodule growth is pathognomonic for malignancy. On the contrary, some studies reported that nodule growth itself is not necessarily a risk factor. For example, re-aspiration of nodules that became enlarged over a 5-year period revealed malignancy in only 1 of 74 nodules despite the average increase in volume of 69% (21). A small study showed similar rates of tumor growth between 15 cancers and 12 benign thyroid nodules (23). Recently, Kim et al. (24) followed 854 benign thyroid nodules and found that 171 (20%) showed a greater than 50% increase in volume, and among the 17 nodules that were operated on and 88 that were re-aspirated, only 1 malignant nodule was found (24).
The results of the present study demonstrate that nodule growth itself is not a predictor of malignancy in the FNAC-diagnosed ANs. Among the 196 nodules diagnosed as AN on FNAC but surgically resected thereafter because of enlargement during follow-up, there were only 1 PC and 1 FC. It should also be noted that the FNA specimens of these two malignant cases were not satisfactory for correct evaluation, because they contained colloid but very few epithelial cells. If the patients had undergone re-aspiration during the observation period, different cytologic diagnoses with more suspicious interpretations might have been made. The largest increase in the nodule volume change was in a 51-year-old female who initially presented with a 1.2 cm×0.5 cm×1.0 cm solid nodule (0.314 cm3 in volume). Over 8 years, the nodule became a mixed type lesion of 3.0 cm×2.3 cm×2.4 cm (8.61 cm3 in volume, 27.6 time-increase) and was surgically resected. The histologic diagnosis was AN. Four nodules were histologically diagnosed as FT-UMP, which is defined as an encapsulated tumor composed of well-differentiated follicular cells with questionable capsular invasion, no blood vessel invasion, and no PC-type nuclear changes (25).
Although the prognosis of FT-UMP is believed to be fairly good, similar to another borderline lesion, namely well-differentiated tumors of uncertain malignant potential (26), FT-UMP can be included among the candidates for surgical treatment. In the present study, the tumors deemed to need surgery (FT-UMP plus malignancy) accounted for only 3% of the 196 growing nodules. This ratio is significantly lower than that in the 346 benign nodules resected for reasons other than nodule growth (Fig. 1A). Because the other reasons for surgery in the latter group included US features suspicious for malignancy and large size of the nodule(s), this difference between the two groups is understandable.
For comparison, we also investigated the risk rate of growing FNs. Surgical excision for histologic diagnosis is generally advised for FN, which may comprise 20–30% of malignant lesions (7,8). Although the surgical approach is reasonable, it is also true that if all patients with FN are operated on, more than 70% of them would be undergoing unnecessary surgery. Therefore, at Kuma Hospital some FNs with no suspicious features on US are followed without immediate operation when they do not have any questionable clinicopathologic features as described in the Materials and Methods section. In the present series, there were 82 patients who were followed for some time and had a late operation after nodule growth (late-operation group) and 327 patients who had immediate surgery. The ratio of FT-UMP plus malignant nodules, i.e., the candidates for surgery, in the late operation group (46.3%) was significantly higher than that (30.0%) in the immediate surgery group (Fig. 1B). However, the initial volume, the final volume, and the percent ratio of nodule enlargement were similar between the benign nodule (AN plus FA) group and the FT-UMP plus malignant group. Because the observation periods varied between the patients, we have presented the percent ratio of nodule growth per year, and these data were also not significantly different between the two groups (Table 3). This suggests that an increase in nodule volume in FN should be considered a risk factor, but the growth rate itself does not correlate with malignancy.
Because the critical value of nodule growth is different between AN and FN, the clear differentiation of these two lesions at the preoperative stage, if possible, is clinically very useful. Although several observation keys for FNAC have been proposed (27) and US examination is helpful (28 –30), it is not always possible to make a correct differentiation of AN from follicular lesions including FA, FC, and the follicular variant of PC before histologic examination (27,31,32). In fact, strong disagreement regarding the assessment of encapsulated follicular lesions by FNAC has been described even among established thyroid pathologists (33). The difficult distinction between non-neoplastic ANs and neoplastic FAs was also demonstrated by a genetic microdissection analysis study: although the histologic appearance suggested a nonclonal hyperplastic AN, a genetic microdissection analysis revealed a homogeneous distribution of RAS mutations within these nodules, indicating that they are also clonal neoplastic lesions as follicular tumors (34). In this sense, we can satisfy the accuracy of FNAC at our institution: in the present study, among the whole groups of resected nodules, 80% of the 540 FNAC-diagnosed ANs were histologically confirmed to be true ANs, and there were only 38 FT-UMP plus malignant nodules (7%), for which surgery should be considered.
The ATA guidelines use a 50% increase in nodule volume as the criterion for significant change (5). This is based on the study by Brauer et al. (35), which included the nodules of 42 patients and reported the interobserver variation for the determination of thyroid nodule volume among three ultrasonographers as 49%. Since the variation may differ with each institution, we examined our interobserver variation among 13 ultrasonographers for the measurement of nodule volume using 50 patients with nodules and found that the interobserver variation at Kuma Hospital was almost negligible in light of the intraclass correlation coefficient results (0.983, 95% CI: 0.973–0.990). Based on the coefficient of variance for each ultrasonographer (approximately 20%), we decided that a >20% increase is a significant change in nodule volume at our institution. It should be noted that our cutoff value as a significant change in nodule volume cannot necessarily be applicable to other institutions. Theoretically, each institution should determine its own cutoff value based on its own interobserver variation.
This study has some strength and limitations. The advantage is that all benign nodules analyzed in this study were surgically resected and confirmed by histologic diagnosis. In the previous studies, the final diagnosis of the nodules was made by FNAC only (21) or surgery was done for only a small portion of whole patients (24). For example, the nodules not treated by surgery were all assumed to be benign in the study by Kim et al. (24), but as the authors acknowledged, the possibility of malignancy could not be fully excluded. In fact, the only malignant nodule they found among 105 nodules (17 nodules resected and 88 nodules re-aspirated) was a follicular variant of PTC, which exhibited benign US features and a benign FNAC result (24).
The major limitation of this study is derived from its retrospective nature. It is not exempt from the risk of selection bias, which is inherent to retrospective studies. The decisions regarding whether and when surgical resection was recommended to a patient with a growing nodule were dependent on each doctor's judgment. The follow-up examination intervals, the length of the observation periods, the performance of re-aspirations, and the ratios of nodule growth at operation varied among the patients. The second limitation may be the fact that the 196 growing nodules we analyzed had a low risk for malignancy from the beginning. Their US scores were all less than 3 and nodules with some undefined suspicious features for malignancy were excluded from this group. Therefore, the conclusion of the present study can only be applied to growing benign nodules with no suspicious features for malignancy on US. Third, although US examination can provide much information about the character of nodules in addition to the size, i.e., margin, shape, structure, taller than wide, calcification, intrathyroidal blood flow, and regional lymph nodes, we could not evaluate these US features in detail with respect to the malignant potential.
Despite these limitations, this is the first study, to our knowledge, to analyze many resected FNA-diagnosed benign nodules to determine whether nodule growth is indicative for malignancy and to reveal that the risk of malignancy is very low in FNAC-diagnosed ANs when there are no suspicious US features, even if the volume has increased significantly. By contrast, FNAC-diagnosed FNs have a higher risk of malignancy when they are growing.
Footnotes
Acknowledgments
The authors would like to thank all the doctors and staff at Kuma Hospital.
Author Disclosure Statement
No competing financial interests exist.