
Abstract

Several physicians have asked Genzyme to explain why serum thyroglobulin (Tg) sampling after recombinant human thyrotropin (rhTSH) stimulation cannot be done very early in the regimen.
Patients with differentiated thyroid cancer (DTC) who have an excellent response to initial treatment may require less aggressive ongoing management (1). The measurement of serum Tg is used as a biochemical tumor marker to identify persistent or recurrent disease in patients with DTC (2). Although Tg measurement while a patient remains on thyroxine therapy with a low serum thyrotropin (TSH) is under evaluation, optimal detection of smaller foci of disease has traditionally required stimulation of Tg production by high serum TSH concentrations (3). This can be performed by either thyroid hormone withdrawal (THW) or with the use of rhTSH.
The protocol for Tg stimulation approved by regulators in every country where rhTSH is marketed consists of an intramuscular (IM) injection of 0.9 mg of rhTSH in the buttock, followed by a second injection of rhTSH 0.9 mg IM 24 h later. A serum Tg is obtained 72 h after the second rhTSH injection (4). This leads to the question of how it was determined that serum Tg should be obtained at 72 h. To answer this question, further details of the data from the second phase 3 study (TSH95-0101) are reported (5). Formal new statistical analyses by Genzyme on these data from the 1990s were not possible at this time, and the company wants to present the data as actually reviewed by FDA in 1998 that resulted in the approved product label.
That phase 3 study included 113 thyroidectomized DTC patients who received injections of rhTSH on two consecutive days. But some of the patients had large thyroid remnants or substantial tumor in neck nodes, and seven patients had distant metastases. So those patients had levels of Tg >10 ng/mL at baseline, and their data are not included here. For the present question, we focused on just the 72 patients who had baseline Tg values <10 ng/mL after prior radioiodine remnant ablation. Even within this smaller group, the range of baseline Tg values was wide (1.0–9.0 ng/mL) but with a mean of 1.7 ng/mL.
These patients received rhTSH 0.9 mg IM on the equivalent of Monday and Tuesday, and serial Tg measurements were made on the equivalent of Monday (baseline) and then on Wednesday, Thursday, Friday, and the following Tuesday. That regimen of Tg specimen collection was referred to in the formal Genzyme study report as baseline and then as days 1, 2, 3, and 7 after the second injection of rhTSH. All serum Tg assays were performed in duplicate at one institution (University of Southern California, Endocrine Services) using a radioimmunoassay (RIA) employing certified reference material CRM-457 standardization.
The RIA used in the late 1990s had an analytical sensitivity of 0.2 ng/mL, a functional sensitivity of 0.5 ng/mL, and a reference range for euthyroid subjects of 3–40 ng/mL. All samples collected from an individual patient were tested in a single assay run. The basal serum specimen for each patient was screened for the presence of Tg antibodies using a quantitative RIA method with a detection limit of 1.0 IU/mL, which was calibrated against the WHO First International Reference Preparation 65/93 (5).
We plotted the serum Tg level at baseline and then at days 1, 2, 3, and 7 after the second rhTSH injection (Fig. 1). The results demonstrate that the highest mean Tg level was achieved more than 48 h after the final rhTSH injection. Although there was a wide variation in the individual patient Tg responses, likely in large part due to the nearly 10-fold range of baseline Tg values, the mean values continued to increase for 3 days, and then declined by day 7 (6).
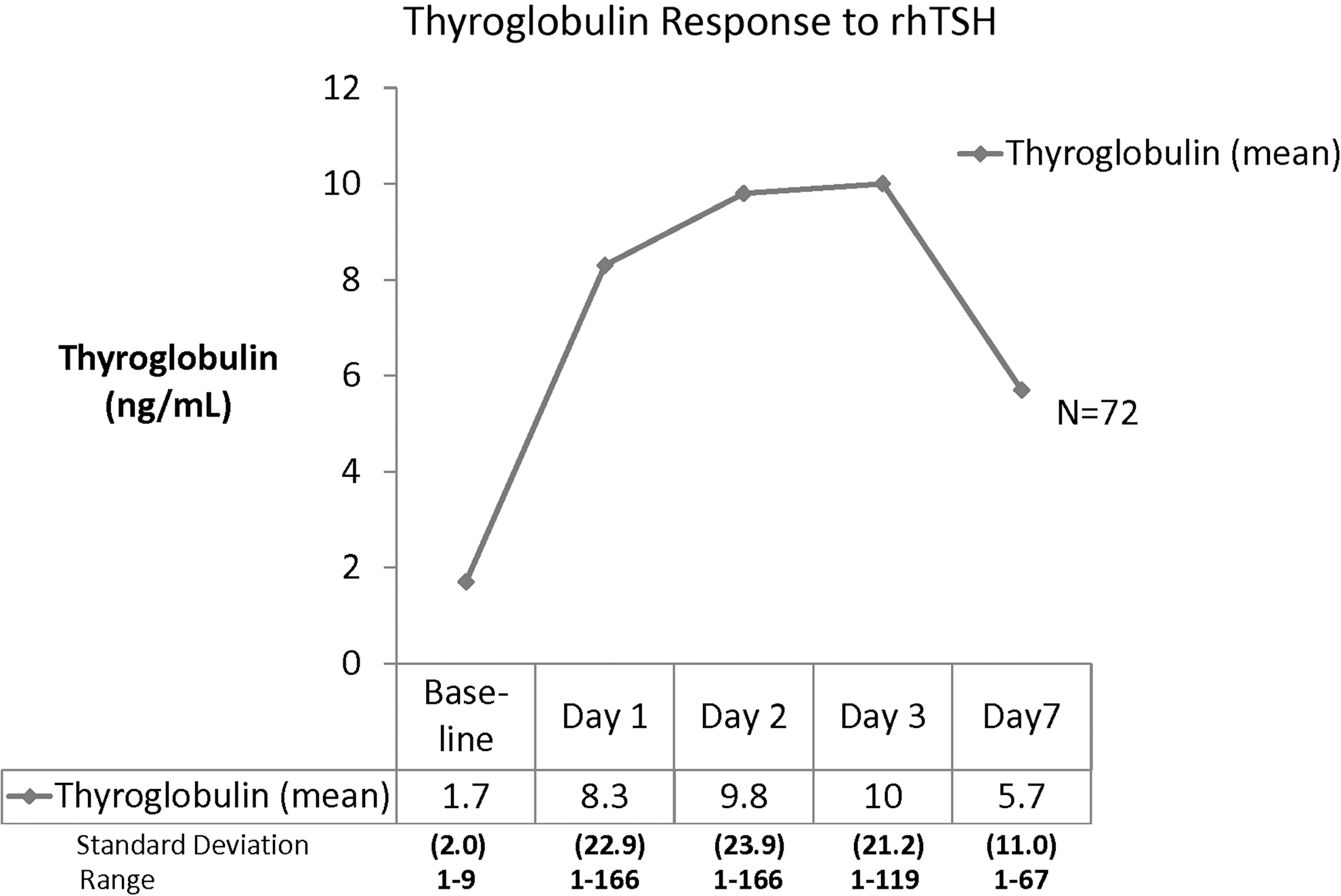
Thyroglobulin level at baseline and in response to recombinant human thyrotropin (rhTSH) injections on two consecutive days. Days 1, 2, 3, and 7 refer to days after the second rhTSH injection.
In 1998, Genzyme prepared extensive and complex receiver operator curve (ROC) analyses of the serial Tg data to evaluate proper timing of a measurement, as well as what useful cut-off level of Tg might exist. It was found that most patients had a peak serum Tg level on day 3 (Friday), equivalent to 72 h after the second rhTSH injection. The FDA's review of the kinetic data led to incorporation of this regimen into the U.S. package insert (PI), which specified that serum Tg testing should be performed 72 h after the second rhTSH injection.
Although Genzyme had prepared ROC analyses, likely due to a focused FDA interest on whole body scan (WBS) results, the analyses were viewed as secondary. In view of the fact that the first and second pivotal studies of diagnostic use of rhTSH were focused on what were then state of the art WBS results (as Tg was a newer technology at that time), the FDA agreed to a Tg measurement for evaluation after rhTSH, but the recommended timing of the draw was influenced, in the mind of the FDA, by the need for the patient to return for the WBS on day 3 (Friday). Additionally, the Tg kinetics data do support day 3 (Friday) as a reasonable day for the measurement.
In the 21st century, if physicians now wish to reduce scanning and emphasize Tg for follow-up, a larger and more detailed new clinical study focused on Tg likely would help clarify a number of questions, including which day is most appropriate for drawing the Tg level in response to TSH stimulation by rhTSH.
Additionally, we would like to clarify that obtaining serum TSH levels are not necessary in order to assess the Tg response to TSH stimulation with rhTSH. TSH levels rise and fall quickly with the use of rhTSH, which does not affect the efficacy of rhTSH. The rapidly declining TSH level could confuse physicians due to the traditional expectation of a serum TSH level >25 mIU/L that occurs with thyroid hormone withdrawal. So the measurement of TSH is not part of the approved protocol indicated in the U.S. PI.
Finally, the value of publishing these data from the 1990s is to inform clinicians and researchers of the actual data environment in 1998 when the FDA worked with Genzyme to construct the Tg draw regimen currently in the approved U.S. PI.
Footnotes
Acknowledgments
The phase 3 study TSH 95-0101 was performed by skilled investigators globally who included: Bryan R Haugen, Furio Pacini, Christoph Reiners, Martin Schlumberger, Paul W. Ladenson, Steven I. Sherman, David S. Cooper, Kathryn E. Graham, Lewis E. Braverman, Monica C. Skarulis, Terry F. Davies, Leslie J. DeGroot, Ernest L. Mazzaferri, Gilbert H. Daniels, Douglas S. Ross, Markus Luster, Mary H. Samuels, David V. Becker, Harry R. Maxon III, Ralph R. Cavalieri, Carole A. Spencer, Kevin McEllin, Bruce D. Weintraub, and E. Chester Ridgway.
Division of Endocrinology, University of Colorado Health Sciences Center (B.R.H., E.C.R.), Denver, CO; Division of Endocrinology, University of Pisa (F.P), Pisa, Italy; Klinik und Poliklinik fuer Nuklearmedezzin der Universitaet Wuerzburg (C.R, M.L.), Wuerzburg, Germany; Service de Medecine Nucleaire, Institut Gustave Roussy (M.S.), Villejuif, France; Division of Endocrinology and Metabolism, The Johns Hopkins University School of Medicine (P.W.L.), Baltimore, MD; Department of Medical Specialties, M. D. Anderson Cancer Center (S.I.S.), Houston, TX; Division of Endocrinology, Sinai Hospital of Baltimore (D.S.C.), Baltimore, MD; Division of Endocrinology, Oregon Health Sciences University (K.E.G., M.H.S.), Portland, OR; Genetics Division, Brigham and Women's Hospital (L.E.B.), Boston, MA; Division of Intramural Research, National Institute of Diabetes and Digestive and Kidney Diseases, National Institute of Health (M.C.S.), Bethesda, MD; Division of Endocrinology Mount Sinai Scholl of Medicine T.F.D.), New York, NY; Department of Medicine, University of Chicago School of Medicine (L.J.D.), Chicago, IL; Department of Internal Medicine, Ohio State University Health Sciences Center (E.L.M.), Columbus, OH; Thyroid Unit, Massachusetts General Hospital (G.H.D, D.S.R.), Boston, MA; Division of Nuclear Medicine, New York Hospital-Cornell Medical Center (D.V.B.), New York, NY; Nuclear Medicine, University of Cincinnati Medical Center (H.R.M.), Cincinnati, OH; Nuclear Medicine, Veterans Administration Medical Center (R.R.C.), San Francisco, CA; Department of Medicine, University of Southern California (C.A.S.), Los Angeles, CA; Genzyme Transgenics Corp. (K.E.), Boston, MA; and Laboratory of Molecular Endocrinology, University of Maryland School of Medicine (B.D.W.), Baltimore, MD.
Author Disclosure Statement
Richard Weiss, MD, and James Magner, MD, are employees of Genzyme, a Sanofi company, and are shareholders in Sanofi.