
Abstract
Background:
Establishing the reference interval for thyrotropin (TSH) and free thyroxine (T4) is clinically important because a number of disease states have been linked to alterations in TSH and free T4 concentrations that are within the 95% confidence interval for normal thyroid hormone values. Age, sex, time of day, and ethnicity are known to affect circulating levels of TSH and free T4 but have not been used to establish reference intervals. The purpose of this study was to define the reference interval for TSH and free T4 taking into account age, sex, ethnicity, and circadian and circannual variability.
Methods:
We performed a retrospective analysis of 465,593 TSH and 112,994 free T4 measurements from subjects ages 1–104 years with no thyroid disease using a single TSH and free T4 immunoassay method. Boundaries for the central 95% of patient values, taking into account hour of day, day of year, sex, and age were calculated.
Results:
Females had significantly higher TSH and free T4 levels than males; the magnitude of these differences did not exceed 0.1 mIU/L or 0.1 ng/dL respectively. Although the 2.5% TSH reference interval remains constant through the day, date, and age ranges, the upper limit (97.5%) of the TSH reference interval increases from 6.45 to 7.55 mIU/L with age, due primarily to a progressive increase in the amplitude of the nocturnal TSH surge. Additionally, significant ethnic differences in TSH circadian periodicity occur between African American, Pacific Island, and Caucasian populations.
Conclusions:
The reference interval for TSH varies significantly by age, sex, hour of day, and ethnicity. Time of year does not affect the TSH reference interval, and age, sex, hour of day and time of year do not affect the free T4 reference interval.
Introduction
I
Serum concentrations of TSH and free triiodothyronine (T3) are reported to show significant circadian periodicity (21 –24). The circadian variation in TSH is absent in infants younger than one month old (25) and in patients with Sheehan's syndrome (26). Sleep deprivation (27,28) and short-term untreated hypothyroidism (29) affect the nocturnal TSH surge. In contrast, the circadian TSH rhythm is not affected by treatment of hypothyroidism with either thyroxine (T4) or T3 (30). In addition to diurnal variations in thyroid hormone levels, circannual changes in a number of indices of thyroid function, including thyroid size, TSH, free and total T4 and T3 concentrations, and presentation of thyroid disease vary throughout the year (31 –38).
Reference ranges for thyroid hormone values, however, do not take into account variations in thyroid hormone concentrations that are circadian or circannual. To investigate whether diurnal or seasonal fluctuations in thyroid hormone values represent a significant independent source of reference interval variability, we conducted a retrospective review of the diurnal and annual variation in TSH and free T4 levels in 465,593 outpatients with no known thyroid disease.
Materials and Methods
This study, approved by the Intermountain Healthcare (Salt Lake City, Utah) Institutional Review Board, used data collected between June 2010 and November 2013 extracted from the Intermountain Healthcare Enterprise Data Warehouse.
Subjects
We studied 465,593 TSH measurements from 324,750 outpatients, ages 1–104 years, identified as having no clinical thyroid disease using the following criteria: Serum TSH 0.4–10.0, No diagnosis of thyroid disease, No filled prescription for medications used to treat hyper- or hypothyroidism (Supplementary Table S1; Supplementary Data are available online at No prescription for lithium, amiodarone, or anti-epileptic medications, No obstetric event (i.e., miscarriage or delivery) within 9 months of thyroid hormone measurement, No diagnosis of thyroid malignancy, and No hospital admission within 24 hours of blood collection.
The age, sex, number of TSH determinations (some patients had TSH measured on more than one occasion), and self-described ethnic distribution of these subjects are shown in Tables 1 and 2.
Outpatient blood testing took place at clinics, outpatient surgery centers, and laboratory drawing facilities located in urban and rural Utah and southern Idaho. The date and time at which each specimen was collected was recorded for each subject.
Hormone assays
Serum TSH and free T4 were measured using Abbott Architect immunoassays with external controls performed daily.
Data analysis
Quantile regression was used with periodic splines to calculate boundaries for the central 95% of patients given the hour of the day, day of the year, sex, and age group (the 2.5th percentile and 97.5th percentile were computed). Significance of the periodic splines was determined by comparing the smallest p-value, after adjusting for multiple comparisons by using the false discovery rate method within a group of splines, to the alpha level of 0.05 (39 –41).
Results
Table 3 and Figure 1 display the circadian reference interval (defined as the distribution of values that encompass 95% of all observations) for TSH by sex, age, and time of day. Supplementary Table S2 displays all age band reference intervals differed (p<0.05) from the reference interval for individuals of both sexes over 80 years of age. Additionally, for each age band, the reference interval for females was significantly higher than the reference interval for males. Circannual TSH reference intervals are shown in Table 4 and Figure 2. The circannual variation in TSH showed that the upper limit of the 95% reference interval for both sexes and all age groups had a low value of 4.31 in August and peak value of 6.06 in December. The lower limit of the 95% reference interval for TSH was 0.5 throughout the year. Although statistically significant differences in the upper limit of the monthly TSH reference interval were found (p<0.05), there were no clinically significant differences in the circannual TSH reference range by sex or age.
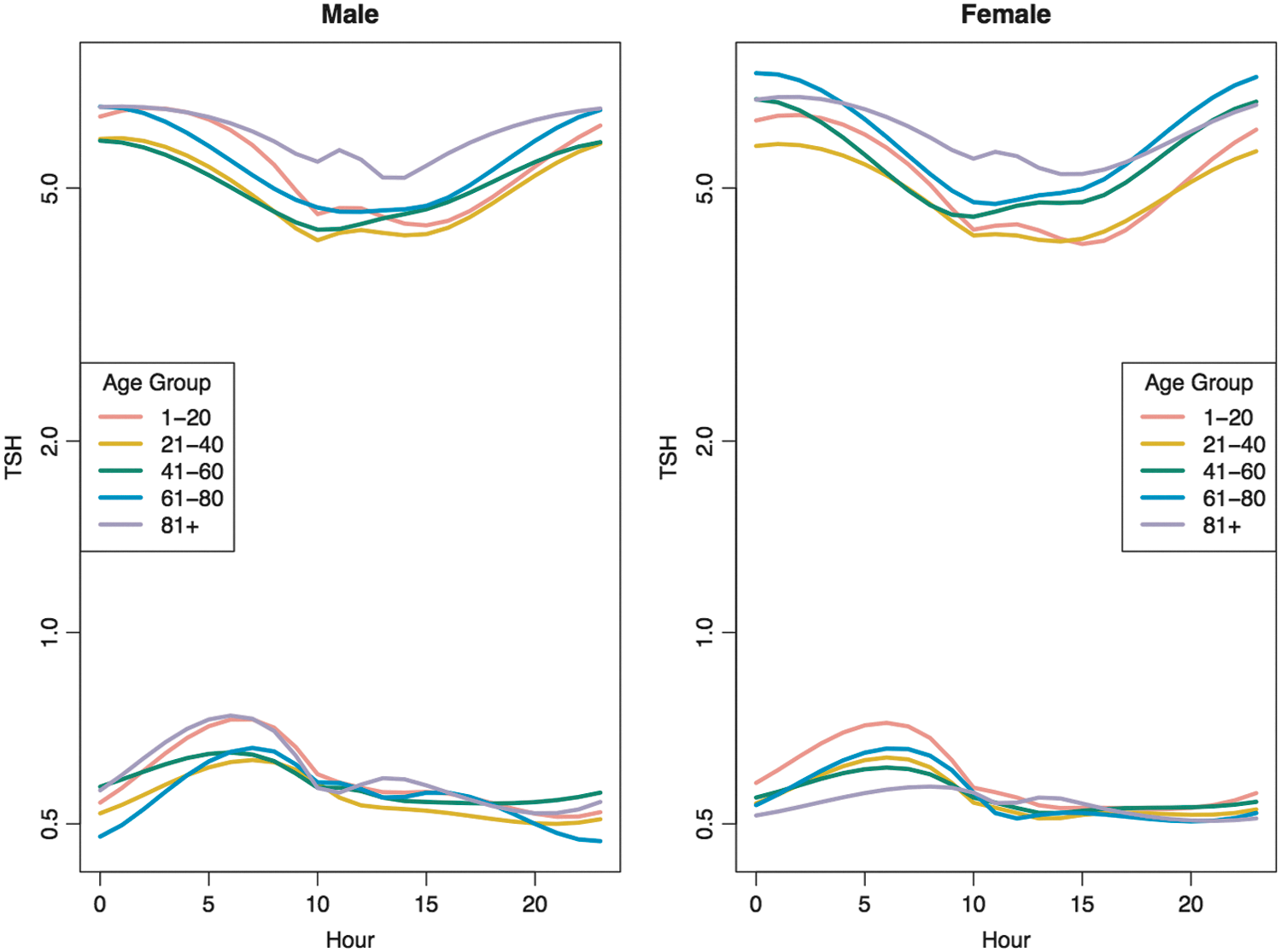
Thyrotropin (TSH) circadian reference interval by sex, age, and time of day.
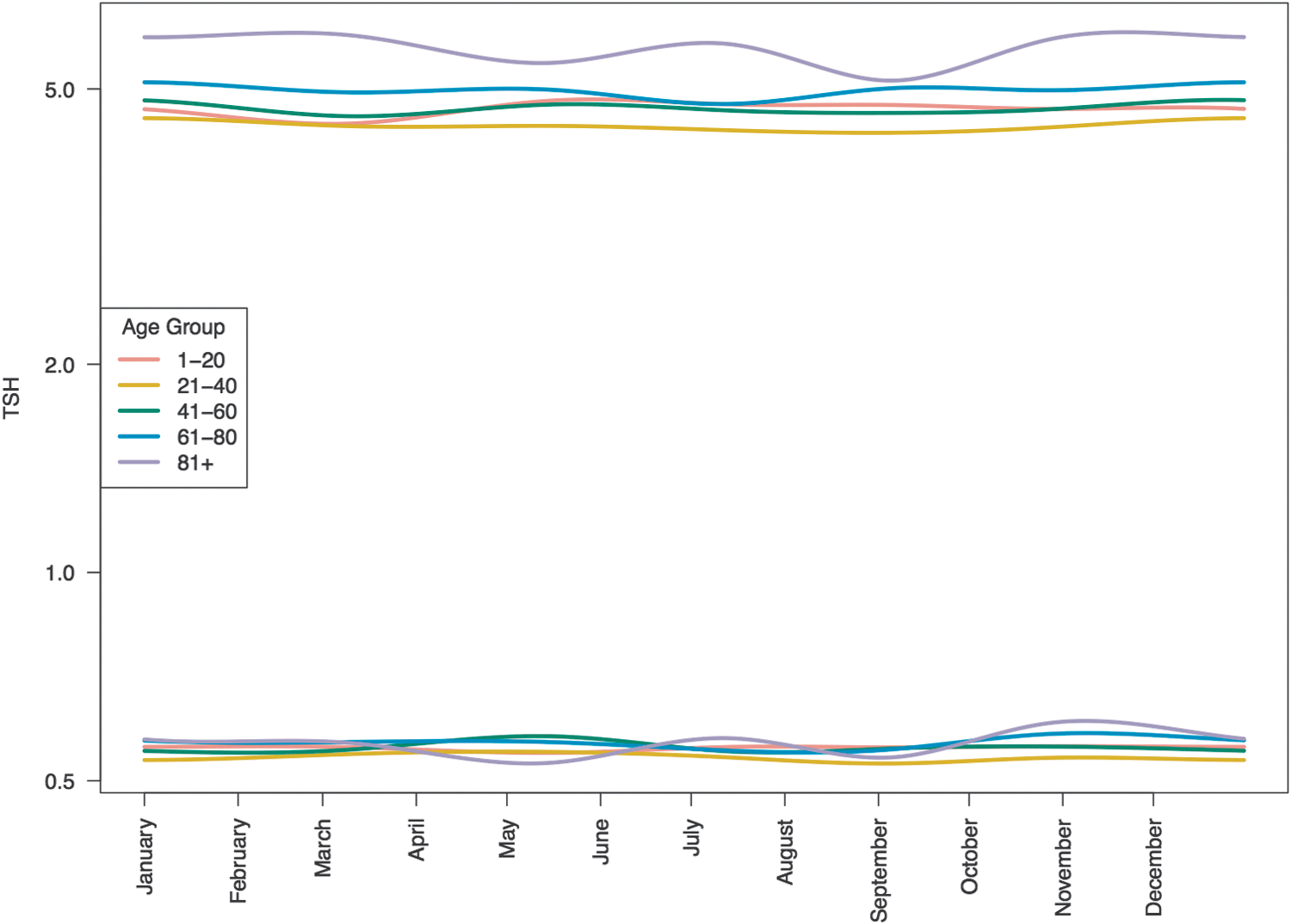
TSH circannual reference interval by age.
F, female; M, male.
Supplementary Tables S3A and S3B present the median TSH by age, sex, hour, and ethnicity. Self-described ethnic groups consisted of Native Americans, Pacific Islanders, African Americans, Asians, and Caucasians as well as other, unidentified, or unknown ethnicity. Although significant differences (p<0.05) in 24 hour mean TSH values between ethnic groups were present, the small number of subjects, shown in Supplementary Table S4, particularly in the >80 years age group, limit the interpretability of these observations.
Table 5 shows the number of subjects in whom free T4 was measured and number of free T4 observations. Table 6 and Figure 3 display the circadian variation in free T4 by age and sex. Table 7 and Figure 4 display the circannual variation in free T4 by age and sex. The circadian and circannual free T4 variations are modest in amplitude and the differences between age groups are not significant.
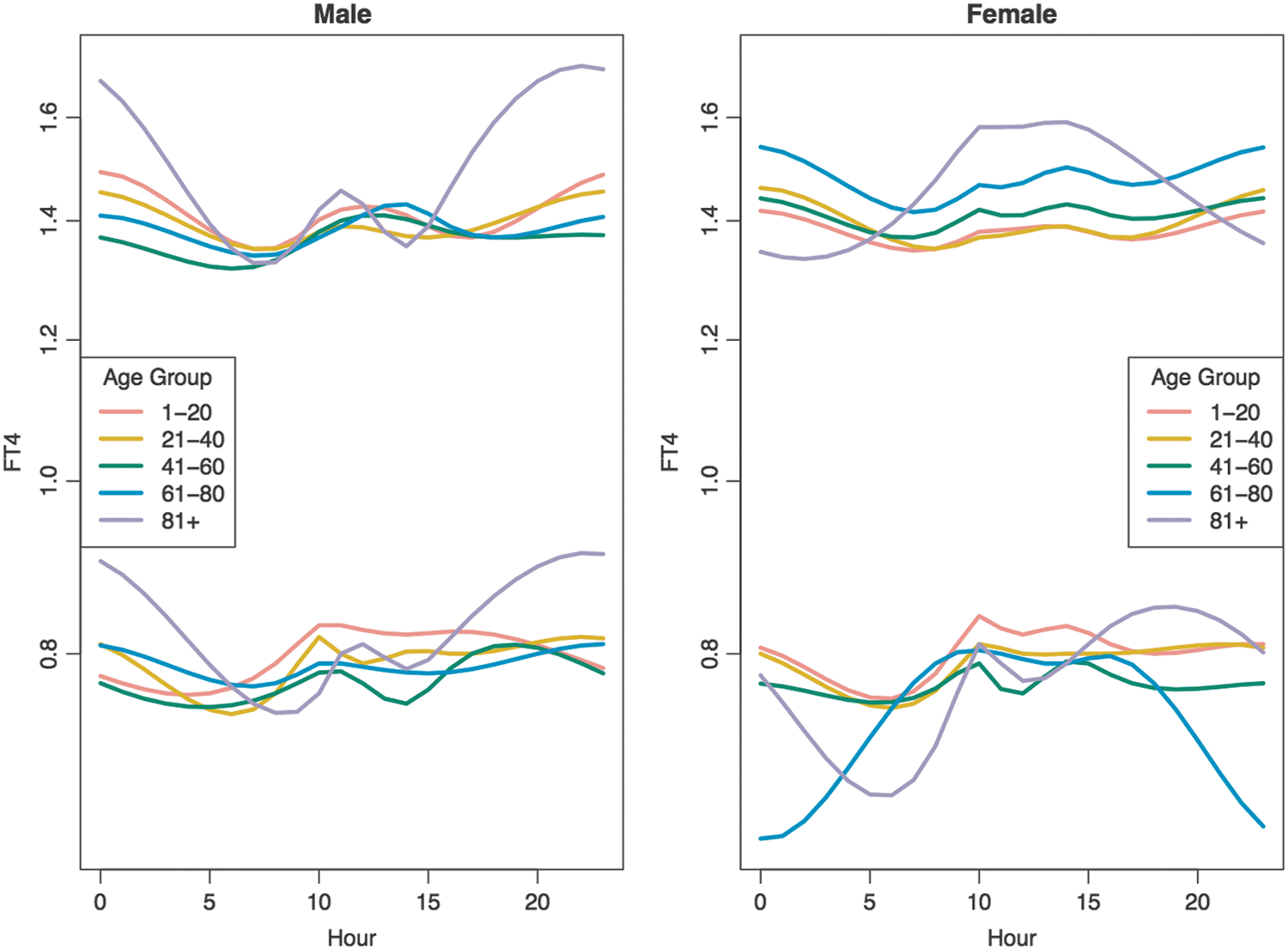
Free thyroxine (FT4) circadian reference interval by sex, age, and time of day.
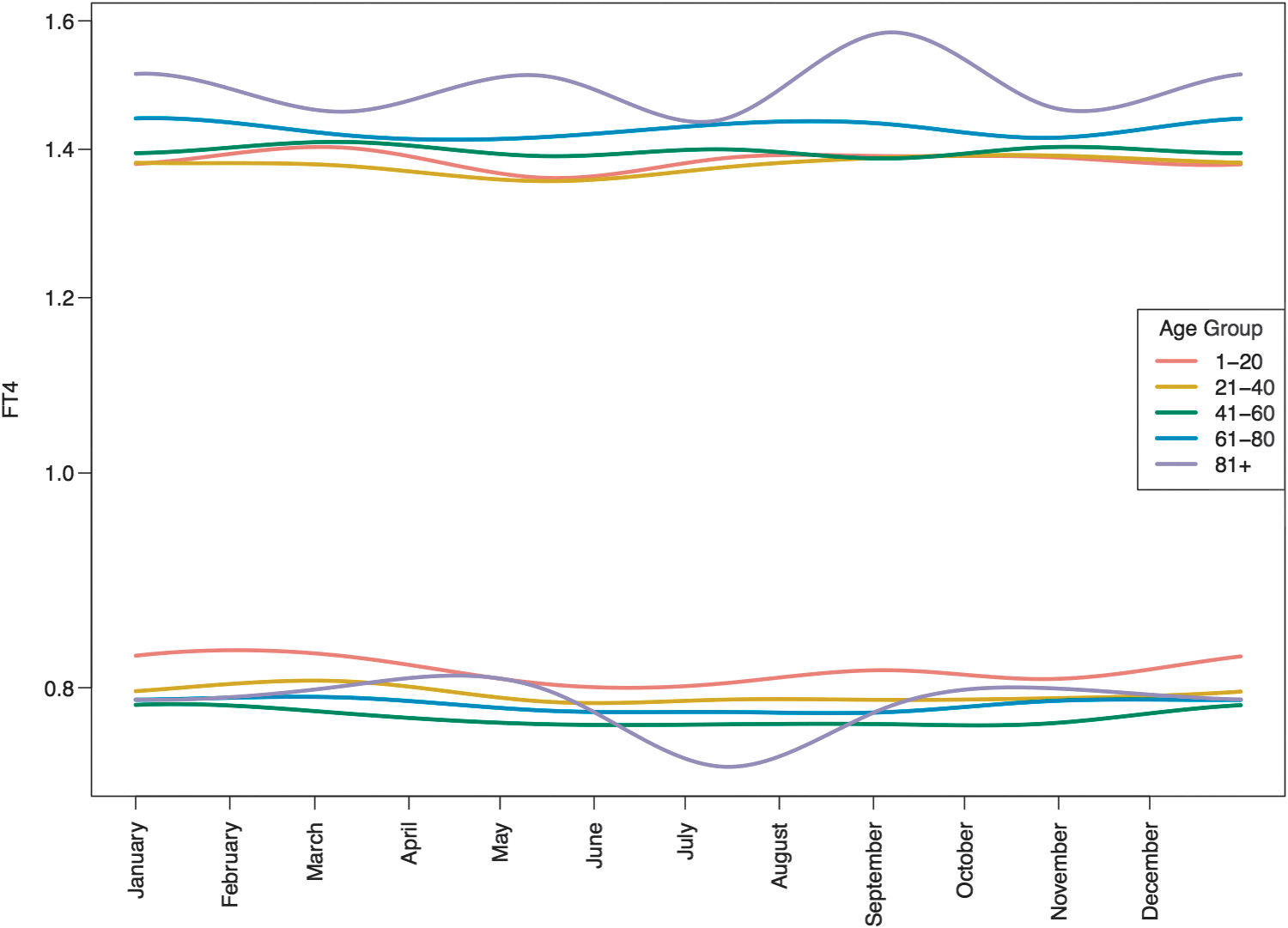
Free T4 circannual reference interval by age.
For all age bands and both sexes, the time of day when the lower bound of the reference interval was lowest was 0500h; the time of day when the lower bound of the reference interval was highest was 1000h.
For all age bands and both sexes, the time of day when the upper bound of the reference interval was lowest was midnight; the time of day when the upper bound of the reference interval was highest was 0700h.
For all age bands and both sexes, the month when the lower bound of the reference interval was lowest was February; the month when the lower bound of the reference interval was highest was June.
For all age bands and both sexes, the month when the upper bound of the reference interval was lowest was September; the month when the upper bound of the reference interval was highest was June.
Table 8 displays the composite 24 hour TSH and free T4 reference range for all age groups, times of day, and days of year. Although females have slightly higher TSH and free T4 values in all age cohorts, these sex differences never exceed 0.1 mIU/L or 0.1 ng/dL for either TSH and free T4 respectively; thus, sex (excluding pregnant women and oral estrogen administration) does not represent a significant variable for establishing a reference interval and is omitted. The 2.5% reference interval remains constant through the day, date, and age ranges. These data, however, demonstrate that the upper limit (97.5%) of the reference range increases significantly with age due primarily to a progressive increase in the amplitude of the nocturnal TSH surge.
Discussion
These results confirm prior observations that TSH exhibits a pronounced circadian rhythm in normal children and adults and agree with prior reports that mean TSH levels increase with age (42 –47). The 97.5 percentile for TSH reported here (6.5–7.6) is higher than has been previously reported. This is due to the inclusion of TSH values obtained throughout the 24 hour cycle. Prior studies did not include nocturnal TSH values. Although the vast majority of blood samples for thyroid hormone measurement are obtained between the hours of 0700 and 2000, clock time does not always correspond to biological time, particularly in individuals performing shift work or with jet lag or sleep disorders. To avoid incorrectly identifying TSH values as abnormal, the TSH reference range needs to take into account the subject's age and the time of day when the blood sample was drawn. For example, a TSH value of 7.5 mIU/L would generally be considered elevated and indicative of subclinical hypothyroidism. However, if the sample was drawn from an 80 year old woman at midnight, a TSH of 7.5 mIU/L is within the 95% reference range and is in fact normal.
Age-related alterations in thyroid function are well known, and a number of explanations for the progressive rise in median TSH have been proposed. These include alterations in TSH immunopotency and bioactivity, thyroid atrophy, chronic goitrogen exposure, subclinical hypothyroidism, and alterations in the negative feedback set point (48,49). Although medical TSH concentrations progressively increase with age and longevity, this study confirms prior observations that, despite an age-related increase in median TSH concentration, the circadian rhythm and nocturnal surge in TSH secretion do not change with age (50).
A prior study (50) of 46 normal subjects (mean age of 42±3 years) did not find sex differences in TSH secretory patterns between men and women. This study also found that age-related changes in TSH secretion occurred in women and not in men. We found, however, that sex differences in TSH circadian rhythms do occur and that both men and women show a progressive rise in TSH levels with age. Our study is based upon retrospective and aggregated data obtained from 324,750 individuals, while the prior study used 46 normal volunteers who had blood drawn under controlled conditions at 10 minute intervals over 24 hours. Demographic, data collection, analysis, and sample size differences are likely explanations for the discrepancy between our findings and those previously reported.
A number of prior publications have documented ethnic differences in thyroid hormone concentrations and recommend establishing population-specific reference intervals (51 –56). Self-reported ethnicity encompasses cultural, environmental, and geographic factors, as well as genetic factors. The basis for ethnic variations in mean circadian TSH values is not apparent and could result from a combination of iodine intake variability, obesity, tobacco use, goitrogen exposure, and genetic polymorphisms in thyroid hormone metabolism. Nonetheless the findings reported here confirm that ethnic variation in mean TSH values are present throughout the 24-hour cycle in African Americans, Asian, and Caucasians and extend these findings to include Native American and Pacific Island populations.
These findings raise a number of questions: how to determine whether TSH is suppressed, how to determine optimal T4 replacement dosage, and if TSH targets in the treatment of hypothyroidism vary by age. TSH suppression is standard treatment of thyroid cancer (57,58), and documenting TSH suppression is based upon a single TSH measurement. The measurement is usually obtained between the hours of 0700 and 2000, when TSH is normally lowest. TSH suppression during the day does not invariably mean that TSH is suppressed at night. Studies to determine the relationship between daytime TSH suppression and nighttime TSH suppression and the relationship between partial and complete 24 hour TSH suppression on thyroid cancer need to be performed. Determining TSH suppression in patients with thyroid cancer from a single daytime TSH value is similar to determining glycemic control in an individual with diabetes based upon a single blood glucose measurement. Selection bias makes the interpretation of the results and their clinical relevance questionable. Similarly, a recent study (59) concluded that T4 administration at bedtime resulted in higher T4 and lower TSH levels than an identical dose administered in the morning. In this study, the time of T4 administration did not alter the circadian TSH periodicity, but did change the amplitude of the nocturnal TSH surge.
The limitations of this study include the following: 1. The data are retrospective observations that used patient inclusion criteria of 0.4≤TSH≤10. This a priori assumption constrains the TSH reference interval to values between 0.4 and 10.0. Current standards of care (60) use TSH values between 0.45 and 10.0 as the established reference interval. Our use of TSH values 0.4≤TSH≤10.0 as a criterion for identifying individuals with normal thyroid function is consistent with accepted practice. 2. Thyroid ultrasonography and thyroid antibody measurement were not obtained to confirm that the subjects were euthyroid. The prevalence of anti-peroxidase and anti-thyroglobulin antibodies in the general population is sufficiently high and nonspecific that attributing the rise in median TSH levels with age to an increased prevalence of subclinical autoimmune thyroiditis is speculative (3). 3. The population studied is not representative of the United States population in general. Utah and the surrounding intermountain west are iodine sufficient. The ethnic makeup is primarily European ancestry and African Americans are under-represented. 4. The study assumes that immunoactivity corresponds with bioactivity. This is not necessarily the case. Thyrotroph cells secrete a variety of isoforms of TSH and immunoreactivity of the isoforms does not parallel bioactivity. Additionally, isoform variation can affect immunoassay results (61). The nocturnal TSH surge may reflect a variation in TSH isoform secretion from the pituitary (58) and not necessarily a change the concentration of bioactive TSH (61
–63). The nocturnal rise in T3, however, suggests that the nocturnal TSH rise does in fact have target tissue effects (22).
The strengths of the study are the large number of subjects (465,593 TSH measurements from 324,750 outpatients; 112,954 free T4 measurements from 69,223 outpatients), the multiyear study duration, and the use of a single analytic method for measurement of TSH and free T4 for the duration of the study. Prior studies show that interassay variation is a large source of variation in the measurement of both TSH and free T (64,65). Observations on this cohort, in summary, demonstrate that the reference interval for TSH varies significantly by age, sex, time of day, and ethnicity. Time of year does not affect the TSH reference interval, and age, sex, hour of day, or time of year do not affect the free T4 reference interval.
Footnotes
Author Disclosure Statement
No competing financial interests exist.