
Abstract
Background:
This study was performed to determine the benefits of core needle biopsy (CNB), as compared with fine-needle aspiration (FNA), for the diagnosis of thyroid nodules with macrocalcifications.
Materials and Methods:
The institutional review board approved this retrospective study, and informed consent was waived. From February 2010 to March 2012, the study included 147 thyroid nodules with macrocalcification of 145 consecutive patients who underwent simultaneous FNA and CNB for each nodule. Diagnostic accuracy and inconclusive diagnoses, including nondiagnostic reading and atypia of undetermined significance or follicular lesion of undetermined significance reading were compared among FNA, CNB, and a combination of FNA and CNB (FNA/CNB) using McNemar's test; the benefits of CNB were calculated.
Results:
Compared to FNA, CNB and FNA/CNB showed fewer inconclusive diagnoses (FNA vs. CNB: 62/147 [42.2%] vs. 14/147 [9.5%], p<0.001; FNA vs. FNA/CNB: 62/147 [42.2%] vs. 14/147 [9.5%], p<0.001), resulting in the avoidance of repeat FNA or diagnostic surgery in 48 of 62 patients (77.4%, respectively in CNB and FNA/CNB) who would have undergone these procedures if only FNA was performed. Compared to FNA, FNA/CNB showed higher sensitivity and accuracy (sensitivity: 23/32 [71.9%] vs. 31/32 [96.9%], p=0.008; accuracy: 77/86 [89.5%] vs. 85/86 [98.8%], p=0.008), resulting in avoidance of delayed surgery in eight of nine patients (88.9%) with thyroid cancer in whom the surgery would have been missed if FNA only had been performed.
Conclusion:
In the workup of thyroid nodules with macrocalcification, compared with FNA alone, FNA/CNB decreases inconclusive diagnoses and increases sensitivity, thereby reducing repeated FNA procedures, diagnostic surgeries, and delayed therapeutic surgeries.
Introduction
F
Macrocalcification is a frequently encountered finding in thyroid nodules. Although macrocalcification is known to be mainly dystrophic, many recent articles have reported that it is frequently associated with thyroid cancer, with malignancy rates ranging from 23.9% to 66.7% (9 –14). However, because macrocalcification in a thyroid nodule may restrict free needle movement during FNA, this procedure may not yield an adequate and representative cytological specimen. In fact, macrocalcification has been reported to be an important factor in the inadequacy of FNA (15,16). In addition, as for diagnostic accuracy, because the false negative rate of FNA is reportedly as high as 10.2% (17), it might be considered non-negligible in cases of thyroid nodules with macrocalcifications.
Traditionally, spring-activated core needle biopsy (CNB) has been suggested as a safe complementary tool for the work-up of thyroid nodules (2,18 –20), and several recent articles have noted its better diagnostic accuracy and adequacy compared with FNA (21 –24). A recent article also reported on the benefit of CNB in the diagnosis of calcified thyroid nodules (25). However, until now, there has been no investigation comparing CNB with FNA, a current diagnostic standard, for the diagnosis of thyroid nodules with macrocalcifications.
The purpose of the present study, therefore, was to determine the benefits of CNB, as compared with FNA, for the diagnosis of thyroid nodules with macrocalcifications.
Materials and Methods
Study population
The institutional review board approved a retrospective review of medical records and waived the requirement to obtain informed consent. From February 2010 to March 2012, simultaneous ultrasound-guided (US-guided) FNA and CNB were performed for 712 patients at two institutions (Seoul National University Hospital and Seoul National University Hospital Healthcare System Gangnam Center).
Using the definition of macrocalcification as a punctate echogenic focus >1 mm in diameter, 567 patients with 576 thyroid nodules without macrocalcifications were excluded. A total of 145 patients (112 female; M age=53.27 years; range 28–78 years) who presented for initial or repeat workup of 147 thyroid nodules with macrocalcification were enrolled (Fig. 1). Final diagnoses were obtained in 84 patients with 86 thyroid nodules. For 32 malignant nodules in 31 patients, the diagnosis was determined by histopathological results after surgery (30 papillary carcinoma; 2 follicular variant papillary carcinoma). For 54 benign nodules in 53 patients, a clinical diagnosis of a benign non-neoplastic nodule was made in the absence of a surgical diagnosis using the following criteria: (a) benign readings on FNA, repeated at least twice (n=11, 20.4%); (b) benign readings on FNA or CNB and stable size at follow-up for more than a year (n=13, 24.1%); and (c) concordant benign readings of FNA and CNB (n=30, 55.6%). During the study period, CNB was not successful in two nodules and could not be performed in one nodule, resulting in a 2% technical failure (3/150). Of these three cases, the core needle was not inserted into the nodule because of calcifications in two and because of a difficult location for performing CNB in one.
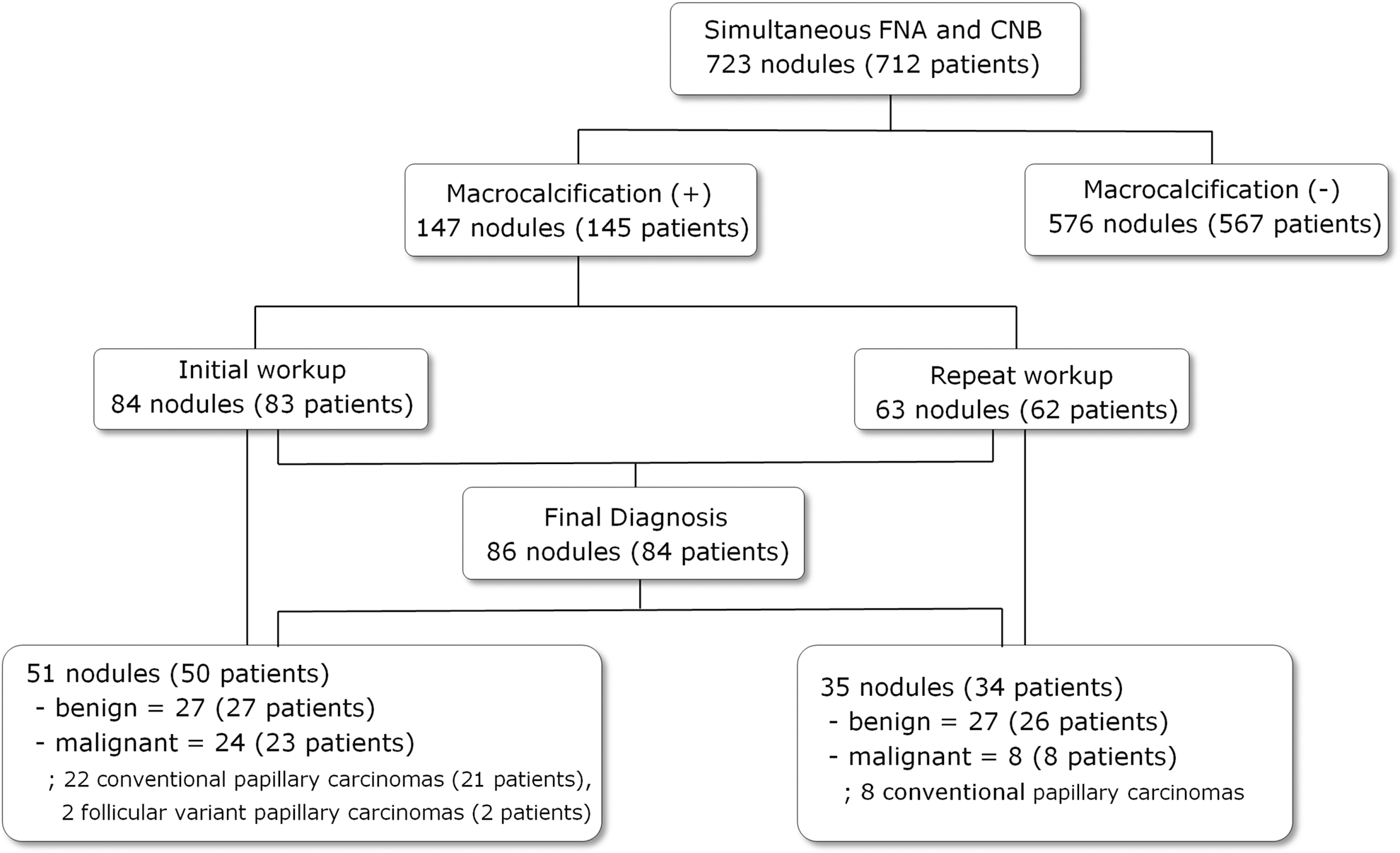
Flowchart of the study group.
US-guided FNA and CNB procedures
In the two hospitals, in addition to FNA, CNB was performed under US guidance in patients with thyroid nodules who had previous nondiagnostic or indeterminate FNA results, previous benign FNA results but features suspicious for malignancy on US, or an increased risk of nondiagnostic or nonrepresentative sampling through FNA alone (e.g., thyroid nodules with macrocalcifications). CNB was not performed in patients with bleeding tendencies, nodules with very strong hypervascularity on color Doppler US, or nodules in locations that rendered CNB technically infeasible. Whether FNA or CNB was performed first in the same nodule was determined by the operator according to the characteristics of each nodule.
High-resolution US machines with a 10–12 MHz linear transducer (IU22, Philips Medical Systems, Bothel, WA; AixPlorer, Supersonic Imagine, Aix en Provence, France; Logiq9, GE Medical Systems, Milwaukee, WI) were used to guide FNA and CNB. All FNA and CNB procedures were performed by four radiologists (D.G.N., J.H.K., H.B.S., and K.S.Y., with 17, 9, 4, and 5 years of experience in performing thyroid US, respectively). FNA and CNB were performed after administration of subcutaneous and perithyroidal local anesthesia with 1% lidocaine.
Sampling the entire nodule as evenly as possible, the operators aimed to obtain adequate specimens with sufficient visible aspirates with up to four needle passes for each nodule, using a combination of capillary and aspiration technique with 25-, 23-, or 21-gauge needles. Smears of the specimens were immediately fixed with alcohol and stained with Papanicolaou.
In the CNB procedures, the operators attempted to insert the tip of the biopsy needle into a gap or relatively weakened area of the calcified portion of the nodule, fire the stylet and cutting cannula of the needle sequentially, and thereby obtain a tissue sample from a noncalcified area, using a disposable 18-gauge, double-action, spring-activated needle (1.1- or 1.6-cm excursion; TSK Ace-cut, Create Medic, Yokohama, Japan) up to three times for each nodule. All tissue cores were placed immediately into 10% buffered formalin solution and were fixed and stained in the conventional fashion for histological examination.
All procedures were continuously monitored with real-time US to evaluate complications such as the development of hematoma or parenchymal edema. Each patient was observed with local compression of the biopsy site for 20–30 min.
Specimen interpretation
Independent and blinded evaluations of FNA cytological and CNB histological specimens were performed by a staff pathologist (H.S.M., with nine years of experience in thyroid cytohistopathology), according to the Bethesda system for reporting thyroid cytopathology (26).
Histopathological categorization of CNB specimens according to the Bethesda system was set according to recently published studies (21,22,24). To interpret the results of FNA/CNB, specimens were also categorized into the same six categories used by Sung et al. (22).
US analysis
Two blinded radiologists (C.H.S. and J.H.K., with 16 and 9 years of experience performing thyroid US, respectively) retrospectively evaluated US features of the thyroid nodules with regard to size, internal content, shape, margin, echogenicity, and calcifications according to the recommendations of Moon et al. (27). The radiologists obtained a consensus on a picture archiving and communication system workstation monitor (m-view; Marotech, Seoul, Korea).
One radiologist blinded to the histopathological results (K.S.Y., with five years of experience performing thyroid US) performed a computer-aided planimetric assessment to determine the proportion of calcification in each nodule. This assessment was done by manually tracing the macrocalcification area and the area of the entire nodule in two representative imaging planes using image analysis software (ImageJ 1.46; National Institutes of Health).
The proportion of calcification was defined as follows:
Proportion of calcification (%)=[(macrocalcificaiton area/entire nodule area)transverse view+(macrocalcificaiton area/entire nodule area)longitudinal view]/2×100.
If posterior shadowing from the calcification hindered the assessment of the portion of calcification, the shadowed areas were included in the calcified portion.
Statistical analysis
The incidences of each Bethesda category, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of diagnosis of thyroid malignancy were calculated for FNA, CNB, and FNA/CNB. Results categorized as suspicious for malignancy or malignant were defined as positive; the others were defined as negative. Results that were either nondiagnostic or categorized as atypia of undetermined significance or follicular lesion of undetermined significance (AUS/FLUS) were defined as inconclusive. In patients with a final diagnosis of thyroid cancer, delayed surgery was defined as a therapeutic surgery that was delayed because they were not properly diagnosed with thyroid cancer using FNA or CNB, although they were finally proved to have thyroid cancer.
The calculated values were compared between FNA, CNB, and FNA/CNB using McNemar's test for total, initial, and repeat groups. For analysis of the association between US features and diagnostic adequacy and accuracy for thyroid cancer in FNA and CNB, continuous variables in total group were compared by unpaired Student's t-tests, and categorical variables were compared by chi square analysis or Fisher's exact test as appropriate.
Statistical analysis was performed with SPSS Statistics for Windows v19.0 (IBM, Armonk, NY). A statistically significant difference was defined as p<0.05.
Results
Comparison of diagnostic results
Two nodules in one patient in the initial group were ultimately diagnosed as conventional papillary carcinomas; these were correctly diagnosed as malignancies on FNA, CNB, and FNA/CNB. Similarly, two nodules in another patient in the repeat group were ultimately diagnosed as benign; these were correctly diagnosed as benign on FNA, CNB, and FNA/CNB.
Table 1 lists the diagnostic results for FNA, CNB, and FNA/CNB in the total group. Tables 2 and 3 list results in the initial and repeat groups, respectively. For nondiagnostic results, CNB and FNA/CNB showed a significantly lower rate than FNA in the total, initial, and repeat groups. For benign diagnoses, CNB and FNA/CNB showed a significantly higher rate of diagnostic readings than FNA in the total, initial, and repeat groups. For the diagnostic category suspicious for malignancy, FNA/CNB showed a significantly lower rate than FNA in the total and initial groups. For the diagnosis of malignancy, CNB and FNA/CNB showed a significantly higher rate of diagnostic readings than FNA in the total and initial groups, and FNA/CNB showed a significantly higher rate of diagnostic readings than FNA in the repeat group.
Comparison of diagnosis of FNA and CNB.
Comparison of CNB and FNA/CNB.
Comparison of FNA and FNA/CNB.
CNB, core-needle biopsy; FNA, fine needle aspiration; FNA/CNB, combination of FNA and CNB; NA, not applicable; AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance; FN/SFN, follicular neoplasm or suspicious for a follicular neoplasm.
Comparison of diagnosis of FNA and CNB.
Comparison of CNB and FNA/CNB.
Comparison of FNA and FNA/CNB.
Comparison of diagnosis of FNA and CNB.
Comparison of CNB and FNA/CNB.
Comparison of FNA and FNA/CNB.
The histopathology of two nodules that had yielded nondiagnostic results on CNB revealed fibromuscular tissue in one, and thick fibrous tissue with dystrophic calcification in the other. These results suggest a mistargeted biopsy in the first, and the absence of a cellular component in an adequately targeted specimen in the second. The proportions of calcification in these two nodules were 98% and 72.6%, respectively.
Comparison of diagnostic efficacy
Of the 40 nodules that yielded nondiagnostic results on FNA, 31 (77.5%) were benign, four (10%) were AUS/FLUS, and three (7.5%) were malignant on CNB. Only two nodules (5%) were also nondiagnostic on CNB. No other nodules were nondiagnostic on CNB.
Of the 22 nodules that were AUS/FLUS on FNA, 11 (50%) were benign, two (9.1%) were suspicious for malignancy, six (27.3%) were malignant, and three (13.6%) were also AUS/FLUS on CNB. On CNB, nine nodules in addition to these three were AUS/FLUS.
The incidence of inconclusive readings was smaller for CNB (total: 14/147 [9.5%]; initial: 6/84 [7.1%]; repeat: 8/63 [12.7%]) and FNA/CNB (total: 14/147 [9.5%]; initial: 7/84 [8.3%]; repeat: 7/63 [11.1%]), compared to FNA (total: 62/147 [42.2%]; initial: 31/84 [36.9%]; repeat: 31/63 [49.2%]), (p<0.001, both CNB and FNA/CNB in all groups, respectively).
As a result, repeat FNA or diagnostic surgery was avoided in patients who would have undergone these procedures if FNA only performed, with CNB (total: 48/62 [77.4%]; initial: 25/31 [80.6%]; repeat: 23/31 [74.2%]) and with FNA/CNB (total: 48/62 [77.4%]; initial: 24/31 [77.4%]; repeat: 24/31 [77.4%]).
Diagnostic accuracy
Table 4 shows the diagnostic values of FNA, CNB, and FNA/CNB in the total, initial, and repeat groups.
p<0.008 between FNA and FNA/CNB.
PPV, positive predictive value; NPV, negative predictive value.
The sensitivity and accuracy of FNA, CNB, and FNA/CNB increased in order in the total, initial, and repeat groups, although statistical significance was attained in sensitivity and accuracy between FNA and FNA/CNB only in the total group.
The higher sensitivity for diagnosing thyroid cancer resulted in avoidance of delayed surgeries for patients with thyroid cancer, in whom the surgery would have been delayed if only FNA was performed. This was the case with CNB (total: 5/9 [55.6%]; initial: 4/6 [66.7%]; repeat: 1/3 [33.3%]) and with FNA/CNB (total: 8/9 [88.9%]; initial: 5/6 [83.3%]; repeat: 3/3 [100%]; Fig. 2).
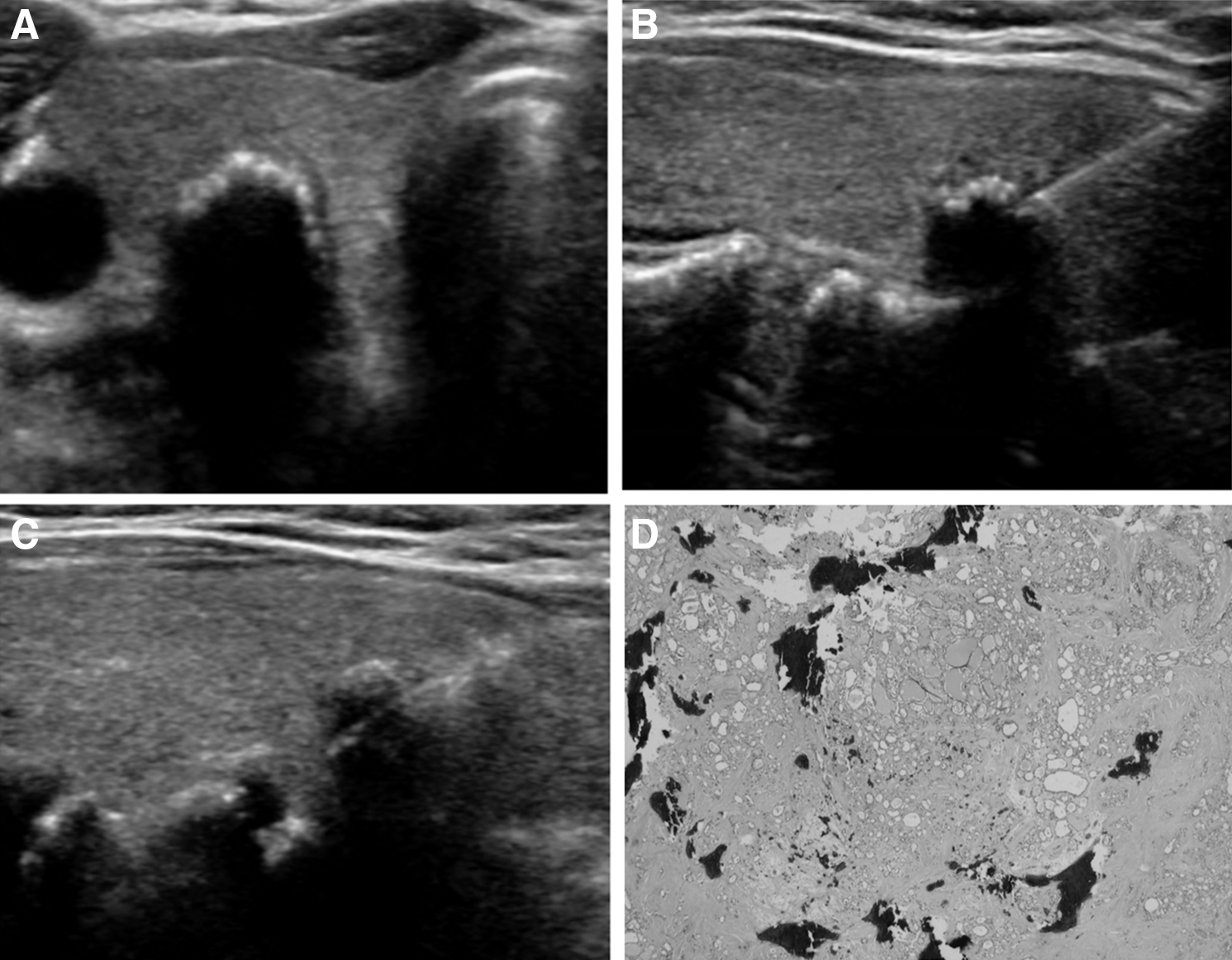
Images of a 63-year-old woman with a thyroid nodule with macrocalcifications (95.2% calcification). (
Four cases in the total group yielded false negative results on CNB; three were misdiagnosed as benign, and one was misdiagnosed as AUS/FLUS. Three of these cases were correctly diagnosed as either malignant or suspicious for malignancy on FNA and FNA/CNB. Only one case was misdiagnosed as benign on FNA and FNA/CNB. There were no false positive cases with FNA, CNB, or FNA/CNB.
US features affecting diagnostic adequacy and accuracy
Among the various factors, the proportion of calcification in nodules showing an inadequate diagnostic result was significantly larger than those showing an adequate diagnostic result in both FNA (40.1±29.3 vs. 29.3±26.7 %, p=0.036) and CNB (85.6±18.4 vs. 31.5±27.2, p=0.006).
The proportion of calcification in nodules yielding inaccurate results was significantly larger than in those yielding accurate results in CNB (64.3±32.7 vs. 27.3±25.4, p=0.001). The proportion of calcification in nodules with inaccurate results was larger in those with inaccurate results in FNA, but statistical significance was not obtained (35.2±30.8 vs. 27.2±25.5, p=0.203)
There were no statistically significant differences in other US features, demographic data, or needle passes for diagnostic adequacy and accuracy.
Complication
Four patients (2.7%) showed minor complications after simultaneous FNA and CNB procedures: perithyroidal hematomas in three (2.0%), and parenchymal edema in one (0.7%), all of which improved after compression and observation for less than an hour. There were no other serious complications that necessitated hospitalization or intervention in any of the patients.
Discussion
The results of our study confirm that thyroid nodules with macrocalcification require great clinical attention because of their substantial malignancy rate (37.2%, 32/86) and nondiagnostic and false negative rates on FNA (27.2%, 40/147, and 28.1%, 9/32). These results are consistent with the results of previous studies (10 –17).
For thyroid nodules with macrocalcifications, the study shows that adding CNB to FNA reduces the incidence of inconclusive diagnoses and produces more sensitive and accurate diagnoses than does FNA alone. This results in significant reduction of repeat FNA procedures, diagnostic surgeries, and delayed therapeutic surgeries. The results are in agreement with several previous reports and recommendations on the benefit of CNB over FNA, especially for nodules with prior nondiagnostic results (2,18 –21,23,24).
In the subgroup analysis, it was found that CNB and FNA/CNB did result in diagnostic benefits as an initial as well as a repeat diagnostic step. A recent report by Trimboli et al. argued that CNB could be applicable even in an initial diagnostic step (28). This argument could be especially relevant for nodules in which inadequate and inaccurate FNA results might be expected, such as nodules with macrocalcifications, as presented in this study.
Regarding factors that can cause nondiagnostic or inaccurate results in thyroid nodules with macrocalcifications, the data indicate that a high proportion of calcification might be the only important factor in FNA and even CNB. This is to be expected because a high proportion of calcification can prevent the free movement of the fine needle during an FNA and the advancement of the core needle in CNB from approaching the soft tissue component of the nodule. However, as this study shows, in most cases with nondiagnostic and inaccurate results on FNA, the powerful spring-activated core needle seems to resolve the difficulty of penetrating the calcification and allows collection of sufficient thyroid follicular cells for analysis.
Although many studies have reported on the diagnostic advantage of CNB alone, some studies have shown that a combination of CNB and FNA is more beneficial than CNB alone (22,23). This argument is also in line with the results of the present study. Although CNB yielded fewer false negative cases (4/32, 12.5%) than did FNA (9/32, 28.1%), three of the four false-negative cases found on CNB in the present study could have been correctly diagnosed as having thyroid cancer by adding FNA. The tissue diagnosis from CNB and cytological diagnosis from FNA seem to be synergistic for obtaining a correct diagnosis. For this reason, using FNA/CNB rather than CNB alone is advocated. In fact, many studies have shown that neither a combination of FNA and CNB nor CNB alone result in significant complications, as was the case in the present study (21 –23,29).
Ideally, CNB should precede FNA because CNB requires an intact tissue component, while FNA requires a cellular component that may be obtained after CNB is performed. FNA may destroy tissue integrity during the repetitive to-and-fro motion of the needle. In addition, for some thyroid nodules with macrocalcifications, the powerful spring action of the core needle into a hard calcification during CNB may make it easier to collect an adequate cellular component in a subsequent FNA procedure. However, if the nodule shows prominent vascularity on color Doppler US and seems to have a greater risk of hemorrhage after CNB, FNA should precede CNB. CNB may causes hematomas slightly more frequently than FNA does, although hematomas associated with CNB are not severe and are easily controlled.
There are several limitations to this study. First, because it is a retrospective review, there could be an unavoidable selection bias in addition to limitations in evaluating the US features. FNA and CNB are not usually performed in benign-looking nodules, and nodules diagnosed as benign on FNA and CNB do not undergo surgery and may not undergo follow-up US. Because of this, most nodules read as benign in this study were not confirmed through surgery and surgical pathology. Second, a lack of standardization in the cytohistopathologic diagnoses of CNB and FNA/CNB specimens demands further study.
In conclusion, in the workup of thyroid nodules with macrocalcifications, FNA/CNB decreases inconclusive diagnoses and increases the sensitivity compared to FNA alone, thereby reducing repeat FNA procedures, diagnostic surgeries, and delayed therapeutic surgeries.
Footnotes
Author Disclosure Statement
No competing financial interests exist.