
Abstract
Background:
The accurate diagnosis of thyroid nodules is important for making management decisions. The purpose of this study is to evaluate the clinical usefulness of BRAFV600E mutation analysis with core-needle biopsy (CNB+BRAFV600E ) in thyroid nodules with previous atypia of undetermined significance (AUS) or follicular lesions of undetermined significance (FLUS) results.
Materials and Methods:
From January 2011 to December 2012, 590 CNB+BRAFV600E mutation analyses were performed. We analyzed 200 nodules from 200 patients with previous AUS/FLUS results (22 men, 178 women; mean age, 48.6 years). The clinical usefulness of CNB+BRAFV600E was assessed by comparing the rates of conclusive results, the additional value of BRAFV600E mutation analysis, diagnostic performances, and therapeutic/diagnostic surgery results with those of CNB alone. For the subgroup analysis, the study patients were divided into those with nodules with previous AUS results and those with previous FLUS results.
Results:
All CNB+BRAFV600E procedures were well-tolerated. CNB+BRAFV600E did not show significantly better diagnostic performance than CNB alone in thyroid nodules with previous AUS/FLUS results. However, the conclusive result rate of CNB+BRAFV600E was improved in thyroid nodules with previous AUS/FLUS results (76.5% vs. 73.0%, p=0.016), especially with previous AUS results (81.1% vs. 76.4%, p=0.031). Of the 56 previous AUS result thyroid nodules with surgical management, BRAFV600E mutation analysis led to therapeutic surgery in 5.4% by decreasing unnecessary diagnostic surgery.
Conclusions:
In general, CNB+BRAFV600E did not show significantly higher diagnostic accuracy than CNB alone. Although CNB+BRAFV600E may add additional value in nodules with previous AUS results, routinely adding BRAFV600E mutation analysis to CNB is not recommended.
Introduction
T
To overcome this limitation, BRAFV600E mutation, a specific biomarker for papillary thyroid carcinomas, was suggested as an adjunctive diagnostic tool for patients with thyroid nodules, because it improves the diagnostic accuracy of FNA alone (10 –14). Several previous studies reported that BRAFV600E mutation analysis had a high positive predictive value (95.5%–100.0%) for the diagnosis of thyroid malignancy in thyroid nodules with AUS/FLUS FNA results (15,16).
Recently, US-guided, core-needle biopsy (CNB) has been suggested as an alternative diagnostic technique to FNA because it has better diagnostic performance and prevents unnecessary diagnostic surgery (17 –20). However, only one previous study of BRAFV600E mutation analysis with CNB (CNB+BRAFV600E ) has been reported (21), and the clinical usefulness of BRAFV600E mutation analysis of CNB has not been evaluated, especially in thyroid nodules with previous AUS/FLUS results.
The purpose of our study was to evaluate the clinical usefulness of CNB+BRAFV600E in thyroid nodules with previous AUS/FLUS results.
Materials and Methods
This retrospective study was approved by the institutional review board of our hospital, which waived the requirement for informed consent. However, all patients provided written, informed consent for CNB prior to undergoing the procedure.
Patients
From January 2011 to December 2012, 2411 US-guided CNB were performed at our institution. Of these 2411 CNB procedures, 590 BRAFV600E mutation analyses were performed when thyroid nodules had a previous indeterminate result including nondiagnostic or AUS/FLUS results, a discordance between previous FNA/CNB results and US findings, or a discordance between previous FNA and CNB results. A nondiagnostic result included the absence of any identifiable follicular thyroid tissue or the presence of only a few follicular cells insufficient for diagnosis. We included thyroid nodules with previous AUS/FLUS results. Finally, we analyzed 200 nodules from 200 patients with previous AUS/FLUS results (Fig. 1). There were 22 men (mean, 50.0 years; range, 31–65 years) and 178 women (mean, 48.5 years; range, 18–74 years) with a mean overall age of 48.6 years (range, 18–74 years). Twenty-two of the 200 patients were previously reported (17,20,22). These prior articles dealt with the diagnostic role of CNB in patients with nondiagnostic or inconclusive FNA results, whereas in this study we evaluated the clinical usefulness of CNB+BRAFV600E in thyroid nodules with previous AUS/FLUS results.

Flowchart of patient enrollment. US, ultrasonography; CNB, core-needle biopsy; AUS, atypia of undetermined significance; FLUS, follicular lesion of undetermined significance; FNA, fine-needle aspiration.
A final diagnosis was made in 159 nodules (79.5%). Sixty-five malignant final diagnoses were made when malignancy was confirmed on surgical pathology (n=65, 40.9%). Ninety-four benign final diagnoses were made when the benign status was confirmed on surgical pathology (n=6, 3.8%), with benign cytology findings obtained on at least repeated FNA and/or CNB (n=20, 12.6%), and when benign results obtained in CNB with a stable size at follow-up (n=68, 42.8%) (17,18,20).
US-guided CNB procedures
US examinations were performed using an iU22 or an HDI-5000 unit (Philips Healthcare, Bothell, WA, USA) or an EUB-7500 unit (Hitachi Medical System, Tokyo, Japan). All patients underwent a comprehensive US evaluation of their neck and thyroid gland (23). CNB procedures were performed by two clinically experienced thyroid radiologists (J.H.B. and J.H.L., with 17 and 12 years of thyroid US experience, respectively) or by residents or Fellows under their supervision.
For CNB, the biopsy procedures were performed using a 1.1 or a 1.6 cm excursion, 18-gauge, double-action, spring-activated needle (TSK Ace-cut; Create Medic, Yokohama, Japan) (17,18,20,22). We measured the longest diameter of the nodule and used power Doppler US to carefully evaluate the vessels along the approach route to avoid hemorrhage. After applying local anesthesia with 1% lidocaine, the end of the biopsy needle was advanced into the solid part of a nodule using a free-hand technique. After the tip of the biopsy needle had been advanced into the edge of the nodule, we re-evaluated the vessels around the nodule so as to minimize possible vessel injury. After measuring the distance of fire (1.1 or 1.6 cm), the stylet and cutting cannula of the needle were sequentially fired. Tissue cores were placed in 10% buffered formalin immediately after the procedure and were then conventionally processed (17,20).
The adequacy of the specimens was assessed by visual inspection. To be adequate, all negative smears obtained on CNB had to contain identifiable thyroid tissue (17,20). Additional CNBs were performed when a lesion was considered inaccurately targeted or when visual inspection indicated an insufficient specimen (17,20).
The biopsy site was firmly compressed and the patient was monitored for 10–20 minutes. We evaluated the occurrence of major complications. A major complication was defined as one that, if left untreated, might be life-threatening, lead to substantial morbidity or disability, or result in a lengthened hospital stay.
CNB histopathology analysis
CNB histopathologic specimens were reviewed by an experienced pathologist. Because the diagnostic criteria of CNB have not been standardized for thyroid nodules, the CNB histopathologic results were categorized into the same six categories as those for FNA cytology, according to the Bethesda System for Reporting Thyroid Cytopathology (17,18,20,24); that is, nondiagnostic, benign, AUS/FLUS, follicular/suspicious follicular neoplasm (FN/SFN), suspicious for malignancy, and malignant. A nondiagnostic CNB result included the absence of any identifiable follicular thyroid tissue, the presence of only normal thyroid tissue, or biopsies containing only a few follicular cells insufficient for diagnosis. Benign CNB findings included colloid nodules, nodular hyperplasia, and lymphocytic thyroiditis. AUS/FLUS results for CNB included nodules containing some atypical cells, although not consistent with suspicious for malignancy findings or malignancy, as well as follicular nodules that could not be definitively classified as follicular neoplasms or hypercellular hyperplastic nodules. FN/SFN results for CNB included nodules with histologic features suggestive for follicular neoplasm. Follicles suspicious for malignancy on CNB were those with specimens showing atypia, although with insufficient evidence for a definitive diagnosis of malignancy. CNB samples were classified as malignant when they showed unequivocal evidence of cancer (17,18,20,25).
DNA isolation and direct DNA sequencing
After a histopathologic review, 0.5 mL of lysis buffer (100 mmol/L sodium chloride; 10 mmol/L tris(hydroxymethyl)aminomethane [Tris], pH 8.0; 10 mmol/L EDTA, pH 8.0; and 0.5% [w/v] sodium dodecyl sulfate) and 7 μL of proteinase K (20 mg/mL, Gibco BRL, Carlsbad, CA) were added to the rest of specimen. The samples were incubated at 55°C for 12 hours to approximately 18 hours and at 95°C for 10 min in order to inactivate any remaining proteinase K. Genomic DNA was purified using QIAamp DNA Mini Kits.
For BRAFV600E mutation analysis, exon 15 of the BRAF gene was amplified by polymerase chain reaction (PCR), using the primer set of 5′-TGCTTGCTCTGATAGGAAAATG-3′ (forward) and 5′-CTGATGGGACCCACTCCAT-3′ (reverse). The amplification protocol consisted of an initial denaturation at 94°C for 2 minutes; 40 cycles of denaturation at 95°C for 10 seconds, annealing at 60°C for 30 seconds, and extension at 68°C for 40 seconds, followed by a final extension at 68°C for 7 minutes using KOD FX Taq DNA polymerase (Toyobo, Osaka, Japan). PCR products were electrophoresed on 2.5% (w/v) agarose gels and were subsequently sequenced using the above forward primer and the Big Dye Terminator (ABI systems, Applied Biosystems, Foster City, CA). Each DNA sequence was determined using an ABI-PRISM 3100 automatic sequencer (Applied Biosystems), and analyzed for the presence of the BRAFV600E mutation (26).
Statistical analysis
We calculated the rates of conclusive results of CNB and CNB+BRAFV600E . In CNB, a conclusive result was defined as a benign CNB finding or a malignant CNB finding according to the Bethesda System. Also, in CNB+BRAFV600E , a conclusive result was defined as a definite benign result (benign CNB finding with negative BRAFV600E result), or a definite malignant result (malignant CNB finding or positive BRAFV600E result). To evaluate the clinical usefulness of CNB+BRAFV600E , we calculated the additional value for BRAFV600E mutation analysis and compared the rates of conclusive results between the two examinations. An additional value was defined as a positive BRAFV600E mutation with a CNB deemed nondiagnostic, benign, AUS/FLUS, FN/SFN, or suspicious for malignancy.
The sensitivity, specificity, positive predictive value, and negative predictive value of CNB and CNB+BRAFV600E for the diagnosis of thyroid malignancy as well as the overall diagnostic accuracy were calculated, respectively.
For the subgroup analysis, we divided the study patients into two groups; that is, nodules with previous AUS results and previous FLUS results. The rates of conclusive results and the additional value for BRAFV600E mutation analysis, and the statistical measures were evaluated in each subgroup.
The surgical results and the reasons for surgery were analyzed. The rates of therapeutic and diagnostic surgery were calculated and the changes in the therapeutic and diagnostic surgery rates were evaluated after adding BRAFV600E mutation analysis to the CNB. Therapeutic surgery was defined as surgery performed for a therapeutic purpose due to FN/SFN, a suspicion of malignancy, or a malignant result on CNB or if there was a positive BRAFV600E result. Diagnostic surgery was defined as surgery performed for a diagnostic purpose if a nodule shows benign or inconclusive results on CNB+BRAFV600E , thus requiring further diagnostic examinations clinically.
Categorical parameters of the CNB and the CNB+BRAFV600E groups were compared using McNemar tests. A p-value <0.05 was considered statistically significant. All statistical analyses were performed using statistical software (SPSS, version 21.0; SPSS, Chicago, IL).
Results
All CNB procedures were well-tolerated and were completely finished without any major complications. The mean size of the 200 nodules was 11.7 mm (range, 3–50 mm).
Diagnostic outcomes of CNB and CNB+BRAFV600E
The results of CNB and CNB+BRAFV600E with the final diagnosis in all of the 200 nodules are summarized in Table 1. The incidence of conclusive results for CNB+BRAFV600E was significantly higher than that for CNB (76.5% vs. 73.0%, p=0.016). CNB+BRAFV600E showed a 5.5% (11/200) additional value for BRAFV600E mutation analysis for the detection of malignancy.
The benign and malignant final diagnosis (n=159) was classified according to the CNB/CNB+BRAF V600E findings.
CNB/CNB+BRAF V600E findings mean the test results for CNB and CNB+BRAF V600E and classified into six findings according to the Bethesda System.
The nodules which had an additional value on BRAF V600E mutation analysis were re-classified as malignant in CNB+BRAF V600E .
The initial result of this nodule was an FN/SFN with a positive BRAF V600E mutation, and the final diagnosis was a follicular adenoma which was confirmed by surgery.
FN/SFN, follicular neoplasm/suspicious for follicular neoplasm.
Of the 127 nodules with previous AUS results, the incidence of conclusive results for CNB+BRAFV600E was significantly higher than that for CNB (81.1% vs. 76.4%, p=0.031) (Table 2). Nine of 127 nodules (7.1%) showed the additional value for BRAFV600E mutation analysis.
CNB/CNB+BRAF V600E findings mean the test results for CNB and CNB+BRAF V600E and classified into six findings according to the Bethesda System.
The nodules which had an additional value on BRAF V600E mutation analysis were reclassified as malignant in CNB+BRAF V600E .
Of the 73 nodules with previous FLUS results, the incidence of conclusive results for CNB+BRAFV600E did not differ significantly from those for CNB (68.5% vs. 67.1%, p>0.999) (Table 2). Two of 73 nodules (2.7%) showed the additional value of BRAFV600E mutation analysis.
The diagnostic performance of CNB and CNB+BRAFV600E is summarized in Table 3. In total, in the 200 nodules with previous AUS/FLUS results, the sensitivity, negative predictive value, and diagnostic accuracy for CNB+BRAFV600E were slightly higher than those for CNB; however, there was no significant difference (p>0.05). In the 127 nodules with previous AUS results, the changes in the diagnostic performance after adding BRAFV600E mutation analysis to CNB showed the same tendency as those of all of the study patients. However, in the 73 nodules with previous FLUS results, all statistical measures, except for sensitivity, were slightly lower for CNB+BRAFV600E than for CNB, although without statistical significance (p>0.05).
Analysis of the reasons for surgery
Of the 159 nodules with a final diagnosis, surgery was performed for 71 (44.7%) of them; that is, six benign and 65 malignant lesions. Of these 71 nodules, 56 (78.9%) had previous AUS results and 15 (21.1%) had previous FLUS results.
Figure 2 shows the proportion of thyroid nodules according to the reasons for surgery. In all 71 nodules with previous AUS/FLUS results, the rates of therapeutic and diagnostic surgery for CNB were 83.0% (59/71) and 14.1% (10/71), respectively. After adding BRAFV600E mutation analysis, the therapeutic surgery rate increased to 87.3% (62/71) by decreasing the diagnostic surgery rate to 9.9% (7/71). Of the three nodules with changes from diagnostic surgery to therapeutic surgery by BRAFV600E mutation analysis, all of these nodules had previous AUS results and were confirmed as malignant (Table 4). Therefore, of the 56 nodules with previous AUS results, BRAFV600E mutation analysis led to therapeutic surgery in three (5.4%) nodules without delayed diagnoses or repeated examinations.
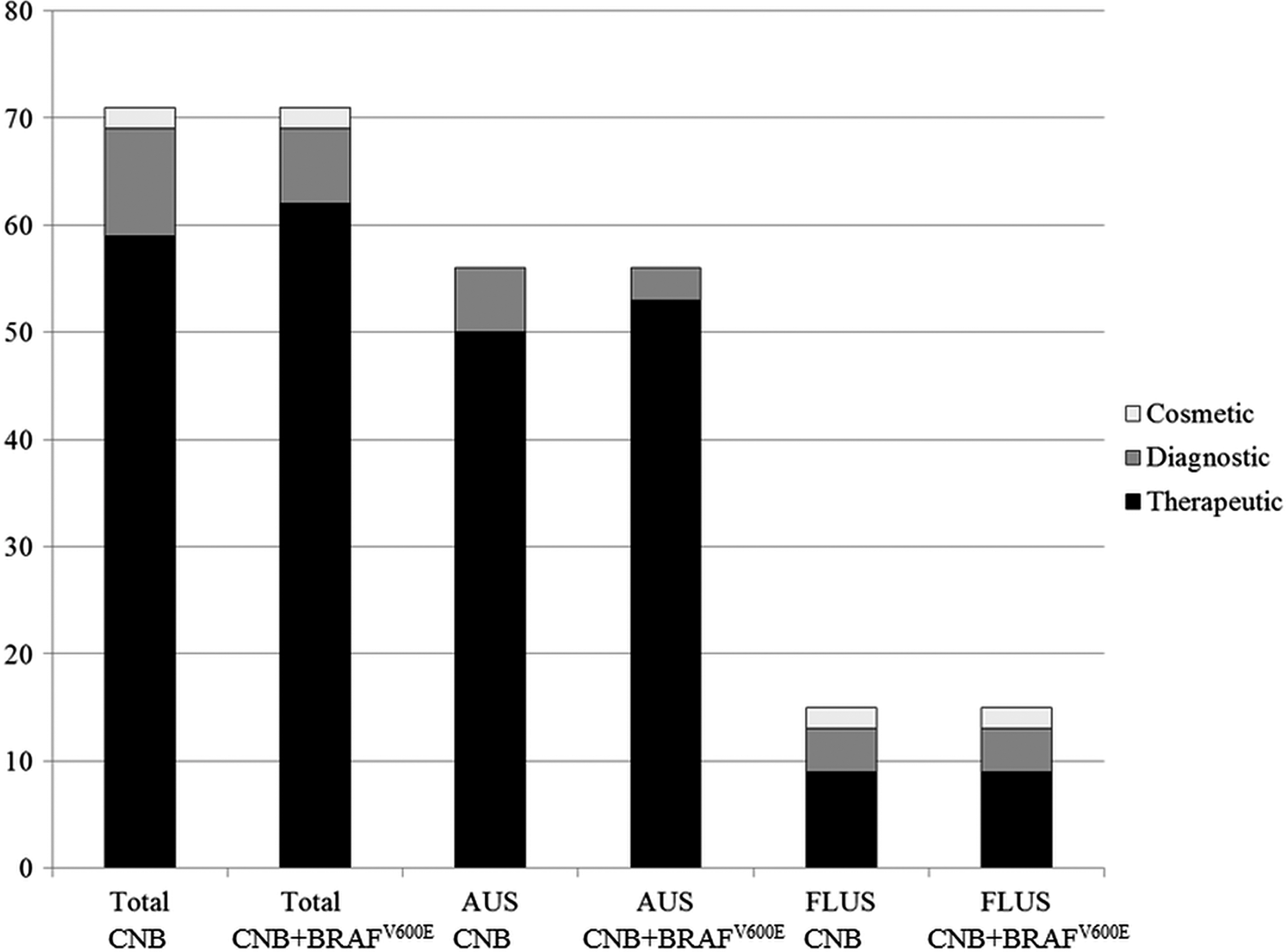
The reasons for surgery in the 71 thyroid nodules with previous AUS/FLUS results (AUS, 56 nodules; FLUS, 15 nodules).
Discussion
Our study demonstrates that CNB+BRAFV600E did not show a significantly higher diagnostic accuracy than CNB alone in thyroid nodules with previous AUS/FLUS results. However, the conclusive result rate of CNB+BRAFV600E was improved in thyroid nodules with previous AUS/FLUS results (76.5% vs. 73.0%, p=0.016). For the subgroup analysis, the conclusive result rate of CNB+BRAFV600E was improved in thyroid nodules with previous AUS results (81.1% vs. 76.4%, p=0.031), although it did not improve in thyroid nodules with previous FLUS results (68.5% vs. 67.1%, p>0.999). BRAFV600E mutation analysis also led to therapeutic surgery in 5.4% of thyroid nodules with previous AUS results. These results suggest that routinely adding BRAFV600E mutation analysis to CNB in thyroid nodules with previous AUS/FLUS is not effective, but selectively applying BRAFV600E mutation analysis to CNB in thyroid nodules with previous AUS results should be considered.
Several previous studies reported a significant improvement of sensitivity in FNA in combination with BRAFV600E testing (11,13). However, our study shows that the diagnostic performance for CNB+BRAFV600E was not significantly higher than that for CNB alone. According to the results of several recent studies, CNB had better diagnostic performance than FNA and showed a higher diagnostic accuracy (94.8%–98.4% vs. 60.0%–84.5%) and a higher sensitivity (91.3%–95.7% vs. 52.0%–72.3%) because CNB could include larger tissue samples and was able to assess the histological architecture and relationship to the adjacent thyroid tissue (17,25). Also, in several recent studies, the rate of nondiagnostic results for CNB was lower than that for FNA (1.1%–3.1% vs. 6.1%–40.0%) (17,18,22,25). Considering these differences between CNB and FNA, the improvement of the diagnostic performance achieved by adding BRAFV600E mutation analysis to CNB would not be significant.
Our study shows that BRAFV600E mutation analysis improved the conclusive results rate of CNB alone in thyroid nodules with previous AUS/FLUS results. This result was associated with improvement of the conclusive result rate of CNB+BRAFV600E in thyroid nodules with previous AUS results as there was no improvement in thyroid nodules with previous FLUS results. Recently, Choi et al. (22) suggested that the management strategy for AUS should differ from that for FLUS because there is a higher incidence of malignancy and surgical candidates in AUS than in FLUS. In contrast to AUS, because FLUS had a low association with papillary thyroid carcinoma and BRAFV600E mutation has rarely been seen in follicular variant of papillary thyroid carcinoma and is not found in follicular carcinoma (22,27,28), routinely adding BRAFV600E mutation analysis to CNB in all thyroid nodules with previous AUS/FLUS would not be effective. Previous studies have reported that BRAFV600E mutation analysis of FNA samples could create a 4.5%–19.3% improvement of the conclusive result rate with a 2.9%–12.6% additional value (10,12,13,15,16). In our study, CNB+BRAFV600E showed a similar additional value, but a slightly lower improvement of the conclusive result rate than FNA+BRAFV600E , as seen in previous studies. The improvement of the conclusive result rate for CNB by adding BRAFV600E mutation analysis could be lower than that for FNA, considering the higher conclusive result rate for CNB than for FNA (17,18,20,22,25). Therefore, in CNB, selectively applying BRAFV600E mutation analysis should be considered, especially in thyroid nodules with previous AUS results.
BRAFV600E mutation analysis in FNA is suggested for AUS/FLUS FNA results in the American Thyroid Association Management Guidelines (29). However, because most BRAFV600E mutation analyses have been separately performed from FNA and routinely added to FNA prior to determining the FNA results, selectively applying BRAFV600E mutation analysis for AUS/FLUS FNA results could be difficult. Recently, Poller and Glaysher (30) and Poller et al. (31) reported that BRAFV600E mutation co-testing was feasible by extracting DNA from FNA cytology smears. Therefore, selective applying BRAFV600E mutation analysis for AUS/FLUS FNA results could be done more easily by using BRAFV600E mutation co-testing. Considering that CNB can include larger tissue samples, BRAFV600E mutation co-testing from CNB is feasible and a further study for this application is needed.
According to the current guidelines, diagnostic surgery can be recommended for solid thyroid nodules with previously nondiagnostic or AUS/FLUS results (6,29). Several previous studies have addressed the clinical usefulness of CNB for preventing unnecessary diagnostic surgery, especially in patients with initially nondiagnostic FNA results (17,18,20), inconclusive FNA results (22,32), follicular neoplasm (33), and calcified nodules (34). In our study, BRAFV600E mutation analysis led to therapeutic surgery in 5.4% of the thyroid nodules with previous AUS results, thus preventing unnecessary diagnostic surgery. This is similar to the results of Moon et al. (35) who reported the diagnostic value of BRAFV600E mutation analysis for determining the need for therapeutic surgery. Therefore, adding BRAFV600E mutation analysis in thyroid nodules with previous AUS results could be clinically useful.
Our study has several limitations. Due to the retrospective study design, it may have an inevitable patient selection bias. This limitation could be minimized by including all of the thyroid nodules with CNB+BRAFV600E for the 2-year study period. Second, because there has been no previously published study regarding CNB+BRAFV600E using DNA sequencing, we could not directly compare the results of our study with those of a previous study or studies. Third, the lack of clinical indications for adding BRAFV600E mutation analysis requires further investigation.
In conclusion, CNB+BRAFV600E did not show a significantly higher diagnostic accuracy than CNB alone. Although CNB+BRAFV600E may add additional value in nodules with previous AUS results, routinely adding BRAFV600E mutation analysis to CNB is not recommended.
Footnotes
Author Disclosure Statement
No competing financial interests exist.