
Abstract
Background:
Differentiated thyroid cancer (DTC) is among the most common malignancies in the adolescent and young adult (age 15–39 years) population, and its incidence is rising. Younger age (<45 years) is an important prognostic indicator and is incorporated into the TNM classification system. This study hypothesized that this would result in distinct treatment patterns for younger and older patients.
Methods:
Using the California Cancer Registry, 24,362 patients with DTC from 2004 to 2011 were identified, and they were divided into younger (<45 years) and older (≥45 years) cohorts. Demographic and clinical variables were tabulated and then compared using chi-square tests. Treatment variables included total or near total thyroidectomy, other types of thyroid surgery, and the administration of radioiodine as part of the initial treatment. Multivariable logistic regression was used to identify independent predictors of treatment administered.
Results:
Younger patients were more likely to be Hispanic (32.5% vs. 21.2%) and female (82.7% vs. 74.7%), and to have papillary carcinoma (92.9% vs. 90.9%) and lymph node involvement (32.8% vs. 19.7%; p<0.0001). On multivariable analysis, younger patients (OR 1.20 [CI 1.11–1.30]), higher T-stage tumors, higher socioeconomic status (SES), and papillary carcinoma were predictors of undergoing total thyroidectomy versus less than total thyroid surgery. After adjustment, predictors of radioiodine administration included younger age (OR 1.12 [CI 1.05–1.18]), higher SES, total thyroidectomy, higher T stage, and lymph node positivity.
Conclusions:
Younger patients with DTC in California are more likely to be female and Hispanic with papillary histology. After adjustment for disease and demographic characteristics, younger patients are more likely to undergo total thyroidectomy as their initial surgery and are more likely to receive radioiodine. Given their excellent prognosis and the potential for adverse sequelae from initial treatment for DTC, these findings warrant consideration when managing younger patients with DTC.
Introduction
D
Pediatric thyroid cancer (age <15 years) is associated with an increased risk of presentation with advanced disease and nodal involvement (5,6). For this reason, more intensive initial surgery and more frequent use of radioiodine in pediatric patients has been recommended by several authors (7 –10). Young adult patients may not have as aggressive an initial course as pediatric patients, but the implication of the rising incidence of this disease on the type and intensity of initial treatment for young adult patients is not clear (11).
Surgical extirpation is the initial treatment for thyroid cancer, although the extent of initial surgery can vary based on risk assessment and provider or patient preferences. Similarly, the provision of postsurgical radioiodine is recommended for more advanced cases, but may not improve outcome in lower risk disease (12). Radioiodine treatment can have acute and long-term adverse effects, including salivary gland dysfunction, altered fertility, and the potential for secondary malignancies (13 –15). These effects may be particularly relevant to a younger population.
Given the rise in incidence of this disease in the young adult population and the potential consequences of treatment, this study sought to describe the epidemiology and initial treatment patterns of younger adult patients with newly diagnosed DTC.
Materials and Methods
Setting and subjects
A cohort of thyroid cancer patients was identified from the California Cancer Registry (CCR), a statewide, population-based cancer registry. The CCR is the single largest population-based cancer registry in the United States and contains demographic, diagnostic, treatment, and outcome information extracted from medical records for every reportable cancer diagnosed among residents of the state since 1988. Patients aged 15 years and older with histologically confirmed invasive DTC as the first primary malignancy diagnosed between 2004 and 2011 were included. Patients identified through death certificate or autopsy only and those for whom no surgical therapy was performed were excluded from the study.
Tumor variables
Pathologic data, including pathologic T, N, and M stages, are extracted from the pathology reports from the reporting institution. The International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3), histology codes 8050, 8260, and 8340-8344 defined papillary thyroid cancer. Histology codes 8290, 8330–8332, and 8335 defined follicular cancer.
Sociodemographic variables
Age, race, sex, and socioeconomic status (SES) were obtained as sociodemographic descriptors. Younger patients were defined as those younger than 45 years of age, as this is the major division for age within the AJCC staging system. SES is based on U.S. Census characteristics of the patient's address at diagnosis combined into the summary Yost index (16).
Treatment variables
The initial surgical treatment of the thyroid was obtained from the CCR field SURGPRIM, which captures the most extensive type of surgery performed during the first course of treatment. For the purposes of this study, initial surgery registry codes for total thyroidectomy or near total thyroidectomy were categorized into a total thyroidectomy group. All other primary thyroid surgeries were categorized as less than total. Similarly, the number of lymph nodes removed with the initial surgery and the administration of radioiodine data were acquired from the relevant registry fields.
Statistical analyses
After creating cross-tables between age categories among tumor, sociodemographic, and treatment variables, chi-square tests were used to identify whether the distributions were significantly different between the two age categories. In order to estimate the effects of tumor characteristic and sociodemographic predictors on treatment administered, simple and multivariable logistic regression analyses were performed for extent of initial surgery. These logistic regression analyses were repeated for the administration of radioiodine, including the additional variables of nodal status and extent of initial surgery. For logistic regression models, the odds ratio (OR) for each predictor and confidence intervals (CI) were reported. SAS v9.3 was used to conduct these analyses, and p-values of<0.05 were considered statistically significant.
Results
A total of 24,362 patients with newly diagnosed papillary or follicular DTC treated with surgery met the inclusion criteria for the study and were included (Fig. 1). Among these, 42.5% were diagnosed between the ages of 15 and 44 years (Table 1). Younger patients were more likely to be of Hispanic ethnicity and female, and less likely to be non-Hispanic white. Older patients were more likely to have a higher SES. Younger patients were more likely to have node positive disease (32.8% vs. 19.7%; p<0.0001) and less likely to have small T1 tumors. Presentation with distant metastatic disease was rare in both age groups. In unadjusted analysis, younger patients were more likely to have had complete thyroid surgery and received radioiodine.
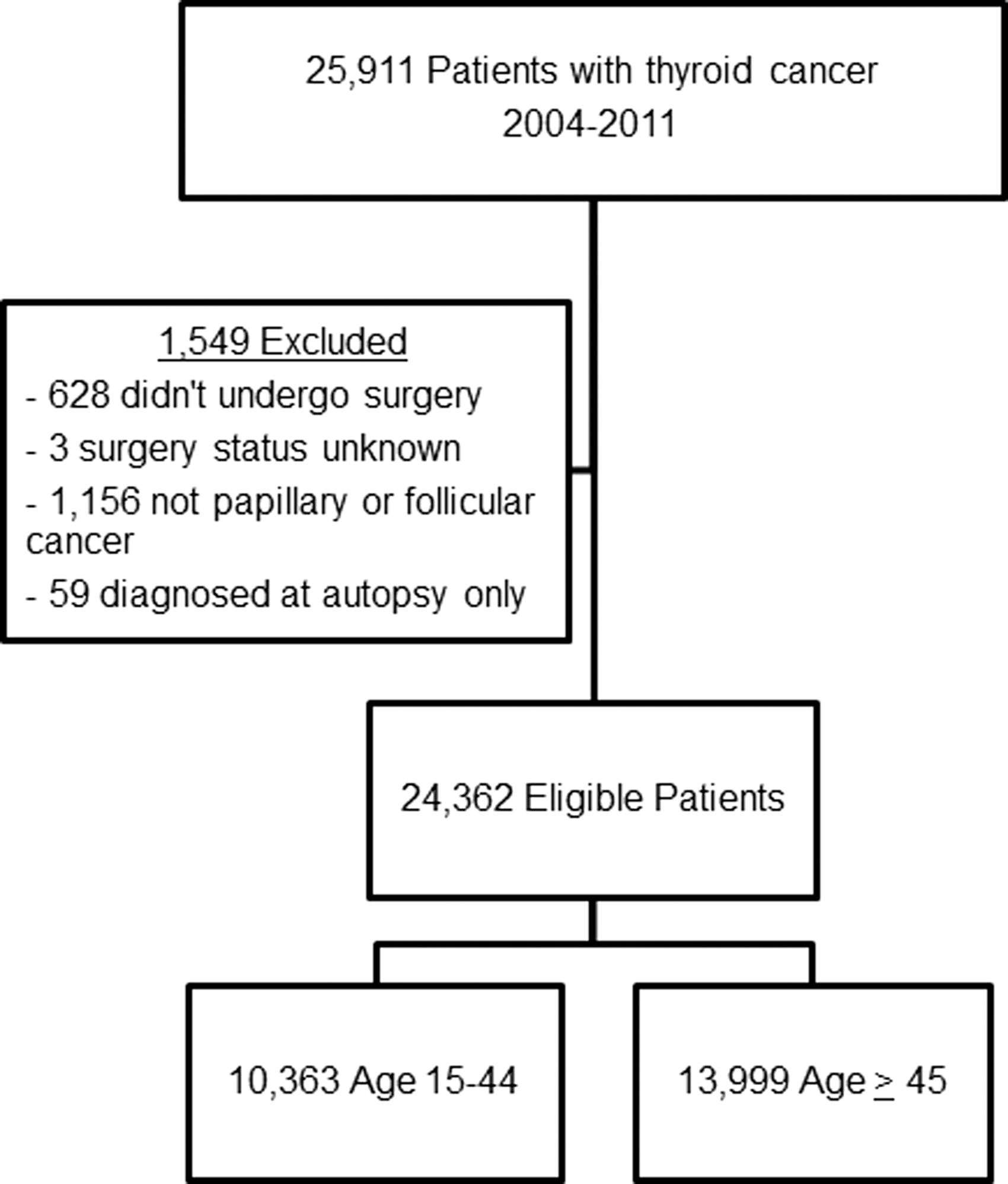
Selection of thyroid cancer patients included in this study.
n=10,363 (42.5%); b n=13,999 (57.5%).
Positive predictors of receiving a total thyroidectomy compared to less than total thyroid surgery included younger age, higher SES, higher T stage, the presence of distant metastatic disease and follicular histology in both simple and adjusted models (Table 2). The odds ratio for total thyroidectomy as initial treatment was lower in non-Hispanic black patients on univariate analysis, but this relationship did not persist when controlling for other sociodemographic predictors. Similarly, the odds ratio for total thyroid surgery in the Hispanic population was not significant on multivariable analysis.
In unadjusted analyses, younger and female patients were more likely to receive radioiodine during initial treatment (Table 3). Tumor stage and treatment predictors of increased radioiodine use included T stage other than T1, total thyroidectomy, and follicular cancer. Reduced odds were observed in node negative patients and those with fewer nodes harvested. Paradoxically, reduced radioiodine treatment was seen as part of the initial treatment in the small numbers patients presenting with distant metastases. However, this effect was not present in multivariable analysis. In multivariable adjusted analyses, the only significant predictors of radioiodine use were younger age, higher T stage, node positivity, and more extensive thyroid surgery.
Discussion
In this analysis of more than 24,000 patients diagnosed with DTC in California from 2004 to 2011, significant differences in the demographics and treatment of younger patients with thyroid cancer were found compared to older adults. Younger patients are more likely to be Hispanic and female. They tend to present with more advanced disease. Moreover, even after accounting for differences in staging distribution, it was found that younger patients with thyroid cancer are more likely to undergo complete initial thyroid surgery and be treated with radioiodine.
The underlying biology of younger patients with thyroid cancer may differ from that of older patients. In childhood thyroid cancer, the sodium iodide symporter (NIS) is frequently well expressed, and response to radioiodine is generally good, even in advanced disease (7,17). The data imply that while young adult patients may tend to present with slightly less advanced disease than children, larger tumors with positive nodes are more common in this population than they are in the older adult population. A high prevalence of Hispanic females was observed in the younger population. While the Hispanic population in California is on average younger than the general population, the incidence rates between age groups vary between foreign-born and US-born Hispanic subpopulations (18).
Major strengths of this study are its size and the quality of data captured by the CCR. As the natural history of thyroid cancer is long and this population-based cohort is relatively recent, survival outcomes based on initial treatment and sociodemographics were not examined. Nonetheless, the recent rise in thyroid cancer incidence has been tied to SES, suggesting that greater health utilization and access to care may impact the diagnosis of thyroid cancer (19,20). Younger patients tended to have lower neighborhood SES levels in this study. However, this may have been strongly influenced by a larger Hispanic population, a group that has lower average neighborhood SES levels (21). In a large study of AYA thyroid cancer patients, lack of insurance was found to be an independent risk factor for more advanced disease at presentation (22). The data from this study add to the literature by suggesting that the decision regarding the extent of initial treatment is also influenced by SES, resulting in different decisions in similar stage patients with different sociodemographic characteristics. The results are consistent with a smaller study of thyroid cancer patients in the Surveillance, Epidemiology, and End Results program that suggested increased odds of radioiodine use in the AYA thyroid cancer population (23). Moreover, the present results provide large-scale support to the concept that there is significant variation in the administration of radioiodine for low-risk thyroid cancer that goes beyond tumor characteristics to include those of preferences of the patient and experience of the medical team (24 –26).
There are several limitations of this large retrospective cohort design. It is possible that unmeasured prognostic characteristics may differ between younger and older cohorts and impact the decision for initial treatment. Indeed, each of the factors included in the American Thyroid Association risk stratification algorithm cannot be captured (12). Specifically, there is limited information on capsular invasion and no information regarding angiolymphatic invasion. The details of the nodal dissection during the initial surgery are incomplete. Nonetheless, a larger number of nodes examined was not predictive of radioiodine administration on multivariable analysis. Importantly, there are no data regarding the activity of radioiodine administered. It is possible that the higher odds of radioiodine administration in younger patients are indicative of administration of lower activities for remnant ablation. Given the long natural history of DTC, there was insufficient follow-up to analyze differences in survival based on the initial treatment administered in this recent cohort.
In California, the demographics of thyroid cancer differ between younger and older patients. Younger patients are more frequently female and Hispanic. Patterns for initial treatment are also different between younger and older patients, as younger patients are more likely to undergo complete thyroid surgery and receive radioiodine. Given the rapid rise in the incidence of this disease, the relatively good prognosis of young patients diagnosed with thyroid cancer, and the potential for long-term sequelae from these treatments, these results suggest that further study is need to confirm that this does not represent overtreatment of this population.
Footnotes
Acknowledgments
T.S. was supported by the National Cancer Institute of the National Institutes of Health under award number K12CA138464. This study was also supported by the UC Davis Cancer Center Support Grant, P30CA093373-06. This work was presented in part at the 84th Annual Meeting of the American Thyroid Association, Abstract 2041168.
Author Disclosure Statement
All authors have no conflicts of interest to disclose.