
Abstract
Background:
Standard dosimetric methods to determine the maximum tolerated activity (MTA) of 131I for the treatment of metastatic, well-differentiated thyroid cancer (DTC) are time-consuming and require complex analysis. As a result, reliable, accurate, and simplified methods are desirable. The objective of this study was to evaluate the validity of a simple regression dosimetry model.
Method:
Previously, the authors reported a bi-exponential model for estimating the MTA of 131I for the treatment of metastatic DTC based on a limit of 2 Gy to the blood. This model uses the patient's body surface area (BSA) along with the fractional whole-body retention (WBR) at 48 hours following oral administration of a diagnostic dosage of 131I. A bi-exponential regression model was developed between the MTA normalized to the patient's BSA and the percent retention value at the 48-hour time point (R): MTA (GBq)/BSA (m2) = (13.91 · e−0.0387R + 42.33 · e−0.8522R). In this study, the same model was applied to a different set of adult patients referred for dosimetry and possible 131I treatment of DTC under conditions of thyroid hormone withdrawal or recombinant human thyrotropin (rhTSH) stimulation. All patients (n = 170; 96 female) referred to the authors' clinic for dosimetry and possible 131I treatment for metastatic DTC during the collection period were included in this study, apart from those undergoing renal dialysis. The MTA predicted (MTAp) using the model described above was compared to the measured MTA (MTAm), with statistical analysis performed using ProStat v4.5.
Results:
In this group, the MTAm ranged from 2.3 to 41.1 GBq. The linear correlation between the MTAp and MTAm was excellent (r = 0.96), with an average deviation of only ± 1.2%. However, to avoid overdosing a patient on the basis of the MTAp, a weighting factor (<1.0) should be applied (e.g., using a value of 0.7 would result in only one patient receiving a prescribed activity of 131I that exceeded the MTAm [<3%]).
Conclusions:
The % 48-hour WBR as determined by the bi-exponential function noted herein with reasonable restrictions has been validated as a reliable simplified dosimetry model.
Introduction
T
Consequently, an empirically determined activity of 131I is often used for the treatment of metastatic DTC and assumed to be applicable to the overall general population of patients with DTC. However, the use of empiric fixed prescribed activities is not without risk. As reported by Tuttle et al. (1), an empiric prescribed activity of 7.4 GBq (200 mCi) would have actually exceeded the calculated maximum tolerated activity (MTA) in 8% of the patients, and this would have increased to 19% if 9.25 GBq (250 mCi) were to be administered. Furthermore, 50% of elderly patients (aged ≥70 years) would have exceeded their MTA if 9.25 GBq (250 mCi) were to be administered for their 131I treatment. Very similar results were reported by Kulkarni et al. in a study of 127 dosimetries (2). In order to avoid excessive exposure to radiosensitive organs, such as the bone marrow, some form of patient-specific dosimetry would be required in order to determine if a higher prescribed activity of 131I could still be “safely” administered or if a lower prescribed activity of 131I should be administered. Unfortunately, dosimetry involves time and resources, along with a moderately complex data analysis. Therefore, Sisson et al. proposed a simplified approach that utilizes the percent 48-hour whole-body retention (% 48-hour WBR) of 131I as the basis for modifying the standard empiric dosage of 131I (3,4). Subsequently, the authors reported on a more quantitative model with a number of distinct advantages that incorporated Dr. Sisson's % 48-hour WBR with a bi-exponential function (BF) to estimate the MTA of 131I for the treatment of DTC (5). This BF is much easier to use than conventional whole-body dosimetry (WBD), and is based on a relatively simple measurement of the % 48-hour WBR of 131I. Although the whole-body clearance of iodine may be 30% faster when using recombinant human thyrotropin (rhTSH) injections rather than thyroid hormone withdrawal to stimulate iodine utilization by the metastatic thyroid tissue (6), it has also been demonstrated previously that the same model is applicable to either method of patient preparation (7). One problem with prediction models is that they tend to perform better on the data set that was used to construct the model than on a new data set (8). This difference in performance stems partially from optimism in the validity of the model based on the derivation data set. While some methods of internal validation such as bootstrapping have been used (9), external validation is essential for prediction models to be used in clinical practice (8).
The objective of this study was to evaluate the validity of the previously developed regression dosimetry model (5) in a large, independent group of patients with DTC.
Materials and Methods
A retrospective Institutional Review Board–approved review was conducted of all thyroid carcinoma dosimetries performed on adult patients (aged ≥16 years) at the authors' institution between February 2000 and May 2009 who (i) were not used to establish the previous regression model and who (ii) had DTC, (iii) had a total or near-total thyroidectomy, (iv) were suspected of having metastatic disease (e.g., by clinical exam, elevated serum thyroglobulin levels with negative antithyroglobulin antibodies, other imaging modalities, and/or histology), and (v) either underwent thyroid hormone withdrawal in preparation for 131I therapy with adequately elevated TSH levels at the start of the dosimetry (e.g., >25 mIU/mL or if <25 mIU/mL, then <25 mIU/mL with 131I uptake >5% in thyroid bed/lesion) or received rhTSH. Patients receiving renal dialysis were excluded.
For the dosimetry, whole-body retentions at approximately 24-hour intervals were determined from the geometric mean of anterior and posterior scans normalized to the initial measurement performed one or two hours post-administration. The MTA was determined using the Benua–Leeper method originally developed at the Memorial Sloan Kettering Cancer Center, with the incorporation of several minor modifications in the data collection, as previously reported (10). This dosimetry is based on a maximum tolerated radiation absorbed dose of 200 rad (cGy) to the blood (MTD). The % WBR at 48 hours was interpolated from the whole-body time–activity curve using a log–log function for correlation with the MTA. The MTA for each patient was normalized to their body surface area (BSA), which was calculated based on the Mosteller formula that was used to minimize sex effects by incorporating the patient's height and weight into the analysis.
Results
The validity of the model was assessed in an independent group of 191 dosimetry studies that were performed in 170 patients (96 females) in anticipation of 131I therapy (Table 1). The preparation for their radioiodine therapy was either thyroid hormone withdrawal (THW) (n = 94) or rhTSH stimulation (n = 97). The average measured MTA (MTAm) based on the standard dosimetry protocol for the collective group was 11.6 GBq (430 mCi; range 1.7–41.1 GBq). As seen in Figure 1, excellent linear correlation (r = 0.96) is demonstrated between the predicted and measured MTA based on the model shown above. Based upon an average discrepancy of approximately zero, there is no apparent bias in the methodology.
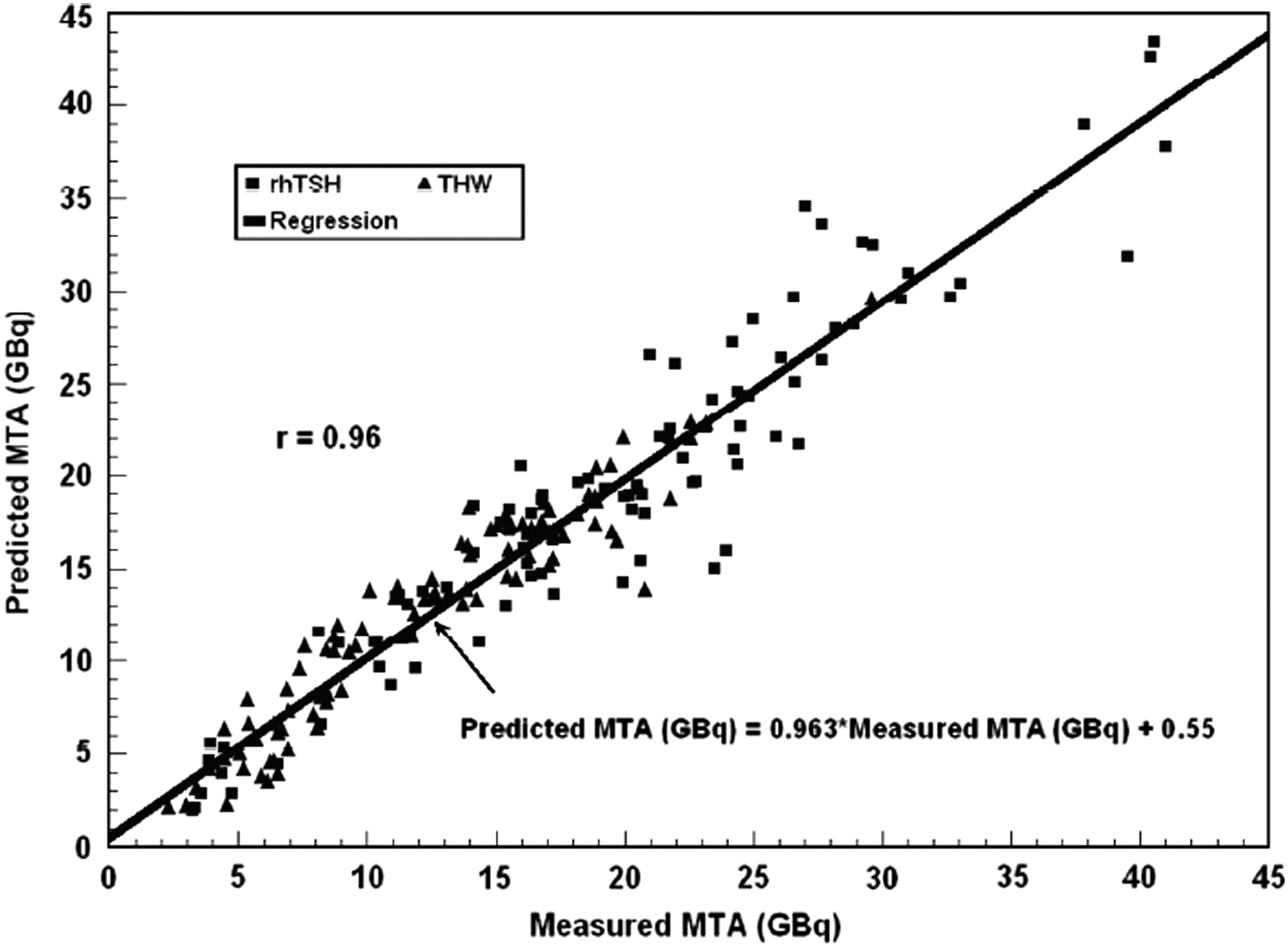
Linear correlation of predicted versus measured maximum tolerated activity (MTA; GBq).
MTA, maximum tolerated activity; THW, thyroid hormone withdrawal; rhTSH, recombinant human thyrotropin; N.S., not significant.
However, because some patients had multiple studies that might potentially bias the validation of the study, the analysis was repeated including only the first dosimetry for each patient. In this case, the linear correlation coefficient is only slightly smaller (0.92 vs. 0.96) in part due to the fewer samples used for the analysis, and the regression itself deviates only very slightly from that of the larger data set, as seen in Figure 2.
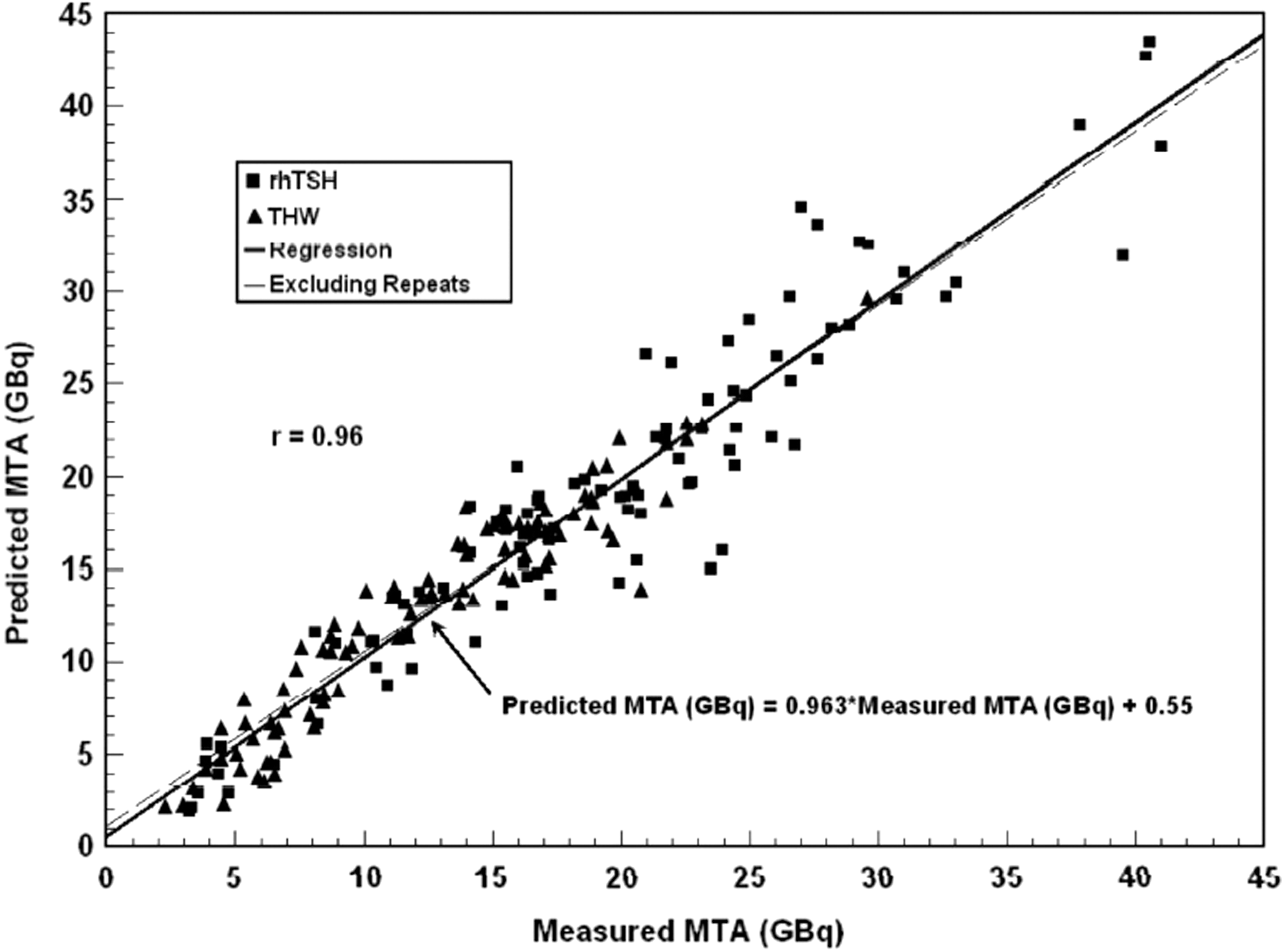
The solid line represents the analysis including repeat dosimetries performed in the same patient as demonstrated in Figure 1. The dashed line (difficult to see, but present) represents the dosimetric data for only the first dosimetry performed on each patient. The linear correlation coefficient is only slightly smaller (0.92 vs. 0.96), in part due to the fewer samples used for the analysis, and the regression itself deviates only very slightly from that of the larger data set.
Effect of method of patient preparation (THW or rhTSH)
The bi-exponential model was originally established using a large group (n = 142) of patients who had all been prepared by THW. However, at the present time in the authors' facility, rhTSH is being used more frequently than THW. Nevertheless, it would appear based on these results that the model is not dependent on the patient preparation mode. The same correlation factor was observed for each group when analyzed separately. The primary difference is the more rapid clearance when using rhTSH rather than THW as the mode of preparation, which is reflected in the average MTAm for each group: 12.6 GBq for THW and 19.2 GBq for rhTSH (p < 0.001).
Despite the strong correlation between the estimated values based on the simplified two-time point model and the observed values of the MTA, a fairly large dispersion in the two values is present. These deviations would result in an overestimation of a patient's MTA by >15% in approximately 1/10 therapies. This would be unacceptable in clinical practice, and thus a relatively conservative threshold needs to be applied to this model if it were to be used in place of a more comprehensive dosimetry. However, as the value of the MTAm becomes smaller (<9.25 GBq [250 mCi]) the agreement is not as good, resulting in an underestimation using the model (Fig. 3). Furthermore, although the model incorporates the patient's BSA, which substantially removes any sex dependence, this parameter itself is not correlated to the MTA.
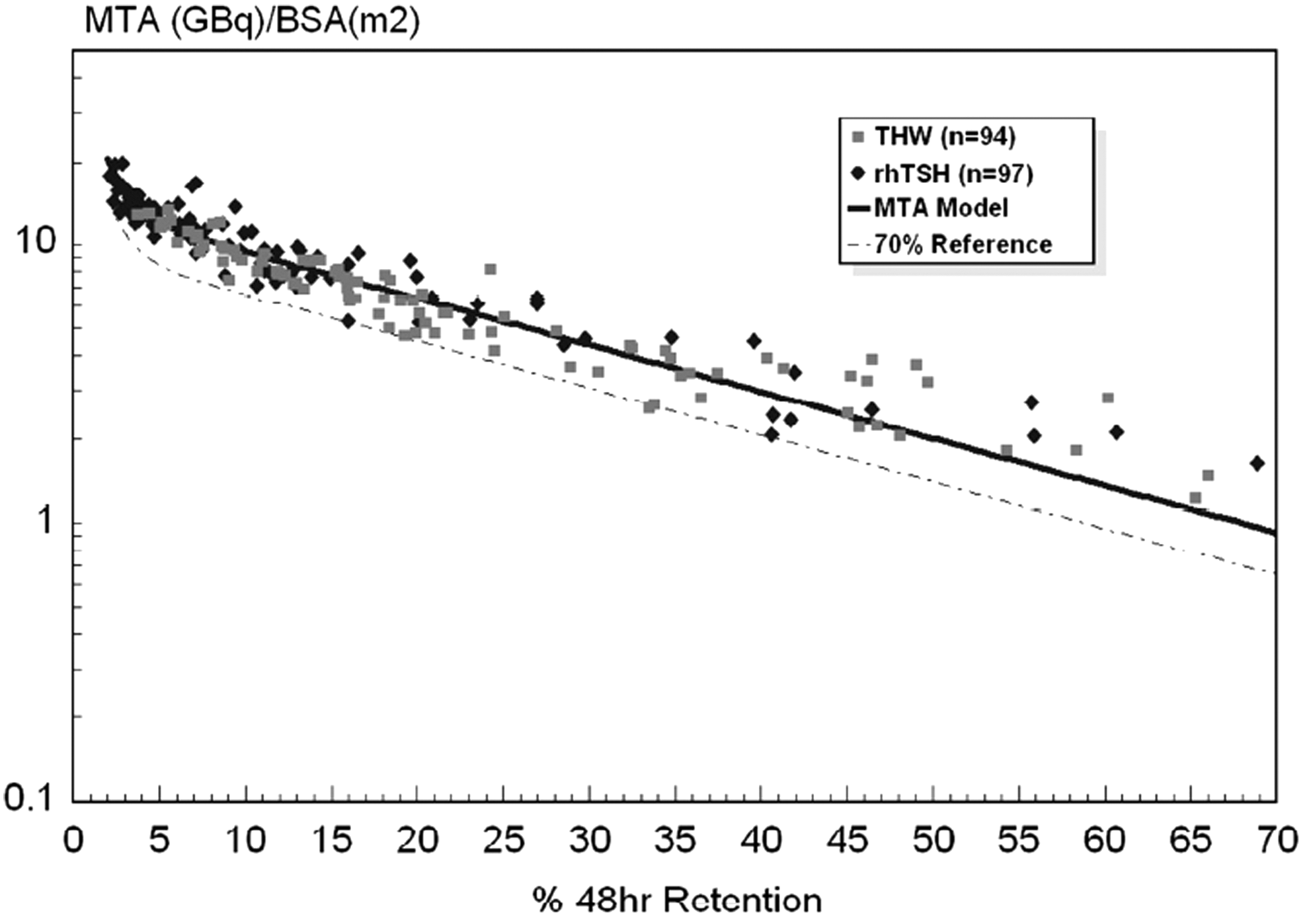
MTA normalized to body surface area (BSA) with 70% reference bound.
In evaluating the first dosimetry in patients with creatinine values of >1.0 mg/dL, which is the upper limit of the reference standard in the authors' facility, the correlation is shown in Figure 4 as r = 0.96, which is identical to the entire group shown in Figure 1.

Linear correlation of predicted versus measured MTA (GBq) in first dosimetry in patients with creatinine levels >1.0, which is the upper limit of the reference standard for creatinine at the authors' institution. The r-value was 0.96, which is identical to the entire group, as noted in Figure 1.
Discussion
External validation of any proposed prediction model is essential in order for that model to be used in clinical practice, and this study validates the previously reported % 48-hour WBR with a BF to estimate the MTA of 131I for the treatment of DTC. However, because of deviations of individual patient data from the model, the patient's MTA may be overestimated by >15% in approximately 1/10 therapies. Such errors would be unacceptable in clinical practice. Consequently, some fraction of the predicted MTA needs to be used for the treatment planning.
The limitations to the use of such a simplified model remain the same as discussed in the original study (5). To the authors' knowledge, this is the first study to validate an “alternative” simplified dosimetry for full patient-specific dosimetry. However, there are other reports evaluating potential excellent alternative methods. Thomas et al. (11) evaluated a first-order approximation of the hematopoietic radiation dose based solely on whole-body data. Hänscheid et al. (12) incorporated this approach into an analysis based on the MIRD formalism, which was recommended by the EANM Dosimetry Committee (13), and recently, Jentzen et al. (14) evaluated multiple potential parameters as “alternative” simplified dosimetry for full patient-specific dosimetry. Further work, as well as validations of these potential approaches, is encouraged.
In summary, this study validates the previously developed regression dosimetry model based on the % 48-hour WBR of 131I alone. This model (i) can help to identify those patients for whom the proposed empiric amount of 131I should be reduced so as not to exceed the MTA or may be increased to deliver more absorbed dose of radiation to the tumor, and (ii) may be used with patients prepared by either rhTSH or THW. Once again, it is demonstrated that the 70% threshold (Fig. 3) of the value generated using the bi-exponential model can be safely used as an upper limit for selecting the patient's therapy prescribed activity, and the % 48-hour WBR can also be used to verify that the absolute retention at 48 hours does not exceed 120 mCi (4.4 GBq) when the patient does not have lung metastases, or 80 mCi (3.0 GBq) at 48 hours if the patient has lung metastases. Since there were only a few patients with prolonged retention (>50%) used in forming the model, the agreement is not as good in that region, as seen in Figure 3.
Finally, the use of the % 48-hour WBR is not being advocated as a replacement for full patient-specific dosimetry when full patient-specific dosimetry is available or could be adopted. Rather, its use is proposed when a more comprehensive dosimetry is not feasible, in which case this approach and the information provided could be used to guide the therapist in selecting the 131I prescribed activity to be used to treat the patients with metastatic DTC.
Footnotes
Acknowledgments
This study was supported by grants from grateful patients.
Author Disclosure Statement
D.V.N. and L.W. are consultants with Genzyme. The other authors have nothing to declare.