
Abstract



Thursday, October 30, 2014
Autoimmunity Thursday Oral Clinical 9:00 AM
External eye muscles are often affected in Graves' orbitopathy (GO) and diplopia (double vision (DVis)) is the most common cause of sick-leave in GO. Still, studies of GO often focused on inflammation and only scored subjective DVis. We objectively quantitated DVis and studied relation to other GO characteristics.
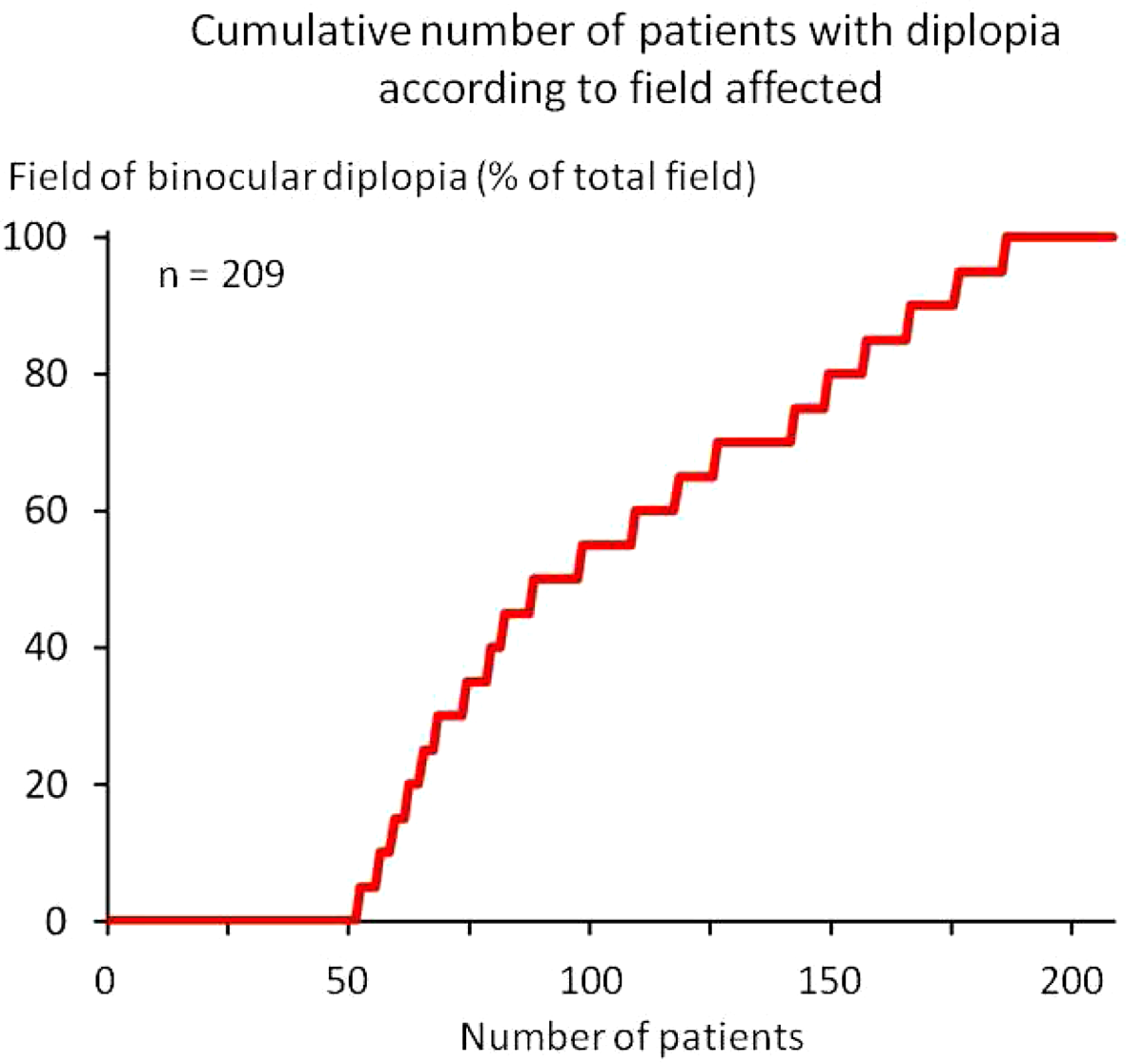
We prospectively measured binocular field of DVis during eye movement for fixation in a single center cohort of 215 patients with incident moderate to severe GO and correlated field of DVis with other characteristics. Fields of DVis and motility restriction were measured by grid based planimetry from charts and expressed in %.
6 monocular vision cases were excluded. 75.1% (157/209) had DVis ranging from 5% (DVis in 5% of gaze field) to 100% (DVis in the entire field)(median 70% in affected)(Fig 1). Patients with ≥50% DVis (n=121) were 54 yrs (mean), women 77.7%. This was similar in patients with DVis 5–45% or no DVis. DVis was the main indication for therapy in 53.5% of the 209 patients. DVis % correlated positively with eye motility reduction (Spearman's rho 0.26, p<0.001), and also with asymmetry of GO (rho 0.28, p<0.001). In contrast, correlation was negative with the commonly recorded GO manifestations inflammatory signs (rho−0.24, p<0.001) and proptosis (Hertel)(rho−0.36, p<0.001). No correlation was observed with type or duration or previous episodes of thyroid dysfunction, with time difference between debut of thyroid and eye disease, duration of GO, previous radioiodine therapy, position of eyelids, eye closure deficiency, eye ball tension, visual acuity, patient body weight, age, sex and smoking habits. Findings were consistent in multivariate models.
Double vision was the main indication for therapy in around half of patients with moderate to severe Graves' orbitopathy. Unexpectedly, double vision % correlated negatively with orbital inflammation and eye proptosis that are often the prime measures of clinical outcomes in trials of therapy. Standardized quantitative measurements of eye motility and double vision in GO should be part of clinical routine, and indispensable in controlled clinical trials of therapy.
Autoimmunity Thursday Oral Translational 9:15 AM
The TSH receptor (TSHR) structure contributes to TSAb generation in Graves' disease. by undergoing intramolecular cleavage into disulfide-linked A- and B-subunits with consequent A-subunit shedding. Hyperthyroidism is induced in mice by the isolated human TSHR A-subunit but not by a non-cleaving TSH holoreceptor. A puzzling phenomenon is that two A-subunit forms (residues 22–289) are secreted by transfected CHO cells; one recognized by Graves' TSAb (‘active’) the other (‘inactive’) by a mouse mAb 3BD10 generated to TSHR-289. TSAb and 3BD10 interaction with TSHR-289 is mutually exclusive. Understanding the structural difference between active and inactive A-subunits could provide insight into Graves' disease pathogenesis. The 3D structure of active TSHR residues 22–260 is known because this protein is in complex with a human monoclonal TSAb Fab (M22). However, the structural difference with inactive A-subunits is unknown.
We solved the 3D structure of 3BD10 by generating Fab from purified IgG and obtaining crystals for x-ray diffraction. We then docked 3BD10 to the active TSHR-260 monomeric structure using an in silico docking program (Z-dock), facilitated by prior knowledge of a portion of the 3BD10 epitope.
TSAb and 3BD10 binding to the TSHR A-subunit monomer excluded a conformational difference as the basis for the active-inactive dichotomy, suggesting, instead a role for A-subunit quaternary structure (multimerization). We determined the full structure of TSHR-289 by extending that of TSHR-260 by molecular modeling based on the FSH receptor structure. Indeed, in silico analysis provided evidence that a TSHR-289 trimer was bound by TSAb M22 but not 3BD10, whereas a TSHR-289 dimer was bound by 3BD10 and not by M22. The validity of these models (higher intrinsic energy in the trimer vs the dimer) is supported by experimental data of temperature sensitive irreversible conversion from active to inactive forms.
We provide evidence that this difference between active and inactive TSHR A-subunits resides in the degree of A-subunit multimerization (trimer versus dimer). The importance of these findings is that affinity maturation of TSAb in Graves' disease is likely to involve a trimer of the shed TSHR A-subunit.
Autoimmunity Thursday Oral Translational 9:30 AM
A critical barrier to studying the pathogenesis of and potential novel therapies in Graves' disease is that thyroid stimulating antibodies (TSAb) only develop in humans. TSAb can be induced transiently in mice by vectors expressing the human TSHR or its A-subunit. However, the instability of these antibodies, as well as the confounding effect of the immunization protocol, limits the value of transient Graves' disease models and no spontaneous animal model is available. NOD-H2h4 mice spontaneously develop thyroiditis and antibodies to thyroglobulin (TgAb) and thyroid peroxidase but, unfortunately, NOT to the TSHR. We previously generated transgenic BALB/c mice that express the human (h)TSHR A-subunit in the thyroid that do not spontaneously develop thyroid autoantibodies. However, we hypothesized that transferring the hTSHR transgene to the NOD-H2h4 mice would generate mice that spontaneously develop TSHR antibodies (Ab.
We backcrossed hTSHR transgenics on to the NOD-H2h4 background, thus far at the 6th backcross (N6) on the way to generating fully congenic animals (N10). We examined TSHR transgenic backcrosses (N1-N6) at age 24 weeks for TSHR antibodies by ELISA (non-pathogenic) and clinically relevant TSH binding inhibition (TBI) and TSAb, as well as serum T4 and thyroid histology.
As expected, all animals (NOD-H2h4 controls and TSHR/NOD-H2h4 transgenics) developed TgAb. However, from the N3 to N6 back-crosses, only the TSHR transgenics developed TSHRAb on ELISA (10/30 mice). Remarkably, pathogenic TSHRAb developed in female TSHR transgenics; 7/23 with elevated TBI and 3/9 with TSAb activity. High TSH levels interfered with these assays in males. Due to concurrent thyroiditis and decreased thyroid reserve, hTSHR/NOD-H2h4 mice were euthyroid. However, this is not a problem because it is reversing or preventing TSAb generation that is the essential requirement for a future cure of Graves' disease.
The development of the first animal model that spontaneously develops pathogenic TSHR antibodies represents a significant advance that will provide insight into the pathogenesis of Graves' disease and facilitate investigation of potential approaches for specific immunotherapy for its cure, rather than its treatment.
Thyroid & Development Thursday Oral Basic 9:45 AM
The decision steps in human thyroid cell speciation remain incompletely characterized. We have shown that overexpression of the regulatory transcription factors pax8 and nkx2-1 (ttf-1) directs murine embryonic stem (mES) cells to differentiate into thyroid follicular cells. Such cells subsequently organized into three-dimensional follicular structures in the presence of extracellular matrix. In the present experiments we have studied human embryonic stem (hES) cells (line H9) with the aim of producing functional human thyroid cell lines.
We used pEZ-lentiviral vectors to express human PAX8-GFP and NKX2-1-mcherry in hES cells followed by induction of differentiation into thyroid cells directed by activin A and TSH.
Both these transcription factors were expressed efficiently in hES cells expressing either PAX8 or NKX2-1 alone or in combination. Thyroid specific genes including thyroglobulin, thyroid peroxidase, sodium/iodide symporter (NIS) and the TSH receptor were activated in the double transfected cells as assessed by RT-PCR and immunostaining. Since transcriptional regulation was important in provoking thyroid cell differentiation we also assessed the haematopoietically expressed homeobox gene HEX, which is regulated directly by PAX8 itself. HEX was markedly under expressed in hES cells compared to normal human thyroid but was induced in double positive cells while the calcium-dependent transcription repressor Downstream Regulatory Element Antagonist Modulator (DREAM) was suppressed as the cells differentiated. This suggested that one mechanism for the success of the PAX8/NKX2-1 transfection approach was via the induction of HEX and suppression of DREAM in undifferentiated ES cells.
These data indicated that overexpression of PAX8 and NKX2-1 in hES cells induced thyroid cell differentiation and that additional transcriptional regulation by factors such as DREAM and HEX are likely to be critical in human thyroid cell speciation.
Thyroid Cancer Thursday Oral Basic 1:50 PM
KRASG12D can cause lung cancer rapidly, but is not sufficient to induce thyroid cancer. It is not clear whether long-term serum thyroid stimulating hormone (TSH) stimulation can promote KRASG12D mediated thyroid follicular cell transformation. In the present study, we investigated the effect of long-term TSH stimulation in KRASG12D transgenic mice and the role of Sprouty1 (SPRY1) in KRASG12D mediated signaling.
We used TPO-KRASG12D mice with thyroid specific expression of KRASG12D under the control of thyroid peroxidase (TPO) promoter. Twenty TPO-KRASG12D mice were given anti-thyroid drug propylthiouracil (PTU, 0.1% w/v) in drinking water to induce serum TSH and 20 mice were without PTU treatment. Equal number of wild-type littermates (TPO-KRASWT) was given the same treatment. The expression of SPRY1, a negative regulator of receptor tyrosine kinase (RTK) signaling, was analyzed in both KRASG12D-and BRAFV600E-induced thyroid cancers.
Without PTU treatment, only mild thyroid enlargement and hyperplasia were observed in TPO-KRASG12D mice. With PTU treatment, significant thyroid enlargement and hyperplasia occurred in both TPO-KRASG12D and TPO-KRASWT littermates. Thyroids from TPO-KRASG12D mice were 6 times larger than TPO-KRASWT littermates. Distinct thyroid histology was found between TPO-KRASG12D and TPO-KRASWT mice: thyroid from TPO-KRASG12D mice showed hyperplasia with well-maintained follicular architecture whereas in TPO-KRASWT mice this structure was replaced by papillary hyperplasia. Among 10 TPO-KRASG12D mice monitored for 14 months, two developed follicular thyroid cancer (FTC), one with pulmonary metastasis. Differential SPRY1 expression was demonstrated: increased in FTC and reduced in papillary thyroid cancer (PTC). The increased SPRY1 expression in FTC promoted TSH-RAS signaling through PI3K/AKT pathway whereas down-regulation of SPRY1 by BRAFV600E in PTC resulted in both MAPK and PI3K/AKT activation.
Chronic TSH stimulation can induce KRASG12D mediated oncogenesis, leading to FTC. SPRY1 may function as a cellular switch to control MAPK signaling and its down-regulation by BRAFV600E favors PTC development.
Thyroid Cancer Thursday Oral Basic 2:05 PM
Cancer gender disparity has been observed for a variety of human malignancies. Thyroid cancer is one such cancer with a higher incidence in women, but more aggressive disease in men. There is scant evidence on the role of sex hormones on cancer initiation/progression. We evaluated the effect of sex hormones on thyroid cancer using Thrb-PV/PV transgenic mice, a model that mimics human follicular thyroid cancer (FTC) development.
Sham surgery or castration was performed on 6-week-old Thrb-PV/PV mice. When the mice reached 8–9 months old, their hormone and thyroid cancer status were examined. The mechanisms of how sex hormones mediate their effect on thyroid cancer progression were examined using genomic analysis and validated by q-RT-PCR, immunohistochemistry, in vivo hormonal status reconstitution, and in vitro functional assays.
Castration led to lower rates of cancer in female mice and less advanced cancer in males. Mechanistically, the less advanced cancer in castrated males was due to increased expression of tumor suppressor (Glipr1, Sfrp1) and immunoregulatory genes, and higher tumor infiltration with M1 macrophages and CD8 positive cells. Exogenous testosterone reconstitution in castrated male mice reversed the differences in FTC progression and the molecular and cellular changes observed with castration. In human FTC samples, we found reduced expression of GLIPR1 and SFRP1 compared to normal thyroid tissue, demonstrating the relevance of the mouse model to human FTC. Furthermore, our in vitro functional studies showed that knockdown of GLIPR1 in human cells increased cellular proliferation and colony formation, and deceased CCL5 secretion, a chemokine known to have a role in attraction and activation of immune cells.
Sex hormones play an important role in the development and progression of follicular thyroid cancer. The effect of male sex hormone on cancer progression is through regulating the expression of tumor-suppressor genes and modulating tumor immunity.
Thyroid Cancer Thursday Oral Basic 2:20 PM
Telomerase reverse transcriptase (TERT) plays an important role in human tumorigenesis. Two activating TERT promoter mutations chr5:1,295,228C>T and chr5:1,295,250C>T have been recently identified in thyroid cancer, which, in association with BRAF V600E mutation, have been found to cooperatively define the worst aggressiveness of thyroid cancer. The present study was to explore the molecular mechanisms underlying this corporative role of the TERT and BRAF mutations observed clinically.
Using genetic, molecular and cellular experimental tools to investigate the interplay between TERT promoter and BRAF V600E mutations in their impacts on the function of TERT gene and thyroid cancer cell behaviors.
Luciferase reporter assay showed that the transcriptional activity of the mutated TERT promoter was several folds higher than that of the wild-type TERT promoter in thyroid cancer cells. Induced expression of BRAF V600E further enhanced the activities of mutated TERT promoter but not the wild-type TERT promoter. shRNA knockdown of BRAF V600E, causing the suppression of the MAP kinase pathway, resulted in profound inhibition of the mutated TERT promoter, but not the wild-type TERT promoter. Treatment with the MEK inhibitor AZD6244 dramatically decreased TERT expression in thyroid cancer cells harboring TERT promoter mutation, but not in cells harboring the wild-type TERT, although AZD6244 could inhibit the MAP kinase pathway in all the cells. Moreover, shRNA knockdown of either TERT or BRAF inhibited the proliferation and migration of thyroid cancer cells. This inhibition was even more pronounced with dual knockdown of TERT and BRAF than the knockdown of either alone. Several other TERT promoter and cellular properties were also affected by the TERT and BRAF mutations in a cooperative manner.
BRAF V600E promotes TERT expression in a TERT promoter mutation-dependent manner, which explains the corporative role of the TERT promoter and BRAF V600E mutations in aggressive cellular and tumor behaviors of thyroid cancer, providing a novel molecular mechanism in thyroid tumorigenesis. Further effort in dissecting this mechanism is currently ongoing in our lab and more results are expected.
Iodine Uptake & Metabolism Thursday Oral Basic 2:35 PM
The tumor-homing property of mesenchymal stem cells (MSCs) allows targeted delivery of therapeutic genes into the tumor microenvironment. The sodium iodide symporter (NIS) as theranostic gene allows non-invasive imaging of MSC biodistribution as well as potent therapeutic application of radioiodine. The chemokine RANTES/CCL5 is secreted by MSCs in the course of tumor stroma recruitment and differentiation into cancer associated fibroblasts. We have previously shown that linking NIS expression to induction of the chemokine RANTES allows a more focused expression within primary tumors but it was not clear if it would also be effective in controlling growth of metastatic disease. In this study we wanted to investigate the tumor recruitment and therapeutic potential of MSCs transfected with NIS under control of the RANTES promoter in a liver metastasis mouse model of colon cancer.
We stably transfected human MSCs with NIS driven by the RANTES promoter (RANTES-NIS-MSC). To establish liver metastasis of colon cancer the human colon cancer cell line LS174t was injected into the spleen resulting in liver metastasis after 2 weeks. We investigated distribution and recruitment of RANTES-NIS-MSCs by 123I-scintigraphy, 124I-PET-imaging and ex vivo analyses before the evaluation of the therapeutic potential for NIS-based 131I therapy.
After establishment of liver metastasis of colon cancer, RANTES-NIS-MSCs were systemically injected and MSC distribution was analyzed by γ-camera and PET-imaging. Injection of 123I or 124I resulted in a tumor-selective radioiodine accumulation showing active MSC recruitment and tumor-specific promoter activation. These findings were confirmed by ex vivo γ-counter analysis, immunohistochemistry and real-time PCR. Administration of a therapeutic dose of 131I in RANTES-NIS-MSC-treated mice resulted in a significant delay in tumor growth and improved overall survival.
Our results demonstrate selective recruitment of RANTES-NIS-MSCs into liver metastases of colon cancer and promotor activation allowing tumor-specific radioiodine accumulation. This novel gene therapy approach opens the prospect of NIS-mediated radionuclide therapy of metastatic cancer after MSC-mediated gene delivery.
Thyroid Cancer Thursday Oral Basic 2:50 PM
Increased p21-activated kinase (PAK) signaling and expression was identified in the invasive fronts of aggressive papillary thyroid cancers (PTC), including those with RET/PTC, BRAF V600E, and mutant RAS expression. Functionally, in vitro thyroid cancer cell motility is dependent on Group 1 PAKs, particularly PAK1. PAK1 is a known oncogene in breast cancer, which regulates cell motility and proliferation via kinase and scaffolding functions. It also potentiates both Akt and MAPK signaling through these two mechanisms. In the present study, we hypothesize that BRAF regulates thyroid cancer cell motility in part through PAK activation.
Cell Culture, Migration Assay, Immunofluorescence and Confocal Microscopy, Immunoprecipitation, Immunohistochemical Staining, Statistical Analysis.
Using three well-characterized human thyroid cancer cell lines (BCPAP, FTC133 and TPC1), we demonstrated in all cell lines that BRAF knockdown reduced PAK phosphorylation of direct downstream targets while, unexpectedly, PAK suppression did not affect ERK activation. In contrast, MEK inhibition achieved either pharmacologically or using siRNAs did not reduce PAK activity, demonstrating that PAK activity is dependent on BRAF but independent of MEK. Concordantly, inhibition of cell migration through BRAF loss was rescued by overexpression of either constitutively active (CA) MEK1 or PAK1, demonstrating that both effectors are involved in BRAF-regulated thyroid cancer cell motility. To further characterize BRAF-PAK signaling, immunofluorescence and immunoprecipitation experiments were performed using cells transfected with WT BRAF and PAK1 or using thyroid cancer cells that express both proteins endogenously. In both conditions, PAK1 and BRAF co-localize and co-immunoprecipitate. Moreover, the interaction of the endogenous proteins was enhanced in mitosis. Finally, we demonstrated that acute induction of BRAFV600E expression in vitro in PCCL3 thyroid cells, and in vivo in murine thyroid glands, results in increased PAK activity.
In conclusion, we have identified a previously unrecognized signaling pathway in thyroid cancer cells in which BRAF activates and physically interacts with the oncogene PAK1 and regulates cell motility.
Thyroid Cancer Thursday Oral Basic 3:05 PM
Undifferentiated or anaplastic carcinomas arising from preexisting PTCs have a high prevalence of BRAF mutations and commonly have inactivation of p53. BRAFV600E-induced PTCs regress upon genetic inhibition of oncogene expression, consistent with dependence on the oncoprotein for viability. However, it is unknown if advanced thyroid cancers harboring additional alterations retain this dependency.
We created mice with thyroid-specific deletion of p53 and dox-dependent expression of BrafV600E (TPO-Cre/p53flox/flox/LSL-rtTA_GFP/tetO-BrafV600E). Mice were followed by MRI, and expression arrays performed to identify pathways mediating tumor progression and reoccurrence.
Nine weeks after dox treatment ∼50% of the quadruple transgenic mice died from large ATCs, primarily due to tracheal invasion/compression. Expression profiles of Braf-induced ATC were enriched for genes involved in cell migration, mitotic cell cycle, blood vessel development and TGFβ signaling. When dox was discontinued for 3 weeks, the thyroid masses showed a dramatic reduction in tumor volume in all mice studied. Histology of the residual lesions revealed debris, inflammatory cells and fibrosis, and small nests of tumor cells that retained a differentiated appearance. Mice with documented tumor regression were followed in the absence of dox for up to 52 weeks (n=44). 22/44 (50%) recurred, with the time to relapse being shorter in mice with larger tumors prior to dox withdrawal. 3/11 recurrent tumors showed re-expression of the BrafV600E transgene, which was not associated with acquired mutations in the reverse tetracycline transactivator transgene (rtTA). We generated a MAPK transcriptional output score (Pratilas C PNAS 2009) for each sample: Primary ATC and all relapsed tumors had a 3–18 fold higher MAPK output compared to normal thyroid. Exomic sequencing of Braf, Craf, Nras, Hras, Kras, Mek1, Mek2 identified an Hras-Q61K mutation in 1/8 relapses. The molecular basis of MAPK reactivation in the remaining recurrent ATCs is unknown.
Primary ATCs driven by Braf are dependent on the oncoprotein. However, cancers that recur largely do so in a Braf-independent manner, through mechanisms that converge to reactivate the MAPK pathway.
Thyroid Cancer Thursday Oral Clinical 1:50 PM
In the absence of prospective trials of initial treatments for patients with differentiated thyroid cancer (DTC), debate remains as to appropriate extent of surgery, post-operative radioiodine (RAI), and TSH-suppressive thyroid hormone therapy (THST). The National Thyroid Cancer Treatment Cooperative Study Group (NTCTCSG) presents updated analyses of multi-institution prospectively collected data related to clinical outcomes following initial treatment in patients with DTC.
We examined effects of initial therapies (thyroidectomy, RAI) and long-term THST in 4,941 patients treated per local standard of care (6 yrs median follow-up; 34,631 person-yrs of documented follow-up time). Overall and disease-free survival (OS, DFS) were assessed by univariate and multivariate analyses. NTCTCSG staging system was applied.
Improved OS was noted in stage III patients who received RAI (risk ratio [RR] 0.66, p=0.04) and in stage IV patients who received both total/near-total thyroidectomy (T/NTT) and RAI (RR 0.66 and 0.70, combined p=0.049). Moderate (TSH maintained subnormal-normal) but not aggressive (TSH maintained undetectable- subnormal) THST was associated with significantly improved OS in all stages (RR in stage I 0.13, stage II 0.09, stage III 0.13, IV 0.33) and DFS in all stages (RR in stage I 0.52, stage II 0.40, stage III 0.18). Only moderate THST was associated with significantly improved OS when distant metastatic disease was diagnosed during long-term follow-up. Both lower initial disease stage and moderate THST were independently predictive of improved OS. Further, moderate THST was independently predictive of improved DFS for at least the first 3 years of follow-up in patients rendered disease free after initial therapy.
We confirm previous findings that T/NTT followed by RAI is associated with survival benefit in high risk but not low risk patients. In contrast with our earlier reports, only moderate THST is associated with better outcomes in all stages (including low-risk stage I patients), and aggressive THST may not be warranted even in patients diagnosed with distant metastatic disease during follow up. Moderate THST continued at least 3 years after diagnosis may be indicated in higher risk patients.
Autoimmunity Thursday Oral Clinical 2:05 PM
Perturbation of signaling pathways regulating immunity by endogenous or exogenous stimuli has been increasingly recognized to induce a painless thyroiditis syndrome characterized by transient thyrotoxicosis and hypothyroidism. Herein, we report on the occurrence of such a syndrome in a subgroup of patients receiving immunotherapy with program death 1 (PD-1) receptor monoclonal antibodies for the treatment of metastatic malignancies.
Ten patients with documented metastatic malignancies (7 malignant melanoma, 3 non-small cell lung cancer) who received immunotherapy with PD-1 receptor antibodies as part of a clinical trial were noted to have abnormal thyroid function tests after reporting symptoms compatible with thyroid dysfunction. They were referred to a tertiary Thyroidology Clinic for diagnostic confirmation and management.
In this cohort, the mean patient age was 55 years and 60% were female. Transient thyrotoxicosis was observed in 6 (60%) patients and required only temporary beta-blocker therapy, and thyrotropin binding inhibitory immunoglobulins (TBII) were uniformly negative, whereas anti-thyroid antibodies (anti-thyroglobulin and anti-thyroid peroxidase) were documented in 4 (67%) patients. Thyrotoxicosis resolved spontaneously in all patients after approximately 4 weeks, and was followed by hypothyroidism requiring thyroid hormone replacement with levothyroxine. A hypothyroid presentation, without a previously documented thyrotoxic phase, was observed in the remaining 4 (40%) patients, showed serological evidence of anti-thyroid antibodies, and was identified 6–8 weeks after initial drug exposure. The occurrence of this painless thyroiditis syndrome had no consistent relationship with the patients' oncological response to immunotherapy.
Immunotherapy with PD-1 receptor antibodies for metastatic malignancies can induce a painless thyroiditis syndrome in a subset of susceptible patients. Given the increasing application of immunotherapy for the treatment of a variety of malignancies, clinicians should monitor such patients for clinical and biochemical signs of thyroid dysfunction.
Thyroid Cancer Thursday Oral Clinical 2:20 PM
The DECISION trial established that sorafenib prolonged progression-free survival (PFS) compared to placebo in patients with progressive RAI-rDTC (Lancet 2014). Here we sought to identify prognostic and predictive factors correlated with treatment outcomes.
Multivariate Cox proportional hazards models adjusted for treatment effect and subgroup analyses defined by maximum target lesion size and existence of disease-related symptoms were used to explore the relationship between clinical baseline variables and PFS. Patients were deemed symptomatic at entry if they had symptoms/findings consistent with thyroid cancer reported in the medical history or pre-treatment adverse event dataset.
A total of 417 patients were randomized to receive placebo (n=210) or sorafenib (n=207). Multivariate Cox model analyses indicated that lower maximum individual target lesion size, lower number of lesions, thyroglobulin levels at baseline less than the median (486 ng/ml) and region Asia versus Europe and North America were prognostic for longer PFS in placebo patients and in all patients when adjusted for treatment. Subgroup analyses indicated that patients whose maximum individual target tumor size were <1.5 cm had longer PFS and appeared to have less benefit from sorafenib treatment than patients with lesions ≥1.5 cm. Lesions ≥1.5 cm as well as lung metastases were predictive for better treatment effect with sorafenib. Both symptomatic and asymptomatic patients at entry had improved PFS following treatment with sorafenib.
Maximum tumor size, number of lesions, thyroglobulin levels at baseline and geographic regions were prognostic for longer PFS in RAI-rDTC patients. Individual tumor size ≥1.5 cm and lung-only metastases were predictive for better treatment effect with sorafenib. Patients appeared to benefit from sorafenib treatment irrespective of disease-related symptoms at baseline. Thus, based on these post hoc exploratory analyses, patients with progressive RAI-rDTC and maximum tumor size <1.5 cm appear to have a good prognosis and may be candidates for “watch and wait” before initiating sorafenib.
Table - Exploratory subgroup analyses
Thyroid Cancer Thursday Oral Clinical 2:35 PM
Although some studies have reported that preoperative vitamin D deficiency (VDD) is a risk factor for hypocalcemia after TT in patients with nontoxic multinodular goiter or Graves' disease, the association between VDD and postoperative hypocalcemia in thyroid cancer patients undergoing total thyroidectomy (TT) plus central compartment neck dissection (CCND) remains unclear. We evaluated whether preoperative VDD was associated with postoperative symptomatic hypocalcemia.
Data were collected prospectively between September 2012 and May 2013. A total of 267 consecutive thyroid cancer patients underwent TT with CCND were analysed regarding the association between preoperative VDD and postoperative hypocalcemia. Patients were divided into two groups according to preoperative vitamin D levels: group 1 for VDD, <10 ng/ml and group 2 for Non-VDD, ≥10 ng/ml. Symptomatic hypocalcemia was defined as serum calcium <8.2 mg/dL along with the presence of any symptoms or signs of hypocalcemia. The rate of postoperative symptomatic hypocalcemia and clinicopathological features were compared between two groups.
The rate of postoperative symptomatic hypocalcemia in VDD group were higher in VDD group than in non-VDD group (43.8% vs. 30.4%, p=0.043). With logistic regression analysis, predictive factors for postoperative symptomatic hypocalcemia included a preoperative vitamin D level less than 10 ng/ml (P=0.007; odds ratio=3.00). In case of postoperative intact parathyroid hormone (iPTH) levels less than 15 pg/ml, symptomatic hypocalcemia was more prominent in VDD group than Non-VDD group. (77.5% vs. 53.2%, P value=0.008). In determining an appropriate vitamin D threshold level minimizing symptomatic hypocalcemia, preoperative vitamin D levels more than 20 ng/ml reduced the risk of symptomatic hypocalcemia by 72% as compared with vitamin d deficiency (P=0.003).
VDD is significantly associated with postoperative symptomatic hypocalcemia in thyroid cancer patients undergoing TT plus CCND. VDD could predict symptomatic hypocalcemia in cases of postoperative serum iPTH levels less than 15 pg/ml.
Thyroid Cancer Thursday Oral 2:50 PM
Papillary thyroid carcinoma (PTC) is associated with excellent overall prognosis. Standard treatment consists of surgical resection with the possible addition of radioactive iodine (RAI) for tumors believed to have a higher risk of recurrence. The actual benefit of RAI is still debated, though, especially for microcarcinomas. In this study, we examine the effect of RAI on PTC mortality, particularly as it relates to tumor size.
The National Cancer Database (NCDB) was queried from 1998 to 2011, identifying 284,635 patients with PTC. Tumors were classified into four size groups: 10 mm or less (microcarcinoma), 11–20 mm, 21–40 mm, and >40 mm maximum diameter. The use of RAI was then analyzed and Kaplan-Meier curves were created for each group, comparing no RAI versus RAI. Cox regression was used to quantify the effect of RAI, correcting for clinicopathologic, demographic, and socioeconomic variables.
RAI was utilized in 47% of PTC cases, with higher percentages for larger tumors: 29% of ≤10 mm tumors vs. 58% for >40 mm (p<0.001). With a mean follow-up of 7 years, RAI was associated with a survival benefit in all size categories, even after correcting for age, gender, tumor grade, operation received, TNM stage, insurance status, hormone suppression, and presence of positive margins, positive lymph nodes, and distant metastases. The benefit of RAI for each tumor size category was as follows: HR for ≤10 mm: 0.73 (95% CI 0.61–0.87, p<0.001); HR for 11–20 mm: 0.82 (95% CI 0.68–0.99, p=0.04); HR for 21–40 mm: 0.63 (95% CI 0.52–0.78, p<0.001); HR for >40 mm: 0.62 (95% CI 0.47–0.81, p=0.001).
The use of RAI showed a small but statistically significant survival benefit for all PTC tumor size categories, even after correcting for disease severity, demographic factors, and extent of operation.
Thyroid Cancer Thursday Oral Clinical 3:05 PM
MTC is a rare form of thyroid cancer accounting for 5% of all thyroid cancers. Survival outcomes are influenced by numerous factors, including stage at presentation and the ability to resect all disease. The aim of our study was to design a predictive nomogram for cancer specific mortality (CSM) utilising clinical, pathological and biochemical variables in patients with MTC.
249 MTC patients managed entirely at Memorial Sloan-Kettering Cancer Center between 1986–2010 were identified. Patient, tumor and treatment characteristics were recorded from patient charts. Variables predictive of CSM were identified by univariable analyses. A multivariable competing risk model was then built to predict the 10-year cumulative incidence of medullary thyroid cancer. All predictors of interest were added in the starting full model before selection, including age, gender, pre- and post- operative serum calcitonin, pre- and post- operative CEA, RET mutation, perivascular invasion, margin status, M status, pathologic N status and pathologic T status. Stepdown method was used in model selection to choose predictive variables.
Of 249 MTC patients, 22.5% (56/249) died from MTC, while 6.4% (16/249) died secondary to other causes. Mean follow-up period was 87 +/− 67 months. The 7 variables with the highest predictive accuracy included age, gender, postoperative calcitonin, perivascular invasion, pathologic T status, pathologic N status and M status. These variables were used to create the final nomogram (Figure 1). Discrimination from the final nomogram was measured at 0.77 with appropriate calibration.
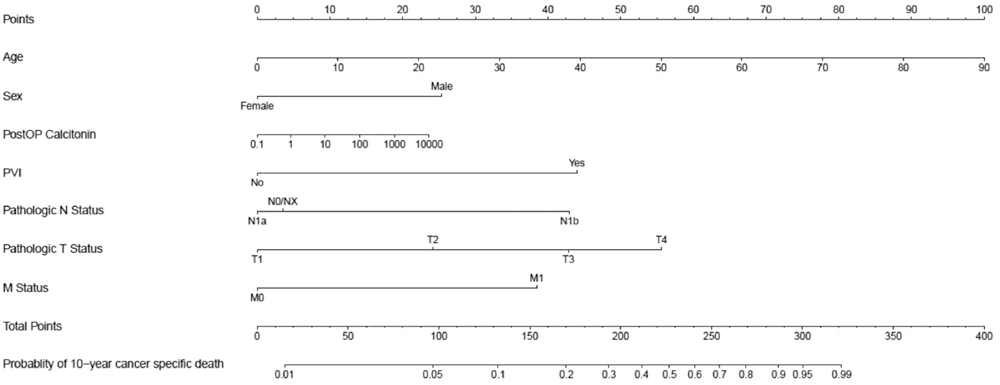
Nomogram of medullary thyroid cancer.
We describe the first nomogram which estimates cause-specific mortality in individual patients with MTC. This predictive nomogram will help patient counseling in terms of prognosis and in subsequent clinical follow up.
Autoimmunity Thursday Poster Basic
We have previously shown that a (TC)n microsatellite in intron 5 of the FOXP3 gene was associated with a variant of the autoimmune polyglandular syndrome type 3 (APS3v), that is defined as the co-occurrence of type 1 diabetes (T1D) and autoimmune thyroiditis (AITD) in the same individual. Allele 10, containing 25 repeats of the microsatellite (long repeats), is preferentially transmitted to offspring with APS3v, while allele 2, containing 14 repeats of the microsatellite (short repeats), is protective (Villano et al JCEM 2009; 94: 1458). We hypothesized that the long repeats of the intron 5 microsatellite decreased FOXP3 splicing and function, thereby reducing regulatory T cell activity and promoting the development of APS3v.
We cloned genomic DNA fragments containing the long and short repeats of the FOXP3 intron 5 microsatellite and transfected them into HEK 293 cells to perform direct splicing analysis.
We identified a novel splice variant of FOXP3 lacking exon 6, and showed that it is expressed in human thymus, lymph node and T regulatory cells. However, the length of the repeats in the microsatellite did not significantly influence the level of mRNA expression of this new FOXP3 splice variant in vitro.
Further studies are needed to examine whether variation in the expression of this FOXP3 splice variant may alter the function and quantity of regulatory T cells, leading to the development of autoimmunity.
Autoimmunity Thursday Poster Clinical
Although low serum vitamin D levels have been association with several autoimmune diseases, their association with thyroid autoimmunity is still conflict. Our study aimed to evaluate the vitamin D status in autoimmune thyroid disease and its affecting factors involved in the disease.
Our cross-sectional study included 66 patients with autoimmune thyroid disease (34 Hashimoto disease and 32 Graves disease) and 52 healthy controls. Serum 25(OH)D3, calcium, PTH, FT3, FT4, TSH, TPOAb and TgAb were measured in all subjects.
In AITD patients, mean serum 25(OH)D3 levels were significantly lower than that in healthy controls (14.8±6.1 ng/ml vs. 17.64±5.6 ng/ml, P<0.01). The prevalence of vitamin D insufficiency, defined as serum 25(OH)D3<20 ng/ml, was 81.7% in AITD subjects and 71.1% in controls. In AITD patients, when divided by TPOAb titer (0–60 IU/ml, 61–500 IU/ml, 501–1300 IU/ml and>1300 IU/ml), only patients with TPOAb>1300 IU/ml showed a significantly lower serum 25(OH)D3 levels compared to controls. The PTH and calcium level in AITD patients was higher than controls. We also found that the level of 25(OH)D3 in those who had less outdoor exercise is lower than who do outdoor exercise often. People with mental labour also showed lower 25(OH)D3 than those with manual labour outdoor. However, there was no association between the levels of 25(OH)D3 and FT3, FT4, as well as TSH.
Vitamin D insufficiency is a common problem in Chinese even in healthy people. Low vitamin D levels were associated with higher titer TPOAb in AITD patients, which suggest that vitamin D insufficiency might be associated with the occurrence of AITD.
Autoimmunity Thursday Poster Clinical
Vitamin D has been pointed out as an important immune response regulator. Studies have shown a relationship between vitamin D insufficiency and the presence of autoimmune diseases such as Hashimoto's Thyroiditis (HT). It's possible that the autoimmune process in HT is inhibited in its different stages by vitamin D on its active form. Our aims were to study the prevalence of vitamin D insufficiency and relationship of the serum concentrations with thyroid volume, function and autoimmunity markers in HT.
Blood samples were collected from 54 patients with HT and 54 healthy individuals without a diagnosis of HT, aged 18 to 75 years. We conducted serum 25OH vitamin D, TSH, free T4, calcium, phosphorus, PTH, TPOAb, TgAb and TRAb. Thyroid volume was estimated by ultrasound. Data on weight, height, body mass index and time since diagnosis were collected. Patients and control subjects were matched by sex, age, weight and body mass index. The significance level for statistical analysis was 5%.
Prevalence of vitamin D insufficiency was found in 63,2% of patients and in 36,8% of subjects in the control group (p=0.04). In the group of patients, lower levels of vitamin D were associated with higher concentration of TSH (p=0.017) and greater thyroid volume (p=0.021). Goiter and vitamin D insufficiency were present in 41.7% of patients. There was a positive correlation between TPOAb and volume in patients (p=0.008). There was no correlation between vitamin D concentration and TRAb, TgAb or free T4 (Table 1).
Table 1
Hormonal evaluation indicated higher levels of TSH in patients with HT showing insufficiency of vitamin D. Low concentrations of vitamin D are also associated with a greater thyroid volume in patients. These correlations did not occur in the control group. In conclusion, low concentration of vitamin D is involved in the pathophysiology of HT.
Autoimmunity Thursday Poster Clinical
Autoimmune thyroid diseases, particularly thyroiditis, may initially show symptoms of hyper or hypothyroidism, but they usually evolve in a rather short span toward a steady hypothyroidism or euthyroidism.
N/A
We present a case of a patient that over a period of 5 years went through at least 3 episode of hyperthyroidism, preceded or followed by severe hypothyroidism, with the eventual recovery to euthyroidism. The patient, a 39 year-old female of Chinese origin, was first see en consultation during a pregnancy for a follow-up of a hypothyroidism already treated with 0.05 mg of Synthroid. She was clinically euthyroid and thyroid function tests were normal, but she had a previous history of at least documented episodes of hyperthyroidism followed by the hypothyroidism for which she was treated. Five months later she had a normal delivery. Thereafter she stopped spontaneously the thyroid medication and 3 months later she was clinically hypothyroid with a TSH at 96.2 mUi/L (N=0.35–3.5) and FT4 at 4.2 pmol/L (N=11–22). However, by the time she was seen again in our clinic she had completely recovered and the TFT suggested a subclinical hyperthyroidism (FT4=24, TSH=0.14), but 6 months later TFT were normal. 6 months later the TFT were and remained normal for the following 6 months when another episodes of hyperthyroidism reoccurred (FT4=34; TSH=0.03). it was followed 1 month later by a marked hypothyroidism (TSH=60.9; FT4=5.5) with partial recovery (FT$=10.6; TSH=11.3) in the next 2 months, but evolving toward hypothyroidism during the last visit 9TSH=21.5; FT4=8.1)for which thyroid replacement was restarted. During all these episodes the patient had minimal or no symptoms of thyroid dysfunction, anti TPO antibodies were always negative, as well the anti TSH receptor antibodies done during the episodes of hyperthyroidism. A 131I thyroid scan performed during one of the episodes of hyperthyroidism, showed an uptake of 41% and a diffuse goiter with a pyramidal lobe, while a thyroid ultrasound displayed a very heterogeneous gland.
The whole clinical picture is consistent with an autoimmune thyroiditis with a very particular and infrequent evolution.
Thyroid Cancer Thursday Poster
Papillary thyroid cancer can metastasize to ovarian tissue, or can develop in a struma ovarii. Radioiodine uptake in the ovary has also been reported in mature teratoma containing thyroid tissue. We report here a case of ovarian radioiodine uptake in a mature teratoma containing no thyroid tissue.
N/A
Case : A 31 year old woman was referred for a 3 cm palpable left thyroid nodule. She was euthyroid and presented no local symptoms. Her first fine needle aspiration showed a follicular lesion with atypia of unknown significance (FLUS). It was repeated 3 months later with the same findings. She was referred for surgery. She had a left hemi-thyroidectomy, and on pathology, a 2,6 cm follicular variant of a papillary carcinoma was found, with lymph-vascular invasion but no extra-thyroid extension. She had a completion of thyroidectomy and a papillary microcarcinoma of 3 mm was found in her right lobe. On her diagnostic scan before radio ablation, a significant uptake was noticed on her left ovary. Pelvic ultrasound confirmed a solid, hyperechoic mass of 1,5×1,5×1,7 cm containing hyperechoic points suggestive of calcifications. A cystic lesion was also found on her right ovary of 7,5×6,8×7,3 cm. She underwent laparoscopic resection of both masses, and her left ovarian mass showed a mature teratoma, but neither thyroid tissue nor cancer was found.
Although this finding is surprising, given the evident and significant uptake of the left ovary, thyroid tissue is not always present in such teratomas. It may vary between 7–18%. Therefore the uptake could depend from tissues present in these cysts that may be able to retain iodine.
Autoimmunity Thursday Poster Translational
The clinical utility of the functional serum thyroid stimulating (TSAb) and blocking (TBAb) autoantibodies was prospectively evaluated in patients with thyroid-associated orbitopathy (TAO).
At an academic joint thyroid-eye clinic, complete ophthalmic, endocrine and serological investigations were performed in 101 consecutive patients with active and severe TAO. Serum TSAb and TBAb levels were measured with two bioassays using a chimeric TSH receptor and a CRE-dependent luciferase. TSAb results are expressed as percentage of specimen-to-reference ratio (SRR%). Blocking activity is defined as percent inhibition of luciferase expression relative to induction with bovine TSH alone.
Median age was 52 years (range 23–75 years, 76 female, 53 current smokers). Graves' disease (GD) and Hashimoto's thyroiditis were present in 97 (96%) and four (4%) patients, respectively. Median duration of TAO was 11 months. Diplopia was present in 63 patients with 12 having constant double vision. Chemosis, corneal lesions and asymmetric TAO were present in 27, 14 and 20 patients, respectively. Median clinical activity (CAS) and severity (CSS) scores were 4 (range 3–6) and 5.75 (1–11), respectively. Upper or lower lid retraction was present in 52 or 42 patients. Median palpebral aperture and proptosis were 12 mm (6–17) and 22 mm (13–30). All 101 patients with TAO were TBAb negative. In contrast, 91(90%) were TSAb positive of whom 90 had GD. Four, two, one and three TSAb negative patients had thyroidectomy, radioactive iodine (seven and 10 years before), antithyroid drug treatment, and Hashimoto's thyroiditis, respectively. TSAb correlated with the diplopia score (p=0.016), upper lid retraction (p=0.006), thyroid binding inhibiting immunoglobulin (TBII, p<0.001) and negatively with the duration of TAO (p=0.002). Median serum values of TSAb and TBII were SRR% 418 (28–795) and 7.35 IU/L (0.3–174), respectively. Daily cigarette consumption or pack years had no significant impact on CAS, CSS, intraocular pressure or TSAb and TBII.
TSAb, not TBAb, are widely present in TAO and mirror clinical severity.
Disorders of Thyroid Function Thursday Poster Basic
Exposure of the thyroid to radiation during radiotherapy of the head and neck is often unavoidable. The present study aimed to investigate the protective effect of α-lipoic acid (ALA) on radiation-induced thyroid injury in rats.
Rats were randomly assigned to four groups: healthy controls (CTL), irradiated (RT), received ALA before irradiation (ALA+RT), and received ALA only (ALA, 100 mg/kg, i.p.). ALA was treated at 24 h and 30 minutes prior to irradiation. The neck area including the thyroid gland was evenly irradiated with 2 Gy per minute (total dose of 18 Gy).
Greater numbers of abnormal and unusually small follicles in the irradiated thyroid tissues were observed compared to the controls and the ALA group on days 4 and 7 after irradiation. However, all pathologies were decreased by ALA pretreatment. The quantity of small follicles in the irradiated rats was greater on day 7 than day 4 after irradiation. However, in the ALA-treated irradiated rats, the numbers of small and medium follicles were significantly decreased to a similar degree as in the control and ALA-only groups. The PAS-positive density of the colloid in RT group was decreased significantly compared with all other groups and reversed by ALA pretreatment. The high activity index in the irradiated rats was lowered by ALA treatment. TGF-β1 immunoreactivity was enhanced in irradiated rats and was more severe on the day 7 after radiation exposure than on day 4. Expression of TGF-β1 was reduced in the thyroid that had undergone ALA pretreatment. Levels of serum pro-inflammatory cytokines (TNF-α, IL-1β and IL-6) did not differ significantly between the all groups.
This study provides that pretreatment with ALA decreased the severity of radiation-induced thyroid injury by reducing inflammation and fibrotic infiltration and lowering the activity index. Thus, ALA could be used to ameliorate radiation-induced thyroid injury.
Disorders of Thyroid Function Thursday Poster Clinical
Recent studies showed that exposure to methimazole (MMI) during the first trimester of pregnancy increased the incidence of specific congenital anomalies called MMI embryopathy. However, for Graves' disease (GD) patients who are treated with MMI and cannot tolerate PTU because of adverse effects, treatment for hyperthyroidism during the first trimester of pregnancy becomes a problem. We investigated whether switching from MMI to iodine in the first trimester would result in a lower incidence of major congenital anomalies than continued treatment with MMI alone. Another major outcome of interest was the incidence of neonatal thyroid dysfunction.
We reviewed the cases of 260 women with GD whose treatment was switched from MMI to inorganic iodide in the first trimester (iodine group) and for comparison reviewed the cases of 1134 patients treated with MMI alone (MMI group). The subjects of the analysis of major congenital anomalies and neonatal thyroid dysfunction were live-born infants.
The incidence of major anomalies was 4/260 (1.53%) in the iodine group and was significantly lower than the incidence of 47/1134 (4.14%) in the MMI group. Two neonates in the iodine group had MMI embryopathy (0.8%), as opposed to 18 neonates in the MMI group (1.6%). One neonate whose mother had been exposed to iodine alone had an FT4 level of 0.97 ng/dl and TSH level of 11.99 mU/L. The neonate's thyroid function improved without any medication, and no goiter was detected. Severe neonatal hypothyroidism (FT4<0.9 ng/dl) were all detected from neonates who were exposed to ATDs in the third trimester.
Switching from MMI to iodine to control hyperthyroidism in GD patients during the first trimester is a good option to minimize the risk of congenital abnormalities, especially the risk of MMI embryopathy.
Disorders of Thyroid Function Thursday Poster Clinical
Although both free T4 (fT4) and TSH are traditionally measured to diagnose and monitor the treatment of thyroid disease, ATA/AACE Guidelines recommend treating patients for primary hypothyroidism when TSH exceeds 10 mIU/L independent of the fT4 concentration. We reviewed fT4 and TSH values in patients with and without diagnosed thyroid disease to determine the relationship between an abnormal fT4 and an abnormal TSH.
The Intermountain Healthcare IRB approved this retrospective study of 235,377 specimens from 108,624 outpatients ages 1–104, of whom 52% had and 48% did not have a prior diagnosis of thyroid disease. FT4 and TSH were measured by Abbott Architect immunoassay with external controls performed daily. Clinical data, including patient, age, gender, and thyroid diagnosis were obtained by query of the Intermountain Enterprise Electronic Data Warehouse. Data were analyzed by plotting the % of fT4<0.71 ng/ml or >1.85 ng/ml versus a simultaneously measured TSH concentration.
When TSH was within the reference range, abnormal fT4 values occurred in less than 1% of patients. When TSH exceeded 5.0 mIU/L, 90.5% of outpatients with no history of thyroid disease and 87.3% of outpatients with thyroid disease had normal fT4 concentrations. When TSH was less than 0.45 mIU/L, 93.4% of outpatients with no history of thyroid disease and 91.2% of outpatients with thyroid disease had normal fT4 concentrations. (Figure 1).
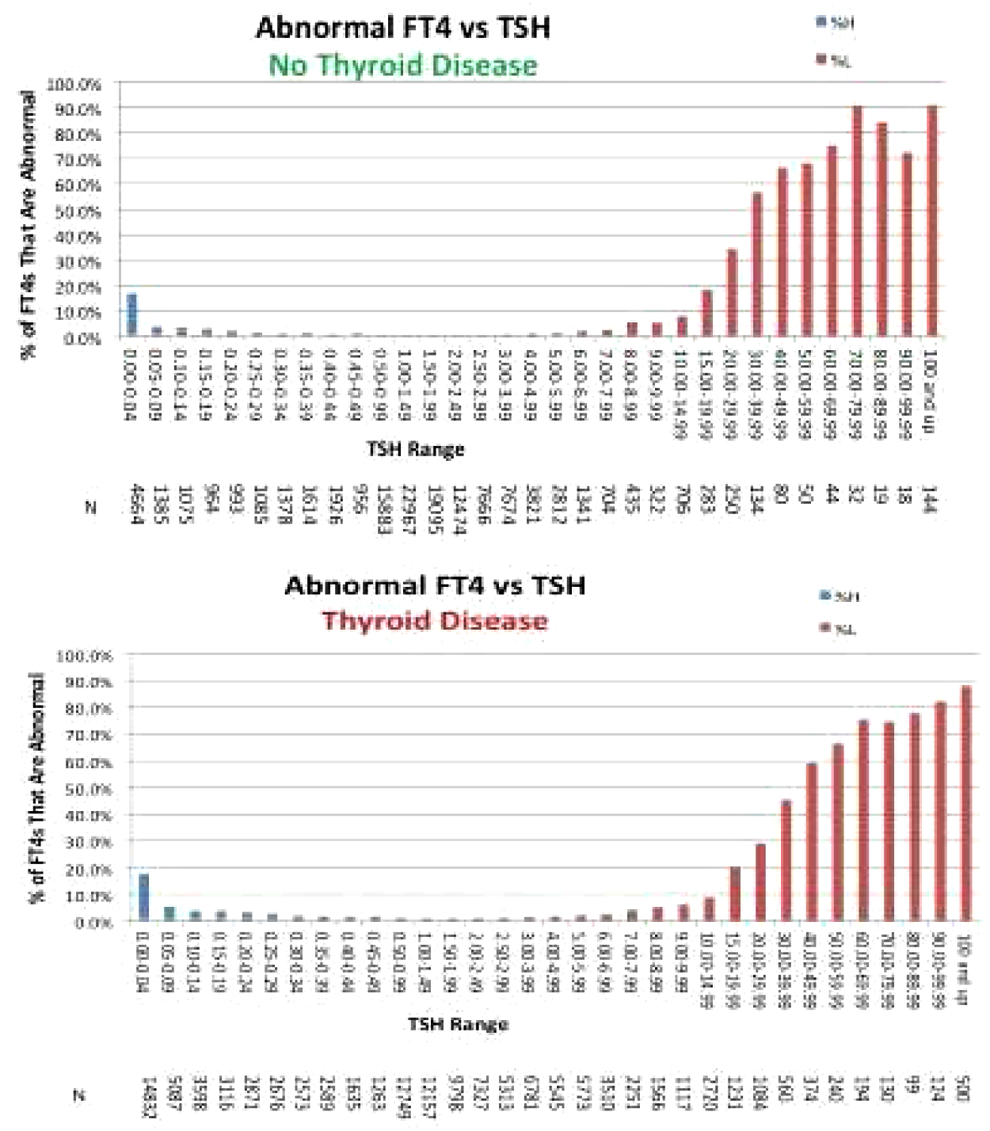
Free T4 versus TSH in patients with and without a prior diagnosis of thyroid disease.
In patients with normal, elevated or depressed TSH levels, fT4 values are rarely outside the reference range. In patients with or without a history of thyroid disease, the likelihood of finding an abnormal fT4 concentration when TSH>5 mIU/L is less than 12%, and the likelihood of finding an abnormal fT4 concentration when TSH<0.45 mIU/L is less than 8%. The findings show that measuring fT4 is not likely to provide significant clinical information and should not be routinely performed.
Disorders of Thyroid Function Thursday Poster Clinical
Graves' disease (GD) patients suffer from impaired Quality of Life (QoL). Clinical profile of GD patients referred for surgery and radioiodine (RAI) therapy is generally different. The aim of the current study was to investigate if difference in clinical profile changes QoL perception in GD patients referred for surgery and RAI therapy.
Prospective study (January 2013 to May 2014) consisting of 72 GD patients referred for definitive therapy after failed medical management. Patients were divided in two groups: Gr. 1- Referred for surgery (n=25), Gr. 2- Referred for RAI therapy (n=47). Patients filled ThyPROhin questionnaire (validated translated version of ThyPROus) before and 6 months after definite therapy. ThyPROhin questionnaire consists of 12 domains (85 items) which evaluate thyroid specific QoL in patients with benign thyroid disorders. The best score for each domain is 0 and worst 100. Clinical profile and QoL scores between groups were compared by non-parametric tests.
Mean age (37 vs 36 years, p=.96), gender distribution (M:F=1:2.6 vs 1:2.1, p=.79), smoker status (p=.49), education levels (p=.86) and serum TSH (1.5 vs 0.7 mU/L, p=.07) were comparable in two groups. Duration of symptoms (39 vs 18 months, p=.003), incidence of ophthalmopathy (44 vs 19%, p=.049) and compressive symptoms (24 vs 3% p=.01) were significantly higher in Gr. 1. Active eye disease was noted only in 3 patients of Gr. 1. Estimated thyroid weight was less and more than 50 gms in Gr. 1 and 2 respectively. QoL scores were impaired in both groups but the differences were not significant (Table 1). Available follow up (Gr. 1=4, Gr. 2=5 patients) showed significant recovery 6 months after therapy.
QoL Scores in Two Groups
Despite different clinical profiles GD patients referred for Surgery and RAI therapy have comparable impairment in QoL.
Disorders of Thyroid Function Thursday Poster Clinical
Metabolic syndrome (MS) is associated with an increased risk of developing cardiovascular disease and Type 2 diabetes. Thyroid dysfunction is also a known cardiovascular risk factor, mediated at least in part by its effect on lipid metabolism and blood pressure. In obese patients, serum TSH tends to be higher than in lean controls.
The objective of this study was to assess the associations between serum TSH levels and MS as well as individual components of MS. This was a cross-sectional observational study of obese and overweight patients seen for initial evaluation at the Boston Medical Center Weight Management Clinic from February 2013-February 2014. MS was defined as 1. Waist circumference ≥40 in (men) or 35 in (women) 2. Serum triglycerides ≥150 mg/dL or drug treatment for elevated triglycerides 3. Serum HDL<40 mg/dL in men or <50 mg/dL in women or drug treatment for low HDL-C 4. Blood pressure ≥130/85 mm Hg or antihypertensive treatment 5. Fasting plasma glucose ≥100 mg/dL or drug treatment for elevated blood glucose or history of diabetes or elevated HbA1c≥5.7%. Multivariate regression analysis was used to determine associations between serum TSH levels and prevalence of MS and its individual components.
A total of 3447 patients without known thyroid dysfunction were identified from electronic medical records. 75.6% were female and 38% were African-American. Mean age was 46.74 years (SD±15.11) and mean BMI was 38.32 (±9.04). Among 1005 patients without any missing data, prevalence of MS was 71.84%. In patients with MS, the median serum TSH was 1.405 μIU/mL compared to 1.36 μIU/mL in patients without MS (P value- 0.45). In multivariable models, after adjustment for age, sex, race, education, socioeconomic status and smoking, there was no significant association between serum TSH level and presence of MS. There were also no significant associations between serum TSH level and individual components of the MS.
Serum TSH level does not appear to be a potentially modifiable risk factor for MS in obese and overweight subjects.
Disorders of Thyroid Function Thursday Poster Clinical
Traditionally, thyroxine (L-T4) is worldwide suitable in tablets form but novel formulations in soft gel capsule or liquid formulation are now available. L-T4 is usually taken with water in the morning before breakfast, as the absorption is maximal when administered on an empty stomach. Recent studies showed that oral liquid L-T4 could remove the problem of levothyroxine malabsorption by coffee and food observed with traditional tablets formulations. We show the preliminary data of the TICO study, aimed to assess if thyroid hormonal profile (TSH, fT4 and fT3) of patients treated with liquid levothyroxine is modified by food intake.
Double-blind, randomized controlled clinical study, designed to enrolled 80–100 hypothyroid patients, aged from 18 to 75 years old, who have to start L-T4 replacement therapy. At recruitment all patients will be treated with liquid L-T4 (Tirosint® fiala monouso, IBSA Farmaceutici Italia) at the dosage of 1.6 mcg/Kg. To all the patients will be given two identical and indistinguishable vials (labeled A and B) containing in a single dose the oral solution and placebo; one is to be assumed half an hour before breakfast and the other one during the usual breakfast. After 40 days of treatment all the patients will be submitted to TSH, fT4 and fT3 evaluation to ensure achieve euthyroidism. In this case all the patients have to switch the order of vials assumption. After 40 days TSH, fT4 and fT3 assay will be performed again.
At this time 44 patients (36/8 female/male, mean age 48.8±5.7 years old) completed the study. The mean dose of LT4 was 64.71±30.17 mcg/day. No difference of serum TSH (2.32±1.64 vs. 2.94±2.10 mlU/L, p=0.129), fT4 (10.51±1.29 vs. 10.60±1.32 pg/mL, p=0.774) and fT3 (2.70±0.34 vs. 2.72±0.35 pg/mL, p=0.774) were observed before and after the switching of vials assumption.
Our preliminary data show no difference in thyroid hormonal profile of patients assuming liquid levothyroxine before and during breakfast. If these data will be confirmed, liquid L-T4 formulation could improve the compliance of hypothyroid patients who have to start a L-T4 replacement therapy. Finally, the oral solution l-T4 could be suitable for patients who cannot swallow the solid formulations.
Disorders of Thyroid Function Thursday Poster Clinical
Intravenous levothyroxine (IV T4) provides a rapid repletion of thyroid stores and is often used in endocrinologic emergencies such as myxedema coma. The efficacy and safety of IV T4 for other clinical conditions is uncertain. Given the cost differential, hormone repletion rates, bioavailability and half-life, a retrospective study was conducted to evaluate the usage of IV T4.
A survey was sent to the Division of Endocrinology and University Health Consortium to establish compelling indications for IV T4 in addition to the FDA indication (myxedema coma). These included: NPO greater than 3 days, cardiogenic shock, and suspected thyroid malabsorption. Hospital in-patients receiving IV T4 were retrospectively evaluated over 6 months. Patients were assessed for presence of compelling indications for IV T4, appropriate dose reduction from oral T4, and duration of IV T4. A safety analysis was conducted to describe adverse events to IV T4 at higher risk from rapid supplementation (geriatrics, history of congestive heart failure, atrial fibrillation, or coronary artery disease). A cost analysis was performed to evaluate patients without compelling indications to IV T4.
76 patients were evaluated in the study period (Table 1). Among these, there were diagnoses of 5 (6%) cases of myxedema,3 (4%) suspected T4 malabsorption, and 2 (2.5%) cardiogenic shock. Of patients without compelling indications, 49 (79%) patients had PO access while receiving IV T4. Of patients receiving IV T4, 22% were not converted correctly from their oral form. In addition, 13.5% developed atrial fibrillation and 14% developed troponin elevations while on IV T4.
Intravenous Levothyroxine Analysis (N=76)
Evaluation of necessity for IV T4 administration revealed that use of IV T4 was often unwarranted. Further analyses projected that implementation of an order set including standardized laboratory requests and conversions of T4 dosage forms coupled with clinical decision support aimed at limiting use of IV T4 to compelling indications could result in drug acquisition cost avoidance totaling $68,000 per year in our hospital. A post intervention analysis is to follow.
Disorders of Thyroid Function Thursday Poster Clinical
Few studies have investigated thyroid disease and primary hyperparathyroidism in patients undergoing thyroid or parathyroid surgery. Awareness of these conditions prior to surgery will alter surgical planning and clinical outcomes. Herein, we examined in our experience the incidence of concomitant thyroid nodular and primary hyperparathyroidism in patients who have undergone parathyroidectomy or thyroidectomy.
This is a retrospective study of prospectively collected database for one endocrine surgeon in a single institution. after screening preoperatively for concomitant thyroid nodular disease and primary hyperparathyroidism.
279 patients underwent thyroidectomy, parathyroidectomy, or both.141 patients were primarily referred for surgical management of thyroid disease. Of these patients, Twenty three patients (16.3%) underwent both thyroidectomy and parathyroidectomy. Forty-two of the 297 patients were referred primarily for surgical management of hyperparathyroidism, 6 of whom underwent thyroidectomy and parathyroidectomy (14.2%). Controlling for age, the likelihood of having both final diagnoses, is higher compared single disease [OR: 4.726, 95%CI: (1.839, 12.15), p=0.0013]. Controlling for age, the likelihood of having both thyroid and parathyroid surgeries is higher compared to single surgery: [OR: 12.34, 95%CI: (2.496, 60.995), p=0.0021].
Routine implementation of comprehensive neck ultrasound, serum levels of PTH, and calcium levels in the preoperative workup for every patient referred for surgical management of thyroid nodules may increase the detection rate of concomitant hyperparathyroidism., and vice versa. Such implementations may assist in better surgical planning and outcomes.
Withdrawn
Withdrawn
Thyroid & Development Thursday Poster Clinical
Several studies have shown that identification of the RLN with aid of intraoperative neuromonitoring (IONM) has decreased rates of RLN palsy; however, unexpected RLN palsy still occurs, even though the visual integrity was assured. The aim of this study is to evaluate the tractional injuries of RLN using a swine model via continuous IONM and the traction power which can cause loss of signal (LOS).
Thirteen living orally intubated pigs underwent tractional injury to the RLNs. During stretching of the RLN, continuous IONM were performed. Follow-up examinations were carried out for 7 days using continuous IONM, and then fresh swine RLNs were harvested. All nerves were stretched to failure at a rate of 1 cm/min (strain rate of 0.5%/s). Load deformation and stress-strain curves were determined.
The mean structural diameter of RLN was 1.5 mm (range 1.2–2.0 mm) and the average intraoperative tractional force at the time of LOS in continuous IONM was 4 N (range 2–6 N). At postoperative day 7, we observed normal electromyography of RLNs using continuous IONM in all swine. After harvesting of RLNs, stress-strain curves were determined. Traction injury of swine RLNs with power of 2.83 MPa can cause LOS. In stress-strain curves by ex vivo study using swine RLNs, the mean physiologic limit strain and tensile strength of the swine RLNs were found to be 15.0% and 4.9 MPa. And the mean ultimate strain and tensile strength of the swine RLNs were found to be 21.5% and 6.6 MPa. And, histological analysis by scanning electron microscopy showed no abnormal structural findings in all nerves.
Traction injury of swine RLNs with power of 2.83 MPa can cause LOS and reversible traction injury might not induce the structural damage of the RLNs.
Thyroid Cancer Thursday Poster Basic
In this study, we compared the gene expression of PTMC which showed lateral neck node metastasis at initial diagnosis with PTMC without node metastasis and validated the functional evidences of over- or under expressed genes which correlated with early extensive lymph node metastasis.
We performed the oligonucleotide microarray analysis with 8 PTMCs and paired normal thyroid tissues using Illumina HumanHT-12 v4.0 Expression Beadchip. Of these, three were PTMC without cervical lymph node metastases (N0 PTMC), and others were PTMC with lateral neck node metastasis (N1b PTMC) at initial diagnosis. Statistical significance of the differentially expressed genes (DEGs) was determined using independent T-test with two-sided P<0.05 and median fold change cut off >1.5. The quantitative real-time PCR, Western blotting and immunohistochemistry were used to confirm the microarray data.
In microarray analysis, 131 genes whose expression differed significantly between two groups. 107 genes showed significant up-regulation and 24 genes showed down-regulation in N1b PTMC when compared with N0. Genes which are related with the epithelial-to-mesenchymal transition and stem cell marker was significantly up regulated in N1b PTMCs. The quantitative real-time PCR of including IL1RL1, ALDH1A3, FGFBP1, TM4SF1, PROM1, CAV1, CCL18, TGIF1, SMAD3 and CDCP1 confirmed the data of microarrays. In Western blotting, the expression of CAV1, TM4SF1 and IL1RL1 were increased in N1b PTMC than N0 PTMC. In regarding immunohistochemistry, ALDH1A3 and CAV1 were more frequently expressed in N1b than N0 PTMCs.
Genes that play a role in epithelial mesenchymal transition and thyroid cancer stemness are up-regulated in early extensive lymphatic spread of PTMC.
Thyroid Cancer Thursday Poster Basic
Autophagy is implicated in cancer cells response to metabolic stress. In medullary thyroid cancer (MTC) cells Nelfinavir induced metabolic stress and inhibited cell growth. We studied whether autophagy was involved in the MTC cells response to NFV.
TT and MZ-CRC-1 MTC cell lines with C634W or M918TRET mutations were exposed to NFV alone (0–20 μM) or in combinations with inhibitors of autophagy (Chloroquine [10 μM] and Wortmannin [0.1 μM]) or activator of autophagy Rapamycin (10 nM). Expression of autophagy-related genes (Beclin-1, atg 5, 7, 12, LC3A/B, p62) and apoptotic markers (caspase-3, PARP) was determined by Western Blot. Cell viability and cell death were evaluated by Vi-Cell and by propidium iodine (PI) staining, respectively.
NFV had no significant effects on Beclin1, atg 5, 7 and 12 expression, but induced expression of the lipidated form of LC3B. NFV also led to degradation of sequestrosome 1 (p62), therefore, indicating the activation of autophagy in MTC cells. CQ did not induce apoptosis alone but increased the cytotoxic effects of NFV in both MTC cell lines. NFV (10 μM) decreased TT and MZ-CRC-1 cell viability by 46% and 10%, respectively, as a single agent, and by 92% and 78% in combination with CQ. CQ-NFV induced apoptosis at 48 hours and lead to massive MTC cell death at 72 hours. Inhibitor of early autophagy (Wortmannin) sensitized cells to NFV. Treatment with NFV (5 μM) alone was not sufficient for induction of caspase-3 cleavage in MTC cells, but induced apoptosis in combination with Wortmannin. Pre-treatment with activator of autophagy (Rapamycin) did not potentiate the pro-apoptotic effects of NFV in MTC cells.
Pharmacological inhibitors of autophagy increase cytotoxicity of NFV in MTC-derived cell lines. Thus, inhibition of autophagy may be a promising therapeutic option for improving the anti-tumor effect of NFV in MTC patients.
Thyroid Cancer Thursday Poster Basic
Notch1 signaling guides stem cell fate and behaves contextually as a tumor suppressor. Yet, Notch3 has been less explored. Here, we assess Notch3's role in thyroid cancer migration, differentiation, and explore Notch3 activating agents' therapeutic utility.
FTC236 cells were transfected with a Tet-responsive transcriptional activator and a NOTCH3 response element (FTC236-NOTCH3) or an empty vector. A CBF-1-luciferase reporter measured functional Notch signaling. Cell migration was measured using a scratch assay. Notch3 and downstream target levels were assessed with quantitative real-time polymerase chain reaction and Western analysis in TPC1, BCPAP, FTC236, HTh7, 8505c, TT, and MZ thyroid cancer lines and in Nthy-Ori normal thyroid line. We identified and tested Notch3 activating agents, SAHA, VPA and the structural analog of SAHA, AB3 on cell growth using an MTT assay.
All thyroid cancer lines had minimal Notch3 levels compared to Nthy-Ori. Doxycycline treated FTC-NOTCH3 cells dose dependently induced NOTCH3, increased CBF-1 binding activity, activated downstream Hes1, Hes6, Hey1, Hey2 (p<0.0001), reduced gap migration (p<0.0001), and increased levels of sodium symporter gene (p=0.002), thyroid stimulating hormone receptor (p=0.0001), and thyroid transcription factor 1 (p=0.002) and 2 (p=0.08), suggesting that Notch3 may induce redifferentation. No effect was seen in the empty vector line. A screen for Notch3 activation revealed that AB3 among a library of SAHA analogs increased Notch3 mRNA the highest (p<0.0001). While VPA, SAHA and AB3 activated Notch3 in all thyroid cancer cell lines, AB3 caused the highest degree of Notch3 induction. Notably, AB3 achieved the lowest IC50 compared to that of SAHA (p<0.05), and VPA (p<0.00001) in all thyroid cancer cell lines.
Notch3 may be a tumor suppressor in thyroid cancer given its absence compared to normal thyroid. Notch3 restoration reduces cell migration and induces functional signaling and thyroid redifferentiation, suggesting it may potentiate radioiodine or t3/t4 therapy. SAHA, VPA and AB3 activate Notch3 and inhibit thyroid cancer cell growth. Moreover, AB3 may be more efficacious given its higher potency and ability to activate Notch3 to a higher degree.
Thyroid Cancer Thursday Poster Basic
When operating in the vicinity of vital nerves using energized surgical devices, care must be taken to avoid injury both from heat transfer and the passage of electrical current. Ultrasonic blades, which pass no current, have been shown to produce less electrophysiological damage than monopolar electrosurgery both acutely and subacutely when used at a distance of 1–4 mm from the sciatic nerve, and, in fact, are similar in effect to cold scalpel. This study was undertaken to determine whether ultrasonic shears are also less likely to produce nerve injury than electrosurgery.
Muscle incisions were made at a distance of 2 mm from the sciatic nerve in rat using the ultrasonic shears, Harmonic ACE+ and Harmonic FOCUS, monopolar electrosurgery (MES), and cold steel scissors. Sciatic nerve conduction was assessed acutely via electrophysiological monitoring of the compound action potential, conduction velocity and peripheral sensory function by von Frey hair probing of the hind paw. Histological examination was used to evaluate inflammation (via H&E) and impaired axonal transport (via β-APP).
MES displayed greater variability in the compound action potential, longer depolarization and repolarization times, slower conduction velocity, higher von Frey hair stimulation force, and more β-APP infiltration than the ultrasonic devices and scissors. There were no statistically significant differences between the ultrasonic devices and scissors for any of these responses.
Overall, MES showed greater negative effects on nerve electrophysiology than cold scissors, and ultrasonic devices were not significantly different from scissors for any of the responses. The more variable compound action potential observed for MES, along with longer polarization times, may indicate that nerve injury is occurring via inhibition of Na/K-ATPase pumps, and/or voltage-gated Na and K channels. This study confirms that when operating near nerves, ultrasonic devices are less likely to cause electrophysiological damage than electrosurgery, and implies that passage of electrical current is a more important factor than thermal effects.

Repolarization times of the compound action potential for the 3 hr period post-surgery with each of the devices.
Thyroid Cancer Thursday Poster Basic
As the morbidity of thyroid carcinoma has recently increased, new investigations into potential molecular and prognostic markers have been conducted to help facilitate diagnosis and better predict disease prognosis. Laminin-5 (332), a major component of the extracellular matrix, is an important autocrine factor produced by cancer cells to promote tumorigenesis. We aimed to investigate the relationship between laminin-5 expression in papillary thyroid carcinoma and lymph node metastasis.
Forty patients with papillary thyroid carcinoma (7 men and 33 women) were enrolled in the study. Twenty patients presented with lymph node metastasis, whereas the other 20 did not. Laminin-5 expression was determined by immunohistochemical staining with antibodies against the laminin-5γ2 chain in all 40 patients. The correlation between laminin-5 expression and clinical factors such as tumor size, multiplicity, and lymph node metastasis were investigated.
Laminin-5 was expressed specifically within tumor tissue compared to normal thyroid tissue. The frequency of laminin-5γ2 chain expression showed significant correlation with cervical lymph node metastasis (p=0.003). As the tumor size increased, laminin-5 showed a tendency for higher expression, although the correlation was not statistically significant (p=0.082). No relationship between the presence of multiple tumors and the expression of laminin-5 was identified.
Laminin-5 expression may be helpful in the diagnosis of papillary thyroid carcinoma, and our results suggest that high levels of laminin-5 expression may be a useful marker for predicting lymph node metastasis of papillary thyroid carcinoma.
Thyroid Cancer Thursday Poster
The Afirma Gene Expression Classifier (GEC) measures the mRNA expression of 167 genes to classify indeterminate thyroid FNAs as either Benign or Suspicious. A clinical validation study of nodules ranging up to 9.1 cm in size found no relationship between false negative (FN) results and nodule size; however, no independent studies have confirmed GEC performance in a consecutive series of large thyroid nodules (≥3 cm).
GEC testing was prospectively performed on 50 consecutive nodules ≥3 cm submitted to the Veracyte CLIA laboratory after cytopathology diagnosis by Old Dominion Pathology Associates from 3/28/2012 to 3/27/2013. Among the 47 with GEC Benign or Suspicious results, 40% were GEC Benign. Surgical pathology was obtained when available for nodules ≥3 cm through 2/14/2014 (26 nodules, mean size 4.2 cm, range 3–7.1 cm). 25/26 nodules had an indeterminate (Bethesda III-IV) cytopathology diagnosis of “cellular follicular lesion” while 1 nodule had an indeterminate diagnosis of “thyroid neoplasm, favor MTC.”
25/26 (96%) nodules had sufficient mRNA for GEC testing. Of resected nodules with GEC results, 10/25 (40%) were malignant and 15/25 were benign (60%) on surgical pathology. Five were classified as GEC Benign and twenty as GEC Suspicious (Table 1). All five GEC Benign nodules were benign on surgical pathology (NPV 100%). Of the twenty GEC Suspicious nodules, ten were malignant by surgical pathology (PPV 50%). The sensitivity of the GEC was 100%. The “thyroid neoplasm, favor MTC” indeterminate nodule was correctly identified as MTC by the GEC.
Afirma GEC and Surgical Pathology Results for Thyroid Nodules ≥3 cm
We conclude that in the absence of other indications for surgery, molecular analysis can correctly identify ≥3 cm nodules for clinical observation instead of surgical resection. The GEC accurately predicted benign status in large cytologically indeterminate thyroid nodules with high sensitivity and low FN rate (1-sensitivity), both useful metrics as a complement to NPV because they are independent of the pre-test risk of malignancy. With high NPV and sensitivity along with a low FN rate, these findings are consistent with previously reported GEC performance and support GEC use in large nodules to consider observation in lieu of diagnostic surgery.
Thyroid Cancer Thursday Poster Clinical
Thyroglobulin (Tg) immunoassays might not be reliable in 20–30% of thyroid cancer patients due to anti-thyroglobulin auto-antibodies (TgAb). Mass spectrometric Tg assays (Tg-MS) are not affected by TgAb, allowing accurate determination of Tg in TgAb+ patients. The goal of this study was to assess the degree of TgAb interference in four automated immunoassays (AIAs) (Beckman Access, Roche Elecsys, Siemens Immulite and Thermo Kryptor) and two radioimmunoassays (RIAs) through comparison with a Tg-MS assay.
Residual samples from 625 patients who had undergone Tg and TgAb testing (Tg: Beckman, TgAb: Roche) were evaluated. The Tg concentrations ranged from <0.1–2000 ng/ mL and included 269 TgAb- and 356 TgAb+ samples. All samples were tested with the four Tg and TgAb AIAs and by Tg-MS. Subsets of the samples were also tested by Tg-RIA (USC n=111 and UK n=126).
In TgAb+ samples with detectable Tg by Tg-MS and AIAs, the Tg concentration was underestimated on average by 40% (Kryptor), 60% (Roche and Beckman) and 95% (Immulite). In the Tg RIAs, TgAb+ samples with detectable Tg by Tg-MS and Tg RIA, the Tg concentration was slightly underestimated by the USC-RIA and overestimated by the UK-RIA. In specimens that were TgAb+ by 1 or more TgAb assays, Tg was detectable by Tg-MS, but undetectable by the AIAs in 7% (15/221; Kryptor), 7% (15/220 Beckman), 8% (18/225; Roche) and 15% (36/243; Immulite) of specimens. In TgAb+ samples with undetectable Tg by Tg-MS, Tg was detectable by RIA in 57% (39/68; USC-RIA) and 60% (26/43; UK-RIA) of specimens. Spiking sera, which contained neither Tg nor TgAb, with increasing concentrations of TgAb also resulted in detectable Tg by the RIAs but not by Tg-MS.
The Immulite Tg assay was most affected by TgAb, the Kryptor assay least. The RIAs tended to show possibly false-positive, detectable Tg in cases undetectable by Tg-MS, a finding that is further being investigated. Finally, studies are underway to correlate our results with the patients' clinical outcomes.
Thyroid Cancer Thursday Poster Clinical
Radioactive iodine (RAI) is currently recommend for patients with advanced and aggressive cases of differentiated thyroid carcinoma (DTC), but its use in patients with early-stage disease remains an area of much debate.
Population-based study using Surveillance, Epidemiology, and End Results (SEER) data from 1973- 2009 for patients with differentiated thyroid carcinoma. The association between RAI and cancer-specific survival was examined using multivariate analyses in 149 population subgroups, and controlling for age, decade of diagnosis, race, sex, tumor, nodal, metastasis stage, and RAI therapy.
Among 85,740 patients with DTC, RAI was used in 43.3% of patients. By AJCC stage, RAI was used in 54.6% of Stage I, 40.5% of Stage II, 94.2% of Stage III, and in 84.8% of Stage IV disease. Patients with T1a disease received RAI 41.9% of the time and in 88.2% of T4 cases. Across the entire cohort, RAI use had a positive association with survival (hazard ratio (HR) 1.3, P=0.002). Statistically significant HRs for RAI were seen in 49 population subgroups. RAI use was associated with decreased risk for disease-specific mortality in patients with metastatic (M1) disease (HR range 2.28–3.82). Similar protective effects from RAI were observed in patients with regional metastases (HR range 1.4–2.9), T3+ tumors (HR range 1.36–1.39), T4 tumors (HR 1.85), and in patients with stage IV disease (HR range 1.47–1.73). In patients with T1a disease, there was an increased likelihood of thyroid cancer-specific mortality when RAI was used (HR 0.13, P<0.001). The same was found in multiple other subgroups of patients within those with T1a disease (HR range 0.04 to 0.25). No statistically significant effect of RAI was seen in patient subgroups with T1b or T2 tumors.
In this cohort of patients with DTC, the use of RAI was associated with improved disease-specific survival in patients with advanced disease. The use of RAI showed a negative effect in patients with micropapillary carcinoma. Future studies are warranted to further investigate and confirm the negative effect seen in T1a patients in this study.
Radioactive iodine utility in subpopulations of differentiated thyroid carcinoma
Thyroid Cancer Thursday Poster Clinical
Age at diagnosis is incorporated into all relevant staging systems for differentiated thyroid carcinoma (DTC). There is growing evidence that a specific age-cutoff may not be ideal for accurate risk stratification. We sought to evaluate the interplay between age and oncologic variables in patients with DTC using the largest cohort to date.
The Surveillance, Epidemiology, and End Results (SEER) database was queried from 1973 and 2009 to identify patients with DTC as their only malignancy. Multivariate analyses using a range of age-cutoffs and age sub-groupings were utilized in order to search for an optimal age that would provide the most significant risk stratification between young and old patients. The primary outcome was thyroid cancer-specific mortality and covariates included: age, race, sex, tumor/nodal/metastasis (TNM) stage, decade of diagnosis, and radioactive iodine therapy.
85,740 patients were identified. 76% of patients were American Joint Committee on Cancer (AJCC) stage I, 8% were stage II, 7% were stage III and 8% were stage IV. Age over 45 years (hazard ratio (HR) 19.2, P<0.001) and metastatic disease (HR 13.1, P<0.001) were the strongest predictors of thyroid cancer-specific mortality. Other factors that significantly predicted cancer-specific mortality included: not receiving radioactive iodine (HR 1.3, P=0.002), T3 (HR 2.6, P<0.001) and T4 (HR 3.3, P<0.001) disease, and nodal spread (HR 2.6 to 3.3, P<0.001). Female gender showed a significant protective effect (HR 0.7, P=0.001). Adjusting the age-group cutoff from 25 to 55 years showed consistently high hazard ratios for advanced age, without a distinct change at any point. Comparing hazard ratios for T, N, and M stage between young and old patient subgroups showed that advanced disease increased the risk for cancer-specific mortality regardless of age, and was oftentimes a worse prognosticator in young patients.
The contribution of age at diagnosis to a patient's disease-specific mortality is considerable, but there is no age-cutoff that affords any unique risk-stratification in patients with DTC.
Thyroid Cancer Thursday Poster Clinical
In non-metastatic differentiated thyroid cancer (DTC) patients with macroscopic extra-thyroidal extension (MAEE), high dose radioactive iodine(RAI) is recommended. It's unclear whether these patients could be treated with low dose RAI when preablative stimulated thyroglobulin (ps-Tg) is low. This study aims to evaluate the ablative efficacy and clinical outcome of low dose radioiodine in patients with MAEE but low ps-Tg level.
This is a retrospective study of 103 DTC patients with total/near-total thyroidectomy and selective lymph node resection, and with MAEE, any N stage, ps-Tg≤5ng/ml when thyroglobulin antibodies (TgAb) ≤46 IU/ml and no evidence of distant metastasis were included. Fifty-two received low dose RAI (1110 MBq) and 51 received high dose (≥3700 MBq). Successful ablation was identified as 1) stimulated Tg≤1.0 ng/ml; 2) negative diagnostic 131I whole body scan; 3) negative neck ultrasonography. When suppressive serum Tg was ≤1.0 ng/ml and neck US was negative, patients were defined as disease-free. Clinical recurrence was defined as the reappearance of disease confirmed by cytology or pathology.
Successful ablative rate was 86.5% (45/52) in low dose group and 86.3% (44/51) in high dose group, with no significant difference. For people who were followed up for more than one year, disease-free status was observed in 97.4% (38/39) in low dose group and 97.5% (39/40) in high dose group. One patients had clinical recurrences with trachea invasion in high dose group.
Ablation with low dose RAI is proved to be non-inferior to high dose in non-metastatic patients with MAEE when ps-Tg level is less than 5 ng/ml.
Thyroid Cancer Thursday Poster Clinical
It was reported that BRAFV600E mutation correlates with radioactive iodine (RAI) refractory papillary thyroid carcinoma (PTC) in local recurrence, whereas its relationship with 131I uptake status in distant metastatic PTC remains uncertain. This prospective study tried to explore the association between 131I uptake in distant metastases (DM) of PTC and BRAFV600E mutation status in their primary tumor.
Seventy-three patients with DM were divided into BRAFV600E mutation group (n=19) and wild-type BRAF group (n=54) according to the BRAF mutation status. After posttherapy 131I whole-body scan (RxWBS) were performed, the relation between 131I uptake in DM, BRAFV600E mutation status and clinicopathological characteristics of two groups were compared.
The mean age of mutation group was older than that of the wild-type group (P<0.05). In the mutation group, 16 patients (84.2%, 16 of 19) were found to be Non-RAI-Avid DM, while in wild-type group, only 5.6% (3 of 54) were Non-RAI-Avid DM. The sensitivity and specificity of using BRAFV600E mutation for the identification of Non-RAI-Avid DM were 84.2% and 94.4%, respectively.
BRAFV600E mutation in primary tumor might be a promising molecular marker to predict the status of 131I uptake in distal metastases.
Thyroid Cancer Thursday Poster Clinical
The RLN injury caused by thyroidectomy is a problem which puzzled both surgeons and patients. However, the experience to identify variation of the RLN, choose the right protection method timely, reveal proficiently, is uneven among the doctors at different levels, who lack of the direction by IONM guideline. Improving the traditional surgical approach, giving up the blind resection within the thyroid capsule, and further raising the preservation awareness, completely acquisiting the anatomical characteristics, surgical conception, operating techniques, routine exposing the laryngeal nerve, and assisting by IONM, could improve surgical safety.
From March 2009 to December 2013, 2597 patients underwent thyroidectomy with RLN protection were included in this study, in which 1447 cases were protected by visual identification only, and 1150 complex cases were protected by visual identification and IONM. Vagus nerve and RLN were tested respectively before and after resection of thyroid lobe. Video recording of cord mobility was performed routinely pre- and postoperatively.
By the “multi-sites, three steps” RLN exposure method,1417 cases (85.16%) were successfully recognized and the recognition time was (3.57±1.26)min. The recognition time in the rest 30 complex cases (2.07%) without IONM was (17. 02±5. 48) min. By this method, the temporary RLN injury occurred in 23 cases (1.54%) and 15 cases (65. 22%) recovered within 2 weeks. In patients undewent IONM, the recognition rate was 100% and recognition time was (2.18±0.67) min. The temporary RLN injury occurred in 20 cases (1.74%) and 15 cases (75.00%) recovered within 2 weeks. All temporary RLN injuries recovered within 1 month and no persistent RLN injury occurred. Accurately detect non-RLN in 34 nerves.
Conventional visual identification can reduce the RLN injury, but not meet the needs of the RLN protection during complex thyroidectomy. Apply the IONM as an adjunct to avoid RLN injury. The combination of visual identification and IONM can further improve the recognition rate and shorten the recovery time of vocal cord dyskinesia. IONM could make RLN identification more reliable and precise, test the functional integrity of RLN.
Thyroid Cancer Thursday Poster Clinical
Removal of all macroscopic thyroid tissue is mandatory in total thyroidectomy. Although surgeons do their best to completely remove thyroid tissues, several anatomical variants of the thyroid may remain after total thyroidectomy, including the thyroglossal duct remnant (TGDR) and pyramidal lobe. These remnant thyroid tissues can provide undesirable radioiodine uptake foci. Thus, we tried to evaluate the frequency of visualization of TGDR on post-therapy 131I-SPECT/CT and the relationship between TGDR uptake on post-therapy 131I-SPECT/CT and the presence and features of pyramidal lobes.
Total 179 DTC patients who treated with total thyroidectomy underwent 131I-SPECT/CT imaging of the neck after 131I ablation therapy. In the preoperative neck CTs, the pyramidal lobe was defined as longitudinally arranged thyroid tissue protruding from the upper margin of the thyroid lobes or isthmus on three or more serial axial images. In cases where the pyramidal lobe existed, radiologists classified it into one of three categories according to the location of the upper end: above the hyoid, thyrohyoid membrane, or thyroid cartilage. The TGDR uptake was defined as distinguishable uptake from the thyroid bed corresponded to the expected pathway of thyroglossal duct when there was no evidence of detectable metastatic lesion in this area on CT images. Patients exhibiting positive TGDR uptake were classified according to the center of its activity.
The number of patients with TGDR uptake was 44.7% on 131I-SPECT/CT images. In 179 studied patients, remnant pyramidal lobes were detected in 61 cases and there was correlation between the upper border level of remnant pyramidal lobe and location of radionuclide uptake in 33 patients (38.4%) (Figure).
Thin and small volumes of pyramidal lobe were noted up to the level of the hyoid bone on preoperative neck CTs (A). 131I-SPECT/CT showed strong tracer uptake in the same area where the upper margin of pyramidal lobe was located.

131I uptake on remnant pyramidal lobe or TSH-activated dormant thyroid tissue in the thyroglossal duct are frequently visualized and well clarified on 131I-SPECT/CT. It helps nuclear medicine physicians to interpret post-therapy 131I-WBSs.
Thyroid Cancer Thursday Poster Clinical
I-123 is considered an ideal isotope for diagnostic studies. A significant advantage of I-123 over I-131 is that, the radiation dose delivered is about 100-fold less. Consequently, potential “stunning” because of the dosimetry procedure prior to treatment would be less concerning. However, its relatively short half-life makes it impractical for a prolonged biokinetic study. The aim of the current study was to assess the relationship between actual I-131 retention and the success rate of I-131 ablation in differentiated thyroid carcinoma (DTC) following I-123 whole body scan (WBS).
23 consecutive patients with newly diagnosed DTC (21 papillary, and 2 Follicular), underwent total or near total thyroidectomy, followed by I-123 WBS, and subsequent I-131 ablation were enrolled in current study. The whole body external exposure rate from the patient at 1 meter was measured immediately after ingestion of I-131, after 24 and 48 hours, using a calibrated Victoreen 451P ionization chamber survey meter (Fluke Biomedical, USA). The retained activity at 48 h, and the whole body effective half-life for each patient were then calculated. Patients were classified according to their follow up data after 6 months into two groups; those who have successful ablation (Negative WBS and an undetectable serum thyroglobulin level in the absence of antithyroglobulin antibodies), and those who need reablation (Positive WBS and/ or elevated serum Thyroglobulin).
Of the 23 patients studied, 15 were considered to have successful ablation and 8 still need reablation. No significant difference regarding age, gender, histopathology, and activity of I-131 ablation dose between both groups. The retained I-131 activity at 48 hours was 13.50±3.87% of the administered dose, and the effective half-life was 16.37±2.43 hours for patients who have successful ablation compared to 7.79±3.28% (p<0.05), and 12.64±2.27 hours (p<0.05) respectively for patients who need reablation.
We found a significantly higher retained I-131 activity at 48 hours and longer effective half-life among patients successfully ablated compared to those who need reablation, and recommend dosimetric adjusted I-131 ablation dose whenever feasible accordingly.
Thyroid Cancer Thursday Poster Clinical
The aim of this study was to investigate the therapeutic potential of lithium (Li) during radioactive iodide therapy (RAI) in patients with metastatic radioiodine-refractory differentiated thyroid cancer (DTC).
Twenty nine patients (9 men, 20 women; age 53±15 years) with metastatic radioiodine-refractory DTC underwent combined treatment with 131I and Li. During each combined treatment, patients were administered oral Li for 7 days (from 5 day before RAI to 1 day after RAI) at 300 mg daily. Treatment responses were assessed using serum thyroglobulin (Tg) levels and the change in tumor size 6 months after the combined treatment. To verify the therapeutic potential of Li, overall survival was compared between these combined treatment group (N=24) and control groups (N=48) with conventional RAI using Kaplan-Meier method after propensity score matching.
After the combined treatment using 131I and Li, 13 patients showed stable disease and 16 patients showed progressive disease, summarizing an overall response rate of 45%. The patients with stable disease showed better progression free survival than patients with progressive disease (26 months vs. 47 months, p=0.070), but these patients with stable disease did not associate with better overall survival (p=0.42). Patients with Li combined treatment survived longer than patients with conventional RAI (115.5 months vs. 43.5 months, p<0.0001).
The combined treatment using 131I and Li revealed a response rate of 45% among patients with metastatic radioiodine-refractory DTC and patients with these combined treatment showed better overall survival than patients with conventional RAI. Li could be applied for the patient with advanced DTC during RAI.
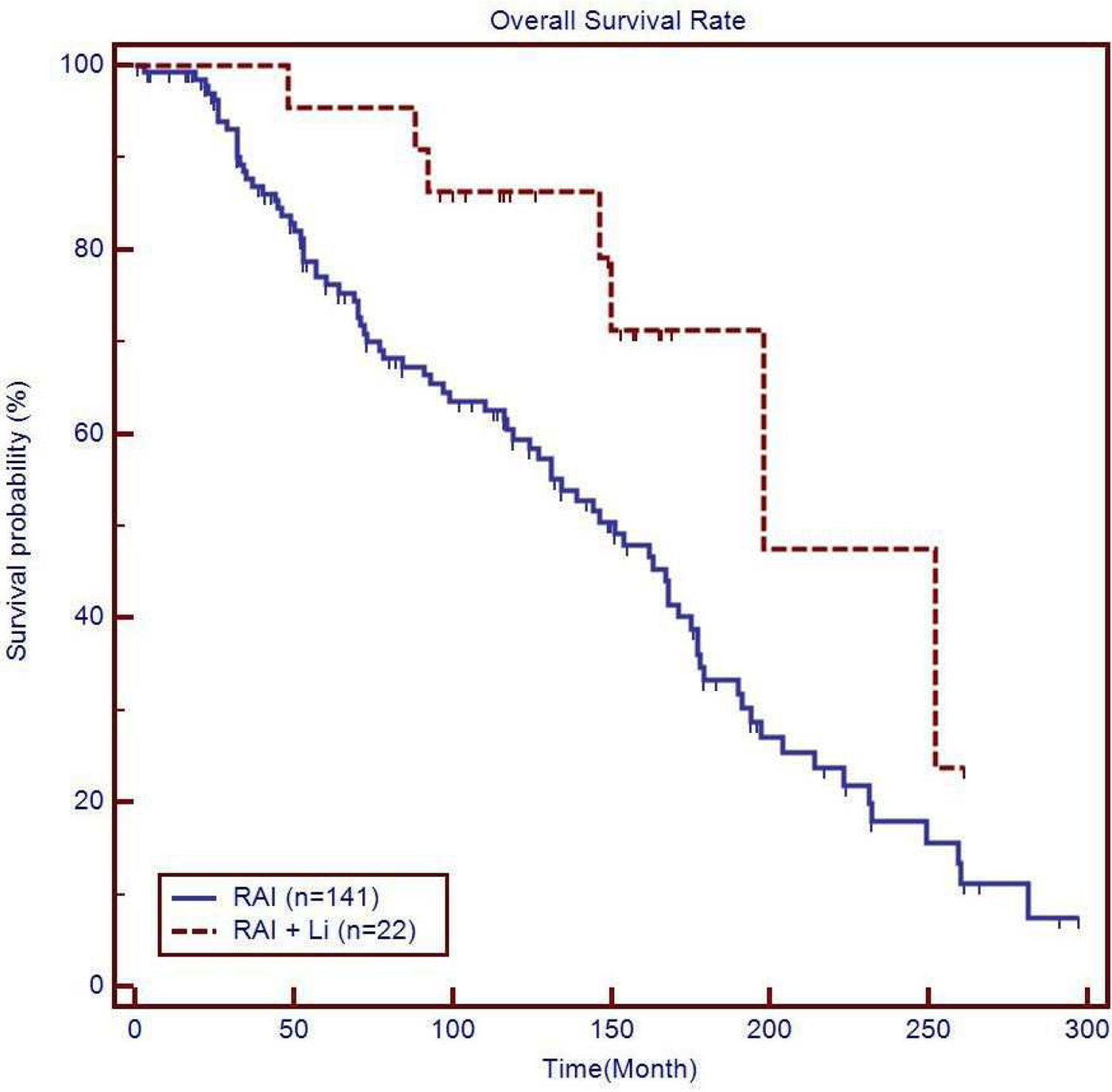
Thyroid Cancer Thursday Poster Clinical
Fine-needle aspiration (FNA) cytology has been the standard of care in the workup of cervical lymph nodes (LNs) in patients with recurrent papillary thyroid cancer (PTC) and suspicious cervical LNs. Recently FNA thyroglobulin (TG) washout measurement has been proposed to be an adjunct in the management of these patients. We hypothesized that surgeon-performed ultrasound using TG washout for suspicious cervical LNs would increase the accuracy of diagnosing metastatic cervical LNs in patients with recurrent PTC.
This is a retrospective study of prospectively collected database for thyroid cancer patients who underwent preoperative FNA followed by selective neck dissection by one surgeon at an academic institution. FNA-cytology and FNA-TG washout were performed simultaneously in the same sitting. One hundred thirty eight patients were included in our study of which 67 (48.55%) had undergone surgery. Thirty of these patients had a modified radical neck dissection, 31 had a central LN dissection, and 6 had a modified radical neck dissection in addition to central LN dissection. Results of both methods were then correlated with the final surgical pathology.
FNA-cytology alone showed a sensitivity of 81.48%, specificity of 100.00% with a negative predictive value (NPV) of 85.07%. In contrast, FNA-Tg washout had a sensitivity of 93.75%, specificity of 93.94% with a NPV of 91.18%. Combination of the FNA-cytology with FNA-Tg washout increased the diagnosis accuracy with a sensitivity of 100.00%, specificity of 100.00% with a NPV of 100.00%. All of the 7 malignant cervical LNs with false negative FNA- cytology had elevated TG washout, 6 of which were cystic in nature or highly vascular on ultrasonography.
FNA-Tg washout increases the diagnostic accuracy in detecting metastatic disease in patients with recurrent thyroid cancer. TG washout may be of special diagnostic importance in cystic or highly vascular LNs, which might have falsely negative cytology. Routine performance of US-guided FNA-Tg washout as an adjunct to FNA-cytology should be considered in-patients with suspicious metastatic cervical LNs.
Withdrawn
Thyroid Cancer Thursday Poster Clinical
The decision to accept or reject radioactive iodine remnant ablation (RRA) in patients with low-risk papillary thyroid cancer (PTC) is subject to uncertainty. We explored for variables associated with PTC survivors' RRA decision satisfaction.
We recruited low risk PTC survivors who participated in a randomized controlled trial of a decision aid (DA) explaining RRA choice. The primary outcome was RRA decision satisfaction (DS), measured on a 5-point Likert Scale. We compared DS in the DA group compared to controls. We explored for correlations of DS with the following questionnaire scores: Feeling of Being Informed questionnaire, Decision Regret Scale, Assessment of Survivor Concerns (cancer-related worry), Patient Health Questionnaire-4 (PHQ-4, depression and anxiety screen), and Trust in Physician Scale. We explored for differences in DS according to patients' perceptions of who made the final RRA choice (ANOVA).
95% of the trial participants consented to this study (70/74); about half of participants had been exposed to the DA (34/70) and about a quarter had RRA (18/70). The mean time since first thyroid cancer surgery was 19.9 months (standard deviation, SD 3.0). There were 57 females (81%); the mean age was 47.1 years (SD 12.3). RRA choice was primarily attributed to the following individuals: patient - 42% (29/69), physician - 14.5% (10/69), or both - 43.5% (30/69). Since DS was not significantly associated with DA use (p=0.142), data from both groups was combined. The following positive Spearman correlations with DS were observed: Feeling of Being Informed (r=0.664, p<0.001) and Trust in Physician (r=0.300, p=0.012). The following negative correlations with DS were observed: Decision Regret (r=−0.811, p<0.001) and cancer-related worry (r=−0.245, p=0.041). Mood was not significantly associated with DS (PHQ-4, r=0.008, p=0.948). Patients who were more involved in decision-making were more satisfied (p=0.012).
Patients' RRA decision satisfaction may incorporate perceptions of the decision-making process, patient-physician relationships, and ongoing cancer-related worry.
Thyroid Cancer Thursday Poster Clinical
We have previously reported that bilateral papillary thyroid carcinoma (PTC) presents with more advanced tumor stage and has a shorter disease-free survival than unilateral PTC in a cohort of 891 patients. Here we have expended our study to more than 2,000 PTC patients treated in a single institute. We further compared the difference between bilateral PTC and unilateral-multiple PTC in this study.
The clinicopathological features of 2,211 consecutive PTC patients who underwent surgical treatment in our institute between 1997 and 2011 were reviewed. Among these patients, 425 (19.2%) were bilateral PTCs and 1,786 were unilateral PTCs. We subdivided the unilateral PTCs into two groups, unilateral-multiple PTCs (210 patients) and solitary PTCs (1576 patients) respectively. The rates of disease-free survival (DFS) and overall survival (OS) were calculated to compare the prognosis among different groups. We also examined the BRAFV600E mutation by polymerase chain reaction amplification and DNA sequencing.
When comparing between various groups, we found that bilateral PTCs had larger tumor size, higher prevalence of extrathyroidal invasion, lymph node metastasis, and more advanced tumor stage than unilateral PTCs, including unilateral-multiple PTCs. More importantly, the patients' outcomes were significantly different among groups in terms of disease-free survival rate. The 10-year DFS was 78.7% in bilateral PTCs, while it was 85.7% in unilateral-multiple PTCs and 89.3% in solitary PTCs (p=0.005). The prevalence of BRAFV600E mutation in bilateral PTCs was much higher than that in unilateral PTC (75.7% vs. 67.1%; p=0.023), but with no difference than that in unilateral-multiple PTCs.
The present study indicates that bilaterality is a predictor of more advanced stage and shorter disease-free survival. Furthermore, bilateral PTCs are associated with more aggressive behavior than unilateral-multiple PTCs.
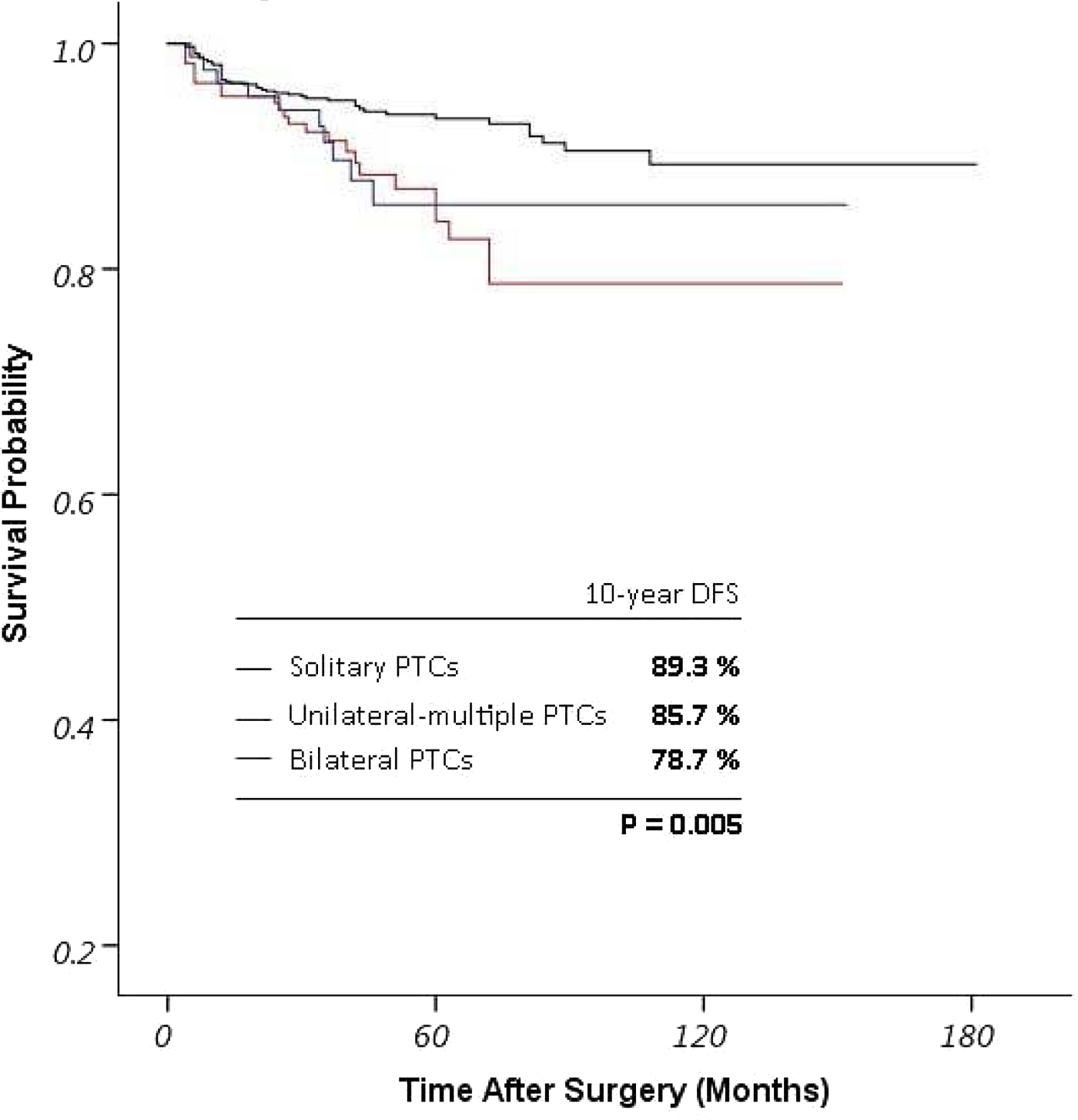
Kaplan-Meier survival curves showing disease-free survival for patients with bilateral PTCs, unilateral-multiple PTCs and solitary PTCs.
Thyroid Cancer Thursday Poster Clinical
Identifying malignant thyroid nodules is a challenging step in managing patients with thyroid nodules. Ultrasound Elastography, mapping the elasticity of thyroid tissue, was proposed to contribute to an increased detection of malignant thyroid nodules. Our systematic review compared diagnostic role of Elastography to Conventional Ultrasound and defined whether elastography has a complementary role to Fine Needle Aspiration (FNA) in differentiating benign from malignant nodules.
The Embase and PubMed databases were searched for English articles evaluating more than 50 nodules using specimen histopathology as reference standard. Nodules were divided into benign/malignant cytology (group 1) and indeterminate cytology (group 2). Elasticity score was compared to Ultrasound features such as taller than wide, irregular margins, internal vascularity, calcification and absent of halo to determine validity measures and likelihood ratios (LR).
Fourteen studies met our criteria. Of 2732 nodules,1734 were benign,685 malignant,313 indeterminate. For group 1, elastography showed sensitivity 75.2%, specificity 80%, Positive predictive Value (PPV) 60.5%, Negative Predictive Value (NPV) 88.8%, LR of 5.67 with higher predictive value for nodules <1 cm (PPV 79%; NPV 83.3%). The strongest Ultrasound-predictor of malignancy for group 1 was ‘taller than wide’ feature (specificity 92%; PPV 51.3%), however, its sensitivity was 24.3%. Irregular margins also showed higher predictive values (specificity 90.7%; sensitivity 48.2%; PPV 64.4%). Combination of elastography and ultrasound had higher sensitivity (96%) and NPV (96.2%) but lower specificity (46.5%) and PPV (46.1%). For group 2, elastography revealed higher sensitivity (89.5%) and NPV (92%). On Ultrasound, type III vascularization had higher sensitivity (78.1%) and PPV (71.4%) while ‘taller than wide’ feature had greater specificity (84.8%) but limited sensitivity and PPV.
Conventional ultrasound-predictors proved to be more specific in delineating malignant and benign thyroid nodules. However, combination of elastography and ultrasound display markedly increased sensitivity leading to better selection of candidates for FNA. Future studies are warranted to define its precision for indeterminate nodules.
Thyroid Cancer Thursday Poster Clinical
Follicular variant of papillary thyroid carcinoma (FVPTC) had histological subtypes according to the invasiveness and a presence of fibrous capsule around the tumor. Neck ultrasonography (US) might be a useful tool for evaluation of thyroid nodules in terms of malignant potentials. This study aims to evaluate whether preoperative US findings can predict clinico-pathological features and clinical outcomes of FVPTC.
This retrospective study enrolled patients with FVPTC (n=70), size-matched classical PTC (CPTC, n=328), follicular thyroid carcinoma (n=85), and follicular adenoma (FA, n=120). Histological subtypes of FVPTC were categorized as encapsulated (E-FVPTC; n=51) and non-encapsulated subtypes (NE-FVPTC; n=19). Preoperative US were reviewed and graded by US scoring system based on orientation, echogenicity, margin, and calcification. FVPTCs were also classified as low US group (score <2.5; n=42) and high US group (score >2.5; n=28).
Median US score of FVPTC (2) was lower than CPTC (7, p<0.001), and higher than FA (0, p<0.001). In FVPTC, median US score of NE-FVPTC was significantly higher than E-FVPTC (4 vs. 2, p=0.009). In fine needle aspiration cytology (FNAC), NE-FVPTC was more likely to diagnosed as malignancy or suspicious for malignancy than E-FVPTC (p=0.002). Cumulative risks of cervical LN metastasis and distant metastasis according to tumor size were significantly higher in NE-FVPTC than E-FVPTC (all p<0.001). Cumulative risks of cervical LN metastasis and that of capsular invasion according to tumor size were significantly higher in high US group than low US group (p=0.005, p<0.001, respectively).
Histological subtype of FVPTC was an important prognostic factor of FVPTC. US findings might be useful for prediction of the histological subtype and clinical behavior of FVPTC.
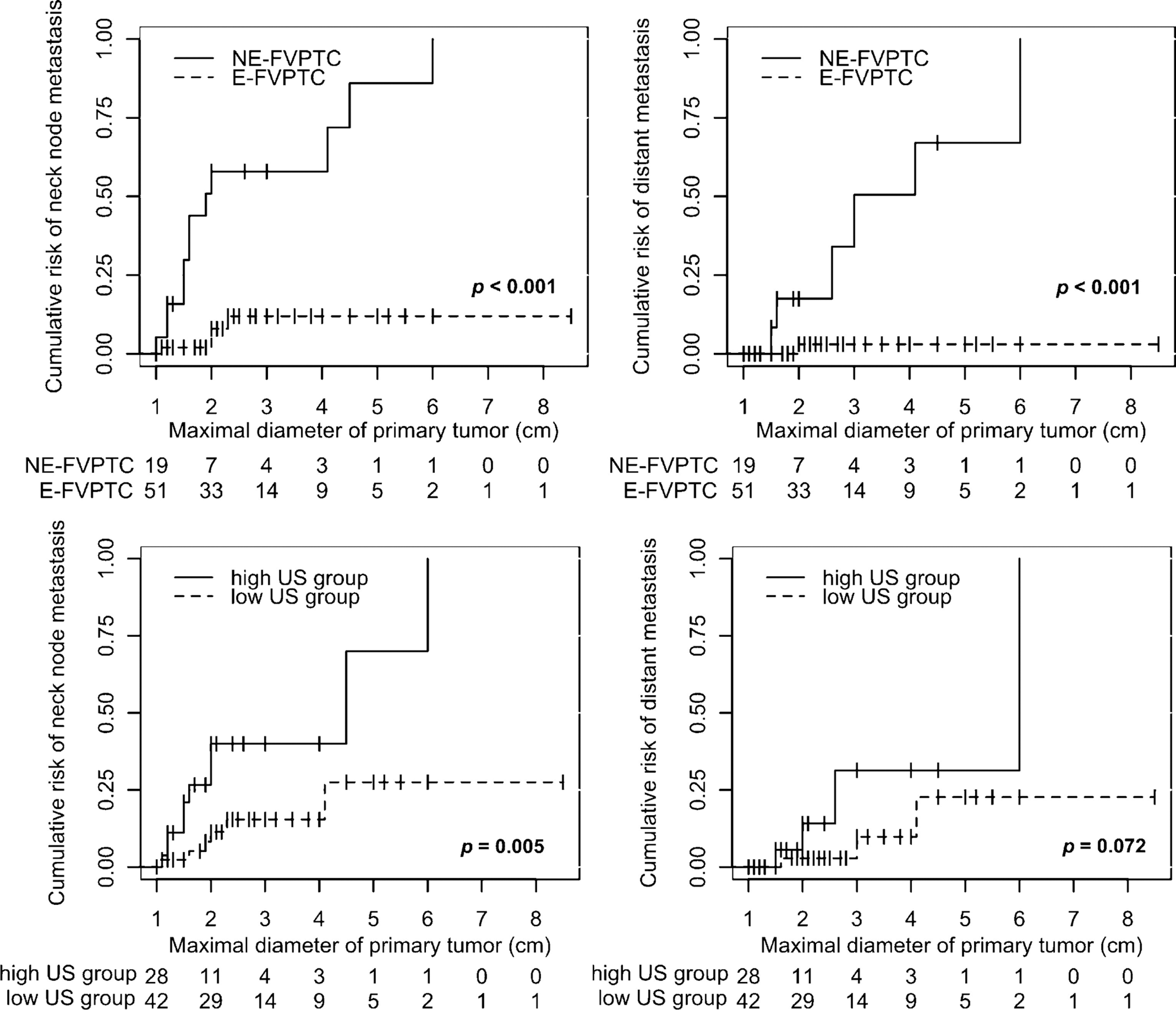
Thyroid Cancer Thursday Poster Clinical
Recent guidelines from the American Thyroid Association suggest that all patients with anaplastic thyroid cancer (ATC) and a reasonable performance status should be offered multimodality therapy (MMT) in the form of surgery with radiation (XRT) +/− chemotherapy. We sought to determine treatment patterns in patients with ATC.
Patients with a diagnosis of ATC from 2004–2010 were identified in the SEER registry. Clinicopathologic, geographic and socioeconomic factors associated with recommendation or receipt of therapy was assessed using univariate and multivariate analyses.
A total of 545 patients were identified, 137 of whom received surgery with XRT and/or chemotherapy (MMT). Seven patients had MMT recommended, but did not receive this treatment. Patients that were recommended or received MMT were more likely to be younger (Age <70, 35% vs 19%, p<0.001), with a higher than median adjusted household income (31% vs 23%, p=0.03), and had tumors that were ≤6 cm (40% vs 19%, p<0.001), with central neck only disease (N1a-51% vs N1b-24%, p<0.001), and a lower overall stage at diagnosis (IVA-41% vs IVB−40% vs IVC-16%, p<0.001). Age, stage and tumor size remained significant independent predictors of receipt or recommendation for MMT on multivariate analysis. Nearly a third of all patients (n=157, 29%) received no therapy; 98 of whom had no recommendations for surgery or XRT. Factors predicting a lack of recommendation for either surgery or XRT, were female gender (20% vs 14%, p=0.05), living in the Pacific coast region (p<0.001), tumor size >6 cm (21% vs 14%, p=0.04), involvement of lateral neck nodes (19% vs 8%, p=0.01), and a higher overall stage at diagnosis (IVC-29% vs IVB-7% vs IVA-7%, p<0.001). On multivariate analysis, tumor stage and geographical region remained significant predictors of a lack of recommendation of treatment.
MMT for ATC is often recommended for younger patients with surgically resectable disease. While older patients with larger tumor burden may not receive MMT perhaps due to poorer performance status or unresectable disease, it is concerning that lack of recommendations for any treatment varied significantly by geography independent of pathologic variables.
Thyroid Cancer Thursday Poster Clinical
Lymph node metastasis involving the central neck is a common finding in papillary thyroid cancer and a hallmark for risk of recurrence. The purpose of this study was to assess the impact of extent and burden of central compartment nodal involvement on disease-free survival in patients with papillary thyroid cancer.
All patients with papillary thyroid cancer treated at our institution from 1999–2012 who had central neck lymph nodes sent for pathologic assessment formed the study cohort. Univariate and Cox multivariate analyses were used to determine clincopathologic factors that were associated with disease-free survival.
A total of 415 patients met inclusion criteria. Median tumor size was 1.8 cm. Positive nodal disease was pathologically confirmed in 72.3% of patients. Within the entire cohort, 75.4% received a formal central neck dissection, of which 27.5% also received nodal clearance of the lateral neck. The remaining 24.6% of patients received sampling of suspicious lymph nodes, 31% of which were positive on final pathology. With a median follow-up time of 36 months, a total of 6.5% of patients suffered a recurrence, the majority being either local (37.0%) or regional (40.7%) in nature. Recurrence was observed in 2.7% of patients with node negative disease, 5.3% of patients with N1a, and 13.1% of patients with N1b disease. On univariate analysis, male gender, tumor size greater than 2 cm, extrathyroidal extension, lymphovascular invasion, positive margins, and receipt of adjuvant RAI were positively associated with recurrence. In addition, surgical specimens with a positive lymph node ratio ≥0.4, extranodal invasion, or nodal spread to the lateral compartment were correlated with poorer disease-free survival (log-rank, p<0.05 for all). On multivariate analysis, however, only LNR≥0.4 (HR 3.2, 95%CI: 1.2–9.2, p=0.015) and male gender (HR 3.7, 95%CI; 1.4–10.4, p=0.010) remained independent predictors of recurrence.
This study demonstrates variable recurrence rates in patients with N0/N1 disease. Stratification with consideration of gender, LNR, and potentially other factors such as extranodal extension better identify patients at highest risk of recurrence.
Thyroid Cancer Thursday Poster Clinical
SEER data suggests that in the United States since 1975 there has been an “ongoing epidemic” of thyroid carcinoma (TC). By contrast, in Olmsted County (OC), Minnesota, TC incidence rates increased between 1935 and 1964, but remained stable during 1964–99.
We used Rochester Epidemiology Project resources to examine the incidence and method of diagnosis of all TC cases in OC residents during 2000–12 and compared rates to those from 1990–99.
The age-adjusted incidence (AAI) for TC increased from 7.1(95% confidence interval, CI, 5.5–8.8) per 100,000 person-years (p-y) during 1990–99 to 13.7 (95% CI 11.8–15.6) per 100,000 p-y during 2000–12. Of 213 TC cases found in 2000–12, 112 (53%) did not present with symptoms or visible lesions. Excluding these 112 clinically “occult” cases, the AAI of TC was 6.3 (95% CI 5–7.5) per 100,000 p-y, near identical to the 6.3 rate seen in OC since 1970. The 112 “occult” cases, when compared to clinically recognized cases, were significantly older at diagnosis (mean age 49.6 vs 42.7 years), had smaller lesions (mean tumor size 1.3 cm vs 2.2 cm) (p<0.01 for both comparisons) and had similar distribution of low-risk papillary cancers (MACIS<6, 87% vs. 84%). The most frequent reasons for recognition of “occult” tumors were incidental discovery during diagnostic neck imaging in 40 (36%), pathology review of specimens from thyroidectomies for benign conditions in 29 (26%), screening through physical exam 22(20%) and investigations of symptomatic patients, whose symptoms were clearly not associated with TC, in 13 (12%).
In OC during 2000–12 more than 50% of thyroid cancers were found in asymptomatic patients. The AAI of clinical recognized TC is nearly identical to the AAI seen in OC since 1970, implying that the increased incidence observed relates to the discovery of a reservoir of previously unrecognized, possibly clinically unimportant, disease.
Thyroid Nodules & Goiter Thursday Poster Clinical
Hypocalcemia is a known complication post thyroidectomy that typically presents within the first 48 hours but has been reported to be delayed as much as 7 days. Decreased parathyroid hormone (PTH) levels intra- or immediately post-surgery have been shown to be a risk factor for hypocalcemia. Various calcium supplementation regimens have been proposed to prevent this complication. In February of 2013, the Department of Otolaryngology and the Division of Endocrinology at Mayo Clinic Florida jointly implemented a protocol using Citracal and Rocaltrol supplementation based on the 1 hour postoperative serum PTH levels.
This was a retrospective chart review of 66 patients who had a total thyroidectomy following protocol implementation and 130 patients operated on prior to the protocol. Our primary aim was to identify hypocalcemia events up to 4 weeks post operatively and hospital re-admissions secondary to severe hypocalcemia. Hypocalcemia was defined as a total calcium level <8 mg/dl. Fisher's exact test was used to analyze associations between variables.
There were 11 episodes of hypocalcemia in the protocol treated group (16.6%) and 27 episodes of hypocalcemia in the control group (20.7%). Central neck dissections did not seem to impact hypocalcemia. Hypocalcemia was noted in 42.8% of pre-protocol cases in which parathyroid glands were noted in pathology specimen compared to a 29.4% hypocalcemia in the protocol group. Four patients in the pre-protocol group were readmitted for severe hypocalcemia. For the post-protocol group there were no readmissions.
Our study confirms that postoperative PTH level <10 pg/mL is a predictor of hypocalcemia following total thyroidectomy (P<0.05). We observed a 4.1% decrease in the rate of hypocalcemia after the implementation of the protocol, even though statistical significance was not achieved (p=0.569). After protocol implementation, no cases of severe hypocalcemia requiring hospitalization were noted.
Thyroid Cancer Thursday Poster Clinical
The surgical management of papillary thyroid microcarcinoma (PTMC), especially regarding the necessity of central/lateral lymph node dissection, remains controversial.
Data from the medical records of consecutive patients diagnosed with PTMC at our center over a 15-yr period were analyzed. The surgical approach was investigated in a large group of Chinese patients, focused on the management of lymph node metastasis in PTMC patients.
There were a total of 1989 patients who met the inclusion and exclusion criteria of the study, 1798 patients (90.3%, 1798/1989) underwent lobectomy, and CLND was typically performed as the initial surgical treatment for all patients. The prevalence of central lymph node metastasis (CLNM) and lateral lymph node metastasis (LLNM) in present study was 44.6% and 14.2%, respectively. Our multivariate logistic regression analysis found younger age (less than 45 yr of age), male gender, tumor size greater than 0.6 cm, extrathyroidal extension and multifocal to be associated with CLNM, while younger age (less than 45 yr of age), multifocal, bilateral, extrathyroidal extension, and CLNM to be associated with LLNM. In patients with a solitary primary tumor, location in the upper third of the thyroid lobe was conferred a higher risk for LLNM. Bilateral and extrathyroidal extension were two predictor for recurrence according to multivariate Cox regression analysis, while LLNM (both unilateral and bilateral positive) was not a statistically associated with recurrence.
Lobectomy may be appropriate for most PTMC patients without risk factors, and CLND is recommended in selective patients with risk factors. Given the prevalence of LLNM in PTMC, a thorough inspection for lateral compartment is recommended in PTMC patients with risk factors; from the viewpoint of radical treatment for tumor, prophylactic LLND aiming to remove occult lateral lymph nodes may be an option for PTMC with risk factors. We recommend prospective multicenter studies with long-term follow-up to ascertain the optimal surgical approach for patients with PTMC.
Thyroid Cancer Thursday Poster Clinical
To conduct a meta-analysis to investigate the clinicopathologic factors predictive of central compartment lymph node metastasis (CLNM) in patients diagnosed with papillary thyroid microcarcinoma (PTMC).
PubMed, EMBASE, Ovid, Web of Science, and the Cochrane Library were searched from their inception to September 2013. Published studies that explored the association between clinicopathologic factors and CLNM in PTMC patients were included. From the identified studies, we extracted the number of individuals with or without each risk factor to calculate the CLNM-positive proportions and used fixed/random effects models for the meta-analyses of overall relative risk (RR). Subgroup analyses were also conducted.
A total of 19 eligible studies that included 8345 patients were identified. Meta-analyses revealed that CLNM was associated with male gender (RR=1.36; 95% CI 1.22–1.52), younger age (<45 yr; RR=1.15; 95% CI 1.04–1.27), larger tumor size (more than 5 mm; RR=1.51 95% CI 1.32–1.65), multifocality (RR=1.40; 95% CI 1.27–1.54), and extrathyroidal extension (ETE; RR=1.81; 95% CI 1.34–2.43). Meta-regression analysis indicated that a disparity in the proportion of PTMC patients with CLNM in each study was the main factor resulting in heterogeneity among the 19 studies. However, subgroup analyses based on different cutoff values of the ratio of PTMC to CLNM showed consistent associations between CLNM and larger tumor size (more than 5 mm) or ETE.
Therapeutic or elective ipsilateral central compartment lymph node dissection (CLND) must be considered in PTMC patients presenting with risk factors. We recommend multicenter studies and long-term follow-up to better understand the risk factors and surgical management of PTMC.
Thyroid Cancer Thursday Poster Clinical
Central node metastasis(CNM) of papillary thyroid cancer(PTC) is common, but definite preoperative diagnosis is still a challenge. Infiltrating tumor growth is known to be an indicator of malignant behavior and can be a significant predictor of CNM in PTC. The aim of this study is to investigate preoperative features that are related to CNM and tumor growth pattern.
158 patients who underwent hemi or total thyroidectomy with ipsilateral central neck dissection at Dongguk University Ilsan Hospital were reviewed from 2009 to 2013. Clinical information including gender, age and pathologic characteristics were obtained. We also analyzed preoperative US features of primary tumor including maximal diameter, echogenicity, presence of calcification, and 2-dimensional tumor diameter, i.e tumor aspect ratio. The clinical information and preoperative US features were statistically analyzed for prediction of CNM and tumor growth patterns (infiltrative vs pushing) of PTC.
Of 158 patients, mean age was 46.1 (19–79) and male was 46 (20.1%). Mean tumor size was 10 mm (3–22 mm). CNM and infiltrative tumor growth were noticed in 65 (41.1%) and 128 (81%) patients. Age <45 years and sonographic maximal tumor diameter were independent risk factor for CNM (odd ratio[OR]=2.58; OR=1.21, respectively). In microPTC, only age <45 yr had a significance (OR=3.91). Independent risk factors for infiltrative tumor margin were male gender and 2-dimensional tumor ratio (OR=9.81; OR=6.16, respectively). These results were also noticed in microPTC (OR=7.62; OR=12.20).
This study suggests that younger age and sonographic maximal diameter of primary tumor are reliable predictors for CNM. In addition, male gender and tumor ratio were significant predictors for infiltrative growth pattern of primary tumor, and additionally, tumor ratio had larger OR in microPTC. These predictors are thought to be helpful for preoperative surgical plan for PTC.
Thyroid Cancer Thursday Poster Clinical
Life expectancy has increased continuously and extremely old patients with papillary thyroid carcinoma (EOPTC) has been frequent during recent several years. This study aims to identify surgical outcomes between patients with PTC at a younger age (45≤years <75) and at an older age (≥75 years).
From Jan 1978 to Dec 2008, the total 4312 patients with PTC underwent curative thyroidectomy in YUMC. Of these, 63 patients (1.46%) were aged 75 years or older. We compared the clinico-pathologic characteristics and prognosis between two groups using propensity score matching (1 : 10) and evaluated survival outcomes and identified prognostic factors.
T4a, N1b node status, and stage IVa were significantly more frequent in EOPTC. Overall, 8 (12.7%) of EOPTC sustained a recurrence after a median follow-up of 35.25 months. Recurrence was occurred significantly more frequently in EOPTC than younger patients (p=0.005). The disease-free survival in EOPTC was significantly shorter than in the younger age (99.37% vs. 85.71%; p<0.001). Old age (p=0.003, OR=3.72), male (p=0.033, OR=2.19), and tumor more than 1 cm (p=0.001, OR=4.562) were independent prognostic factor for recurrence in multivariate analysis. T stage IVa (p=0.041, OR=19.476) were independent prognostic factor for disease-free survival in multivariate analysis.
The general assumption of a poorer prognosis in EOPTC could be confirmed. Therefore, an optimal therapeutic approach is recommended and should not be withheld on the basis of chronological age. If indicated, initial aggressive surgery should be necessary to improve survival.
Patient characteristics
Thyroid Cancer Thursday Poster Clinical
Well-differentiated thyroid cancer (WDTC) incidence is rising in pediatrics, most cancer being papillary (PTC). The prevalence of different mutations underlying WDTC may differ between children and adults. We are expanding on a recently reported pediatric cohort, assessing genotypic variation and correlations with the clinical phenotype of WDTC.
We retrospectively analyzed 43 consecutive tissue blocks from pediatric TC cases (2001–2013). The protocol was IRB approved to analyze these blocks at Quest Diagnostics for commercially available BRAF, NRAS, HRAS and KRAS mutations, and RET/PTC rearrangements (ReAr) in PTC and PAX8/PPARγ fusions in follicular thyroid carcinoma (FTC) or follicular variant of PTC (FVPTC), using validated molecular methods.
Of 43 samples, 40 (30 F, 10 M) were successfully genotyped. Mean age at diagnosis (Dx) was 14.9 (range 7.9–20.8) yrs, most being Hispanic (57.5%) or Caucasian (35%). Mutations were noted in 22/40 (55%). 2/5 cases with FTC had a mutation (PAX8-PPARγ and NRAS (Q61K)). 3/6 females with FVPTC had PAX8/PPARγ fusions. Of 29 subjects with classic PTC, 17 (58.6%) subjects (13 F) had mutations: BRAF in 10/29 (34.5%), 6 (20.7%) with RET/PTC ReAr (5 RET/PTC1+ and 1 RET/PTC3+), and 1 (3.4%) NRAS (Q61K).80% of BRAF mutations were in Hispanics, 20% in Caucasians. 90% of BRAF mutations were in >15 year olds, and 10% in ≤15 yrs. All subjects with RET/PTC ReAr were ≤15 yrs. No significant differences were noted in tumor size, lymph nodes and distant metastasis at Dx or soon after I-131 ablation. Correlation of genotype with response to therapy await longer follow up.
In our pediatric WDTC cohort, BRAF V600E was the most common mutation in PTC, especially in older adolescents of Hispanic descent. BRAF rates vary among the few pediatric cohorts, with higher rates likely reflecting older age distribution. RET/PTC ReAr was less prevalent in this cohort versus prior US pediatric studies. More advanced molecular analysis will likely reveal other types of mutations/ReAr/fusions that can also help evaluate indeterminate FNA specimens. A larger, ethnically diverse pediatric cohort followed long-term is needed to better study genotype-phenotype correlations in TC at Dx and beyond.
Thyroid Cancer Thursday Poster Clinical
Alterations in the thyrotropin receptor (TSHR) gene play an important role in cell proliferation and function. TSHR mutations are reported to occur in 20% to 82% of hyperfunctioning nodules. Since hyperfunctioning nodules are typically benign, fine needle aspiration (FNA) biopsy is frequently deferred. However, a number of follicular thyroid cancers (FTC) harboring TSHR mutations at codons 486, 620, 623, 631, 632, 633 have been reported in a few hyperfunctioning nodule case reports. Despite these findings, the diagnostic use of TSHR mutation testing in FNA specimens has not been systematically studied. We hypothesize that the occurrence of TSHR mutations at specific location within the gene at high allelic frequency confers a high risk of FTC.
We tested 703 consecutive thyroid FNA samples with indeterminate cytology for TSHR mutations using next-generation sequencing, and reviewed records to correlate TSHR mutations with the functional status of each nodule and surgical outcome.
We detected TSHR mutations in 31 (4.4%) nodules, located in exons 281–639 of TSHR, with codon 486 being most commonly affected (8 nodules). Mutations were detected with the allelic frequency ranging from 2 to 45%. Surgical follow-up was available in 15 cases. In 3 nodules, TSHR mutation coexisted with BRAFV600E mutations and these were all papillary thyroid cancers. Among the remaining 12 nodules with isolated TSHR mutations, 9 were benign and 3 were FTC. The FTC mutations occurred in codons 631, 568, 630 with an allelic frequency of 36, 42, 45% respectively. These 3 FTC nodules measured 3.5 cm, 4.3 cm and 3 cm respectively. Hyperthyroidism was confirmed biochemically in 2 of those 3 FTC and the third case had subclinical hyperthyroidism. Of 4 nodules with isolated TSHR mutations with allelic frequency >30%, 3 were FTC, whereas for 9 nodules with TSHR mutations with allelic frequency <30%, all were benign.
TSHR mutations occur rarely (∼4%) in thyroid nodules with indeterminate cytology, but have important diagnostic relevance. Mutations in codons 568–631 occurring with high allelic frequency confer a markedly increased (∼75%) cancer risk, even if the nodule is hyperfunctioning. However low allelic frequency or TSHR mutations in other codons are associated with benign nodules.
Thyroid Cancer Thursday Poster Clinical
Prior studies have shown increased use of imaging over time in the American healthcare system. To date, no one has examined trends in imaging after thyroid cancer diagnosis. We evaluated post diagnosis imaging patterns over time and determined the patient characteristics that correlate with likelihood of imaging.
Using the linked Surveillance Epidemiology and End Results (SEER)-Medicare database, we identified patients diagnosed with localized, regional or distant well-differentiated thyroid cancer (WDTC) between 1991 and 2009. We then reviewed medical claims data and determined use of thyroid ultrasound (US), I-131 scan, or PET scan within 3 years post diagnosis. We evaluated the trend of imaging utilization for the study period using linear regression analysis. Multivariable logistic regression was used to estimate the likelihood of imaging use based on patient characteristics.
23,669 patients with WDTC were included in the analysis. Patients diagnosed after 2001 were more likely to have localized disease (p<0.001) and tumors less than 1 cm (p<0.001). Among patients with localized disease, over time there was increased use of both thyroid US(p=< 0.001) and I-131 scan (p=0.003). Utilization of thyroid US (p=< 0.001) and I-131 scan (p=< 0.001) also grew in patients with regional disease. The distant disease group also had an increase in the number of thyroid US (p=0.001) and I-131 scans (p=0.015) performed. Controlling for patient characteristics, patients diagnosed from 2001–2009 were more likely to have a thyroid US than those diagnosed from 1991–2000 (OR 2.15, 95% CI 2.02–2.28). Patients diagnosed after 2000 were also more likely to have an I-131 scan (OR 1.44, 95% CI 1.35–1.54). PET scan use from 2005–2009, compared to 1996–2004, increased 32.4-fold (p=< 0.001) in the localized disease group, 13.1-fold (p<0.001) in those with regional disease and 33.4-fold (p<0.001) in those with distant WDTC.
Patients diagnosed with WDTC after 2000 were more likely to have smaller, localized cancer. The use of post diagnosis imaging has increased in all patients, regardless of the extent of disease. The largest growth was seen in PET scan, which increased dramatically after 2004.
Thyroid Cancer Thursday Poster Clinical
The incidence of thyroid cancer increased dramatically in the past 20 years in many European countries and in the USA due to a number of factors, including both improved diagnostic techniques and a real increase in the incidence of papillary thyroid carcinoma. Among other significant reasons for the increase, dietary/environmental factors such as iodine deficiency, ionizing radiation, and various endocrine disruptors are being studied. We investigated the number of radiation-induced thyroid cancer in children after Chernobyl in Belarus with respect to thyroid radiation dose and concentration of nitrates in open well water.
Multivariate linear regression model was used.
According to the UNSCEAR 2011 report, the highest collective doses (man Gy) to the thyroid for the populations were in Gomel (321,750), Mogilev (50,020) and Brest (45,170) regions. Prevalence of thyroid cancer in children in 1990–2005 for the cohort aged 0–18 years at exposure per 100,000 population of corresponding age was in Gomel region - 131, in Brest - 67.4 and in Mogilev - 18.3. Despite comparable radiation doses, there is a pronounced difference in the prevalence of childhood thyroid cancer between Brest and Mogilev regions. Average concentration of nitrates in open well water in the early nineties were in Gomel - 112 mg/l, Mogilev - 40 mg/l and Brest - 185 mg/l. Multivariate linear regression model indicated that observed number of cases correlated with both radiation dose (B=1.524, 95%CI: 1.209–1.840, p=0.001) and nitrate concentration (B=1.501, 95%CI: 0.782–2.220, p=0.007).
The prevalence of radiation-induced thyroid cancer matches closely with both the thyroid radiation dose and with the severity of pollution of groundwater with nitrates. Further investigations are necessary to elucidate the combination effect of nitrate (or other environmental pollutants and potential endocrine disruptors) and radiation on modulation of thyroid cancer risk. Such studies may potentially shed light on the increasing rate of the thyroid cancer in the world.
Thyroid Cancer Thursday Poster Clinical
In order to encourage patients' involvement in their own health care plans, some multi-disciplinary teams are choosing a proactive patient partnership approach instead of the traditional patient-centered approach. Our objective was to improve active care for individuals fighting thyroid cancer, through projects elaborated in partnership with patients.
Two patients, who suffered from thyroid cancer, joined the members from the thyroid cancer inter-disciplinary team of the Centre Hospitalier de l'Université de Montréal (CHUM) in a Continuing Improvement Committee (CIC). After our patient-partners mentioned various shortcomings in the announcement of the diagnosis of thyroid cancer, the first project identified by the committee was aimed towards evaluating patients' satisfaction through a survey. The survey was distributed online and in thyroid cancer clinics between October and December 2013. Results were compiled using the Qualtrics software. Results were compiled using the Qualtrics software.
134 patients with thyroid cancer answered. Globally, 28% were not satisfied with the way their diagnosis had been announced, mostly because of lack of information related to their disease, and lack of psychological support. Only 20% had received documentation related to thyroid cancer, and only 25% benefited from psychological support, although most patients wished for a referral. 80% also felt their physician did not take their disease seriously enough.
Integrating patients in the interdisciplinary team helped us better understand the needs of individuals diagnosed with thyroid cancer and target our interventions. Our survey indicated the need for the elaboration of information packages for patients, reviewing how to announce a cancer diagnosis without decreasing the importance of the disease, and improving psychological support for this particular population group. Patients' satisfaction will be periodically reassessed by the CIC.
Thyroid Cancer Thursday Poster Clinical
Bilateral axillo-breast approach (BABA) robotic thyroidectomy have achieved good oncologic outcomes and do not result in neck scars. The purpose of this study was to analyze the influence of body type on the surgical outcomes of BABA robotic total thyroidectomy in papillary thyroid carcinoma.
A total of 347 patients who underwent BABA robotic total thyroidectomy with central lymph node dissection, from January, 2011, through December, 2012, at Seoul National University Hospital, were included in this study. This study was conducted as a retrospective analysis of prospectively collected data. We analyzed association between body type and operation time, hospital stay, postoperative complications, and pathologic details. The body type was described by BMI category, BSA and neck circumference. BMIs were categorized as described by World Health Organization (WHO) classification, and patients were allocated one of three groups [normal and underweight group (NUW), BMI<25 kg/m2; overweight group (OW), 25≤BMI<30 kg/m2; obese group (OB), 30 kg/m2≤BMI]. BSA was calculated by Mosteller formula and Neck circumference was measured horizontally at the level just below the thyroid cartilage on preoperative neck computed tomographic images.
The patients' mean BMI was 22.53±3.22 kg/m2, each BMI group was as follows; 280 patients (80.7%) were NUW group, 57 patients (16.4%) were OW group, and 10 patients (2.9%) were OB group. Only creation of working space time (p=0.013) was correlated significantly with three BMI groups. BSA had positive correlation with creation of working space time (p=0.015, r=0.134). The mean neck circumference was 355.36±25.49 cm, and was correlated with creation of working space time (p=0.039, r=0.114). Postoperative complications such as hypocalcemia, vocal cord palsy, wound complication, and adhesion were not significantly different in the three BMI groups, BSA and neck circumference.
BABA robotic thyroidectomy is safe and effective method in most patients although high BMI patient and larger neck circumference patients need longer creation of working space time in papillary thyroid carcinoma.
Thyroid Cancer Thursday Poster Clinical
Papillary thyroid cancer(PTC) is the commonest pathological type of thyroid cancer with relatively good prognosis. The aim of this study was to examine the clinicopathological and prognostic features of PTC in our institute over a 15-year period.
This study enrolled 2215 consecutive patients with PTC received surgical treatment from 1997 to 2011. We studied the clinical features, management and outcome according to the time of diagnosis: Group I (1997–2001), Group II (2002–2006), and Group III (2007–2011).
No difference in compositions of gender, location, multiplicity of tumor was found in three different periods. Lower percentage of extra-thyroidal invasion rate and lymph node metastasis rate as well as smaller size of tumor were found in the Group II and Group III compared with Group I. According to the AJCC staging, there was a trend towards a higher stage in patients from Group I vs. patients from Groups II and III (stage IV, 10.4% vs. 7.4% and 3.9%, p=0.000). However, no difference in recurrent rate was observed in the three period groups. The overall outcome in terms of 5-year disease free survival (DFS) rate was 91.3%, with 82.7% in Group I, 93.4% in Groups II, and 89.5% in Groups III. The overall outcome in terms of 5-year overall survival (OS) rate was 99.2%, with 98.8% in Group I, 98.8% in Groups II, and 99.6% in Groups III respectively.
Patients diagnosed after 2001 seem to have a better prognosis. This improvement is probably related to earlier diagnosis with smaller tumor size and presentation at earlier tumor stage.
Clinical characteristics. of the patients with BMI of 376 with papillary thyroid carcinoma who underwent bilateral axillo-breast approach robotic total thyroidectomy
SD standard deviation, CND central lymph node dissection, LND lateral lymph node dissection
Clinicopathologic features of the study cohort over three periods
Thyroid Cancer Thursday Poster Clinical
To evaluate the association of category 3, 5, and 6 in Bethesda System for Reporting Thyroid Cytopathology with clinicopathologic prognostic factors and ultrasound (US) features of conventional type of papillary thyroid carcinoma (PTC).
From August 2012 to July 2013, 2300 consecutive patients diagnosed as Bethesda category 3, 5, and 6 on US-guided fine-needle aspiration (FNA) of thyroid nodules underwent surgery and 2005 of 2300 patients diagnosed as conventional type of PTC were included. Preoperative US features were assessed as composition, echogenicity, margin, calcifications, shape, vascularity of thyroid nodules and underlying parenchymal echogenicity. The data about tumor size in histopathologic specimen, extrathyroidal extension, central lymph node (LN) metastasis, lateral LN metastasis of each patient was collected for postoperative features. Multinomial logistic regression was performed to determine the odds ratios (OR) of each variable associated with Bethesda category 3 or 5 based on the reference as category 6.
On multinomial logistic regression of preoperative US features with reference as category 6, malignancies with category 3 and 5 showed smaller size (OR=0.925 and 0.937 in category 3 and 5) and did not show marked hypoechogenicity (OR=0.341 and 0.268 in category 3 and 5) and central vascularity (OR=0.759 in category 5). Malignancies with category 3 and 5 significantly showed macrocalcifications (OR=2.372 and 1.594 in category 3 and 5) and heterogenous parenchyma (OR=1.265 in category 5). On multinomial analysis of postoperative features with reference as category 6, malignancies with category 3 and 5 showed smaller tumor size (OR=0.906 and 0.941 in category 3 and 5). Lateral LN metastasis (OR=2.212 in category 3) were significantly associated with malignancies with category 3.
Although the nodules were surgically diagnosed as conventional type of PTC, their biological behaviors would be different and this might be reflected through Bethesda category 3, 5, and 6. Therefore, Bethesda category 3, 5, and 6 can serve as an ancillary tool to predict prognosis.
Thyroid Imaging Thursday Poster Clinical
To evaluate the diagnostic performance of quantitative parameters obtained from histogram analysis using gray scale ultrasound (US) images in the diagnosis of patients with lymphocytic thyroiditis (LT).
A total of 505 patients (mean age, 43.4±12.2 years; range, 16–85 years) underwent preoperative staging US and thyroid surgery in our institution. Threeblinded radiologists retrospectively reviewed 505 gray scale US imagesand were asked to classify into two categories to decide whether LT exists or not. After two months, each reviewer was asked to repeat with 505 US images whose order were randomly mixed up. Intra- and interobserver variability of three reviewers was anlyzed with the generalized kappa statistic. The indivisual US images were postprocessed with MatLab softwarefor histogram analysis. Four parameters (mean value, standard deviation, skewness and kurtosis) for each case were obtained and the index was calculated from principal component analysis. The diagnostic performances were compared.
Of 505 patients, 125 (24.8%) had LT and 380 (75.2%) had normal thyroid parenchyma. The kappa value of intraobserver variance was ranged from −0.002 to 0.781 and the overall kappa value of interobserver variance was 0.665 and 0.225 in the first and second test, respectively. The sensitivity, specificity, accuracy, positive predictive value, andnegative predictive value of the index from the histogram werer 58.4%, 72.4%, 68.9%, 41.0% and 84.1%, respectively. The index showed the highest areas under the curve (0.6538) and was comparable to the AUC of the reviewers'.
Histogram analysis of gray scale US images provides reliable and quantitative information about LT. The index calculated from histogram analysis can overcome subjectivity and variablility of the performer's assessment to diagnose LT and a further study with technical development would be necessary.
Thyroid Cancer Thursday Poster Clinical
Various staging system or risk stratification system have been used to predict clinical outcome in patients with differentiated thyroid cancer, and age at diagnosis is an important prognostic factor and included in these staging system. However, there are different set of age at diagnosis in these staging systems. To determine the most predictive age at diagnosis that influence differentiated thyroid cancer-specific death in a large patient population.
Patients diagnosed with differentiated thyroid cancer between 1988 and 2010 were selected for the present study from the Surveillance, Epidemiology, and End Results (SEER) registry. We analyzed optimal cut-off point of age estimating overall and thyroid cancer specific death with Youden Index. Multivariate Cox proportional hazards model were applied to assess the hazard ratios (HR) of specific age levels.
Median follow-up time was 5.4 years (range: 0–22.9 years). During the follow-up periods, the proportion of death resulting from thyroid cancer was 1.5% (n=533) and that of death resulting from overall cause was 7.0% (n=2482). A ‘55 years or younger’ criterion with all cause of death and '57 years of younger' criterion with thyroid cancer specific death were the optimal cut-off point of age. The age was the most predictive risk factor for both overall [HR=9.04 (95%CI: 8.26–9.90)] and thyroid cancer specific death [HR=10.02 (95%CI: 8.18–12.28)].
Increasing age was associated with an increased cancer-specific mortality in patients with differentiated thyroid cancer. Cut-off value of age at diagnosis greater than 57 years would be better to predict clinical outcome in differentiated thyroid cancer patients. These results can be useful to identify the patients who should be considered for aggressive treatment and intensive surveillance.
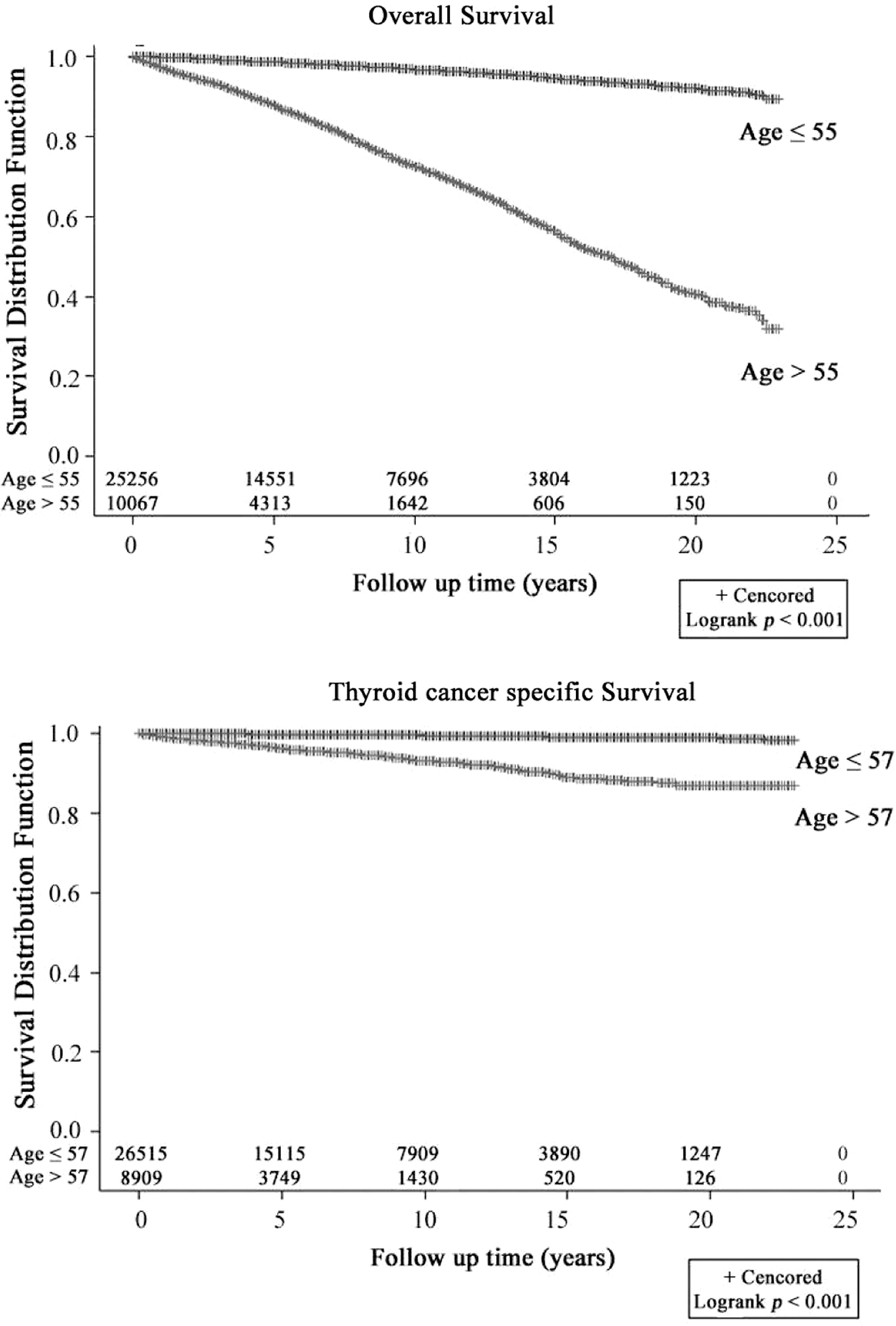
Survival curve for overall survival and thyroid cancer specific survival by age cut-off levels.
Thyroid Cancer Thursday Poster Clinical
Radioactive-iodine remnant ablation (RRA) is commonly used to treat patients with papillary thyroid carcinoma. Predicting the efficacy of RRA is critical for effective treatment planning. The aim of this study was to investigate the factors associated with low dose (30 mCi) RRA success.
A retrospective cohort study was conducted on 691 patients who received low dose RRA. Patients with no remnant thyroid on the follow up whole body scan and low stimulated thyroglobulin (s-Tg) level (<2.0 ng/mL) were deemed as successful treatment cases. Patient demographics, pathologic features, preablative laboratory test, and RAI ablation result were collected.
Initial low-dose RRA was successful in 431 patients (62.3%). RRA success was associated with multifocality (39.3% vs. 47.1%, P=0.045) and bilaterality (23.1% vs. 30.1%, P=0.041) of the primary tumor, coexisting Hashimoto thyroiditis (HT; 25.5% vs. 40.8%, P<0.001), and low pre-ablation s-Tg (1.5±2.4 vs. 6.5±19.0, P<0.001). On multivariate logistic regression analysis, both coexisting HT and pre-ablation s-Tg retained statistical significance. The odds ratio of RRA failure significantly increased by 2.86-fold in patients with coexisting HT; no relationship was observed between TgAb levels and RRA success. Increased pre-ablation s-Tg was also associated with RRA failure (odds ratio, 1.23). In order to annul the effect of thyroglobulin antibody, which causes variation in s-Tg measurement, a subgroup analysis was performed for patients with low TgAb level (<100 IU/mL); the results showed no difference to those of total patients.
These data suggest that coexisting HT is a negative predictive factor for low-dose RRA success. Although minimum doses of RRA are preferred, a tailored approach might be more appropriate for patients with coexisting HT.
Thyroid Cancer Thursday Poster Clinical
Postoperative hypocalcemia is the most common complications after total thyroidectomy but permanent hypocalcemia is very serious problem because it requires life-long treatment. It is not usually easy to predict which patients are prone to the development of permanent hypocalcemia. Measurment of perioperative intact parathyroid hormone(iPTH) may prove helpful in the identification of patients who are at risk for postthyroidectomy hypocalcemia.
We conducted a retrospective investigation utilizing serial iPTH measurement to evaluate the difference in recovery of parathyroid function among 3 groups. Based on the serum levels of iPTH, patients with undetectable level at 2 hours after operation(immediate hypoparathyroidism) were classified into three groups : 1) undetectable, 2) detectable but subnormal, 3) only one time normal level. The level of iPTH and serum calcium were serially measured every 2 month.
Immediate hypoparathyroidism was seen in 65 patients out of 240 total thyroidectomies (27.1%). Of those patients, 19 (29.2%) developed permanent hypoparathyroidism. The incidence of development to permanent hypoparathyroidism was 30%(9/30), 40.9%(9/22), and 7.7%(1/13) in group 1,2,3 respectively (p=0.044). The recovering period was usually 2 to 4 months after surgery in transient hypoparathyroidism. Despite of calcium replacement, 54.5% of patients in group 2 showed subnormal level of serum calcium and hypocalcemic symptoms. 2 patients(3.1%) showed hypocalcemia in spite of normal iPTH level.
An intraoperative injury to vasculariztion of parathyroid glands might be major contributing factor to the development of permanent hypoparathyroidism. Continuous calcium and vitamin D replacement needs until at least 4 months in transient hypoparathyroidism. Serial measurement of serum iPTH might be used as predictive marker in characterizing the high risk of permanent hypoparathyroidism. Immediate subnormal level of iPTH might be high risk for permanent hypoparathyroidism and hypocalcemia.
Thyroid Cancer Thursday Poster Clinical
The utility of preoperative (pre-op) serum thyroglobulin (Tg) in patients with thyroid nodules is unproven. There is evidence in the literature that elevated Tg after thyroidectomy for differentiated thyroid cancer (DTC) suggests the presence of persistent/recurrent disease. To the authors' knowledge, there is no study looking at the value of elevated pre-op Tg in predicting the presence of metastases of DTC. This study aimed to investigate the correlation between pre-op Tg and the presence of distant metastases in patients with DTC.
This was a retrospective study of adult patients with benign or malignant thyroid disease who underwent thyroidectomy between 2004 and 2009 at a single academic center. Patients with positive Tg antibodies were excluded. The relationship between Tg levels and extent of disease at presentation was analyzed. Statistical analyses were performed using t test for continous variables, chi-square test for nominal data and non-parametric statistical tests for skewed distributions of data.
There were 326 eligible patients. Thyroid cancer was diagnosed in 250 patients of whom 243 had DTC. Median pre-op Tg level was 82.0 ng/mL (0.2,108000.0). Sixty-three (25%) patients had distant metastases. At initial presentation, pre-op Tg failed to predict the presence of metastases (Median: 59.9 ng/mL for metastatic vs. 73.3 ng/mL for non-metastatic; p=0.88). Assessment for the ability of Tg>500 ng/mL to predict metastases showed a sensitivity of 14% and a positive predictive value (PPV) of 26%. For Tg>1000 ng/mL, sensitivity was 7% and PPV was 27%.
This study confirmed that pre-op Tg levels did not show any correlation with the extent of disease in patients presenting with DTC.
Thyroid Cancer Thursday Poster Clinical
Cervical lymph node (LN) metastases from well-differentiated thyroid carcinoma (WDTC) can be detected by their ability to concentrate radioactive iodine, fine needle aspiration (FNA) cytology and, more recently by thyroglobulin (Tg) determination in needle washings from FNA samples (FNA-Tg). Previous research investigating the diagnostic accuracy of the latter method consisted of small cohorts of patients. The aim was to assess the ability of FNA-Tg, FNA cytology (FNA-cyto) or both combined to predict positive histology results.
We conducted a retrospective study and reviewed 388 US-guided FNA biopsies of sonographically-suspicious cervical lymph nodes from 351 patients between January 2007 and March 2014. We excluded all cases other than WDTC as well as those with no results of FNA-Tg. FNA-Tg and ratio of FNA-Tg/serum Tg were correlated with final histology when available. Nonparametric receiver operating characteristic (ROC) curves were created and area under the curve (AUC) was calculated. The point with the best combined sensitivity and specificity was chosen as the optimal cut-point.
There were 203 FNA biopsies with available FNA-Tg results; of these, 190 had clinical follow up and only 106 records had true surgical results. FNA-Tg level of 29 (ng/mL) showed the best combination of sensitivity and specificity for predicting malignant histology. This cut-off had a specificity of 100%. A combination of positive FNA-Tg OR positive FNA-cyto provided the highest sensitivity (0.98) and lowest specificity (0.88–0.92). Requiring both FNA-Tg AND FNA-cyto to be positive (Tg AND Cyto) resulted in the lowest sensitivity (0.79). Among surgically-confirmed cases, this combination had the highest specificity (100%). Positive cytology was significantly more likely for W/AP ratio <2 (p=0.032). A similar relationship was observed using FNA-Tg results (p=0.023). For all measures, a history of more advanced node staging was associated with a likelihood of a positive FNA.
Given these findings, it is reasonable to send FNA-cyto first and, if negative or non-diagnostic, proceed with FNA-Tg measurement in a patient with suspected LN metastasis from WDTC.
Thyroid Cancer Thursday Poster Clinical
We investigated the clinical value of TSH-stimulated serum thyroglobulin (sTg) for predicting the malignant potential of cervical lymph nodes with F-18 fluorodeoxyglucose uptake (FDG-avid LNs) and their responsiveness to I-131 ablation therapy (IAT) in papillary thyroid cancer patients.
We enrolled 49 patients who underwent total thyroidectomy and showed FDG-avid LNs incidentally detected on PET/CT before IAT. FDG-avid LNs were followed up with a pathologic or imaging diagnosis. According to follow-up results, we classified FDG-avid LNs into two groups; metastatic LNs (group A) and benign LNs (group B). We analyzed the difference of clinical or histopathologic variables at the time of IAT (such as age, gender, pT stage, pN stage, LN location, serum sTg level, maxSUV and size of each FDG-avid LN) between two groups and investigated which factors among them were significant in predicting group A. In addition, the responsiveness to IAT was assessed by intensity of iodine uptake in posttherapeutic scan and reduction of LN size in follow-up studies.
Twenty of 49 patients were classified in group A. On univariate analyses, sTg (median level: 21.5 ng/mL vs. 1.0 ng/mL, P=0.001), maxSUV of FDG-avid LN (5.94±6.01 vs. 3.32±1.04, P=0.043), the frequency of pT3-4 (P=0.032), pN1b (P=0.004), FDG-avid LN located mid to lower neck compartments (P=0.011) were significantly higher in group A than in group B. Among the 5 variables, sTg level was the only significant variable to predict metastatic LNs on multivariate analyses (odd ratio, 1.86; 95% confidence interval, 1.14–3.06; P=0.014). An ROC curve showed that sTg of 6.0 ng/mL was the optimal cutoff for predicting metastatic LNs (sensitivity, 95.0%; specificity, 93.1%; area under curve, 0.971; SE, 0.0223). These metastatic LNs showed neither significant iodine uptake nor the change of their size in follow-up studies (P=0.251).
sTg was a significant variable to predict malignant potential of FDG-avid cervical LNs. Most of FDG-avid LNs with high level of sTg were metastatic LNs and were resistant to IAT.
Thyroid Cancer Thursday Poster Clinical
We investigated the clinical value of preoperative F-18 fluorodeoxyglucose (FDG) PET/CT for predicting recurrence after I-131 ablation therapy (IAT) in papillary thyroid cancer patients.
This retrospective study included 152 patients who underwent preoperative FDG PET/CT and total thyroidectomy with IAT. FDG uptake was evaluated in primary lesion of thyroid gland and defined as FDG-positive if there was a discernible focal uptake compared with surrounding thyroid tissues. Metastatic lymph node ratio (MLNR) was calculated as follows: number of metastatic lymph nodes/number of removed cervical lymph nodes. We investigated which factors among clinicopathologic variables (gender, age, TNM stage, FDG uptake and MLNR) were significant for predicting recurrence.
Of the 152 patients, 8 (5.3%) developed recurrence in thyroid bed or cervical lymph nodes. On univariate analyses, TNM stage (P=0.014) and MLNR (P<0.001) were associated with recurrence. Among 2 variables, MLNR was the only significant factor to predict recurrence on multivariate analyses (odd ratio, 866.91; 95% confidence interval, 31.56-23809.91; P<0.001). In high MLNR (>0.4), there was a significant difference in the prevalence of recurrence between FDG-positive and FDG-negative groups (41.2% vs. 7.1%; P=0.045).
FDG-positivity in primary lesion provided additional prognostic information in high MLNR. Further studies are necessary to assess the predictive role of preoperative FDG PET/CT in papillary thyroid cancer patients.
Thyroid Cancer Thursday Poster Clinical
To identify whether total tumor diameter (TTD) would predict central neck lymph node metastases (LNM) in papillary thyroid microcarcinoma (PTMC).
Patients who underwent total thyroidectomy with central neck dissection and had a pathologic diagnosis of PTMC between 2003 and 2013 at Wuhan Union Hospital were identified. The frequency of LNM was retrospectively analyzed according to the clinicopathological features. For multifocal lesions, total tumor diameter(TTD) was calculated as the sum of the maximal diameter of each lesion.
492 patients had been included for analysis. The proportion of LNM was not significantly different between multifocal PTMCs with with TTD<1 cm and unifocal tumors with diameter <1 cm (p=0.612). However, LNM frequency was significantly higher in multifocal PTMCs with TTD>1 cm than unifocal tumors with diameter≤1 cm (p=0.021). In addition, LNM were significantly more likely to appear in male patients (p=0.003) and patients younger than 45 years old (p=0.00). But we found that the differeces between LNM with or without capsular invasion (p=0.391) was not dramatic.
TTD>1 cm in Multifocal PTMC is a high risk of lymph node metastases. Routine central neck dissection is recommended in PTMCs with TTD>1 cm.
Thyroid Cancer Thursday Poster Clinical
Evaluation and promotion of health is widely accepted in Japan.
Forty three hundred and sixty-five successive Japanese women received thyroid cancer examination using with ultrasound for four years from December, 2009 to November, 2013. Pre-operative diagnosis of papillary thyroid cancer was made by aspiration cytology and/or needle core biopsy. Follicular carcinoma was diagnosed after surgery.
Ninety-nine patients (23–73 years; median, 55 years) with thyroid cancer (88 patients with papillary carcinoma, a patient with follicular carcinoma) were found. The incidence of thyroid cancer was 2.3%. Diameters of nodules on US ranged from 4 mm to 30 mm (median, 6 mm), and 89 of 99 nodules (90%) were equal to or less than 10 mm. None of them had distant metastases. Nineteen patients (6 patients, <45 years; 13 patients >=45 years) have been in observation as they have tumors less than 10 mm (4–8 mm) in diameter and have no findings suggestive of extra-thyroidal invasion or lymph node metastases. Eighty patients (22 patients, <45 years; 58 patients >=45 years) were operated on. Cervical lymph nodes were not dissected or not found in surgical materials in 6 patients with papillary microcancer. According to UICC TNM classification, they were classified as follows; 40 patients with pT1a, 1 patient with pT2, 37 patients with pT3, and 2 patients with pT4, respectively. Thirty-two of 70 (46%) papillary microcancer patients presented pEx1, and they were classified as pT3. If the patients in observation are included, the incidence of Ex1 is calculated as 41% (32/89 patients). Cervical lymph node metastases were seen in 41% (26/64 patients) of patients with papillary microcancer.
This study may be helpful to know the incidence of thyroid cancer in Japanese women. There are few numbers of patients, but the extra-thyroidal invasion is not rare in papillary thyroid microcancer.
Results of TNM classification; all patiens were cM0
Thyroid Cancer Thursday Poster Clinical
The objective of this study was (1) to evaluate the usefulness of recombinant human TSH in patient preparation for radioiodine therapy by comparing resultant changes in biochemical parameters, and (2) to determine which patients would most likely benefit from recombinant human TSH, as implied by comparison of these parameter changes between patients with and without the well-established metabolic risk factors diabetes mellitus, hypertension and age.
A total of 512 patients, including 163 prepared by recombinant human TSH and 349 by withdrawal of thyroid hormone, were retrospectively analyzed for any changes between pre-operative and pre-ablation biochemical parameters, and differences in the TSH stimulation methods were noted. Charts were reviewed for the presence of diabetes mellitus and hypertension, and changes in biochemical parameters were also analyzed with respect to these comorbidities and age.
Recombinant humanTSH provided TSH stimulation comparable to withdrawal of thyroid hormone, without the change in biochemical parameters associated with short-term hypothyroidism. Although diabetes mellitus patients showed no significant difference other than an increased susceptibility for hypoglycemia, those with hypertension showed increased levels of liver enzymes. Older patients also showed increased levels of liver enzymes.
It has been well demonstrated that recombinant humanTSH not only provides ample TSH stimulation, but also precludes the biochemical changes associated with hypothyroidism brought on by withdrawal of thyroid hormone. While recombinant human TSH has already been made available on a compassionate use basis for patients with endocrine conditions, our study suggests it may be a promising alternative in patients with hypertension.
Thyroid Cancer Thursday Poster Clinical
The most common complication of thyroid surgery is hypocalcemia. Direct injury to, or devascularization of, the parathyroid glands (PTGs) is generally accepted as the most common reason for post-thyroidectomy hypocalcaemia. Therefore meticulous thyroid dissection and thyroid vessel preservation are required. However incidental parathyroidectomy(IP) is found at experienced surgeon. Potential risk factors of IP identified in individual studies: higher thyroid cancer stage, heavier thyroid specimens and concomitant thyroiditis. It has not been studied that IP is relevant to histological and anatomical microstructure around PTGs. The goal of this study is to investigate the histopathological charateristics of thyroidectomy specimens including IP.
Medical records of 704 patients underwent thyroidectomy in Korea University College of Medicine between 2007 and 2012 were reviewed. 90 patients identified IP in pathologic reports were included. Surgical extent and histopathological features were investigated in IP patients. Conducted histopathological features were as follows: PTGs in the thyroid gland, PTGs out of the thyroid gland, PTGs in the thyroid groove, PTGs nearby vessel and tumor.
31(34.4%) patients with PTGs found in the thyroid gland were identified. 59(65.6%) patients with PTGs presented out of the thyroid gland were found. 13(22%) of the 59 patients were not considered PTGs preservation because of distance between tumor and PTGs. 46(78.0%) patients had more than 5 mm distance between tumors and PTGs. 2(3.4%) of 59 patients had PTGs in the thyroid groove. 27(45.8%) patients were difficult to detach PTGs because it was close to thyroid vessels. In 90 patients, 30(33.3%) were extracted PTGs even though the distance between PTGs and thyroid tumor was more than 5 mm, out of the thyroid groove and far away from the thyroidal vessels.
Surgical extent and histopathological features were significantly related to the IP. Histopathological risk factors of IP were that PTGs presented within thyroid parenchyme, adjacent tumor, in the thyroid groove or close to thyroid vessels. However, 33% patients of IP could be avoidable if we exerted great efforts to preserve PTGs by meticulous thyroid dissection.
Thyroid Cancer Thursday Poster Clinical
Cervical nodal metastases are quite commonly seen in papillary thyroid carcinoma (PTC), as micro- and macrometastases can be found in up to 90% of cases. The initial treatment is thought to be decisive in PTC with cervical nodal metastases, because it is associated with an increase in recurrence rate and may impact negatively on quality of life as well as survival. Almost of all reports about PTC with cervical nodal metastases was focused on finding the pathologic characteristics of tumor after surgery or finding usefulness of ultrasonography(US) and computed tomography(CT) for detection of lymph node metastases. It is very helpful to decide treatment strategy and strength of follow up, if we can predict cervical lymph node metastasis even in the case of clinically negative lymph node metastasis of PTC patients preoperatively. In the present study, we investigated whether the preoperative US and CT findings of the primay tumor could predict the lateral cervical lymph node metastases of PTC.
A retrospective analysis was performed on 860 patients who underwent surgery for PTC between 1990 and 2008. By comparing a group with lateral cervical lymph node metastases (n=298) with a group without lateral cervical lymph node metastases(n=662), the findings of US and CT for the primary tumor of PTC were analyzed.
Tumor size in US was significantly different between PTC with lateral cervical lymph node metastases (1.81 cm) and PTC without that (1.46 cm, p<0.024). The number of suspicious findings for malignancy in US was also significantly different between the two groups (4.15 vs. 2.38, p<0.038). The soft tissue invasion of primary tumor in CT was significantly different between the two groups (39 vs 5, p<0.02).
When the tumor more than 1.5 cm and suspicious findings for malignancy more than 4 were found in US and soft tissue invasion found in CT in preoperative evaluation, physician must try to find the lateral lymph node metastasis intensively, and radioactive iodine ablation could be considered postoperatively. Also, patients with above findings have to be kept watch carefully the recurrence of PTC in lateral cervical lymph nodes during follow-up.
Thyroid Cancer Thursday Poster Clinical
Cryptococcal infection occurs mostly in immunocompromised patients. In a patient with thyroid cancer with metastasis to lungs, development of new pulmonary lesions can pose a diagnostic challenge. We present the first reported case of pulmonary cryptococcosis in a patient with stage 4 papillary thyroid cancer with lung metastasis.
A 50 year old Latin American male with metastatic papillary thyroid cancer was admitted to the hospital with worsening cough and fever of one month duration. Patient has a history of stage 4 T1b N1bM1 papillary thyroid cancer with metastatic disease to the lungs diagnosed in 2011. He underwent total thyroidectomy with central lymph node dissection and received 175 mCi of I-131. He was subsequently started on suppressive levothyroxine therapy. Thyroglobulin was 0.8 with negative anti thyroglobulin antibodies prior to admission. He also has type 2 diabetes with an A1C of 8%. Chest x ray revealed multilobar pneumonia, blood cultures and sputum cultures were negative. He failed to improve clinically on different antibiotic regimens. CT of chest with contrast showed numerous pulmonary nodules measuring up to 4 cm. Worsening of lung metastasis was considered but thyroglobulin levels remained unchanged from before admission. Patient underwent bronchoscopy and bronchial wash was positive for cryptococcus along with positive cryptococcal serum antigen. He was treated with intravenous Amphotericin and fluconazole. He improved clinically and CT chest after 2 months showed marked decrease in size of pulmonary nodules to less than 1.6 cm in size.
Serum thyroglobulin is a highly specific and sensitive tumor marker for detecting persistent or recurrent thyroid cancer and for monitoring clinical status. Our patient had metastatic papillary thyroid cancer with lung metastases who developed cryptococcosis. Unchanged thyroglobulin levels in this patient from before and after the development of new lung lesions prompted further investigations which revealed the diagnosis.
Lung lesions in a patient with metastatic papillary thyroid cancer could be from other coexistent infections like pulmonary cryptococcosis.
Thyroid Cancer Thursday Poster
MTC can occur as part of the autosomal dominant hereditary syndrome multiple endocrine neoplasia type 2 (MEN 2). Most cases of MEN 2 syndromes arise from germline mutations in the RET gene. Although a strong genotype-phenotype correlation has been observed, it has been considered that other genetic modifier loci can be potentially associated with milder phenotypes. It is well known that heritable genomic copy number variation (CNVs) represent a significant source of genetic diversity and may modulate gene expression and predispose an individual to disease. Thus, in this study we aim to investigate whether CNVs, present in the constitutional DNA of a pair of monozygotic twins with p.G533C RET mutation and different clinical features, may contribute to earlier age of onset.
Peripheral blood DNA was independently hybridized using a Genome-Wide SNP Array 6.0 platform and the data were analyzed using Nexus Copy Number software. To identify the possible candidate regions associated with earlier age of onset in a pair of monozygotic twins, one case (age 32 yr) was compared to one control (age 36 yr). The genes present on identified autosomal CNVs were analyzed at Enrichr software, a gene list enrichment analysis tool, to better understand the functional relevance of these genes.
When compared to one another, we identified 29 CNVs specific to the case (11 losses and 18 gains). These CNV regions encompass a total of 20 genes. Importantly, upon gene evaluation, we found overrepresented Gene Ontology (GO) terms associated to galactose metabolism (P=0.008), acute myeloid leukemia (P=0.013) and melanogenesis (P=0.024).
The use of disease-discordant monozygotic twins represents a powerful approach to identify inherited CNVs that may be associated with a specific phenotype. We here show the analysis of a pair of monozygotic twins affected with MTC with differences in their clinical features, mainly related to the age of onset. We here describe CNVs that may act as modifiers and, therefore, may explain the differences observed in monozygotic twins. However, further analyses are still needed to determine the role of these CNVs in the etiological basis of the MTC in a family with MEN 2 and RET germline mutation.
Thyroid Cancer Thursday Poster Translational
Well differentiated thyroid cancer accounts for 95% of thyroid malignancies and has a good prognosis. However, up to 20% of these patients will develop distant metastasis and two-thirds of these patients will be refractory to radioiodine therapy. These patients ultimately have a poor prognosis and the limited treatment options make clinical management particularly difficult. The ubiquitin - proteasome pathway has an important role in thyroid cancer and is a promising target for cancer therapy. The aim of the present study was to investigate the anti-cancer effects of Carfilzomib, a second generation irreversible proteasome inhibitor, in differentiated thyroid cancer cells.
Follicular thyroid cancer cell lines (FTC133, FTC236, and FTC238) and papillary thyroid cancer cell line (TPC1) were treated with different concentrations of Carfilzomib (0 nM - 888 nM), well below clinically achievable plasma concentration (5878 nM). Treatment effects on cell proliferation, apoptosis, cell cycle progression, and three-dimensional multicellular tumor spheroids (MCTS) were analyzed.
Carfilzomib treatment significantly inhibited cellular proliferation, which was dose and time dependent, in all thyroid cancer cell lines regardless of the driver mutation status of the cell line. This effect was observed at concentrations up to 1000-fold lower than the achievable plasma concentration in human. Carfilzomib treatment also induced caspase-dependent apoptosis and G2/M cell cycle arrest. Treatment of FTC133 MCTS with Carfilzomib greatly inhibited tumor growth at concentrations 20-fold lower than the achievable plasma concentrations compared to vehicle.
Carfilzomib exhibits promise as an anti-cancer agent for the treatment of advanced differentiated thyroid cancer. Further investigation into the potential use of Carfilzomib as a new therapeutic agent for differentiated thyroid cancer is warranted.
Thyroid Cancer Thursday Poster Translational
Previous studies detecting mutations in thyroid nodule fine needle aspiration (FNA) material differed with respect to the cytological grading applied to the FNAs, the type of FNA material used, and the prevalence of mutations observed in the samples. Therefore, the aim of the present study was to investigate these differences as possible reasons for the discrepant sensitivities and specificities reported for the “ruling in” approach between the previous studies.
RNA and DNA was extracted from 347 consecutive routine air-dried FNAs (8 non-diagnostic, 106 benign, 163 follicular lesion, 39 suspicious, and 31 malignant) with available histology. PAX8/PPARG and RET/PTC rearrangements were detected by qPCR, while BRAF and RAS mutations were detected by high resolution melting PCR/pyrosequencing.
The presence of a BRAF mutation was associated with carcinoma in 100% of samples, whereas the presence of a RAS mutation was associated with carcinoma in 57% of samples. Histologic re-evaluation of 10 RAS positive follicular adenomas revealed the diagnosis of 3 additional minimally invasive follicular carcinomas. 49% of carcinomas were identified by molecular testing in the group of follicular lesions, which increased the sensitivity from 60% (cytology alone) to 80% (cytology+molecular testing). While FNAs with the cytological diagnosis of a follicular lesion alone had a 28% risk of malignancy, the risk of malignancy significantly increased up to 71% for mutation positive follicular lesions, and decreased to 18% for mutation negative follicular lesions.
Our data suggest that molecular FNA testing improves pre-surgical diagnosis irrespective of using fresh FNA material or air-dried smears. The discrepant sensitivities and specificities reported in previous studies are most likely related to the use of different grading schemes resulting in a different composition of the cytological categories, and a different prevalence of RAS mutations in follicular carcinomas. Moreover, the knowledge of the molecular testing (especially the presence of RAS mutations) might support the histological identification of minimally invasive follicular carcinomas, which is characterized by high inter-observer variation.
Thyroid Cancer Thursday Poster Translational
TERT promoter (C228T and C250T) and BRAF (V600E) mutations have been identified in clinically aggressive thyroid cancers of follicular origin. The aim of this study is to identify the prevalence of TERT promoter and BRAF mutations in advanced differentiated thyroid cancers (DTC) that are associated with distant metastasis (DM) and/or local-regional recurrence (LRR), and to determine if pattern of disease correlates to mutation profile.
After institutional QI/QA approval, TERT promoter and BRAF V600E mutations were identified following PCR-amplification and sequencing of 43 DTC that were specifically associated with DM and/or LRR; 41 were PTC, 1 was FTC, and 1 was HCC. The presence of DM and/or LRR was confirmed histologically.
The mean age at initial diagnosis was 53 years old and 51% were men. Among the 16 patients with LRR only, mean time to recurrence was 40.8 months (range 8–140). Mean follow-up was equivalent in patients with DM or LRR only (9.1 vs. 7.2 years, p=0.3). TERT promoter mutations were identified in 19 DTC (44%), were more common in patients age ≥45 years (49% vs. 17%, p=0.02), and were frequent in patients with DM (17/27, 63%). BRAF V600E was identified in 18 DTC (42%) and the incidence was not dependent on patient age (p=0.2). A coexistent TERT promoter mutation was identified in 9/18 BRAF V600E positive DTC and in this study of patients with advanced disease, 100% had DM. Of the remaining 9 DTC with isolated BRAF V600E, 8 patients had LRR only. Two patients with TERT promoter mutations were found to have LRR alone (10.5%) at follow up of 4.9 and 1.3 years.
BRAF V600E was common in advanced DTC (42%) and in the absence of other somatic mutations, was often identified in DTC associated with LRR only (50%). TERT promoter mutations were also frequently detected in advanced DTC (44%) and were likely present in DTC associated with DM (63%). Somatic mutation profiling of DTC including TERT promoter and BRAF mutation analysis has valuable prognostic utility and may help predict biologic behavior.
Thyroid Cancer Thursday Poster Translational
Organic cation transporter 1 (OCT1) is a membrane transporter that mediates cellular uptake of the antidiabetic drug metformin. Metformin inhibits thyroid cancer cell growth via AMPK-dependent inhibition of mTOR/p70S6K signaling. However, metformin's actions may be limited by low OCT1 expression in cancer cells. We recently demonstrated that medullary thyroid cancer (MTC) cell lines have differential sensitivity to metformin. Since expression of OCT1 predicts cancer cell sensitivity to metformin we examined OCT1 in MTC-derived cell lines and in human MTC samples.
Two human MTC cell lines, TT and MZ-CRC-1, which harbor endogenous C634W or M918T RET mutations, respectively, were examined. Expression of OCT1 was evaluated using quantitative RT PCR and Western blot analysis. Thyroid tissue samples from 62 MTC patients were used for immunostaining with anti-OCT1, and tumors demonstrating immunostaining in more than 50% cells were considered “positive”.
The mRNA level of OCT1 was 7.2 fold higher in TT (metformin-sensitive) compared to MZ-CRC-1 (metformin-resistant) cells. Pharmacological inhibition of MAPK/ERK, PI3K/AKT or mTOR/p70S6K signaling pathways did not affect OCT1 expression in MTC cell lines. In human thyroid tissue samples, positive immunostaining with anti-OCT1 was detected in 2/19 normal thyroid tissue and in 29/55 MTCs (p=0.0012). The level of OCT1 expression did not significantly correlate with patient's age, gender, tumor size, and presence of vascular invasion or metastases. The intensity of OCT1 immunostaining was not significantly different between MTCs harboring RET mutations and RET-negative tumors.
In the present study, we demonstrate that OCT1 is differentially expressed in human MTCs independent of RET mutation status. These data suggest that measuring OCT1 expression in MTC tissue could serve as a predictive biomarker of response to metformin, and can be used to help identify patients for enrollment in clinical trials with metformin.
Thyroid Hormone Action Thursday Poster Basic
Thyroid hormone receptor (TR) isoforms TRα1 and TRβ1 are expressed in the heart. While it is accepted that TRα1 has a marked effect on myocardial contractility the role of TRβ1 remains incompletely understood. Furthermore, the actions of individual TRs on cardiac metabolism have not been examined. The goal of this study was to investigate the effects of TRs on expression of key proteins involved in glucose and fatty acid (FA) metabolism.
We used hearts from TRα1 and TRβ KO mice and analyzed protein expression.
Results obtained for proteins involved in glucose metabolism show that protein levels of pyruvate dehydrogenase kinase (PDHK) decreased by 60% (P<0.05) in TRβ KO hearts. In contrast, PDHK did not change in the TRα1 KO heart. Moreover, the insulin-signaling pathway was altered in the TRβ KO heart with two-fold increase in phosphorylated insulin receptor substrate 1 (p-IRS-1, Ser307) while in the TRα1 KO heart p-IRS-1 was decreased by 50% (P<0.05). In addition, phospho-Akt-1 and phosphorylated Akt substrate of 160 kDa were increased two-fold after TRβ1 deletion but no change was observed in the TRα1 KO heart (P<0.05). The glucose transporter GLUT-4 increased two-fold at the mRNA and protein levels in the heart of TRβ KO mice with no changes in TRα1 KO. Regarding proteins involved in FA metabolism we found that TRβ deletion reduced cardiac mRNA levels of the FA transporter Fatp-1 and Fatp-3 by 50% (P<0.05), indicating a reduced FA uptake. TRα1 deletion decreased Fatp-1 mRNA by 50%, but increased Fatp-3 and Fatp-4 (five-fold and 30% respectively, P<0.05). In addition, the AMPK pathway, which stimulates FA oxidation, was inhibited by 33% only in the TRβ KO heart.
We demonstrated that deletion of TRβ markedly alters the expression of key factors that regulate glucose and FA oxidation in the heart. Our results suggest that TRβ has significant effects on cardiac metabolism in contrast to minor or no effects of TRα1. In addition TRβ effects favor fatty acid oxidation over glucose oxidation in the heart.
Thyroid Hormone Action Thursday Poster Basic
Nonalcoholic fatty liver disease (NAFLD) is the most common liver disorder in Western countries, strongly associated with obesity, insulin resistance, hypertension, and dyslipidemia. Mice with adrenergic receptor β1 knock out (AdrB1KO) kept on a high fat diet (HFD) also develop NAFLD and, in the present study, we asked whether treatment with a Thyroid Hormone Receptor Beta (TRB) agonist, GC-24, would mitigate this condition.
To this effect, AdrB1KO mice were placed on a HFD (40% fat) for 6 weeks and developed obesity with severe dyslipidemia, glucose intolerance, insulin resistance and exhibited structural evidence of steato-hepatitis with severe steatosis and fibrosis. Some of these animals were treated with T3 (30 ng/g BW) or equimolar amounts of GC-24 (17 ng/g BW) i.p. daily for 6 weeks.
Notably, in AdrB1KO mice treatment with T3 or GC-24 prevented the majority of the abnormalities induced by HFD, such as greater body weight gain, dyslipidemia and insulin resistance. However, only treatment with GC-24 prevented steato-hepatitis and lipid accumulation in the hepatocytes in both AdrB1KO and WT mice. In addition, only treatment with T3 corrected fasting hyperglycemia and glucose intolerance in AdrB1KO mice, with GC-24 only having a partial effect.
We conclude that stimulation of TRB with a selective agonist has beneficial metabolic effects on an animal model of NAFLD.
Thyroid Hormone Action Thursday Poster Clinical
Longitudinal studies on bone decline in ethnic Korean are sparse, especially for healthy aged women. We performed a retrospective longitudinal study to evaluate the relationship between blood tests including thyroid function tests and bone mass changes at the lumbar spine in Korean healthy women over the age of 40.
The study cohort consisted of Korean healthy women over the age of 40 who had undergone comprehensive routine health examinations with an average follow-up interval of 2 years. The bone mineral density(BMD) at the lumbar spine was measured with dual-energy X-ray absorptiometry using the same equipment at baseline and follow-up. We examined the relation of following factors at baseline to BMD changes at the lumbar spine: TSH, free thyroxine, total triiodothyronine(T3), age, alcohol use, smoking, weight, and LDL cholesterol.
Six hundred and thirty-nine subjects (461 premenopausal women, 178 postmenopausal women) without diseases or medication known to bone metabolism undertook baseline and follow-up evaluations. The annual percentage change in BMD at the lumbar spine was greater in 178 postmenopausal women than 461 premenopausal women (−1.17%/year Versus −0.42%/year). The annual percentage changes in BMD at the lumbar spine showed a significant negative correlation with the age, T3, and LDL cholesterol, but a significant positive correlation with TSH in 639 subjects. However, in analyzing the subgroups according to the menopause, the significant positive correlation between the annual percentage change in BMD and TSH was further strengthened, but the significant negative correlation with T3 disappeared in 461 premenopausal women. In multiple stepwise linear regression analyses, the annual percentage change in BMD at the lumbar spine was associated with TSH(standardized coefficient=0.101, p value=0.08) and age(standardized coefficient=−0.298, P value=0.001).
In the study population of Korean healthy women over The Age of 40, TSH was positively associated with the annual percentage changes in bone mineral density at the lumbar spine, suggesting that it may have implication as a marker for bone mineral changes in premenopausal women over the age of 40.
Thyroid Hormone Action Thursday Poster Translational
Mesenchymal stem cells (MSCs) are actively recruited to growing tumour stroma, where they support tumour vasculature and form the tumour's fibrovascular network. Thyroid hormones may influence the hypoxia response network in the tumour microenvironment by stimulating hypoxia inducible factor- (HIF-) 1α expression mediated through non-genomic mechanisms via integrin αvβ3. To improve our understanding of thyroid hormone action in the tumour stroma, we examined the effects of T3, T4 and the integrin-specific inhibitor tetrac on the hypoxia response network in vitro.
Primary human bone marrow-derived MSCs were treated with 1, 10 or 100 nM T3 or 10, 100 or 1000 nM T4 for 24 hours with or without 100 nM tetrac. A subset of cells was additionally treated with hepatocellular carcinoma (HCC) cell-conditioned medium to mimic tumour microenvironment in vitro. The expression of HIF-1α and HIF-responsive genes was analysed by quantitative real time PCR.
Treatment of MSCs with T3 and T4 in the presence of HCC cell-conditioned medium led to increased mRNA levels both for HIF-1α and HIF-responsive genes compared to cells treated with HCC cell-conditioned medium alone. Strongest effects were observed after treatment with 1 nM T3 and 100 nM T4, respectively. HIF-1α expression was increased 2.3- (T3) and 3.5-fold (T4), vascular endothelial growth factor 1.6- (T3) and 1.8-fold (T4), transforming growth factor β1 1.7- (T3) and 1.6-fold (T4), interleukin 6 2.2- (T3) and 2.3-fold (T4) and stromal derived factor 1 2.5- (T3) and 1.9-fold (T4). All the increases in expression levels were found to be tetrac-dependent and therefore integrin αvβ3-mediated. MSCs treated only with T3 or T4 showed the same gene expression levels as untreated control cells, leading to the conclusion that only the simultaneous influence of tumour signals and thyroid hormones increase the activation of the hypoxia response network in MSCs.
Our data suggest that thyroid hormones T3 and T4 influence the activation of the hypoxia response network in an integrin-dependent fashion. These studies will increase our understanding of the critical role of thyroid hormones in the regulation of tumour stroma formation in the context of hypoxia-induced angiogenesis.
Thyroid Hormone Metabolism & Regulation Thursday Poster Clinical
Non-thyroidal illness syndrome (NTIS) is a decrease in thyroid hormone levels, specifically T3, in response to severe illness. Although it is believed to be a protective compensatory response to illness, T3 is critical for cardiac myocyte function; thus, NTIS may be maladaptive in acute congestive heart failure (CHF). We hypothesized that the presence of NTIS in patients who are hospitalized for acute CHF will correlate with worse outcomes, specifically increased length of stay in the hospital (LOS), ICU admission, need for mechanical ventilation or vasopressor support, and readmission within 30 days of discharge, compared to patients without NTIS.
We prospectively enrolled 117 hospitalized patients with acute CHF. Demographic, laboratory and radiologic data were collected, and thyroid hormone levels were tested using serum obtained upon presentation. Subjects were classified as having NTIS if free T3 (FT3) was below the normal value without increased thyroid stimulating hormone levels. Clinical outcomes were then compared in subjects with and without NTIS.
Of the 117 subjects, 54 (46%) had low FT3 levels and 63 (54%) had normal FT3 levels. There was no significant difference in ejection fraction, serum creatinine, or age between the two groups. Compared to patients with normal FT3, patients with a low FT3 had higher APACHE II scores (median 12 vs. 9, p=0.01), and lower serum albumin (3.44 vs 3.66, p=0.007). Low FT3 predicted increased median LOS (11 days vs 7 days, p=< 0.0001), need for ICU admission (39% vs 17%, p=0.009), and use of vasopressors or inotropes (20% vs 5%, p=0.05). There was no significant difference between groups in rates of mechanical ventilation or readmission within 30 days of discharge. Using multivariate analysis, low FT3 was independently correlated with a 39% increase in LOS (p=0.01), while APACHE II score was not independently correlated with increased LOS (p=0.12).
In patients hospitalized for acute CHF, the presence of NTIS predicts increased LOS and need for ICU admission. Our results support the hypothesis that low levels of FT3 may contribute to the pathophysiology of acute CHF and thus is maladaptive in this setting.
Thyroid Imaging Thursday Poster Clinical
Since the spinal accessory nerve (SAN) has a relatively long and superficial course in the neck, it is vulnerable during procedures. US-guided core needle biopsy (CNB) and radiofrequency ablation (RFA) have recently become widely used for treating neck tumours. There have been several reports of SAN injury during lymph node biopsies. In addition, the possibility of SAN injury was also suggested during RFA of recurrent thyroid cancers. Since many lymph nodes may be located near the course of the SAN, the nerve can be damaged during US-guided procedures such as CNB or RFA. To avoid SAN injury during US-guided procedures, continuous US monitoring of the SAN, including matching of nerve location with lymph node level, is required. This study intended to evaluate the feasibility of US detection of the SAN and to validate the US features.
Fifty participants with 100 SANs were enrolled in this study. The SAN was traced from the trapezius muscle to the upper neck and was identified by a hypoechoic linear structure without colour Doppler flow. The ultrasound characteristics of the SAN, such as visibility, size, relationship with adjacent structures, and its correlation with lymph node levels, were evaluated.
The SAN was identified in 96–100% in each segment. The mean size of the SAN was 0.54±0.09 mm (range, 0.4 – 0.8 mm) and similar in size at each segment. Regarding the relationship with sternocleidomastoideus muscle, 38% were passing deep to the sternal head and superficial to its clavicular head of SCM, and 62% were deep to both heads. In every visible case, the SAN was detected in fat layer between trapezius muscle and levator scapulae muscle. Among them, 90.8% of the SAN were also traced until the branch into trapezius muscle. The SAN was found in level II, III, IV, VA and VB on US; however the SAN is not found in level I or VI.
Continuous ultrasound monitoring of the SAN and its correlation with lymph node levels is available in most patients. Our current findings may assist in the future prevention of SAN injury during ultrasound-guided procedures such as RFA of recurrent thyroid cancers.
Thyroid Imaging Thursday Poster Clinical
Comprehensive neck ultrasound examination has become an essential component of preoperative workup for patients with thyroid cancer. Regional cervical lymph nodes may be involved in cases of Hashimoto's thyroiditis. This study seeks to examine the sonographic pattern of lymph nodes in patients with Hashimoto's thyroiditis.
This is a retrospective study looking at patients with confirmed diagnosis of Hashimoto's thyroiditis on final surgical pathology, who underwent preoperative comprehensive neck ultrasound. We compared preoperative ultrasound for patients with Hashimoto's thyroiditis to patients with goiter. Data collected included number of cervical lymph nodes, cervical level (I-VI), size (short-axis diameter, long-axis diameter, short-axis:long-axis ratio), and presence or absence of fatty hilum.
We included a total of 150 patients, 97 patients with Hashimoto's thyroiditis to 53 patients with goiter. Patients with Hashimoto's thyroiditis had a higher number of total cervical lymph nodes than the control group (1.33±2.02 vs. 0.52±0.98; p<0.007), with higher incidence in level I (0.23±0.64 vs. 0.04±0.19; p=0.004) and level III (0.52±1.1 vs. 0.19±0.4; p<0.001). A significant difference in size was found in level III lymph node short axis diameter (3.35±1.62 vs. 6.2±2.86; p=0.001) and level III short-long axis diameter ratio (0.38±0.12 vs. 0.61±0.18; p<0.001).
Hashimoto's thyroiditis seems to be associated with an ultrasonographic pattern of increased number of cervical lymph nodes, particularly in level III.
Thyroid Nodules & Goiter Thursday Poster
Fine needle aspiration (FNA) of thyroid is the most widely utilized tool for detection of malignancy, however a significant proportion may return as either non-diagnostic or indeterminate. We aimed to evaluate the rates of non-diagnostic and indeterminate results of ultrasound-guided FNA performed at our institution, and assess the outcome of current approach in further evaluation and management of patients with above results as a quality improvement project.
Retrospective analysis of 150 charts of patients who underwent FNA at a single academic center (Diabetes Endocrinology of Western NY) performed by a single supervising attending and fellow physicians between July 2010 and December 2013.
Of the 150 patients undergoing FNA of 202 nodules, the pathology results were as follows - 139 benign (69%), 6 malignant (3%), 25 non-diagnostic (12%), and 32 indeterminate (16%). Outcomes of 26 patients (32 nodules) with indeterminate results were reviewed. Slides for 20 patients were re-reviewed at referral site, of which 13/20 was concordant as indeterminate, however a significant number were read as benign (6/20) or non-diagnostic (1/20). 11/13 patients with indeterminate results had re-biopsy at referral center, 1/13 had surgery (symptomatic goiter) and another(1/13) is still waiting for follow-up. Of patients who had re-biopsy, 2/11 were benign, 5/11 were indeterminate and 4/11 were malignant. Few patients (4/26) refused further evaluation or were lost to follow up. One (1/26) patient underwent repeat FNA at our center which one benign and another (1/26) was referred for surgery due to concomitant malignancy on other nodules.
The FNAs were performed by fellows and a single supervising attending with up to 2 passes per nodule and no bedside microscopic review of specimen for adequacy. The rates of indeterminate and non-diagnostic pathology were comparable to reported nationwide rates. Most patients with indeterminate pathology were referred to tertiary cancer center. We observed significant variation in the pathology results between the primary site and referral site with 35% discordance. Hence re-review of slides of indeterminate results is an important step prior to proceeding with repeat biopsy or surgery.
Thyroid Nodules & Goiter Thursday Poster Clinical
Hypermetabolic thyroid nodules detected on PET scan have a higher risk of malignancy (ROM) than PET-negative nodules (30 – 50%), but it is unknown how hypermetabolism affects the ROM within cytology categories. We assessed the cytological and histological results of PET-positive thyroid nodules seen at Moffitt Cancer Center over the last 5.5 years.
We reviewed the records of patients whose thyroid fine needle aspiration (FNA) was performed at our Institution, between October 2008 and May 2014. A total of 2112 FNA were performed on 1817 thyroid nodules, 470 of which were resected and had histological information available (“control group”). We also reviewed the records of patients with a diagnosis of thyroid nodule (ICD-9 241.0) who underwent PET scanning between July 2007 and June 2013. We selected patients whose hypermetabolic thyroid nodules underwent biopsy within 1 year before or after the scan (“study group”). Cytopathology was classified according to the Bethesda system.
We identified 224 biopsied hypermetabolic nodules. The distribution of cytology results and their comparison to the “control group” are shown in Table 1, along with the proportion of nodules resected and the estimated ROM for each Bethesda category. Significantly more nodules were classified as follicular neoplasm/Hurthle cell neoplasm (B-IV) and malignant (B-VI) in the “study group” than in the “control group” (P<0.05), but no difference in the rate of atypia of undetermined significance (B-III). Amongst patients with a PET positive nodule, those with B-III, B-IV and B-VI were less likely to undergo surgery than the equivalent cytology group in the control patients, presumably because of comorbidity, including other active malignancies. However, the ROM for the B-III and B-IV categories was significantly higher in PET-positive nodules than in the “control group”.
Columns in grey: data of the PET group (hypermetabolic nodules in the PET scan); columns in white data of the control group (based on cytology of 1817 nodules read at our Institution between October 2008 and May 2014). B-I=unsatisfactory; B-II=benign; B-III=Atypia of undetermined significance; B-IV=Follicular neoplasm/Hurthle cell neoplasm; B-V=suspicious for malignancy; B-VI=malignant. “# PET group” and “# control group”: number of nodules classified in each Bethesda category in both groups. “# resected PET group” and “# resected control group”: number of nodules excised in each Bethesda category in both groups. “ROM PET group” and “ROM control group”: Risk of malignancy in each Bethesda category in both groups (based on histology of resected nodules).
excluded metastasis to the thyroid.
The increased ROM of PET positive nodules is related both to fewer specimens with benign cytology and to an increase in the ROM of indeterminate cytology. These data have important implications for the management of patients with cytologically indeterminate PET-positive nodules, and for the interpretation of molecular markers applied to these nodules.
Thyroid Nodules & Goiter Thursday Poster Clinical
Between 70–80% of differentiated thyroid cancers have point mutations in BRAF or RAS, or a PAX8/PPARγ or RET/PTC rearrangement. These mutations can be detected in fine needle aspiration (FNA) specimens using an oncogene panel marketed as miRInform™, by Asuragen Inc. Several studies have evaluated the detection of these mutations in FNA material. We now report the first independent study of the performance of the miRInform™ panel, in an Academic Center.
In this IRB approved study, we reviewed the medical records and pathologic outcomes of all patients with a thyroid cytology specimen sent for miRInform™ testing at Moffitt Cancer Center, before May 30th 2014. Cytology was classified according to the Bethesda system for reporting thyroid cytopathology (Bethesda).
Seventy-eight samples, from 76 nodules, in 70 patients have been sent for miRInform™ testing between August 2012 and May 2014 (Table 1). Amongst the 31 Bethesda-III nodules (Atypia/FLUS), none exhibited a mutation. Ten of these have undergone surgery, 3 of which were malignant (30%), yielding a negative predictive value (NPV) of between 70% and 90%. Amongst 36 Bethesda-IV nodules (Follicular or Hurthle Cell Neoplasm), 10 mutations were identified in 9 nodules. 13 nodules in the Bethesda-IV group have been resected; malignancy was identified in 5 of 6 mutation-positive and in 2 of 7 mutation-negative nodules; yielding a positive predictive value (PPV) of 83%.
Table 1.
B-II=benign; B-III=Atypia of undetermined significant; B-IV=Follicular neoplasm/Hurthle cell neoplasm (HCN); B-V=suspicious for malignancy; B-VI=malignant. # miRInform™ samples=number of samples sent for miRInform™ testing; # miRInform™ mutations=number of mutations detected by miRInform™; # sent to surgery=number of nodules that were resected; # malignant histology=number of nodules with histologic confirmation of malignancy; “Overall surgery”=Percentage of nodules excised for each Bethesda category at Moffitt Cancer Center, estimated in 1817 cytology reports from October 2008 to May 2014; “Overall ROM”=Moffitt Cancer Center risk of malignancy for each Bethesda category estimated on 470 surgeries with cytological correlation performed from October 2008 to May 2014.
miRInform™ has limited utility in our Bethesda III group, due to a very low rate of mutations and an inadequate NPV to avoid surgery. We now recommend repeat FNA cytology and consideration of diagnostic lobectomy for these patients. In Bethesda IV cytology, the high PPV provides the opportunity to offer total thyroidectomy to those patients with a mutation and avoid the need for completion thyroidectomy in these patients. However, the high rate of malignancy in this group means that diagnostic lobectomy is still recommended for mutation negative nodules in the Bethesda-IV category.
Thyroid Nodules & Goiter Thursday Poster Clinical
The effective application of molecular markers to indeterminate thyroid cytology is linked to the pretest risk of malignancy (ROM). In this IRB approved study, we aim to determine the ROM of nodules with indeterminate cytology and therefore the potential utility of molecular marker tests at our Institution.
We reviewed the clinical records of all patients who had thyroid cytopathologic evaluation between October 2008 and May 2014 at our Institution. Thyroid cytology was classified according to the Bethesda System for Reporting Thyroid Cytopathology (Bethesda).
We analyzed 2112 FNA performed on 1817 thyroid nodules. Of these, 470 nodules were resected and had histological information available. The ROM among the indeterminate categories was: 25.6% for Atypia of Undetermined Significance (B-III; 22/86); 32.2% for the Follicular Neoplasms (B-IV; 48/149); and 93.9% for the Suspicious for malignancy (B-V; 31/33). Amongst B-IV lesions, ROM was 24.3% for Hurthle Cell Neoplasms and 35.1% for Follicular Neoplasms. These ROM are higher than reported by the Bethesda Conference, but lie well within the range reported by other specialty thyroid cytopathology groups. This higher than expected ROM reduces the negative predictive value (NPV) and increases the positive predictive value (PPV) of commercially available molecular markers tests. Assuming the reported Sensitivity and Specificity of Veracytes' Afirma™ assay, and of Asuragen's miRInform™ oncogene panel, the expected NPV and PPV are shown in Table 1. Only the Afirma™ assay applied to lesions in the B-III category would approach the generally accepted “less than 5%” residual ROM (NPV ∼95%) required to avoid surgical resection. However, the oncogene panel would offer a high PPV in B-III and B-IV groups, allowing consideration for initial total thyroidectomy in these patients.
Expected Negative and Positive Predictive Values for Veracytes' Afirma™ assay and Asuragen's miRInform™ oncogene panel for the indeterminate Bethesda categories at our Institution
Data calculated on 268 resected nodules with indeterminate cytology and histological correlation at Moffitt Cancer Center from October 2008 to May 2014. The values used for this calculation are: ROM 25.6% for Bethesda III; 32.2% for Bethesda IV; and 35.1% for follicular neoplasms (FN) without Hurthle cell neoplasms (HCN); Afirma™ Sensitivity 90% and Specificity 53% for Bethesda III and Sensitivity 90% and Specificity 49% for Bethesda IV and FN (from Alexander et al, 2012, New England Journal of Medicine). miRInform™ Sensitivity 48% and Specificity 89% for all subgroups (from Beaudenon-Huibregtse et al, 2014, Thyroid).
The currently available commercial molecular markers do not offer a significant advantage to avoid surgery in most patients with indeterminate thyroid cytology, when performed in a specialty cytopathology center. The oncogene panel may have utility in determining the extent of initial surgery in a subset of patients with B-III and B-IV results.
Thyroid Nodules & Goiter Thursday Poster Clinical
The acceptance of any operative or interventional procedures depends on the ability of the surgeon to explain the procedure in detail and associated complications without undue fear to the patient and their relatives. The aim of this prospective randomized study is to establish an ideal model for the surgeon to explain the operative procedure.
We used three models for explaining the procedure of Hemithyroidectomy (removal of diseased lobe plus the isthmus and a cuff of contra lateral lobe and pyramidal lobe if present) for benign nodules using conventional diagram model(2 figures drawn by the surgeon using three colored pens) toy model(thyroid toy made up of plastic and rubber) and using animation model (2 minutes animation video made using Autodesk Maya 3D software). The patients evaluated each model and as well as operative procedure using translated and Validated Modified Patient Satisfaction Questionnaire developed by Croom et al. Each group had 20 patients each after randomization. A single endocrine surgeon using suture less technique performed the operative procedure and no drain was inserted. The explanation of the procedure was given by the same surgeon a week before the operation in the outpatient department. Post operatively all patients discharged on the morning after surgery.
The three groups were similar in the demographic profile. The Mean age in years in three groups were 31.25+−13.5,35.45+−12.8 and 36.6+−11.8 years. Females predominated in all three groups. Most had Left Solitary thyroid nodule (Group-1:18, Group-2: 12 & Group-3: 11). Fine Needle aspiration Cytology in all three groups the most common was colloid. In the Questionnaire out of the 16 items scored by the patients the mean score for Experience with the model (41.85,31.5,18.5) was statistically significant (p<0.000). Other items were not significant.
The toy group and animation group had better idea of the procedure, which was rated using a questionnaire. To conclude the animation model if available shall be the ideal model for explaining the operative procedure. Further studies with large number of patients needed.
Thyroid Cancer Thursday Poster Clinical
Management of undiagnosed and undetermine FNAB results are still problematic. Aim of this study is to determine utility of thyroid nodule aspiration fluid thyroglobulin(Tg) levels at differential diagnosis of undiagnosed or undetermine thyroid nodules.
We enrolled 158 patients who has planned to go to total thyroidectomy at our hospital between 2012–2013. US- guided FNAB was performed by an 22 G syringe. The needle was repeatedly moved inside the nodule and aspirated until the needle hub was filled with material. And then needle was washed out with 1 cc saline for Tg measurement. Patients with post-operative benign patology is called group 1 and malign patology is called group 2.
There was 135 women(%85,5) and 23 men(%14,5). Mean age was 47.8 (21–73) and there was no difference between two groups. Preoperative FNAB results were %27,2 benign, %25,3 undiagnosed (at least twice), %22,8 atype of undefined significance (AUS), %11,4 suspicious for a foliculer neoplazi, %16 suspicious for malignancy and %3,2 malign. Post-operative malignancy rates were %9,3, %20, %27,7, %50, %75 and %100 among FNAB classification groups respectively. Preoperative serum TSH, Tg, anti-Tg levels were similar between two groups. Nodule Tg washout levels mean was 185,3 ng/ml for group 1 and 74,8 ng/ml for group 2 (p:0,016). There was no correlation of nodul Tg between serum Tg, TSH, or tumor size. There was positive weak correlation between nodul Tg and nodule volume(spearman's correlation coeffient :0,272, p:0,01) Levels above 62 ng/dl of nodule wash-out Tg has %79 spesifitivy and %43 sensivity for a benign pathology. Nodule Tg wash-out level of benign cases were significantly high than patients who has malign thyroid pathology independently of serum Tg levels. This study is the first report that suggests thyroid nodule thyroglobuline wash-out levels can be an option at the differansion of benign and malign thyroid lesions.
Nodule Tg wash-out level of benign cases were significantly high than patients who has malign thyroid pathology independently of serum Tg levels. This study is the first report that suggests thyroid nodule thyroglobuline wash-out levels can be an option at the differansion of benign and malign thyroid lesions.
Thyroid Nodules & Goiter Thursday Poster Clinical
Non-diagnostic (ND) results of fine needle aspiration biopsy (FNAB) of thyroid nodules is a frequently encountered clinic problem. We investigated the utility of Core needle Biopsy(CNB) for the nodules that have recurrent ND results.
We enrolled 66 patients who underwent CNB because of at least two ND results of thyroid nodule FNAB. CNB was performed by an endocrinologist using 18 G vacuum-assisted needle with US guide. %10 lidocaine in a sprey formulation was applied for local anesthesia. After removing core biopsy(CB), remaining material inside the needle and CB imprinting were used for preparing smears. CB was preserved in formalin before preparing paraffin blocks. An experienced pathologist examined the specimens and reported according to Bethesda System.
54 women and 12 men with a mean age of 48,3 year were enrolled. The biggest diameter of nodules ranged from 7–110 mm (mean 18.1 mm, median 15.0 mm). CNB yielded a diagnostic result in %92,4 of 66 nodules. % 68,2(n:45) of CNB results were benign. 28 of them has gone to total thyroidectomy(TT), and post-operative pathology revealed 27 benign lesions(%96,4) except one papillary microcarsinoma. %16,7 (n:11) of CNB results were AUS/FLUS. 9 of them has gone to total thyroidectomy and post-operative patology revealed 3 papillary carsinoma(%33,3). There was three folliculer lesions(%4,5) all of which has gone to TT, were benign in postoperative pathological examination. There was one suspicious for malignancy(%1,5) and one medullary thyroid carcinoma (%1,5) diagnosis based on CNB pathology and postoperative pathologies confirmed the diagnoses. For benign pathology specificity was %83,3 and sensitivity was %75. There was no severe complication.
CNB is a useful method with a high diagnostic ability and accuracy for recurrent undiagnosed thyroid nodules.
Thyroid Nodules & Goiter Thursday Poster Clinical
The impact of lymph node metastases on prognosis less clear in papillary thyroid carcinoma (PTC), the aim of this study was to examine whether CLNM for PTC affected long-term prognosis.
All PTC patients identified between January 1995 and December 2007 were analyzed restropectively. CLNM was investigated for the association with cancer-specific survival, locoregional control and distant metastasis. Other clinicopathologic factors and surgical treatments were also obtained and enrolled in the analysis.
Of 1810 patients with PTC included in this study, lobectomy plus ipsilateral central lymph node dissection (CLND) was perform routinely; 250 had TT with bilateral CLND. The mean time of follow-up was 102.7±33.5 months. The cancer-specific survival rate was 98.8% at 10 yr and 97.2% at 15 yr from initial operation. Patients with CLNM showed significantly worsen cancer-specific, not recurrence but worsen distant metastasis-free survival rates by Kaplan-Meier method; bilateral CLNM took more risks significantly. But in Cox multivariate analysis, CLNM was not associated with prognosis; greater maximal tumor size (≥4.1 cm) and distant metastasis were found be predictors for worsen cancer-specific survival, multifocal and extrathyroidal extension for recurrence. Moreover, TT was a predictor for higher cancer-specific survival rate, and bilateral lesions was a predictor for reduced-recurrence inversely on multivariate Cox analysis. Among all patients, 151 (8.3%) had transient hypoparathyroidism and 2 (0.1%) were permanent; 78 (4.3%) had transient recurrent laryngeal nerve injury and 10 (0.6%) were permanent.
CLNM, especially bilateral CLNM, increased cancer-specific mortality as well as distant metastasis in PTC patients. Prophylactic ipsilateral CLND is recommended in PTC patients with high-risk factors; selective TT and bilateral CLND are recommended in PTC patients at least with bilaterally malignant tumors.
Thyroid Nodules & Goiter Thursday Poster Clinical
Surgical resection is the main treatment of thyroid nodules in clinic. However, the recurrence rate is high. The recurrent laryngeal nerves (RLN), and the parathyroid glands are difficult to identify in secondary surgery. This study aimed at exploring the relationship between TSH level and the recurrence rate of thyroid nodules after non-total thyroidectomy for benign thyroid nodules by multi-center and retrospective research.
Participants enrolled in 5 trial centers from 2004 to 2009, and during follow-up through 2012–2013, the TSH level and B-mode ultrasonography of the thyroid were performed. Of the 3843 subjects who were enrolled at baseline, 325(8.46% percent) were with full follow-up data of both thyroid function and ultrasonography records.
Postoperative thyroid nodules recurrence rate was 40.62% (132/325); wherein, recurrence rate of subjects whose postoperative TSH≤1.0 mIU / L was 26.53% (13/49), recurrence rate of thyroid nodule in subjects whose postoperative TSH>1.0 mIU / L was 43.12% (119/276). The P value of Chi-square test between the recurrence rate of different TSH level groups is 0.0294. The P value of linear correlation analysis between postoperative TSH levels and thyroid nodule recurrence is 0.4546.
The recurrence rate increased (P value=0.0294) in those benign thyroid nodules patients whose postoperative TSH>1.0 mIU/L compared to those postoperative TSH≤1.0 mIU/L.
Autoimmunity Thursday Poster
Graves' disease can be associated with hematopoietic dysfunction which is inherently responsive to treatment with anti thyroid agents. We present a case of bone marrow suppression due to possible autoimmune effects of Graves' disease.
48 year old female presented to ER for dysphagia and 25 lbs weight loss for 2 months. She also complained of generalized fatigue for few weeks. No history of fever, night sweats, diarrhea, tremors or palpitations. Family history was significant for hypothyroidism in her mother.
On exam, BP 154/88 mmHg, pulse 104/min, temperature 98.3 F, RR 18/min, weight 85 lbs. She appeared hyperactive. Proptosis and exophthalmos was evident. Neck exam revealed a non-tender, diffusely enlarged thyroid gland, about 60 gm, with palpable isthmus and no bruit. Reflexes were brisk. Rest of the exam was normal. Labs showed WBC of 2.8 (4–11 k/mm cu), ANC 0.7 (1.7–7.7 k/mm cu), platelet 98 (150–450 k/mm cu), Hb 9.7 (12–15 gm/dl). Iron studies, B12 and folate were normal. TSH was <0.005 (0.27–4.2 uIU/ml), FT4 7.77 (0.93–1.7 ng/dl), FT3 6.43 (1.7–4.2 pg/ml), T3 total 205 (80–200 ng/dl). Thyroglobulin, thyroglobulin Ab, TPO antibody, ANA and ESR were normal. TSI was elevated to 432 (n<140%). Iodine 123 uptake scan a week before admission showed 76% and 85% uptake at 6 and 24 hours. No treatment was started at that time. Previous labs one year ago were normal. Patient was started on propanolol and Methimazole after explaining risks and benefits. She preferred oral therapy to I - 131. After 4 days she improved symptomatically, FT4 reduced to 2.62 ng/dl. Bone marrow biopsy was deferred due to patient preference. At 12 weeks of treatment, her CBC and Thyroid function normalized.
Pancytopenia is a rare complication of Grave's disease. Immunologic and toxic mechanisms are implicated in it's pathogenesis. Our patient had a dramatic response to methimazole and this strengthens the association of pancytopenia in untreated Graves' disease. The frequency of this association is under diagnosed. Agranulocystosis is commonly seen after starting anti thyroid drugs. In this case, ANC improved dramatically once Methimazole was started. Hence, it is important to check blood counts in all patients with thyroid dysfunction.
Laboratory tests
Disorders of Thyroid Function Thursday Poster
Thionamides are common treatment options for Grave's diseases in United States, with methimazole being the drug of choice except during pregnancy and thyroid storm. Management of hyperthyroidism in patients who are acutely ill, may not be feasible with oral formulations. Alternative routes are required in such scenarios, but are not available commercially. Very few case reports describe non-oral routes of administration including methimazole as a suppository and intravenous (I.V.) form and PTU as a suppository/enema and I.V. formulation. Only one randomized study compares therapeutic equivalence of water retention enema vs. polyethylene glycol based suppository of PTU. As experience is very limited, management of graves diseases in these patients can be challenging.
We present a unique treatment dilemma in a patient unable to take oral medications due to small bowel resection. The patient is a 51-year-old-female with Graves disease diagnosed over 10 years prior with significant orbitopathy and a recent ruptured globe. She was clinically and biochemically euthyroid on methimazole 10 mg daily. She presented to out tertiary care center after a motor vehicle accident resulting in small bowel volvulus and perforation requiring emergent total enterectomy and hemi-colectomy. In the absence of functional bowel, nutrition and medication were provided via I.V. route. Endocrinology was consulted as patient became hyperthyroid during her prolonged hospital stay. Our colleagues in pharmacy prepared water based retention enema of PTU 50 mg QID for her inpatient treatment. Ten days after this regimen (TSH- 0.223 mIU/L, FT4- 0.7 ng/L) patient's thyroid function stabilized. Eventually, she was transitioned to 10 mg methimazole suppository as an outpatient without any adverse effect and clinically favorable outcome.
This case highlights the utilization of alternative formulation of thionamides in the treatment of graves diseases, when oral route is not feasible.
We successfully treated a patient with rectal retention enema of PTU, although more data is still needed to clarify the dosage equivalency, safety and efficacy of rectal formulation.
Disorders of Thyroid Function Thursday Poster
Suppurative thyroiditis is a rare clinical entity often associated with immunosuppression or anatomic defects predisposing to thyroid infection. Hyperthyroïdism has been rarely described with suppurative thyroiditis. We report the case of an acute bacterial thyroiditis causing thyrotoxicosis followed by hypothyroidism.
CASE: A 42 years old man, with type 1 diabetes, presented to the emergency room with hyperthermia, respiratory symptoms and bilateral pneumonia on chest x-ray. 24 hours later, the patient developed severe anterior cervical pain and compressive symptoms. A neck CT-scan showed thyroid infiltration and a precricoid abscess which necessitated surgical decompression. A diagnosis of suppurative thyroiditis was made and large spectrum IV antibiotics was given. Hyperthermia persisted after abscess drainage and during the next day, while in ICU, he developed confusion, agitation, tremors and sinusal tachycardia. Thyroid function tests showed TSH 0,01: mUI/L (0,35–3,50); free T4: >100 nmol/L (11–22) free T3: 10,8 pmol/L (3,4–6,8), which persisted for 6 days. With clinical evolution, the timing of thyrotoxicosis with iodine injection for the CT, and autoimmune background of the patient, Grave's hyperthyroidism exacerbated by iodine was considered and propylthiouracil was started. Thyroid hormones lowered 48 hours later and patient improved. After hospital discharge, the patient developed hypothyroidism which persisted after weaning and discontinuing anti-thyroid drugs. 1 week later, patient became euthyroid which was consistent with thyroiditis evolution. TRAB and anti-TPO revealed negatives. Investigations for immunosuppression revealed to be normal
Since 1980, about 20 cases of bacterial thyroiditis presenting with thyrotoxicosis have been reported. Only a minority have progressed to hypothyroidism.
Our case show a classical, but rarely reported in suppurative thyroiditis, evolution of with a thyrotoxic phase followed by a hypothyroid phase before returning to normal function. Since the resolution of the thyroiditis the patient remains euthyroid.
Disorders of Thyroid Function Thursday Poster
Hashimoto's thyroiditis is the most frequent cause of hypothyroidism. The most common neuromuscular manifestations include myalgia, fatigue, proximal muscle weakness and hypoactive tendon reflexes. However, infrequent severe cases of rhabdomyolysis with markedly elevated levels of creatine phosphokinase (CPK) and renal disease have been reported. Association between severe hypothyroidism and acute kidney injury (AKI) is rare
We report a case of rhabdomyolysis, acute kidney injury, and myopathy as the only manifestations of severe hypothyroidism secondary to Hashimoto's thyroiditis.
A 32 year old male was admitted to the hospital with bilateral upper and lower extremities progressive pain and swelling. Symptoms started three days prior to admission and became worse the night before admission. Pain was worse with movement. He denied any vigorous activity, trauma, previous medications, and fever. Neurological examination revealed decreased muscle strength symmetrically on lower limb (3+/5+) and upper limbs (4+/5+), and diminished tendon reflexes (1+/4+) symmetrically. Laboratory evaluation revealed the following serum levels: CPK, 2256 IU/L (38–174), creatinine 2.6 mg/dl (0.5–1.20), free thyroxine (FT4) <0.20 ng/dl (0.93–1.70), thyroid stimulating hormone 259.70 uIU/ml (0.400- 5.40), and thyroid peroxidase antibody 452 IU/ml (<35). After ruling out adrenal insufficiency by cosyntropin stimulation test, treatment was started with 125 ug oral levothyroxine. The symptoms gradually improved. The patient was discharged from the hospital five days later, showing only mild muscle pain. CPK levels reduced significantly.
Although hypothyroidism rarely presents with AKI and rhabdomyolysis, it should be suspected in patients presenting with impaired renal function and high creatine kinase level in the absence of other causes of rhabdomyolysis.
Disorders of Thyroid Function Thursday Poster
Although as many as 22% of patients with thyrotoxicosis present with hypercalcemia, the incidence of concomitant thyrotoxicosis and hyperparathyroidism is exceedingly rare since the physiologic response of the body is to suppress PTH in response to T3-induced hypercalcemia1,2. To date there have been only 51 reported cases in literature demonstrating this phenomenon. All of these cases utilized thyroidectomy/parathyroidectomy as definitive treatment strategies.
We describe a patient who presented with thyrotoxicosis with hypercalcemia and hyperparathyroidism, he was treated with radioactive ablation (RAI) and cinacalcet for his thyrotoxicosis.
Resulting in a resolution of his hypercalcemia and hyperparathyroidism.
This is the first documented case in which a new therapy – calcimimetics – was used for treatment control of hypercalcemia while radioactive thyroid ablation was used for control of the thyrotoxicosis. We describe a novel therapy for treatment of PTH-dependent hypercalcemia in the context of hyperthyroidism, without necessitating surgical management.
Thyroid Cancer Thursday Poster
Seven cases of synchronous well-differentiated thyroid cancer (WDTC) originating in struma ovarii (SO) and cervical WDTC have been previously described. The objective of this study was to report the evaluation and management of an additional case and review the literature concerning second primary cervical WDTC in the setting of WDTC originating in SO.
The study design is a case report. The setting is a tertiary care center. A review of the literature was performed via Pubmed using search terms “malignant struma ovarii” and “struma ovarii and carcinoma.”
A 58 year old female with synchronous T2N0M0 papillary thyroid cancer PTC originating in SO with wild type BRAF and T1aN0M0 cervical PTC with BRAF V600E mutation underwent complete surgical resection of both neoplasms (with total thyroidectomy for the latter), subsequent postoperative radioactive iodine and suppressive thyroid replacement therapy at our institution. She completed treatment over three years ago and remains without evidence of disease. According to our review of the literature, 123 cases of WDTC originating in SO have been reported. 60 patients underwent total or near-total thyroidectomy, 11 of which were diagnosed with cervical WDTC. Of these four were metachronous and seven were synchronous cervical WDTC.
This is the only the eighth reported case of a synchronous WDTC originating in SO with a second primary cervical WDTC. Although very rare, review of the literature reveals an increased incidence of a second primary cervical thyroid cancer in the setting of MSO. Further studies are needed to assess for selection bias, as this finding may impact the controversial management of WDTC originating in SO.
Thyroid Cancer Thursday Poster
Endogenous T3 toxicosis in the setting of metastatic Hurthle cell thyroid cancer is rare. Few reports of metastatic Hurthle cell carcinoma producing T3 toxicosis are reported in the literature. We report a case of widely metastatic HCC producing T3 toxicosis.
Chart review.
A 75 year old female underwent total thyroidectomy with bilateral neck dissections in 2004 for widely-invasive Hurthle cell thyroid cancer followed by 3 annual doses of I131 (totaling 550 mCi) over the next 3 years for persistently elevated Tg>3000 ng/ml with widely metastatic disease to liver, bone and lungs. In follow up she required continuously decreasing doses of LT4 in the setting of a suppressed TSH and low FT4 levels with concomitant elevated T3(TSH 0, FT4 <0.3 ng/dl, FT3 5.1 pg/dl and total T3 of 230 ng/dl off of LT4 for 12 weeks). She denied use of exogenous T3. This raised the suspicion of endogenous production of T3 from metastatic HCC in the setting of a thyroglobulin >3000 ng/ml. She was without symptoms of thyrotoxicosis. On PE, she was clinically euthyroid but was noted to have a 30 mm left mid-cervical mass. A Technetium scan revealed abnormal acitivity in the neck mass. A PET-CT showed persistent metastasis in the lungs, liver, and bone. Patient requested surgical resection of neck mass. Surgical pathology of the posterior neck mass revealed metastatic Hurthle cell carcinoma. Two weeks after surgical resection, while off thyroid hormone replacement, her TSH was appropriately elevated at 40 and her FT3 decreased to 2.2 pg/ml with undetectable FT4. At that time she was restarted on LT4 50 mcg daily.
T3 toxicosis in the setting of metastatic Hurthle cell thyroid cancer is rare. We have presented a case of widely metastatic HCC where removal of neck metastasis removed much of excess endogenous T3 production by HCC resulting in conversion from T3 toxicosis to hypothyroidism.
Thyroid Cancer Thursday Poster
Parathyroid carcinoma is a rare malignant endocrine tumor accounting for only 0.5% to 5% of all primary hyperparathyroidism.
We performed a case series study in which initially we diagnosed 22 cases of primary hyperparathyroidism. In the study period, out of the 22 neck masses, 4 were parathyroid carcinoma, 17 parathyroid adenomas and 1 adipose involution. Mean age was 56 years; 19 patients were female.
Bone pain, kidney stones and depressed mood were the most common symptoms presented by all of the patients with parathyroid cancer (n=4). Mean laboratory values showed pre-operatory serum calcium above 12 mg/dL and an average pre-operatory Parathyroid hormone (PTH) of 1190 pg/mL. Gammagraphic studies were made to confirm the existence and location of the tumors. A surgical intervention was scheduled to remove the tumors and obtain a biopsy of the lesion. PTH values were measured before, during and after surgery. Drops to normal values were taken as a sign of resolution. A total thyroidectomy was performed in one of the parathyroid carcinoma patients for presenting a nodule in the contralateral thyroid lobe with cytology Bethesda V - highly suggestive of papillary thyroid carcinoma. Neither loco-regional, nor distant metastasis where found during the surgery. Two of the patients had minor complications: one seroma and one transient hypocalcemia; both resolved with no further complications. CT scan with contrast and PTH values remained normal at follow-up.
This case series displays an exceptional rare malignancy of parathyroid carcinoma, especially one with synchronous papillary thyroid carcinoma. Owing to the rarity of this disease, prospective studies including larger amount of patients are recommended in order to gain greater insight and to monitor disease incidence in the Dominican Republic.
PTH values of Parathyroid Carcinoma Patients
Normal Reference Values: 10 – 65 pg/mL; PTH: Parathyroid Hormone.
Thyroid Nodules & Goiter Thursday Poster
A 59 year-old woman with a history of hypothyroidism from Hashimoto's thyroiditis on thyroid hormone replacement and history of metastatic melanoma presented with a growing thyroid cyst and isthmus nodule. Previously she had a breast mass resected and found to be metastatic melanoma without an identified primary or other metastases. An asymptomatic left thyroid cyst was seen on initial staging scans. The cyst enlarged over 1 year, and she developed dysphagia.
Ultrasound showed multinodular goiter, a left lobe 2.4 cm hypoechoic cystic mass, and a 0.8 cm solid hypervascular hypoechoic isthmus nodule. Restaging showed no other suspicious tumors. FNA of the cystic lesion showed benign follicular cells while the isthmus mass showed atypical cells of unclear etiology–whether melanoma or atypical follicular cells. Given her compressive symptoms and already hypothyroid state, we advised complete thyroidectomy.
Pathology showed a well-circumscribed isthmus tumor with a thin fibrous capsule growing in trabeculae separated by hyalinized stroma (Figure). The tumor was positive for TTF-1 and thyroglobulin (Tg) and negative for calcitonin, synaptophysin and chromogranin A (CgA). It was also negative for MART-1 and HMB-45 which were positive in her prior melanoma. MIB-1 staining showed low cell proliferation index but focal membranous staining. These findings are consistent with a hyalinizing trabecular tumor (HTT) of the thyroid. The remaining thyroid gland showed chronic lymphocytic thyroiditis, adenomatoid nodules, and a 0.1 cm papillary microcarcinoma.
Hyalinizing trabecular tumor of the thyroid: Left panel, H&E (10X); right panel, MIB-1 (10X).
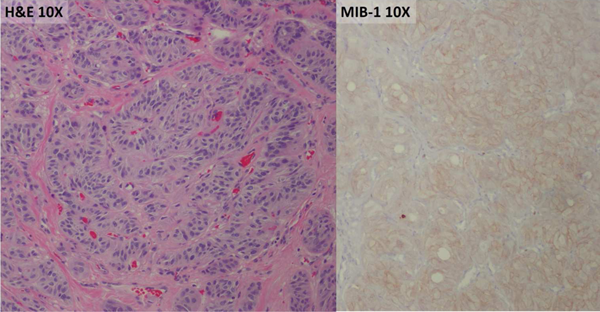
HTT is a rare neoplasm first described by JA Carney in 1987. It can present a diagnostic dilemma but can be discerned from other pathologies by its characteristic histopathology and immunohistochemistry as it is usually positive for TTF-1 and Tg but negative for calcitonin, synaptophysin and CgA. MIB-1 staining pattern can help distinguish HTT from papillary thyroid carcinoma (PTC) as membrane-positive reactivity is distinctive in HTT. BRAF V600E mutation may occur in PTC but not seen in HTT. HTT is felt to be generally benign but with undetermined malignant potential as it rarely metastasizes. Some advocate lobectomy rather than total thyroidectomy in selected patients.
Friday, October 31, 2014
Thyroid Cancer Friday Oral Basic 5:10 PM
Na+/I- Symporter (NIS)-mediated radioiodide uptake (RAIU) in thyroid cells allows targeted treatment of thyroid cancer. Many patients with advanced thyroid cancer do not benefit from radioiodine therapy due to reduced/absent NIS expression/function. MicroRNA (miR) has emerged as a promising therapeutic target in many diseases. However, the role of miRs on NIS-mediated RAIU has not been investigated.
TargetScan and microRNA.org were used to identify miRs that may bind to hNIS 3'UTR. The role of selected miRs on NIS-mediated RAIU was investigated using HEK293 cells expressing exogenous hNIS. The effect of miR-339-5p was further confirmed in MCF-7 human breast cancer cells and PCCl3 rat thyroid cells that endogenously express NIS upon treatment with transretinoic acid/hydrocortisone (tRA/H) and TSH respectively. Luciferase reporter assay was employed to examine if miR-339-5p directly binds to NIS 3'UTR. Nanostring nCounter rat miR expression assay was conducted to identify miRs deregulated by 17-AAG, Akti-1/2 or TGF-β known to modulate NIS-mediated RAIU in PCCl3 cells. The miR expression profiles in a cohort of thyroid tissues were determined by Next Generation Sequencing.
Among the two candidate miRs identified, overexpression of miR-339-5p decreased NIS-mediated RAIU in HEK293/hNIS cells and miR-339-5p directly binds to hNIS 3'UTR. The miR-339-5p decreased NIS mRNA levels and RAIU in tRA/H-treated MCF-7 cells as well as TSH-stimulated PCCl3 cells. Among 38 miRs deregulated by 17-AAG, Akti-1/2 or TGF-β in PCCl3 rat thyroid cells, 18 miRs were conserved in human. The expression profiles of these 18 miRs were able to separate most papillary thyroid tumors from adjacent non-malignant thyroid tissues and thyroid tissues from normal individuals. The miR-339-5p was not selected in the list of 38 miRs due to its low expression level in PCCl3 cells, which did not meet the cut-off value of Nanostring analysis. However, miR-339-5p expression was increased in most papillary thyroid carcinomas.
We identify miR-339-5p as the first miR that modulates NIS-mediated RAIU in various cells. Targeting miR-339-5p may have the potential to further enhance NIS-mediated therapy.
Thyroid Cancer Friday Oral Basic 5:25 PM
Medullary thyroid cancer (MTC) is a neuroendocrine (NE) tumor and accounts for 3–5% of thyroid cancer cases. New adjuvant therapies are needed to improve local/regional control of MTC after surgery and treat distant metastatic disease. Here, we report a unique type of unimolecular micelle conjugated with a somatostatin analog (KE108) as a nanocarrier for a novel histone deacetylase inhibitor, AB3, for targeted MTC therapy. The effects of the KE108 targeting ligands on the cellular uptake and anticancer effects of the AB3-loaded micelles in MTC cell lines have been examined.
Tumor-targeting unimolecular micelles were prepared using a KE108-conjugated multi-arm star amphiphilic block copolymer (i.e., PAMAM-PVL-PEG-KE108). The hydrophobic PVL core was used to encapsulate the AB3 and the hydrophilic PEG shell was used to provide water solubility and reduce opsonization. Human MTC cell lines (TT and MZ) were treated with a family of micelles (AB3-loaded targeted and non-targeted, and empty targeted and non-targeted) at an AB3 concentration of 3 μM for 24, 48 and 72 hrs. The cell proliferation and the expression of NE markers (ASCL1 and CgA) were assessed by MTT assay and Western blot, respectively. The effect of the KE108 targeting ligands on the cellular uptake of the micelles was measured by flow cytometry.
The family of pH-responsive unimolecular micelles was developed for targeted delivery of AB3 to MTC cell lines. The AB3 loaded and KE108-conjugated targeted micelles had the strongest inhibitory effect on MTC cell proliferation and NE marker expression. Moreover, the targeted micelles exhibited a much higher cellular uptake (40 fold increase) than non-targeted micelles based on flow cytometry analysis.
The KE108 targeting ligands substantially increased the cellular uptake of the micelles in MTC cell lines and improved cytotoxic effect of AB3 in vitro. Thus, targeted delivery of anticancer drug AB3, specifically to the tumor tissue could significantly improve the therapeutic outcomes in treating MTC disease while reducing systemic toxicity.
Autoimmunity Friday Oral Basic 5:40 PM
Cell-based bioassays are sensitive diagnostic tools but can exhibit variable reproducibility. In order to promote standardization of results among laboratories that perform thyroid-stimulating antibody (TSAb) bioassays, we calibrated TSAb levels against an international standard.
TSAb was measured using CHO cells expressing a chimeric TSHR. Five concentrations of the second IS (NIBSC 08/204,113 mIU) were applied for calibration. Results were reported as percentage of specimen-to-reference ratio (SRR, cut-off 140%) and converted into mIU/L. Several reference controls were compared: bovine (b) TSH, serum from a healthy subject (HS) and a healthy donor pool (HS pool).
A total of 48 samples of patients with GD were converted into mIU/L. All IS standard curves had R2>0.95. For the IS calibration curve 5, 10, 20, 40 and 80 mIU/L were measured. Using bTSH, average TSAb SRR%±SD values were 116±7.4 (CV 6.4%), 173±4.6 (2.6), 242±9.1 (3.8), 320±14.3 (4.5), 404±14.8 (3.7), respectively. TSAb levels corresponded to 5.5±0.4, 9.4±0.4, 18.3±1.6, 39.1±5.5 and 87.2±12 mIU/L, respectively. Utilizing HS, values were 162±10 (6.2), 241±6.6 (2.7), 336±12.9 (3.8), 446±20 (4.5), 562±20.9 (3.7). Using a HS pool, values were 131±8.5 (6.5), 196±5 (2.6), 274±10 (3.7), 363±16.4 (4.5), 457±16.9 (3.7). When converting patient samples into mean mIU/L, values were 13.8±1.8, 11.9±0.2, 7.8±0.3, 17.8±0.8, 6.1±0.1 and 65.6±17.3 mIU/L for all three reference controls which have been used for measuring TSAb values in selected samples (table).
For the first time, standardization of a bioassay correlating TSAb SRR% to mIU/L was achieved. These results will allow improved comparison of studies involving TSAb levels. In addition, reporting TSAb in mIU/L will be clinically useful for serial TSAb measurements during patient management.
Thyroid Hormone Action Friday Oral 5:55 PM
The sympathetic nervous system (SNS) negatively regulates bone metabolism, via β2-adrenergic receptor (AR-β2), which is expressed in osteoblasts. Alpha2 adrenergic receptors (α2C-AR and α2A-AR) are also expressed in osteoblasts, osteocytes, osteoclasts and chondrocytes of the epiphyseal growth plate (EGP), suggesting that the SNS actions in the skeleton are also mediated by α2-ARs. The present study aimed to investigate if TH interacts with the SNS, via α2C-AR signaling, to regulate the EGP morphology and the longitudinal bone growth (LBG).
We evaluated the LBG and the distal femoral EGP morphology of 21-day old female wild-type (WT) and α2CAR-/- mice (n=8/group), treated for four weeks with a supraphysiological dose of triiodothyronine (7 μg/100 gBW/day), to mimic hyperthyroidism (Hyper), or treated with inhibitory drugs of the thyroid function, methimazole (0.1%) and sodium perchlorate (1%) added to drinking water, for hypothyroidism (Hypo) induction.
Compared to the WT mice, euthyroid α2CAR-/- mice had lower femur length, an important disorganization of the proliferative zone (PZ) and significant increase (30%, p<0.001) in the number of mature hypertrophic chondrocytes (MHC) of the EGP. In WT animals, Hypo promoted expected alterations: a significant reduction in the LBG, PZ disorganization and a decreased number of MHC. Surprisingly, Hypo promoted opposite effects in the EGP of α2CAR-/- compared to WT mice. Hypo was able to partially revert the PZ disorganization observed in euthyroid α2CAR-/-, and resulted in a greater number of MHC (27%) compared to WT Hypo. On the other hand, Hyper caused an increase in the number of hypertrophic chondrocytes (HC) in WT mice and a reduction in α2CAR-/- mice. Furthermore, Hyper α2CAR-/- animals showed a very significant reduction (2-fold) in the number of HC and MHC, when compared to the Hyper WT mice.
These findings strongly suggest that TH interacts with the SNS, via α2C-AR signaling, to regulate the EGP morphology and the bone growth.
Disorders of Thyroid Function Friday Oral Basic 6:10 PM
Endocytic cargo trafficking has an important impact in cell biology, thyroid autoimmunity and cancer transformation. Many cell surface receptors and membrane proteins are internalized through specialized structures of the plasma membrane, called clathrin-coated pits (CPs). Other non-receptor proteins are stochastically endocytosed via rapid macropinocytosis, a mechanism often used in cancer cells. G protein-coupled receptors (GPCRs) such as the TSH receptor (TSHR), undergo endocytosis via CPs and this mechanism has been implicated as an important regulator of signal transduction.
We have used cAMP luciferase assay in CHO cells overexpressed with TSHR and cAMP ELISA for FRTL5 cells. Live-imaging has been performed using labeled TSH and labeled anti-TSHR antibodies. Lysosomal dye and lysosomal construct were also used in live cell-imaging.
Indeed, we have found that abrogating the CPs endocytic process with dynamin (Dynasore) and non-selective PKC-delta (rottlerin) inhibitors suppressed cAMP signaling in rat thyroid cells (FRTL5). Labelled TSH and labelled TSHR-Abs induced endocytic vesicular trafficking via CPs in FRTL5 cells as evidenced by live-cell imaging with total lysosomal degradation of the ligands by 5 days. In contrast, in thyroid cancer cells (ML1), human immortal thyrocytes (tad2) and immortal cells transfected with the TSHR (CHO-TSHR), TSH or antibody vesicular trafficking in these cells was markedly increased with total lysosomal degradation by 3 days; indicative of non-CPs uptake. We found that the endocytic pathways for TSH and TSHR-Abs in these abnormal cells was indeed via non-CPs mechanisms, such as macropinocytosis, as evidenced by lack of typical endocytotic vesicle formation.
Since it is known that inhibition of non-CPs endocytosis may induce cell death, the targeting of such disrupted endocytic pathways may offer new possibilities for inducing cancer cell apoptosis.
Thyroid Hormone Metabolism & Regulation Friday Oral Basic 6:25 PM
Mammals possess both white (WAT) and brown adipose tissue (BAT). WAT has low metabolic potential and is associated with obesity and the maladies of metabolic syndrome, while BAT has high metabolic potential and is associated with resistance to obesity. Functional conversion of WAT into a tissue with BAT-like activity, an action often referred to as “browning” has become an intriguing strategy to combat metabolic disease. Although, thyroid hormone receptors (TRs) have long been associated with metabolic regulation and adaptive thermogenesis, a full understanding of this relationship is lacking.
Here, we report that pharmacological TR activation the synthetic agonist GC-1 evokes a profound functional conversion of WAT into a brown adipose-like tissue. TR agonist treatment of genetically obese (ob/ob) and diet induced obese (DIO) mice dramatically increases UCP-1 expression and upregulates the entire program of adaptive thermogenesis, uncoupled respiration, and mitochondrial biogenesis in WAT that is correspondent with an amelioration of obesity and insulin resistance.
Consistent with the idea that metabolic increase is mediated principally by WAT, this effect does not require functional brown fat, yet all thermogenesis is lost in lean mice that possess little WAT. TR activation can also induce uncoupled respiration in white adipocytes in vitro demonstrating that browning is a cell autonomous effect of TR activation in WAT.
This data demonstrates that TR activation can elicit a functional conversion of white to brown fat, a previously unrecognized component of TR-mediated thermogenesis, and establishes the profound pharmacological potential of WAT browning.
Thyroid Cancer Friday Oral Translational 5:10 PM
Anaplastic thyroid cancer (ATC) is one of the most aggressive human malignancies, with a median survival time of less than one year. Our understanding of the molecular events that lead to ATC is poor. MiRNA have been established as important regulators of cancer initiation and progression but there is limited data on the role of miRNAs in ATC.
miRNA profiling in thyroid cancer samples was assessed using microRNA microarray and RT-PCR. Overexpression of miR-30a-5p was formed in ATC cells ot dertermine the role of miR-30a-5p in ATC. Luciferase assay was used to validate LOX as a direct target of mir-30a-5p. Our in vivo metastastic ATC mouse model was used the evaluate the role of miR-30a-5p and LOX in ATC progression.
miRNA expression profiling in human thyroid cancer samples showed significant downregulation of miR-30a-5p in ATC and poorly differentiated thyroid cancer (PDTC). TCGA dataset showed that miR-30a-5p downregulation was associated with aggressive histologic variants, higher risk thyroid cancer and higher mortality rates. Ectopic expression of miR-30a-5p in vitro decreased invasion and migration of ATC cells, with inhibition of EMT markers and Lysyl Oxidase (LOX) expression-a predicted target of miR-30a-5p. miR-30a-5p significantly decreased lung metastasis in vivo with decreased EMT markers and LOX expression in metastatic tissue. LOX was overexpressed in ATC and PDTC and inversely correlated with miR-30a-5p expression. In TCGA dataset, upregulation of LOX was associated with more aggressive thyroid cancer and higher mortality rate. Transfection of 3'UTR-LOX along with miR-30a-5p demonstrated that miR-30a-5p directly targets LOX. Direct knockdown of LOX inhibited cell proliferation, increased apoptosis and decreased cellular invasion and migration of ATC cells. Moreover, the inhibition of LOX using the LOX inhibitor BAPN or siLOX significantly decreased the lung metastases in vivo.
Together, our data supports an important role of the miR-30a-5p-LOX axis in thyroid cancer progression. The current development of agents targeting LOX could be useful for ATC and PDTC cancer therapy.
Thyroid Cancer Friday Oral Translational 5:25 PM
BRAFV600E is an important driver mutation in thyroid cancer and is found in half of patients with papillary thyroid carcinoma (PTC). Detection of this mutation in tumor DNA obtained cytologically or pathologically is useful in work up of nodules or for determining therapeutic options for using novel targeted therapies. We have previously described a novel, highly sensitive and specific blood-based BRAFV600E assay in patients with melanoma, which allows detection of mutant BRAF in RNA from mixed populations with as few as 0.1% BRAFV600E containing cancer cells and used to assess a therapeutic response to BRAF inhibitor therapy. We hypothesized that our novel blood based BRAF assay could detect circulating mutant BRAF in the blood of patients with PTC.
We collected blood from patients undergoing thyroidectomy for thyroid disease prior to surgery and up to 4 weeks post-operatively. BRAF status was not known at time of initial collection and no patient had a history of colon cancer or melanoma. We analyzed each blood sample and quantified circulating BRAFV600E levels by utilizing a unique restriction enzyme site and a series of PCR amplifications and wild-type BRAF digestions. Extracted RNA was quantified by RT-PCR prior to beginning the assay to normalize all of the samples.
Pre-operative and post-operative blood samples obtained from 23 patients undergoing thyroidectomy for benign (nine negative controls) and PTC (n=14, AJCC TNM stages I-III) were analyzed. A threshold value of 1.0 picogram as “positive” separated the cohort into two distinct groupings (Figure 1). Eight of the nine patients with a “positive” test showed a decrease in circulating BRAFV600E post-thyroidectomy.

Our findings confirm the feasibility of a novel blood assay in detecting circulating mutant BRAF in the blood of patients with papillary thyroid carcinoma. This rapid assay has potential as a more cost-effective method for diagnosis, surveillance in Tg-Ab+ patients post-operatively, and in assessing evidence of disease over time in the adjuvant setting (i.e. treatment with BRAF-inhibitors).
Thyroid Cancer Friday Oral Clinical 5:40 PM
Fine needle aspiration (FNA) cytology is the most common approach to evaluate thyroid nodules, although 20–30% of FNAs have indeterminate cytology, hampering appropriate management of these patients. Follicular (or oncocytic) neoplasm/suspicious for a follicular (or oncocytic) neoplasm (FN/SFN) is a common indeterminate diagnosis with the risk of cancer estimated at 15–30%. In this study, we tested whether the most complete next-generation sequencing (NGS) panel of genetic markers can significantly improve cancer diagnosis in these nodules.
Evaluation of 143 consecutive FNA samples with the cytologic diagnosis of FN/SFN and known surgical outcome included 91 samples studied retrospectively and 52 prospectively. Analysis was performed on Ion Torrent PGM using the ThyroSeq v2 NGS panel that simultaneous tests for point mutations in 13 genes (BRAF, NRAS, HRAS, KRAS, PTEN, TP53, TSHR, GNAS, CTNNB1, RET, PIK3CA, AKT1, TERT) and for 42 gene fusions involving RET, BRAF, NTRK1, NTRK3, ALK, PPARG, and THADA. Expression of 15 genes was used to assess the cell type composition of FNA samples and expression of oncogenes resulting from gene fusions.
Histologic analysis revealed 104 benign and 39 malignant nodules (cancer rate, 27.3%). The most common point mutations affected NRAS, followed by KRAS, TERT, and TSHR. In 2 nodules, NRAS and TERT mutations were found concurrently. The identified fusions affected THADA, PPARG, and NTRK3 genes. The performance characteristics were similar between the two groups. In the cohort of 143 patients, ThyroSeq v2 performed with sensitivity of 90% (95% CI: 80–99%), specificity 93% (88–98%), PPV 83% (72–95)%, NPV 96% (92–100%), and accuracy 92% (88–97%).
The results of this study indicate that comprehensive genotyping of thyroid nodules using a broad NGS panel provides a highly accurate diagnosis for nodules with FN/SFN cytology and should facilitate optimal management of these patients.
Thyroid Cancer Friday Oral Translational 5:55 PM
Protein kinases are known to regulate the majority of cellular pathways, especially those of involved in signal transduction. Recently, the pathogenic kinases and signaling pathways specific to cancer cells were identified. To inhibit the action of the pathogenic kinases, targeted drugs (kinase inhibitors) were developed. Those kinase inhibitors are actively incorporated into management of thyroid cancer. However, the mutational profile of entire kinases (kinome) has not yet been reported in thyroid cancer.
We examined the coding sequences of 612 genes including 500 protein kinases (approximately, 3.2 Mb of DNA per sample) for variant profiles in 259 papillary carcinoma and 75 follicular carcinoma samples. Samples were collected at Seoul National University Hospital. DNA was extracted from formalin-fixed and paraffin-embedded (FFPE) tissue samples and target enrichment was done by using Agilent SureSelect Human Kinome Panel. The paired-end libraries were constructed and sequenced on Illumina HiSeq 2500 with average 250X depth coverage. Generated sequence reads were aligned to human genome hg19 with BWA algorithm, and variants were identified by Genome Analysis Toolkit (GATK) UnifiedGenotyper.
In papillary carcinoma, 36,572 SNPs and 3,650 Indels were detected. Of these, 4,118 were non-silent changes. In follicular cancer, 20,579 SNPs and 2,264 Indels were detected. Of these, 2,122 were non-silent changes. For both tumor types, G to T and A to T substitution were higher than those of normal samples. Also the Transition/Transversion ratio was slightly lower than that of normal samples. Nonsynonymous/Synonymous ratio was 1.20 in papillary cancer and 0.99 in follicular cancer. Of those detected mutations, 860 in papillary cancer and 644 in follicular cancer were reported in COSMIC database.
This is the first comprehensive study that elucidates the mutational landscape of kinome in differentiated thyroid cancer. The mutated protein kinases may contribute to cancer development in a subset of thyroid cancer and may serve as biomarkers for prediction of prognosis and drug response.
Thyroid Cancer Friday Oral 6:10 PM
Next-generation sequencing (NGS) has become a powerful cancer diagnostic technology, as it can detect multiple genomic alterations in a single assay from limited tissue. We developed a novel NGS-based assay designed to provide targeted mutation detection to aid in the diagnosis of indeterminate thyroid nodules from fine needle aspirate (FNA) and FFPE tissue (FFPET) samples. The panel includes gene targets that are commonly mutated in thyroid cancers as well as new gene mutations identified from the Cancer Genome Atlas (TCGA) or recent literature.
DNA for this NGS assay is extracted from thyroid FNA and FFPET samples and fluorometrically quantitated. A laboratory-developed 2-step multiplex PCR process enriches targeted exonic regions of 13 genes (AKT1, BRAF, CTNNB1, EIF1AX, GNAS, HRAS, KRAS, NRAS, PIK3CA, PTEN, RET, TP53, and TSHR), plus the TERT promoter region. Amplicons are then purified, barcoded, and sequenced on the Illumina MiSeq™ platform. Coverage analysis and mutation detection is accomplished using the TruSeq amplicon workflow. A positive control with known mutation frequencies is included in each run to ensure assay performance.
Single-nucleotide variants and insertions/deletions were detected to a 5% sensitivity level with as little as 1 ng DNA assay input. The panel detected all mutations in a cell line control mixture at the expected frequencies. Indeterminate FNA and FFPET samples previously tested for BRAF and RAS mutations were also sequenced; the NGS detected all previously identified mutations, with no false-negative results. In addition, the NGS assay detected mutations not identified with the initial tests, including mutations in the TERT promoter. In-silico simulation of our assay indicated a calculated clinical assay sensitivity of >89%.
We developed an NGS assay for use as an aid in the diagnosis and management of indeterminate thyroid nodules. Importantly, the assay meets the challenges of limited DNA amounts and variable quality often associated with FNA and FFPET clinical specimens. The approach offers the opportunity to streamline the characterization of genomic alterations in thyroid cancers to aid in thyroid cancer diagnosis.
Thyroid Cancer Friday Oral Translational 6:25 PM
The occurrence of papillary thyroid cancer (PTC) is increasing rapidly in the world. BRAFV600E mutation is the most frequent genetic alteration in PTC, and patients with BRAFV600E-PTC have poorer prognosis, higher rates of metastases and mortality, and resistance to radioiodine treatment. Discovery of large non-coding RNA (LincRNA) represents the most recent innovation achieved in the cancer research field. LincRNA can facilitate either tumor progression or elicit tumor suppressor-like function.
Here, we have analyzed the mammalian transcriptome for large non-coding RNA (LincRNA) expression in a novel experimental model of human PTC harboring the BRAFV600E mutation. We validated LincRNA expression using gene multi-profiling quantitative Real Time RT-PCR in 5 normal thyroid (NT) tissues, 5 PTC with BRAFV600E, as well as in 2 primary NT and 4 PTC cell cultures.
We have interrogated the human Body Map 2 project data base in our “RNA Research Center” and identified a LincRNA in the TPO (thyroid peroxidase) gene, which was specifically associated with thyroid tissue compared to other human tissues and cell types including stromal inflammatory cells. Our preliminary data highlighted that TPO-LincRNA showed 4.6 mRNA copy number/million copies of 18S rRNA in NT, whereas PTC samples showed a statistically significant lower copy number of the TPO-LincRNA mRNA expression levels (0.06 mRNA copy number/million copies of 18S rRNA). Similarly, the TPO mRNA expression levels were significantly lower in BRAFV600E-PTC vs. NT samples. Importantly, anti-BRAFV600E therapy with vemurafenib partially rescued the expression of the TPO-LincRNA in primary PTC cells with BRAFV600E in vitro compared to vehicle-treated cells.
In conclusion, we found for the first time the expression of a LincRNA in the TPO gene, which is strongly down-regulated in PTC. This discovery suggests that LincRNA might play a crucial role in the regulation of iodine uptake/metabolism since the TPO enzyme is fundamental for the thyroid function and storage of the intracellular pool of iodine. Additionally, LincRNAs might be tested as novel biomarkers to monitor patients undergoing targeted therapies and enable earlier diagnosis of aggressive BRAFV600E-PTC.
Autoimmunity Friday Poster Clinical
Thyroid-associated orbitopathy (TAO) occurs rarely in patients with autoimmune Hashimotos' thyroiditis (HT). Since TSH-R stimulating autoantibodies (TSAb) play a putative role in the pathogenesis of TAO, we looked for the presence of TSAb in HT patients with or without TAO.
TSAb was measured with a FDA-cleared bioassay that utilizes CHO cells expressing a chimeric TSHR and a cAMP response element-dependent luciferase. All samples were diluted 1:11 in reaction buffer. Results of TSAb activity were reported as percentage of specimen-to-reference ratio (SRR %, cut-off >140%).
A total of 1339 serum samples were collected from 574 HT patients with overt TAO (n=31/574, 5.4%, 24 female, mean age±SD 45.12±16.58 years) or without TAO (n=543, 94.6%, 448 female, 35.98±18.32 yrs.) as well as from 302 healthy euthyroid donors. Compared to controls (SRR% 53±16) and patients with HT only (63.25±70.21), serum TSAb levels were markedly higher in HT+TAO (250.95±206.51, p<0.001). TSAb were present in 43/79 (54.4%) versus 69/959 (7.2%, p<0.001) serum samples of HT+TAO and HT patients, respectively. Serum TSAb titers highly correlated with both clinical activity and clinical severity of TAO (p<0.001). In smokers, serum TSAb levels were markedly higher in HT+TAO samples (236.52±217.10) vs. HT only (69.65±84.39, p=0.001). Serum TSAb levels were also higher (357±192) in hypothyroid (baseline serum TSH 35.64±38.22 mU/L) patients with HT+TAO compared to patients with HT only (107±117, p<0.001). Finally, in patients with combined HT+TAO, serum TSAb titers correlated highly (r=0.7, p<0.001) with serum thyroid binding inhibitory immunoglobulins (TBII, automated binding ECLIA assay).
Serum TSAb are highly prevalent in HT patients with overt TAO and, as with Graves' disease, TSAb may be involved in the pathophysiology of the associated orbital involvement.
Autoimmunity Friday Poster Clinical
The mechanism of Hashimoto's thyroiditis (HT) is still unclear. Thyroglobulin antibody (TgAb) and anti-thyroid peroxidase antibody (TPOAb) are diagnostic hallmarks of HT. These antibodies regulate the balance of immunologic tolerance and autoimmunity via Fc receptors. The aim of our study was to investigate the role of Fc receptors in the pathogenesis of HT.
Blood samples from 48 HT patients (3 males, 45 females) and 21 healthy women were collected. HT patients were further divided into two groups according to thyroid function: patients with hypothyroidism (H, n=27) and euthyroidism (Eu, n=21). Flow cytometry method was used to detect the expression levels of FcγRI, FcγRII, FcγRIII on peripheral blood mononuclear cells (PBMCs) and FcγRIIB on B cells.
The positive percentage of FcγRII on PBMCs from HT patients was significantly lower than that from healthy donors (P<0.05), however, the mean fluorescence intensity (MFI) of FcγRII on PBMCs from HT patients was significantly higher than that from healthy donors (P<0.05). The positive percentage of FcγRIII on PBMCs from HT patients was significantly higher than that from healthy donors (P<0.05). The positive percentage of FcγRIIB on B cells from HT patients was significantly lower than that from healthy donors (P<0.05). In HT patients, negative correlation was found between the positive percentage of FcγRIIB on B cells and TgAb, TPOAb titers (r=−0.31, P<0.05; r=−0.273, P<0.05, respectively), and TgAb, TPOAb titers were also related to the value of MFI of FcγRIIB on B cells (r=−0.344, r=−0.257, P<0.05, respectively).
Our study indicated that the expression of FcγRs, especially FcγRIIB, might be involved in the pathogenesis of HT.
The expression of FcγRIIB on B cells in HT and control group.
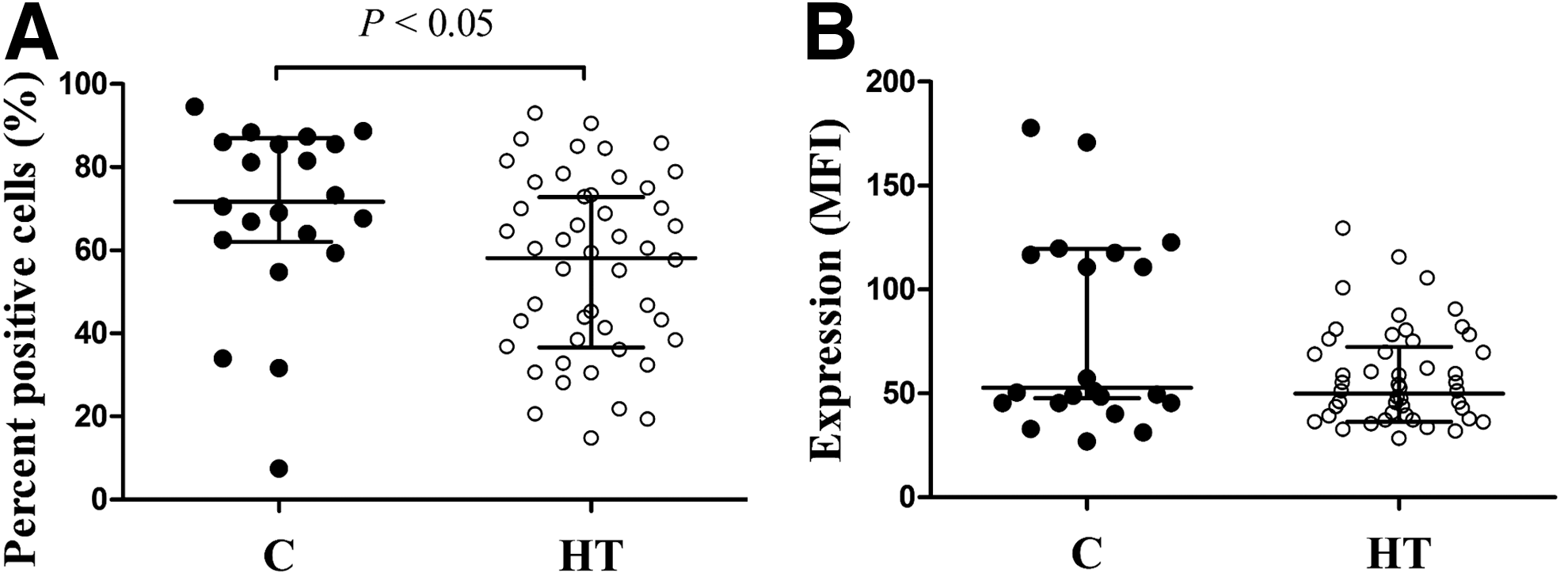
Autoimmunity Friday Poster Clinical
Learning objective- To increase clinicians awareness of Polyglandular Autoimmune Syndrome Type 2, rare, but potentially fatal condition if not timely diagnosed.
Case: A 38 year old female diagnosed with hypothyroidism 15 months ago presented to the Clinic with progressive fatigue, weight loss, bone pains, intermittent nausea and vomiting, myalgia and early satiety since her diagnosis. Examination was significant for the patient looking gaunt, weighing 97 lbs(down from 155), BP:102/58, Pulse 98 and darkening of the face and hands. Initial labs were significant for Na-126, K 5.5, mildly elevated AST, ALT and normal TSH, T3 and T4. Clinical presentation and labs prompted further work up for Adrenal insufficiency. ACTH was 2526 pg/mL, basal Cortisol was <1.0 ug/dL; 30 and 60 minutes after stimulation with ACTH it was 1.0 ug/dL. Adrenal and Microsomal antibodies were elevated (1:4 and 178.8 IU/mL respectively). CT scan showed bilaterally atrophied Adrenals. Patient was started on Prednisone and began to feel significantly better after just 2 hours. Interestingly the patient had the exact same symptoms when she was diagnosed with hypothyroidism 15 months ago (In the limited work up only TSH was elevated). Although she improved transiently with levothyroxine, despite feeling miserable and continuing to lose weight she was reassured without any further investigations because her thyroid and CMP panel were normal.
Discussion: Polyglandular Autoimmune Syndrome (PGA's) Type 2 is a rare disease defined by the occurrence of Autoimmune Adrenal insufficiency with either Autoimmune Thyroid disease or /and Type 1 Diabetes Mellitus. Adrenal insufficiency may not be the initial manifestation in 30% of the patients. The disease may be present sub clinically for a while before manifesting with electrolyte changes.
Clinicians should keep a high index of suspicion for PGA's in Thyroid and DM 1 patients especially in those whose symptoms do not match their disease profile. A work up for antibodies to Adrenals, Thyroid and Diabetes Type 1 would be prudent to avoid potentially fatal outcomes.
Autoimmunity Friday Poster Translational
Graves' disease (GD) involves autoimmunity against thyrotropin receptor (TSHR) bearing cells, leading to hyperthyroidism and often orbitopathy. When hyperthyroidism is treated with radioactive iodine (RAI), exacerbation of the orbital disease can occur. We hypothesized that RAI has immune effects affecting the balance between auto-reactive T cells and T cells with regulatory properties.
We monitored lymphocyte populations in peripheral blood of GD patients, patients with non-autoimmune goiter (NG), and healthy controls.
Circulating T cell interferon gamma production in the presence of TSHR peptides was measured in 10 GD patients and 10 healthy controls. Significant response to at least one peptide was measured in 2/10 and 3/10 GD patients before and after RAI therapy, respectively, and in none of the controls. Regulatory CD4+CD25highFOXP3 +T cells (Tregs) and Vα24+Vβ11+CD3 + Natural Killer T cells (NKT) were counted by flow cytometry in 24 GD patients and in 5 NG patients before and one month post-RAI, as well as in 19 untreated healthy subjects over the same time period. Before therapy, GD patients had a decrease in frequency of Tregs but not NKT cells compared to healthy controls. Variance of Tregs and NKT cells before and after RAI therapy was greater in GD patients compared to NG (Tregs: p=0,0053; NKT : p=0,0117) and to controls (Treg : p<0,0001; NKT : p=0,0217). Suppressive capacity of Tregs was assessed in 9 GD patients and in 3 NG patients before and one month post-RAI, and in 9 healthy controls over the same time period. RAI therapy induced a decrease in the suppressive function of Tregs, only in GD patients.
Collectively, radioiodine therapy has a mild effect on auto-reactive T cells specific to thyroid peptides. However in Graves' disease patients, it induces changes in frequency of peripheral T cells with regulatory properties and a decreased suppressive function mediated by regulatory T cells.
Disorders of Thyroid Function Friday Poster Basic
We hypothesized that isoflavin-β (Iso) administration interferes with the gastrocnemius oxidative stress (OS) preceding muscle mass loss observed after 3 days of 3,3′,5-triiodothyronine (T3) administration in a thyrotoxicosis model.
Male Wistar rats were intraperitoneally injected for 3 consecutive days with T3 (HT: 1 μg/g body weight) and treated with α-tocopherol (HT-αT: 100 mg/kg body weight) or Iso (HT-Iso: 1 mg/kg body weight). Controls included T3 thyrotoxicosis induction, α-tocopherol, and Iso. The rats were weighed daily to calculate the weight loss index (WLI); internal temperature and serum T3 levels were also determined. At 24 h after the final injection, the gastrocnemius muscle was excised and weighed. Muscle oxidative response was evaluated via lipoperoxidation analysis (t-butyl hydroperoxide-stimulated chemiluminescence, thiobarbituric acid-reactive substance), carbonylated protein quantification, mitochondrial cytochrome c oxidase activity (Cyt-c), antioxidant capacity analysis (total antioxidant capacity [TRAP], glutathione [GSH] level, and superoxide dismutase [SOD] and catalase activity). Proteolysis was estimated by analyzing chymotrypsin-like activity, and lipolysis, by analyzing plasma glycerol levels and peritoneal fat content.
Thyrotoxicosis increased the internal temperature and induced a relevant lipolysis-mediated WLI (10.93%) because the gastrocnemius weight did not change and serum glycerol levels increased with decrease in peritoneal fat. α-tocopherol plus Iso treatment did not affect the WLI but restored body temperature. Thyrotoxicosis induced muscle OS, with increase in mitochondrial Cyt-c and total SOD activity, increased lipoperoxidation and carbonylated proteins, and reduced GSH levels. Proteolysis was not affected. Iso treatment significantly modified all oxidative stress-related parameters, restoring Cyt-c, SOD, and catalase activity and GSH to control levels. Iso increased TRAP and reduced MDA and carbonylated protein levels.
These findings show that Iso prevents muscle OS generation during thyrotoxicosis, which can prevent proteolytic pathway activation and the consequent thyrotoxicosis-associated myopathy.
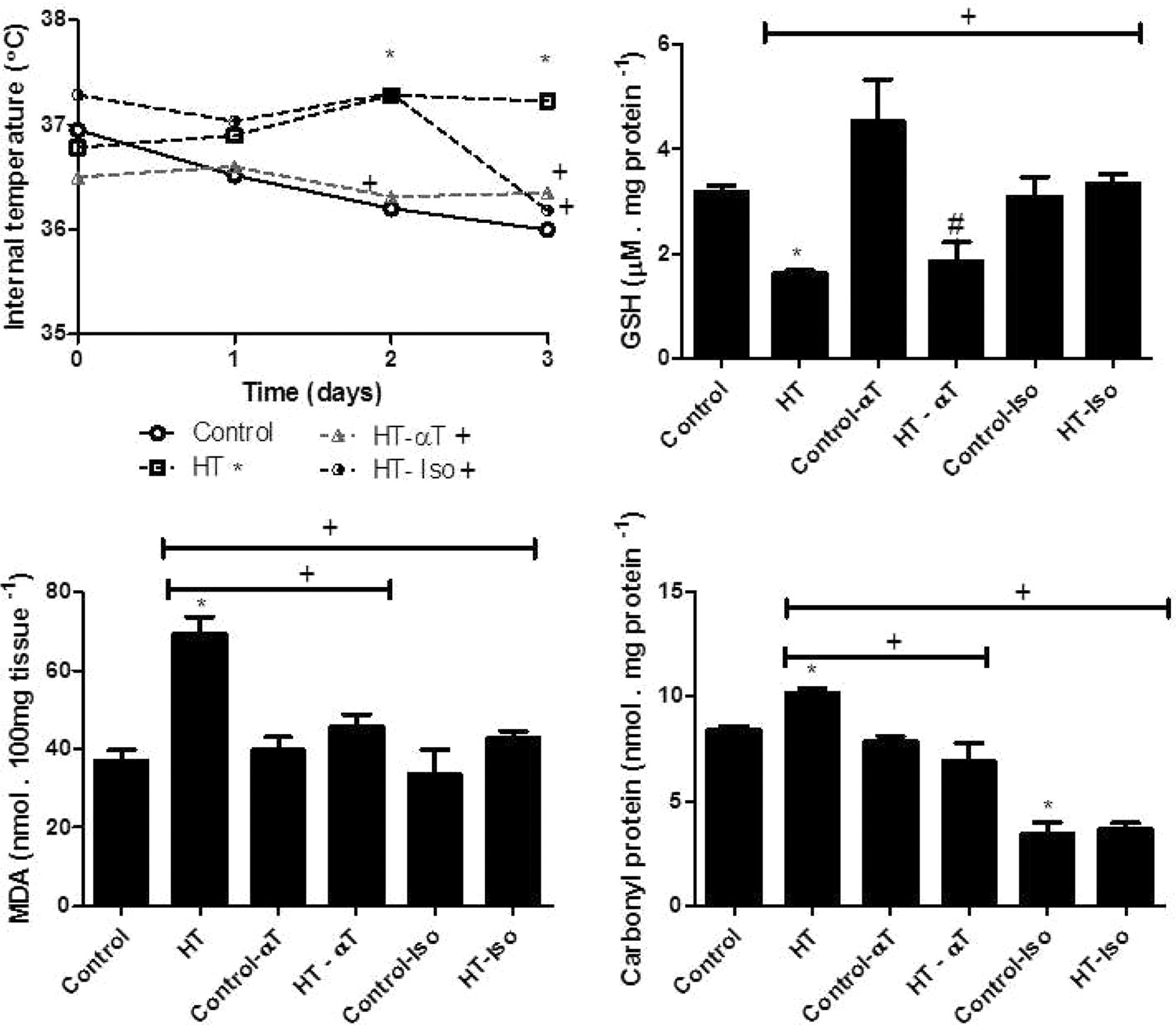
Internal body temperature and gastrocnemius levels of glutathione, malondialdehyde, and carbonylated protein in rats treated for 3 days with 3,3′,5-triiodothyronine (T3; 1 μg/g body weight) or an equivalent volume of vehicle with or without α-tocopherol (αT; 100 mg/kg body weight) or isoflavin-β (Iso; 1 mg/kg body weight). All temperature curves were significantly different by two-way ANOVA with Bonferroni's post hoc test (p<0.05). Muscles were isolated 24 h after the final T3 injection. Results are expressed as mean±SEM. Treatment groups were compared by one-way ANOVA with Tukey's post hoc test (p<0.05) (* compared to control; # compared to control-αT; ω compared to control-Iso;+compared to HT). HT: Hormone-treated; HT-αT: Hormone-treated plus αT; HT-Iso: Hormone-treated plus Iso.
Disorders of Thyroid Function Friday Poster Clinical
Liothyronine (LT3), is used in thyroid cancer patients undergoing thyroid hormone (TH) withdrawal for nuclear medicine procedures to minimize symptoms and signs of hypothyroidism. An accurate estimation of the pharmacokinetics (PK) of LT3 is important because of the narrow therapeutic index. Here we present the PK of T3 during LT3 withdrawal in the absence of endogenous T4, or exogenous levothyroxine (LT4). We also report TSH and indices of TH action on LT4 vs. LT3 therapy, and in response to acute hypothyroidism.
Fourteen patients (7 female) age 47.5±16.0 years undergoing TH withdrawal were studied. At baseline LT3 (thrice daily) was substituted at a 1:3 ratio (mcg/mcg) for LT4, and after one month PK parameters were estimated following the last LT3 dose (day 1). PK compartmental modeling was employed to fit the observed data, followed by simulations to explore different regimens. TSH and indices of TH action were assessed at baseline, day 1, and after withdrawal (day 11).
The doses of LT4 and LT3 were 164±42.4 and 53.6±12.3 mcg, respectively. No difference in TSH was observed between baseline (0.01±0.14) and day 1 (0.06±0.07), while on day 11 TSH was 38.6±20.5 mcIU/mL. Baseline T3 (115.3±26.4) was lower than day 1 (166.7±37.7 ng/dL, p<0.05), and non-measurable at day 11. Baseline weight (73.8±16.3) was higher than day 1 (72.3±15.8 Kg, p<0.05). T3 peak (325±63.1 ng/dL) was reached at a median of 1.5 hours (range 1–3.5 hours) after dosing, with an apparent elimination half-life of 20±9 hours. No difference in Hamilton depression scale was observed between day 1 and 11. No difference was observed between baseline (186.0±51.0) and day 1 (171.0±42.0) cholesterol, while on day 11 the level was significantly higher (230.3±53.2 mg/dL, p<0.05).
The substitution of LT3 for LT4 at a 1:3 ratio with thrice daily administration regimen provides adequate TSH suppression, while maintaining mean T3 levels within normal range, and resulting in weight loss. LT3 withdrawal results in TSH concentrations adequate for treatment over a 12-day period, with minimal hypothyroid symptoms. The PK data fit a two compartment model and simulations suggest that more satisfactory serum T3 levels were predicted with a thrice daily regimen.
Disorders of Thyroid Function Friday Poster Clinical
Agranulocytosis (AG), one of the most serious complications of antithyroid drug (ATD) therapy for Graves' disease, develops abrupty. Therefore periodic monitoring of granulocyte counts is not generally recommended.
Kuma hospital has the system that every Graves' patient under ATD treatment in outpatient clinic has examination of granulocyte counts in addition to serum thyroid hormone levels on each visit and if granulocyte counts is under 1000/uL (granulocytopenia, GP), warning is immediately sent to a physician. We evaluated the usefulness of this system.
Excluding patients who developed AG or GP at other hospital and were referred to Kuma hospital for therapy, we experienced 24 cases of AG and 34 cases of GP over the past 5 years. Among them, only 11 patients came to Kuma hospital directly or went to see other doctors because of infection symptoms (fever and or sore throat). Remaining 47 patients (81%) were found to have AG or GP by routine examinations. Notably 30 cases (52%) (8 AG and 22 GP) were completely asymptomatic. Three of them had high fever shortly thereafter. Although 17 patients had some mild infection symptoms, they ignored them and did not go to doctors. Most AG patients received granulocyte-colony stimulating factor (G-CSF) injection immediately after the diagnosis and 20 patients who did not show prompt response to G-CSF were hospitalized. No one died due to AG.
Recently we demonstrated the abruptness with which AG develops by showing that 111 of 211 Japanese AG patients had normal granulocyte counts within 2 weeks before onset. Concurrently, half of AG patients exhibited a more gradual decline in granulocyte counts (JCEM 2013). The Kuma hospital system works very well to discover AG or GP in patients with no or slight infection symptoms. Since 85% of AG develops within 90 days after ATD-therapy (JCEM 2013), we strongly recommend periodic monitoring of granulocyte counts for every patient with Graves' disease on ATD therapy, especially during the first few months of treatment.
Disorders of Thyroid Function Friday Poster Clinical
Myxedema coma (MC) is a rare, life-threatening form of decompensated hypothyroidism. The goal of this study is to evaluate and characterize the clinical and laboratory changes after treatment of MC with 500 mcg of IV L-thyroxine (LT4 load).
A case series of 45 patients with MC at LAC+USC Medical Center from 2004 through 2014 were retrospectively evaluated. Systolic blood pressure (SBP), diastolic blood pressure (DBP), pulse pressure (PP), heart rate (HR), temperature (T), sodium (Na), creatinine (Cr), hemoglobin (Hg), white blood cell count (WBC), and aspartate aminotransferase (AST) were evaluated for change after LT4 load. Average time from presentation to LT4 load was 27.3+/−18.9 hrs. At 24 hrs post LT4 load, median SBP decreased from 119 to 109.5 mmHg (−8%) and DBP decreased from 66 to 61 mmHg (−0.76%) before returning close to baseline by 48 hrs. Median PP increased from 43 to 46 (+6.6%) at 16 hrs before returning close to baseline at 48 hrs. Median HR decreased from 72 to 70 (−2.8%) before increasing to 74 (+5.4%) at 48 hrs. Median T decreased from 98.2 to 97.7 C from 0 to 48 hrs. At 24 hrs, median Na increased from 137.5 to 138 (+1%), median Cr decreased from 0.96 to 0.93 (−3.2%), Hg decreased from 11 to 10.1 (−8.2%), and median WBC increased from 7.2 to 8.6 (+19.4%). Median AST decreased to 53 from 55 (−3.6%) at 48 hrs. The changes in these clinical parameters demonstrate the direct effect of LT4 on the vasculature. While vasodilation occurred in the first 24 hrs, as indicated by the decrease in SBP and DBP, and increase in PP, HR did not increase until 48 hrs, consistent with the time needed for peripheral T4 to T3 conversion and the lack of T4 receptors on cardiac myocytes. The decline in median T after LT4 load may be due to dissipation of heat from vasodilation.
Iodine Uptake & Metabolism Friday Poster
Goiter and hypothyroidism due to iodine (I) deficiency is rare in the United States because of adequate I intake in most diets and salt.
A 67-yo woman presented with a history of hypothyroidism and goiter. Outside laboratory studies revealed serum TSHs between 2.2 and 12.54 uIU/ml (0.5–3.5 uIU/ml) and FT4 values 0.6 ng/dL to 0.8 ng/dL (0.93–1.7 ng/dL). TPO Ab was negative. A thyroid US demonstrated a heterogeneous thyroid with a left thyroid nodule 1.3x1x1.5 cm. L-T4 therapy was advised, but the patient declined due to her intolerance of all oral medications and all foods except for white organic rice, which had comprised her entire diet for at least 10 years. In order to maintain nutrition, she sprinkled liquid compounded vitamins, amino acids, and electrolytes over the rice.
Physical exam was normal except for a mildly enlarged thyroid gland with an irregular texture. We assessed the I content of the patient's organic rice diet, enriched with sea salt (no I), soluvit (no I), pediatric liquid multi-vitamin (no I), amino acid blend, electrolytes, and iodopen (100 ug NaI added to the entire rice diet every third day) and it contained no detectable iodine. A 24-hour urine I was markedly low at 14 ug/24 h (75–500 ug/24 h) with a creatinine of 1.11 g/24 hr (0.63–25 g/24 hr). Iodine measured in 7 urine samples obtained 1.5 h after ingestion of the rice diet (including iodopen enriched rice) was low, ranging from 16 to 57 ug/L (mean 33 ug/L, normal range 100–400 ug/L). A 24 h thyroid 123I uptake was elevated at 43.4%, and a scan showed diffuse distribution of the isotope.
1. Albeit rare in the US, severe I deficiency resulting in thyroid dysfunction may occur. 2. Urinary I is a reflection of recent I intake, but can be helpful in making the diagnosis of iodine deficiency. 3. An increased 24 h RAIU, while usually associated with hyperthyroidism, may be associated with I deficiency.
Disorders of Thyroid Function Friday Poster Clinical
HPLC measurement of thyroid hormone content in readily available “thyroid supportive” health supplements was reported in Thyroid 2013. Some contained clinically relevant amounts of T4 and T3. The authors noted that these amounts “potentially expose patients to the risk of thyroid level alterations, even to the point of developing iatrogenic thyrotoxicosis”. We explored the physiological consequences of their findings on circulating T4, T3 and TSH by computing the temporal dynamic responses to these oral dosage supplements in simulated hypothyroid and normal groups.
Our internet-based simulation tool THYROSIM conveniently implements these “what-if” experiments into a mechanistically-based model of human thyroid hormone and thyrotropin regulation dynamics. Evolution of this model has been reported in 5 Thyroid publications. It accurately reproduces a wide range of clinical study data reporting hormonal kinetic responses to large and small oral hormone challenges.
In these new simulations, we found T3 content in supplements has a greater deleterious effect than does T4. The accompanying figure illustrates a hypothyroid subject response - simulated with 50% glandular function receiving supplement #5 containing ∼ 32 mcg T3 twice daily, as prescribed on the package. Plasma T4 levels fall well below their normal range (from ∼80 to 10 mcg/L), T3 levels increase 3-fold to ∼3 mcg/L, and TSH falls to <0.5 mU/L. Results were similarly deleterious in simulated euthyroid subjects receiving 2 other products (#4 and #9) with significant T3 (∼ 25) and little (∼9) or no T4. In contrast, for supplements #2 and #3 containing both T3 (∼6 to 16 mcg) and T4 (∼17 to 92 mcg), simulated T3, T4 and TSH response levels are maintained within normal ranges, suggesting that central feedback regulation is doing its job at these higher T4 dose levels.
Clearly, the amounts of T3 in certain of these preparations can cause suppression of TSH leading to reduced serum T4 and diagnostic confusion as well as potentially raising serum T3 into the thyrotoxic range, with adverse effects on bone and heart. These simulations provide support for restrictions on their unregulated availability.
Simulated oral dosing hormone kinetic responses to taking OTC supplement #5 (dashed-green) over 30 days in mildly hypothyroid subjects (solid-blue). T3 in thyrotoxic range, with T4 and TSH greatly suppressed.
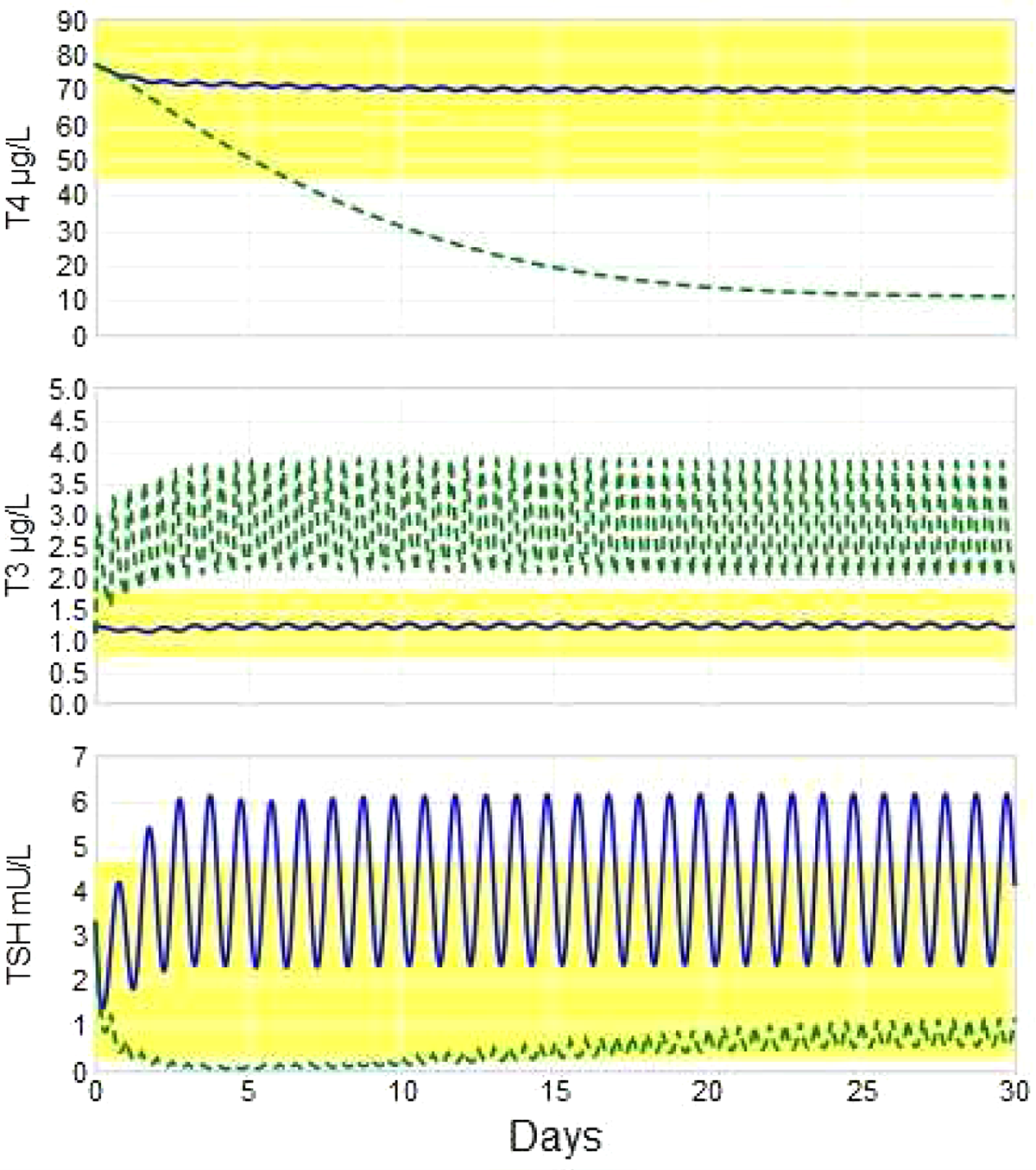
Disorders of Thyroid Function Friday Poster Clinical
Mucormycosis thyroiditis is rare and often seen as part of disseminated infection in immunocompromised patients, mainly with hematological malignancies.
We report 4 cases seen in our institution. We did chart review.
42 y/o woman with acute myelogenous leukemia (AML) presented after 6 months of stem cell transplant (SCT) with tender neck mass, with TSH-0.03 uIU/ml(0.27- 4.20), free T4(fT4)-3.2 ng/dl(0.93- 1.7). Mucormycosis was isolated from her neck mass and she died of disseminated infection 1 month after presentation. 61 y/o man with AML diagnosed with mucormycosis thyroiditis 6 months after SCT. He presented with neck pain and tremors. and TSH<0.01 mIU/ml and fT4>7.7 ng/dl. On proper antifungal treatment, he survived for 17 months but later died of mucormycosis pneumonia. 60 y/o man with mantle cell lymphoma diagnosed with mucormycosis thyroiditis 5 months after SCT. He presented with painful neck mass and anxiety. TSH<0.01 uIU/ml, fT4 8.7 ng/dl. He died one month later of disseminated infection. 18 y/o man with acute lymphoblastic leukemia developed mucormycosis thyroiditis 5 months after induction chemotherapy while on prophylaxis with fluconazole and caspofungin. His TSH- 1.09 uIU/ml and fT4- 1.04 ng/dl. His infection resolved with appropriate antifungal therapy and remained disease free for 1 year. All 4 patients were on azole antifungal prophylaxis at the time of diagnosis and treated with lipid based amphotericin B and posaconazole. Radiological evaluation showed hypoechogenicity on ultrasound, heterogeneous enhancement on CT and increased FDG uptake on PET scan. Fine needle aspiration was used for diagnosis.
Mucormycosis thyroiditis is a rare clinical entity and reported primarily at autopsy in patients with hematological malignancies. Clinical presentation is that of sub-acute thyroiditis with a painful neck mass. Mucormycosis thyroiditis has a poor prognosis despite aggressive antifungal and supportive therapy.
Disorders of Thyroid Function Friday Poster Clinical
Previous studies have shown that miscarriage rate of pregnant women with Hashimoto's Thyroiditis (HT) was higher than normal pregnant women because of the presence of TPOAb and TgAb. Meanwhile, higher TSH level has also been indicated as an important factor of miscarriage. Women who have HT tend to develop overt or subclinical hypothyroidism during pregnancy. Previous studies revealing the relationship between HT and miscarriage rate included HT pregnant women with high TSH level. To exclude the possibility that irregular TSH levels might have caused higher incidences of miscarriages, we looked at the effect of TPOAb and TgAb on miscarriage within pregnant women with normal TSH level. Then, we evaluated whether higher TSH levels were correlated to miscarriage even within normal TSH level.
We retrospectively selected subjects whose TSH levels were under 4.5 μIU/ml during first trimester without any medical treatment. Subjects with multiple fetal pregnant, antiphospholipid antibody syndromes, abortions, stillbirths, recurrent pregnancy losses were eliminated. Of those subjects, 367 pregnant women without thyroid antibodies were selected as control group and 468 pregnant women with the presence of TPOAb or TgAb were selected as HT group. We analyzed the miscarriage rate among those two groups. Then, we divided all subjects into 10 groups of increasing TSH levels and evaluated the miscarriage rate among those groups.
Miscarriage rate between control and HT groups was not significantly different.(P=0.1986) In multivariable analysis using logistic regression and adjusted for delivering age, FT4, TSH, TgAb, TPOAb. TSH levels were independent predictors of miscarriage.(OR 1.36, 95%CI 1.05–1.76, P=0.0173) Using Cochran-Armitage Trend Test to evaluate miscarriage rate among different TSH levels, a positive association to miscarriage was found in higher TSH levels.(P=0.0011)
Among pregnant women with normal TSH level, the miscarriage rate was not significantly different between HT and control groups. However the miscarriage rate among TSH levels was significantly higher in higher TSH level group. Our data demonstrated that higher TSH levels were more correlated to higher miscarriage rate than the presence of TPOAb and TgAb.
Disorders of Thyroid Function Friday Poster Clinical
Thyrotoxic periodic paralysis (TPP) is an alarming and potentially fatal complication of hyperthyroidism characterized by flaccid muscle paralysis and hypokalemia resulting from a massive intracellular shift of potassium. We report two cases of TPP caused by T3 toxicosis.
Case 1: A 27 year old black male presented with generalized muscle weakness after a calorie-rich meal. He reported weight loss, tremor, and diaphoresis for 6 months. Physical examination revealed a diffusely enlarged thyroid gland with bruit, 2/5 muscle strength, unlabored respiration, intact sensation and speech. Laboratory studies revealed low potassium level of 2.1 mmol/L, non-detectable TSH, free T3 of 23.8 pg/mL (1.81–4.06 mmol/L), and less impressive elevated free T4 of 4.48 ng/dL. A thyroid uptake scan was consistent with Graves' disease. Symptoms were relieved after potassium was replaced. No further attacks were reported after methimazole and propranolol were initiated. Case 2: A 35 year old Vietnamese male with Graves' disease status post radioactive iodine ablation 3 months prior presented with worsening intermittent muscle weakness. Laboratory studies revealed a potassium level of 1.4 mmol/L, low TSH, and elevated free T3 of 8.63 pg/mL. Free T4 was marginally elevated. An EKG showed first degree A -V block and prolonged QT. Potassium was emergently repleted. Symptoms resolved once potassium level reached 2.8 mmol/L. He was started on propranolol for several months until a euthyroid state was achieved.
The mechanism of TPP is not fully understood. Studies have shown that increased Na+-K+ ATPase activity stimulated by thyroid hormone, hyperadrenergic state, and hyperinsulinemia coupling with decreased outward K+ from the K2.6 membrane channel hypofunction predispose the sarcolemma to TPP.
With migration, TPP is not only seen in Asian populations. Graves' disease remains the most common etiology of TPP. This complication can affect undiagnosed or post-treatment thyrotoxic patients. Notably, free T3 levels were much more elevated than free T4 in the above cases.
Characterics Between the Two Graves' Disease Patients
Disorders of Thyroid Function Friday Poster Clinical
Postoperative hypocalcemia is the most common complication after total thyroidectomy requiring patients to take calcium and/or calcitriol supplementation. Low postoperative day 1 (POD1) parathyroid hormone levels (PTH) are predictive of hypocalcemia. We aim to determine if same day PTH could replace POD1 PTH in predicting the need for calcium supplementation.
We prospectively studied all patients that underwent total thyroidectomy between July 2012 and December 2013 at our institution. Serum PTH on the day of surgery was compared to POD 1 PTH in patients that did or did not receive same day calcium supplementation. Statistical analysis was performed using two-sided t-test.
197 patients underwent total thyroidectomy during the study period. One hundred twenty-four (63%) patients did not require calcium supplementation on the day of surgery. These patients had a higher PTH on the day of surgery when compared to POD 1 PTH (30.7±17.5 vs. 26.4±12.5 pg/dL, p=0.015). Correlation between PTH on the day of surgery and on POD1 was stronger in those with PTH≤20 pg/dL on the day of surgery compared to patients with PTH>20 pg/dL on the day of surgery (r=0.77 vs r=0.41). There was no drop in PTH from the day of surgery to POD1 in patients with same day PTH≤20 pg/dL. However, there was a significant drop in PTH from the day of surgery to POD1 in patients with same day PTH>20 pg/dL (p<0.01). Patients who did not receive calcium supplementation on the day of surgery experienced a larger decline in PTH between day of surgery PTH to POD1 PTH (p<0.01).
There is a statistically significant decrease in POD1 compared to day of surgery calcium levels in all patients in our study. This decrease was stronger in patients that did not receive same day calcium supplementation, specifically those with a postoperative PTH>20 pg/dL on the day of surgery. We believe decisions about calcium supplementation using same day PTH values should require a higher threshold than those used on POD 1.
Comparison of Same Day to POD1 PTH Trends in patients not receiving Calcium Supplementation by Same Day PTH Cut off of 20 pg/dL
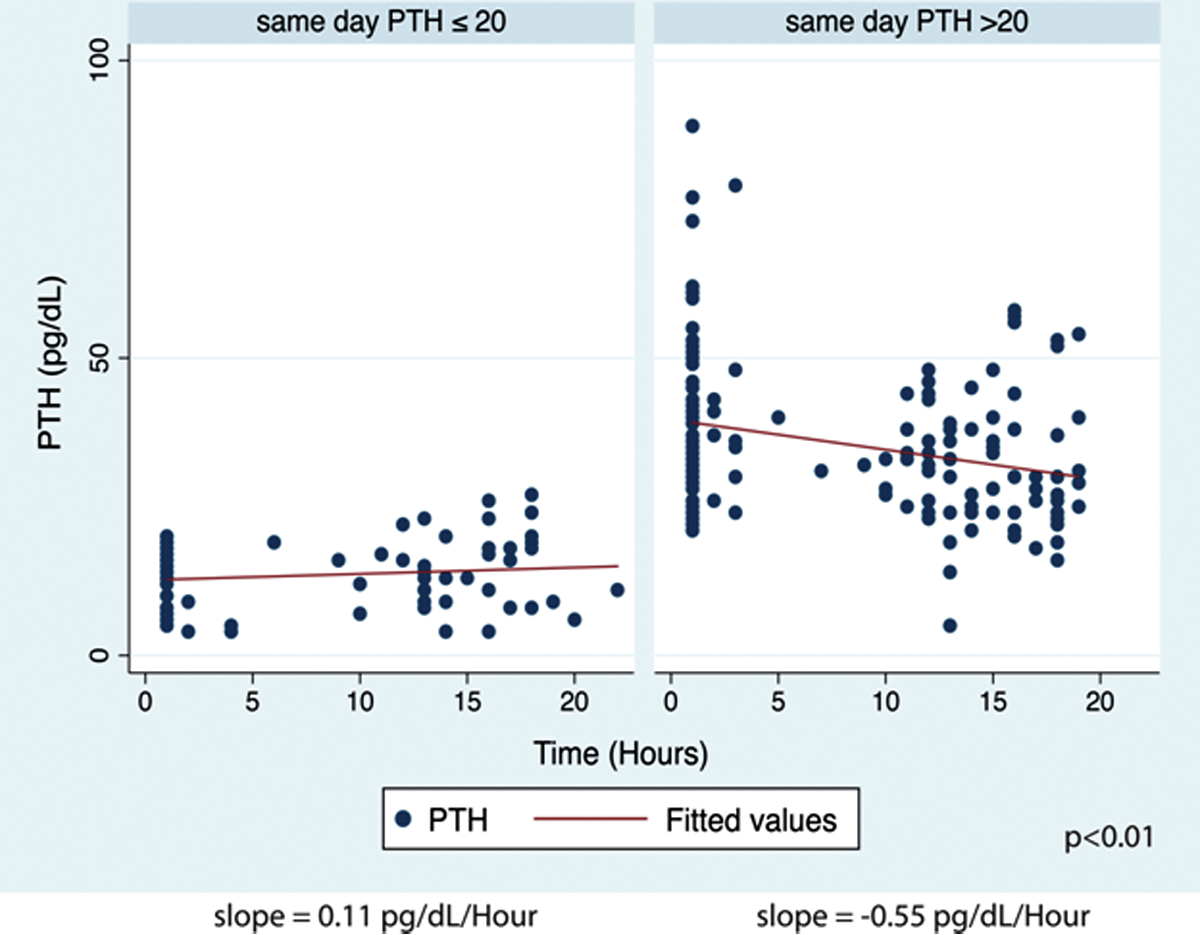
Disorders of Thyroid Function Friday Poster Clinical
To date, information regarding the epidemiology of chronic hypoparathyroidism and its clinical impact on those with the disorder has been limited. Because of its rarity, most publications present a single center's experience with a relatively small number of patients with hypoparathyroidism. PARADIGHM™, a global patient registry sponsored by NPS Pharmaceuticals, Inc., has been initiated to address this gap by characterizing the natural history and clinical features of chronic hypoparathyroidism under clinical practice conditions.
PARADIGHM™ is an observational registry that will provide long-term, prospective, clinical data from the largest cohort of patients with hypoparathyroidism to date. The registry is open to enrollment of patients of any age with chronic hypoparathyroidism of any etiology, regardless of treatment. Enrollment began in the United States in July 2013 and will begin in Europe in early 2015. Patients are recruited through physicians at centers qualifying as investigative sites. The target sample size is 900 patients recruited over a 7-year period, with follow-up data collection planned for at least 10 years. In addition to data on clinical status and treatment, patient demographics, family and medical history, patient-reported outcomes, healthcare utilization, and mortality, other clinical data concerning the psychosocial impact of hypoparathyroidism and associated complications and comorbidities will also be collected.
Preliminary data for patients with hypoparathyroidism enrolled in the registry are available. The majority of cases had a surgical etiology, usually resulting from thyroid surgery; in many cases, these surgeries were due to thyroid cancer.
Data from the registry will add to our understanding of hypoparathyroidism and assist the medical community in clinical, evidence-based decision making in the management of individuals with absent or insufficient parathyroid hormone.
Disorders of Thyroid Function Friday Poster Clinical
Amiodarone induced thyrotoxicosis (AIT) is a known clinical entity caused commonly due to iodine induced excessive synthesis of thyroid hormone, also known as type 1 AIT. However, in rare cases, it is due to amiodarone-induced inflammation of the thyroid tissue resulting in release of pre-formed thyroid hormones and hyperthyroid state or type 2 AIT. Distinguishing between the two amiodarone related hyperthyroid states is important, as both conditions have different treatment implications.
A 63 year old male on chronic Amiodarone therapy for paroxysmal atrial fibrillation, was seen in the Endocrinology department for concerns of hyperthyroidism. He reported 19 lbs weight loss in the past year and worsening hand tremor. Past history was significant for coronary artery disease, hypertension, morbid obesity and peripheral vascular disease with claudication. On examination, the thyroid gland was diffusely enlarged without tenderness or palpable nodules. No lymphadenopathy appreciated. Vital signs were unremarkable with a blood pressure of 110/60 mm Hg.
Thyroid function tests revealed a Thyroid Stimulating Hormone level of 0.01 mIU/mL (n=0.35–4.5 mIU/mL) and Free T4 of 2.7 ng/dL(n=0.6–1.2 ng/dL). Thyroid ultrasound with Color Flow Doppler (CFDS) showed normal to minimally reduced vascularity and a stable, previously biopsied benign nodule. Radioiodine uptake and scan had 0.6% (N=4–20%) and 0.2% (N=5-30%) uptake at 4 hours and 24 hours respectively. Screen for thyroglobulin antibodies returned negative. Thyroglobulin level was 22.6 ng/mL. Interleukin-6 level was elevated at 8.63 pg/mL (n=0.31–5 pg/mL). The patient was diagnosed with AIT type II and treated with low dose steroids (20 mg prednisone daily) for a month and then slowly tapered off following improvement in thyroid function tests.
Amiodarone induced hyperthyroidism still remains a diagnostic challenge due to incompletely understood pathogenesis, unreliable response to therapy and lack of a systemic approach. Besides thyroid function testing, ultrasound, radioiodine uptake and scan, IL-6 levels and CFDS aid in diagnosis and assessing the response to therapy in type 2 AIT. Steroids remain the mainstay for treatment of type 2 AIT.
Following administration of oral I123, Radioiodine uptake values at 4 hour and 24 hours were 0.6% (N=4–20%) and 0.2% (N=5–30%) respectively.
Iodine Uptake & Metabolism Friday Poster Clinical
Iodine is an essential element of thyroid hormone. Proper iodine intake is important during pregnancy for both fetal neurodevelopment and maternal thyroid function. Korea is known as high iodine intake area. However, there is no data regarding iodine status in Korean pregnant women. Therefore, we evaluate the iodine status of pregnant women in Korea using urine iodine concentration.
This study was an observational, prospective design. We enrolled 344 healthy pregnant women who visited Samsung Medical Center for routine antenatal checkup between April 2012 and September 2013. Iodine and creatinine concentrations were measured in spot urine samples.
The median urinary iodine concentration (UIC) was 422.3 μg/L and ranges from 19.0 to 13390.0 μg/L. Only 13.7% of subjects (47/344) were in adequate range of iodine nutrition based on WHO criteria. 65.1% (224/344) consumed iodine exceeding above requirements whereas, 21.2% (73/344) were categorized as insufficient in iodine intake. There was no difference in median UIC among three trimesters (P-value=0.953).
This is a first report of iodine status in normal pregnant women in Korea and the median UIC was 422.3 μg/L. Considering highly variable range of iodine intake, active education about proper iodine intake for the pregnant women in iodine excessive area is necessary. Further investigations about pregnancy iodine status and fetal outcomes are warranted.
Median and mean concentrations of urinary iodine according to trimesters
IQR: Interquartile range
Thyroid & Development Friday Poster Clinical
There are lots of efforts to prevent recurrent laryngeal nerve injury during thyroidectomy. This study was to evaluate the efficacy of intraoperative neuromonitoring (IONM) on voice performance after robotic thyroidectomy.
The study was based on a prospectively randomized series. Between June 2011 to September 2012, 50 patients with thyroid cancer who underwent robotic thyroidectomy in Korea university medical center were enrolled. Both the IONM and non-IONM groups consisted of 25 patients each. Voice handicap index (VHI), voice range profile (VRP) and laryngoscopy were used to test the patient's voice function. All voice evaluations were performed before surgery and at 2 weeks, 3 months and 6 months after the operation.
The Non-IONM and IONM groups had similar VHI results with progression of time postoperatively (p=0.507, p=0.502, p=0.825, respectively). In laryngoscopic findings, there was no palsy observed in both groups. VRP maximum frequency & intensity were not different between the two groups. However, VRP minimum frequency & intensity were statistically different between the two groups. No difference in the mean difference of VRP maximum frequency (p=0.212) & intensity (p=0.533) was observed between the two groups.
Neuromonitoring was effective in providing identification and function of the laryngeal nerves. However, we were not able to reveal the superiority of IONM in robotic thyroid surgery.
Thyroid Cancer Friday Poster Basic
AMPK has emerged as a potential therapeutic target for cancer treatment by regulating different cellular processes involved in carcinogenesis like cell proliferation, cell death and metastasis. Our group recently showed a higher AMPK expression in human papillary carcinomas compared to non-neoplastic tissue (Eur J Endocrinol 169:521, 2013). However, the pathophysiological role of AMPK in thyroid cancer is unclear. The aim of this study is to evaluate the role of AMPK in tumor cell biology in papillary thyroid carcinoma cell lineages
Human thyrocyte transformed cell lineage NTHY-ORI and two papillary carcinoma lineages BCPAP and TPC-1 were treated with the pharmacological activator of AMPK, AICAR (1 mM) for 24, 48 and 72 h. Cell cycle and apoptosis were evaluated by propidium iodide and Anexin V staining, respectively. For invasion and migration assay, cells were incubated in a transwell chamber with or without matrigel respectively and in the presence or absence of AICAR. For adhesion assay cells were pretreated with AICAR for 24 h and plated in a 96 well plate coated with matrigel.
The tumor cell lines BCPAP and TPC-1 showed higher basal phosphorylated AMPK compared with NTHY-ORI. The treatment with AICAR reduced the proportion of cells in G2/M phase in NTHY, TPC-1 and BCPAP indicating reduced cell proliferation after 24 h, 48 and 72 h of treatment respectively. Also, 24 h of AICAR incubation induced apoptosis of tumor cells BCPAP and TPC-1. Interestingly this effect was not observed in NTHY-ORI. The 24 h AICAR treatment reduced cell migration ability in the 3 lineages and reduced cell invasion ability of BCPAP cells. Cell adhesion to extracellular matrix was also reduced in BCPAP and TPC-1 cells treated with AICAR.
AMPK activation through AICAR treatment has an anti-proliferative, pro-apoptotic and reduced in vitro metastatic capacity in all thyroid cell lineages investigated. These data strongly suggests a potential anti-tumorigenic effect of AMPK activation on papillary thyroid tumor cells lineages. Our data also support that AMPK is potential therapeutic target for thyroid cancer treatment.
Thyroid Cancer Friday Poster Basic
Papillary thyroid carcinoma (PTC) and follicular thyroid carcinoma (FTC) are well-differentiated cancers that encompass 75 – 85% and 15 – 20% of all thyroid cancers, respectively. PTC is typically well managed with a 93% overall survival; however, the remaining have aggressive metastatic PTC. FTC is associated with up to 40% of all thyroid cancer related deaths while anaplastic thyroid carcinoma (ATC) is the most deadly form of thyroid cancer with a mortality rate near 100% due to its highly aggressive undifferentiated nature. In order to thoroughly research thyroid cancer, proper preclinical models must be used. Methods: However, the thyroid research community is hindered due to ∼50% of the models proven to be cross-contaminated from redundancy or cells are not of thyroid origin. In addition, it is challenging to develop new thyroid cell lines due to poor success rates.
However, the thyroid research community is hindered due to ∼50% of the models proven to be cross-contaminated from redundancy or cells are not of thyroid origin. In addition, it is challenging to develop new thyroid cell lines due to poor success rates.
Here we report the 18 STR validated thyroid cell lines including 5 new ones (LAM136, JEM493, EAM306, SDAR1, SDAR2) that should be used for thyroid research purposes. All newly established cell lines must be validated by a short tandem DNA repeat (STR) profile that matches the original tumor tissue. Further validation should include: histology of tumor, patient history (if possible), cell line image, thyroid markers [TSHR, PAX8, TTF1, NIS, PDS, TPO, and TG], growth curves, tumorigenicity, and known thyroid mutations such as p53, Rb, PTEN, PIK3CA, RAS, Tert, RET/PTC and PAX8/PPARgamma.
This standard of characterization will prevent future cell line cross-contamination and ensure that only valid preclinical models are used for thyroid research.
Thyroid Cancer Friday Poster Basic
Molecular studies of papillary thyroid cancer (PTC) in atomic-bomb survivors indicated that the echinoderm microtubule-associated protein-like 4 (EML4)-anaplastic lymphoma kinase (ALK) fusion gene occurs more frequently in 1) PTC cases exposed to ≥5 mGy, 2) those with no RET, NTRK1, BRAF, and RAS gene alterations, and 3) those showing solid/trabecular architectures in the cancerous regions. Although these findings strengthen the hypothesis that the EML4-ALK fusion gene plays an essential role in radiation-induced PTC, whether or not the fusion gene is a result of radiation is yet to be clarified.
In the present study, we conducted in vitro X-ray irradiation experiments using immortalized human thyroid epithelial cells and investigated the occurrence of EML4-ALK fusion gene in the irradiated cells using RT-PCR method.
Preliminary results obtained in irradiated NThyori-3 cells indicated for the first time that in vitro X-ray irradiation induced ALK gene rearrangement, i.e. EML4-ALK fusion gene, in immortalized human thyroid epithelial cells.
These findings suggest that in vitro X-ray irradiation induces not only RET/PTC rearrangements but also EML4-ALK fusion gene in human thyroid cells.
Thyroid Cancer Friday Poster Clinical
Up to 20% of patients undergoing total thyroidectomy may present with hypocalcemia postoperatively due to hypoparathyroidism. Although usually transient, severe hypocalcemia may result in arrhythmia or tetany. Teriparatide (recombinant human parathyroid hormone 1–34) raises serum calcium levels. We hypothesized that teriparatide use in patients with post-thyroidectomy hypoparathyroidism would expedite relief from symptomatic hypocalcemia and reduce length of hospital stay when compared to standard therapy.
Hospitalized patients with severe, symptomatic hypocalcemia post-thyroidectomy were treated with teriparatide (20 micrograms subcutaneously twice daily for 1 week, then daily for 2 weeks), and standard therapy (calcium supplementation and calcitriol±hydrochlorothiazide). For this analysis, subjects were matched with subjects with post-thyroidectomy hypocalcemia of similar degree who had received standard therapy only.
8 hospitalized patients (cases) received teriparatide after 12–24 hours of standard therapy. 8 control subjects were matched on gender, age (41.4±11 vs. 42.8±11.8 years, cases vs. controls) and pre-therapy calcium values (mean nadir calcium 6.9±0.5 mg/dL in both groups). Mean BMI was 26.5 kg/m2 in cases and 28 kg/m2 in controls (P=0.37). Most subjects underwent thyroidectomy for the treatment of papillary thyroid cancer (6/8 cases and 7/8 controls, P=0.35). Cases were dismissed from hospital at a mean of 1.1±0.4 days versus 2.4±1.1 days after the same clinical point was reached in controls (P=0.01). Upon dismissal, patients had similar calcium values (8.7 mg/dL for cases, 8.3 mg/dL for controls, P=0.1). All cases remained asymptomatic during teriparatide therapy. At 4 weeks (1 week after stopping teriparatide) 1 patient in each group still had mild symptoms. Calcium supplementation and serum calcium levels were comparable between groups. No adverse events were associated with teriparatide use.
Teriparatide is well tolerated, and corrects severe post-thyroidectomy hypocalcemia rapidly, allowing for earlier hospital dismissal. A larger scale randomized trial should be pursued to verify these results and to assess long-term impact of therapy on clinical outcomes.
Thyroid Cancer Friday Poster Clinical
Papillary thyroid cancer (PTC) is the most common thyroid malignancy in pediatric patients but there is a paucity of data related to the difference in outcome for children and adolescents with radiogenic and non-radiogenic carcinomas. The aim of this study was to compare long-term outcome of PTC in children and adolescents with and without a history of radiation exposure.
Survival rate from the date of initial surgery until the according event of interest or loss of contact was assessed with the Kaplan-Meier estimator. Treatment results were evaluated through Children's Cancer Sub-Registry of Belarus.
A survival analysis for 1078 children and adolescents operated for post-Chernobyl PTC during the years 1990–2005 (followed up for a median of 14.7) and 225 patients aged ≤18 years old treated for sporadic PTC from 1986 to 2010 (followed up for a median of 6.6 years) was conducted. The 20-year treatment result for 974 (90.4%) of 1078 post-Chernobyl patients was a complete clinical remission status; 77 (7.1%) of 1078 children had relapses. Secondary malignancies developed in 10 (0.9%) patients, and 21 (1.9%) patients died. In 225 children and adolescents operated for sporadic PTC 25-year treatment results were evaluated. The outcomes within the evaluated period were as follows: 212 (94.2%) of 225 patients had a complete clinical remission status; 10 (4.5%) had relapses and 3 patients (1.3%) died. Only two patients operated for post-Chernobyl PTC died due to the cancer disease or cancer-related post-therapeutic disease and only one patient operated for sporadic PTC died due to the post-surgical complications. The comparative analysis have shown that the differences between overall (96.9%±SD 0.9% with a median follow-up of 16.21 years vs 86.3%±SD 7.5% with a median follow-up of 6.76 years) and relapse-free survival for patients with radiation induced PTC (92.3%±SD 0.9% with a median follow-up of 15.36 years) vs their counterparts (84.6%±SD 6.4% with a median follow-up of 6.58 years) was insignificant (p=0.8774).
Children and adolescent with PTC have an excellent prognosis regardless of the etiology of carcinoma.
Thyroid Cancer Friday Poster Clinical
Indeterminate thyroid nodule cytology labeled Atypia of Undetermined Significance (AUS) often undergoes further diagnostic analysis with the Afirma Gene Expression Classifier (GEC). GEC reclassifies these indeterminate cytologies as either high probability of being benign or suspicious for malignancy. At Cleveland Clinic Florida we aimed to assess the clinical validity and utility of GEC in the evaluation of AUS cytology.
We conducted a study of a retrospective cohort of patients from January, 2012-January, 2014 who had FNA of thyroid nodules with AUS cytology and underwent GEC testing. Information regarding patient demographics, nodule characteristics, FNA and GEC results, final recommendations by our endocrinologists and subsequent clinical or surgical follow up were collected.
Cleveland Clinic Florida has an overall incidence of AUS at 5%. 191 GEC reports after thyroid nodule FNA's were reviewed: 151 cases were reported as AUS-1 (AUS on 1st FNA). Of the 151 AUS-1, 70 (46.4%) were sent for GEC with 46 classified as suspicious. All 46 patients underwent thyroid surgery. Only 24 (52.2%) had thyroid carcinoma on histopathology. The remaining 81 AUS-1 were sent for a 2nd FNA: 27 (33.3%) were benign and 54 were reported as AUS-2 (AUS on 2nd FNA). 40 (74.1%) cases of these 54 were reported suspicious after GEC all of whom underwent thyroidectomy with 34 (85%) having malignancy confirmed on histopathology.
In our practice the performance of GEC testing in conjunction with the first biopsy showing AUS was associated with a low level of diagnostic accuracy. Surgery directed by suspicious GEC results in this setting was associated with only a 52% likelihood of malignancy. When FNA biopsy was repeated after the first cytology showing AUS, one-third were found to be benign. The diagnostic accuracy of GEC testing was markedly higher at 85% when it was requested only after two consecutive AUS cytologies. Our data suggests that reserving GEC testing for those nodules with repeated AUS cytologies would reduce the numbers of unnecessary thyroidectomies. Prospective studies with long-term follow up are required to evaluate the efficacy of this protocol for accurate detection of thyroid malignancy.
Thyroid Cancer Friday Poster Clinical
An autocrosslinked polysaccharide(ACP) gel(Hyalobarrier®) is an ACP derivative of hyaluronic acid(HA) that displays the biocompatibility properties of HA, but has a higher viscosity which optimizes its residence time. It has been demonstrated that ACP gel prevents adhesion after abdominal or pelvic cavity surgery. The aim of the present study is to compare the effect and safety between ACP gel(Hyalobarrier®) and poloxamer/sodium alginate(P/SA)(Guardix-SG®), in preventing adhesions after thyroidectomy.
This prospective, non inferiority, randomized, double blind, multicenter, phase III study investigates the anti-adhesive effect and safety of ACP gel in comparison with P/SA for 12 weeks. Patients were randomly assigned to receive ACP gel(n=97) or P/SA(n=96). As for assessing the effect and safety, the primary endpoint was the esophageal motility assessed by marshmallow esophagography and secondary endpoints included: changes in SW(swallowing discomfort), SN(hypesthesia or paresthesia on the operative site), SII-6(Swallowing Impairment Index-6), adhesion severity VAS(Visual Analog Scale), VHI-30(Voice Handicap Index-30), grades of POST(Post-Operative Sore Throat), laryngoscopic finding of vocal cords, frequencies and intensities in the VRP(Voice Range Profile). Safety endpoints included: adverse events, changes of hematology, blood chemistry, blood coagulation, urinalysis, thyroid function, vital signs, physical examinations. This study was registered with ClinicalTrials.gov, number NCT01696305.
There was no difference in the esophageal motility assessed by marshmallow esophagography as the primary endpoint (p=0.7428, one-sided 97.5% CI −5.10) with a non-inferiority margin of 9.2% between ACP gel and P/SA. In addition, there was no difference in the secondary endpoints and safety endpoints between the two groups.
The non-inferiority in the effect and safety of ACP gel to P/SA was established in this study. The ACP gel seems to be effective and safe in preventing adhesions after thyroidectomy.
Normal esophageal motility assessed by marshmallow esophagography
the Fisher's exact test is used to test a significant difference in proportions between treatment groups. The difference in proportions between treatment groups and its one-sided 97.5% confidence interval
Thyroid Cancer Friday Poster Clinical
Neck nodal metastases (NNM), which can be found at diagnosis in almost 80% of children and adolescents with papillary thyroid carcinoma (PTC), may, despite definitive thyroidectomy and remnant ablation, recur or persist in up to 15–20% during twenty postoperative years. Conventionally, such regional “recurrences” are treated with further reoperative neck surgeries or higher doses of therapeutic radioiodine. UPEA (Surgery 154: 1448, 2013) has, to date, not been described in the management of recurrent NNM in adolescent PTC.
We studied the long-term efficacy of UPEA in five adolescents (all girls aged 13–19 years; 2 stage II, 3 stage I) ablated at our institution during 2001 through 2012. Prior to UPEA, all had undergone total thyroidectomy and nodal dissection, followed in 4/5 cases by radioiodine treatment (mean 167 mCi, range 69–350). Cytologic diagnosis of eight NNM was confirmed by ultrasound-guided biopsy. UPEA with 95% ethanol, injected under ultrasound-guidance directly into the NNM, was usually performed in two outpatient sessions; the two youngest patients (ages 13 and 14) received minor intravenous sedation.
Eleven injections (averaging 0.4 cc) were used to treat eight nodes (mean diameter 8 mm). After UPEA, all NNM (4 central; 4 lateral) decreased in size and had no Doppler flow; 6/8(75%) disappeared on rescaning. Latest median serum thyroglobulin, on thyroxine suppression, in 4 patients without Tg antibodies was 1.1 ng/ml. None of the eight UPEA-treated NNM, followed on average for 7.3 years (range 24–162 months), required further intervention. None of the ablated adolescent patients developed temporary or permanent hoarseness. Only one has undergone further surgical intervention for two non-ablated NNM.
UPEA for selected persistent/recurrent NNM in adolescents with PTC has proved both safe and effective. It is also considerably cheaper and less dangerous than the alternatives of re-exploratory surgery or further treatment with higher radioiodine doses.
Thyroid Cancer Friday Poster Clinical
Advances in the early diagnosis and treatment of papillary thyroid carcinoma (PTC) have made routine radioactive iodine (RAI) treatments unnecessary in many low and intermediate risk patients. We have previously reported on a novel prospective strategy to select patients who can avoid unnecessary radiation using post-surgical stimulated thyroglobulin (Stim-Tg) and neck ultrasound. The present report extends our follow-up observations to 6 years.
Patients with low/intermediate risk PTC, tumors ≥1 cm and undetectable anti-Tg antibodies were prospectively followed after total thyroidectomy and selective therapeutic central compartment neck dissection. Low/intermediate risk was defined as PTC confined to the thyroid or central (level VI) lymph nodes. Stim-Tg and neck ultrasound were performed approximately 3 months after surgery and used to guide RAI treatment selection. Patients with Stim-Tg<1 μg/L did not receive RAI while those with Stim-Tg>5 μg/L routinely did. Those with Stim-Tg 1–5 μg/L received RAI on the basis of several clinical risk factors. Patients were followed prospectively for a mean of 6 years with serial neck ultrasound and basal/stimulated thyroglobulin measurements.
Among the 129 patients, 84 (65%) had undetectable Stim-Tg after initial surgery, 40 (31%) had Stim-Tg of 1–5 μg/L, and 5 (4%) had Stim-Tg>5 μg/L. RAI was administered to 8 (20%) patients with Stim-Tg 1–5 μg/L and 5 (100%) with Stim-Tg>5 μg/L. Using this approach, RAI therapy was avoided in 17/20 (85%) patients with tumors >4 cm, 72/81 (89%) patients older than 45 years and 6/9 (67%) patients with central lymph node involvement. To date, 116 (90%) patients in this cohort have not received RAI therapy with no evidence of recurrence, whereas among the 13 patients who received RAI, 1 (8%) had a pathological recurrence.
Using the proposed Stim-Tg and neck ultrasound personalized criteria, RAI can be avoided in the majority of low/intermediate risk PTC patients. Moreover, our observations demonstrate that traditional risk factors previously considered to favor RAI treatment are not always concordant with this personalized strategy and may lead to overtreatment.
Thyroid Cancer Friday Poster Clinical
Circulating cancer cells (CTC) are making a major impact in the management of breast, colorectal, castration resistant prostate and other cancers. Unique markers e,g Thyroglobulin, Sodium Iodide Symporter (NIS), TTF-1, BRAF, in differentiated thyroid cancer (DTC), and Calcitonin for medullary thyroid cancers (MTC) in addition to the common epithelial markers CK-19 and EpCam make this cancer more suitable for detection of CTC than other solid tumours.
A pilot study to detect CTC in 6 DTC and 1 MTC patients. With the ethical approval of the Newcastle Cancer Centre Biobank, 8 ml whole blood was collected into CellSave (veridex) blood collection tubes and processed within 48 hours. The samples were subjected to red blood cell lysis and fixation followed by depletion of CD45 positive leukocytes by immuno-magnetism using a CD45 antibody. The remaining cells were permeabilised and stained with Epcam - PerCPcy5.5, CK - PE, CD45 - PEcy7, Vimentin - AF647, Sodium iodide symporter (NIS) - TR & Thyroglobulin (THY) - FI, as well as DAPI as a nuclear stain. The remaining stained cells were individually imaged on an Imagestream imaging flow cytometer.
Successfully ablated DTC patients had no or few CTCs detected. 1 patient with metastatic DTC and 1 with metastatic MTC had numerous CTCs detected.
Our results are very exciting. In this small study there was excellent correlation between CTC enumeration and clinical status because of presence of unique markers in DTC and MTC. Enumeration of CTCs in DTC might help the following: 1. Molecular risk stratification by assessing tumour cell burden. 2. Selection of patients for radioiodine ablation. 3. Molecular characterisation of ablation success. 4. Diagnosis of indeterminate thyroid nodules. 5. An adjunct to thyroglobulin assay which is unreliable in 25% cases of DTC due to thyroglobulin antibody inference Larger studies are planned.
Thyroid Cancer Friday Poster Basic
Since 2008 the National Cancer Survivorship Initiative in the UK has aimed to support services which will ensure that the long term physical and psychological needs of cancer patients are met. Generally thyroid cancers are considered to be indolent, highly treatable and curable. Because of this there appears to be a lack of survivorship initiatives to help patients living with and beyond thyroid cancer diagnsosis and treatment
To identify whether the Nurse Led Clinic can actively screen for survivorship issues All patients reviewed in the nurse led clinic were sent holistic assessment tools two weeks prior to their appointment to complete.
Common areas of concern identified were fatigue, low mood, finance and work related concerns, coping with dependents, relationship issues, sleep disturbance, weight gain, voice problems, dry mouth, osteoporosis risk, atrial fibrillation and anxiety about recurrence. After clinical assessment the Thyroid Nurse Specialist would give appropropriate advice and if required refer on to appropriate specialist.
Ongoing use of the holistic assessment tool has identified common physical and psychological implications of thyroid cancer diagnosis and treatment. Identifying these area of concerns has led to the development of services including patient centred education days which enable patients to understand their disease and management, clinical psychology input for thyroid specific patients - (one to one, group work - Moving on Group, Pilot of patients perceptions of psychological support with thyroid cancer), ongoing relationships with the Butterfly Thyroid Cancer Trust, Macmillan and Maggies Centre (Hospital on site pateint support centre). Satisfaction surveys support this framework and Multi-disciplinary team working is essential.
Thyroid Cancer Friday Poster Clinical
Accelerated repopulation of tumour cells during radiotherapy (RT) is an important cause of radioresistance and consequent local relapse. 18F-Fluorothymidine (FLT) is a thymidine analogue which measures cell proliferation. Correlation between Ki-67 score and FLT uptake has been demonstrated in some cancers. FLT uptake reflects the fraction of tumour cells in S-phase and is high in malignant tissues. Increased FLT uptake on PET CT has the potential to identify tumour subvolumes with a high density of actively proliferating cells which can be targeted for focused RT dose escalation (RDE) to improve local control. One small study has reported on FLT to diagnose postoperative differentiated thyroid cancer (DTC) metastases: sensitivity 50%, specificity 91%. To our knowledge, FLT PET has not been evaluated to guide RDE in Iodine Refractory DTC needing RT.
THRIFT is a single-centre study to assess the feasibility of FLT-PET CT scanning in refractory DTC patients who are planned for radical RT for recurrence in the neck. Dose-escalated RT plans will be generated in patients with FLT-avid disease. Participants undergo a pre-treatment FDG and FLT-PET CT scan in the RT treatment planning position. The first patient recruited was diagnosed with pT3N1b papillary thyroid carcinoma in 2010 and treated with total thyroidectomy (R1 resection due to carotid encasement), level VI neck dissection, radioiodine ablation and 2 therapy doses of radioactive iodine. FDG-PET CT for rising thyroglobulin showed residual disease. It was decided to treat him with RT.
Two lesions in the right side of neck and supraclavicular fossa were apparent on CT. FDG-PET CT demonstrated marked focal uptake within the thyroid bed; 33 mm max transverse diameter; SUVmax 6.9, and right supraclavicular fossa; 19 mm max transverse diameter; SUVmax 10.3. FLT-PET CT showed no focal uptake within the thyroid bed or neck.
FDG-PET CT demonstrated markedly avid lesions in the neck that could be used to guide RT volume definition. In this patient, FLT-PET CT would be of no additional value in RT planning. Further patients are being recruited to the study and Ki-67 scores will be assessed to help evaluate the role and significance of FLT-PET CT in DTC patients.
Images of man with elevated thyroglobulin level 32 (TSH<0.05) after repeated radioiodine ablation. Left image: FDG-PET CT demonstrates intense FDG uptake in right thyroid bed and supraclavicular region. Right image: FLT-PET CT demonstrates no significant uptake in areas excluding normal proliferating bone marrow.
Thyroid Cancer Friday Poster Basic
Chronic inflammation plays an important role in carcinogenesis, and inflammatory tumor-associated macrophages have a deleterious effect in this process. In thyroid carcinoma (TC), proinflammatory cytokines such as tumor necrosis factor (TNF) and interleukin-1β (IL 1β) decrease the expression of the natrium iodine symporter (NIS) and negatively influence cell differentiation. The aim of the present study was to assess the interplay between TC cell lines and the differentiation of monocytes into macrophages, and their influence on the release of inflammatory mediators.
TC cell lines TPC1, BC-PAP and FT133 and HeLa cell line were co-incubated with human monocytes in a trans-well system. Release of cytokines and transcriptomics profiles of the immune cells and of the TC cell lines were investigated.
TC cell lines grown in homeostatic conditions in-vitro did not release the production of proinflammatory cytokines. No release of cytokines were observed after stimulation with Toll-like receptors ligands either, with the exception of TPC1 cells that released low amounts of IL-6 upon stimulation with the TLR4 agonist LPS. In contrast, co-incubation of TC cell lines with human monocytes in a trans-well system led to differentiation of the immune cells into macrophages with a strong proinflammatory profile, that produced 3- to 5-fold more proinflammatory cytokines compared to control macrophages (p<0.05 for all cytokines). This effect was specific for TC cell lines, as a control experiment using HeLa cells failed to exert a similar effect. Transcriptomic profiles of the macrophages incubated with TC cell lines display a chronic inflammatory profile. In turn, the effects of the macrophage-derived inflammatory mediators on the differentiation programing of the TC cell transcriptome is also investigated.
The interplay between TC cells and the immune system leads to macrophages with a strong inflammatory profile, and the resulting inflammation has in turn the capacity to influence the differentiation status of the malignant cells.
Thyroid Cancer Friday Poster Clinical
Shoulder morbidity is a frequently reported complaint after neck surgery. However, no data are available for patients with differentiated thyroid carcinoma (DTC) and hence, its impact on quality of life (QoL) is unknown. Moreover, there are no known predictors of shoulder morbidity in this specific patient population. Aim: To assess the prevalence of shoulder morbidity after DTC surgery and its relation to QoL and clinical characteristics.
The prevalence of shoulder morbidity and its relation to clinical characteristics and QOL after DTC surgery (n=109) was compared to a healthy control group (n=80) and a group of patients undergoing thyroid surgery for benign thyroid pathology (n=59). Main outcome measures: Prevalence of shoulder complaints, results of the Disabilities of the Arm, Shoulder and Hand questionnaire (DASH) and the European Organization for Research and Treatment of Cancer, Quality of Life Questionnaire-C30 (EORTC QLQ-C30).
DTC patients, on average 10.2 years after surgery, reported a 58.7% prevalence of shoulder morbidity, which was significantly more than the 13.8% reported by healthy controls (p<0.01). Of the patients who had surgery for benign causes 50% reported schoulder complaints. DTC patients scored worse than healthy controls on all different DASH subscales and EORTC QLQ-C30. Bivariate association analysis identified level V neck dissection, spinal accessory nerve damage and employment status as being associated with the prevalence of shoulder complaints and DASH score. Prevalence of shoulder complaints and DASH scores were significantly correlated to EORTC-QLQ30 scores. Only 11.9% of DTC patients received preoperative information on possible shoulder morbidity and only 34.9% received additional care for their shoulder complaints.
Shoulder morbidity is an important and highly prevalent problem in DTC patients. Level V neck dissections and spinal accessory nerve lesions should be limited and only be performed when there is a clear oncologic benefit expected. Information provision to the patient should be improved and additional care should be provided when shoulder morbidity arises after surgery, especially because this study shows a strong correlation between shoulder complaints and QoL.
Thyroid Cancer Friday Poster Clinical
Second malignancy status is a risk factor for death in Adolescents and Young Adults (AYA) with thyroid cancer (TC). This study investigates whether age at primary malignancy (PM) (pediatric vs. AYA) is an independent predictor of overall survival for AYA TC patients that have survived at least five years from their initial cancer.
SEER multiple primary session was used to identify all secondary TC cases in patients ages 15–39 in the SEER 9 (1973–2010) and 13 (1992–2010) databases. Patients were categorized by age at primary malignancy (pediatric: <15 years vs. AYA: ages 15–39) and stratified by 5-year survival from their PM. Kaplan-Meir and Cox-proportional regression analysis determined overall survival.
542 cases of secondary AYA TCs were identified; 71 had a primary pediatric malignancy and 471 a primary AYA malignancy. Only 3 patients died of thyroid cancer (all AYAs, p>0.1). 5-year survivors of a pediatric PM had a mean overall survival of 35.76 years whereas 5-year survivors of an AYA PM had a mean survival of 33.22 years (p=0.023). Additional survival differences in these 5-year survivors occurred by race, individual site of PM (not hematologic vs solid), stage of PM, marital status, and having ≥3 independent primary tumors (all p<0.05). However, thyroid tumor characteristics, stage and treatment did not influence survival. Multivariate cox regression demonstrated that patients diagnosed with a PM at ≥15 years of age had a 5.43 relative risk of death (CI: 1.75–16.80) after TC diagnosis compared to those with a prior pediatric PM. Black race (HR: 6.25, CI: 2.05–19.02) and having ≥3 independent tumors (HR: 3.59; CI: 1.62–7.96) also increased one's risk of death in these patients.
Secondary AYA TCs that develop in 5-year survivors of other AYA malignancies have a worse survival than TCs that develop in 5-year survivors of a pediatric malignancy. Although TC is not the cause of death in these patients, it could have an additive effect on the biology and prognosis of the primary AYA malignancy in these patients.
Thyroid Cancer Friday Poster Clinical
Over the last 15 years there has been a change in clinical practice for the detection of recurrence in patients with papillary thyroid cancer (PTC). Recurrence was previously detected by clinical examination supplemented with cytology. However, neck ultrasound and thyroglobulin are now widely used for surveillance to detect recurrence. With the rapid rise in low-risk PTC over the past 15 years, the aim of our study was to justify the increasing use of neck ultrasound in low-risk patients.
1746 patients undergoing total thyroidectomy for PTC between January 2000 and December 2010 were identified from an institutional database. 752 (43.1%) were categorized as low-risk by American Thyroid Association risk stratification and included for analysis. The number of ultrasound examinations for each patient was recorded by retrospective chart review. The number of ultrasounds per patient, per year (patient-year) of follow up was then determined. Follow-up and imaging details were recorded between January 2003 and December 2012. The number of deaths from disease and recurrences were recorded.
The median age was 48 years (range 16–83) and the median follow-up was 34 months (range 0–148). Between 2003 and 2012, the number of ultrasounds per patient-year of follow-up increased 5.3-fold (Figure 1). In 2000, there were 15 low-risk PTC patients treated while in 2010, there were 142. In 2003, there were 11 ultrasounds for 69 patient-years of follow-up, or 0.16 ultrasounds performed per patient-year. By 2012, there were 247 ultrasounds for 290 patient-years of follow-up, or 0.85 per patient-year (Figure 1). Over the same time period, 3 structural recurrences were detected with no disease related deaths.
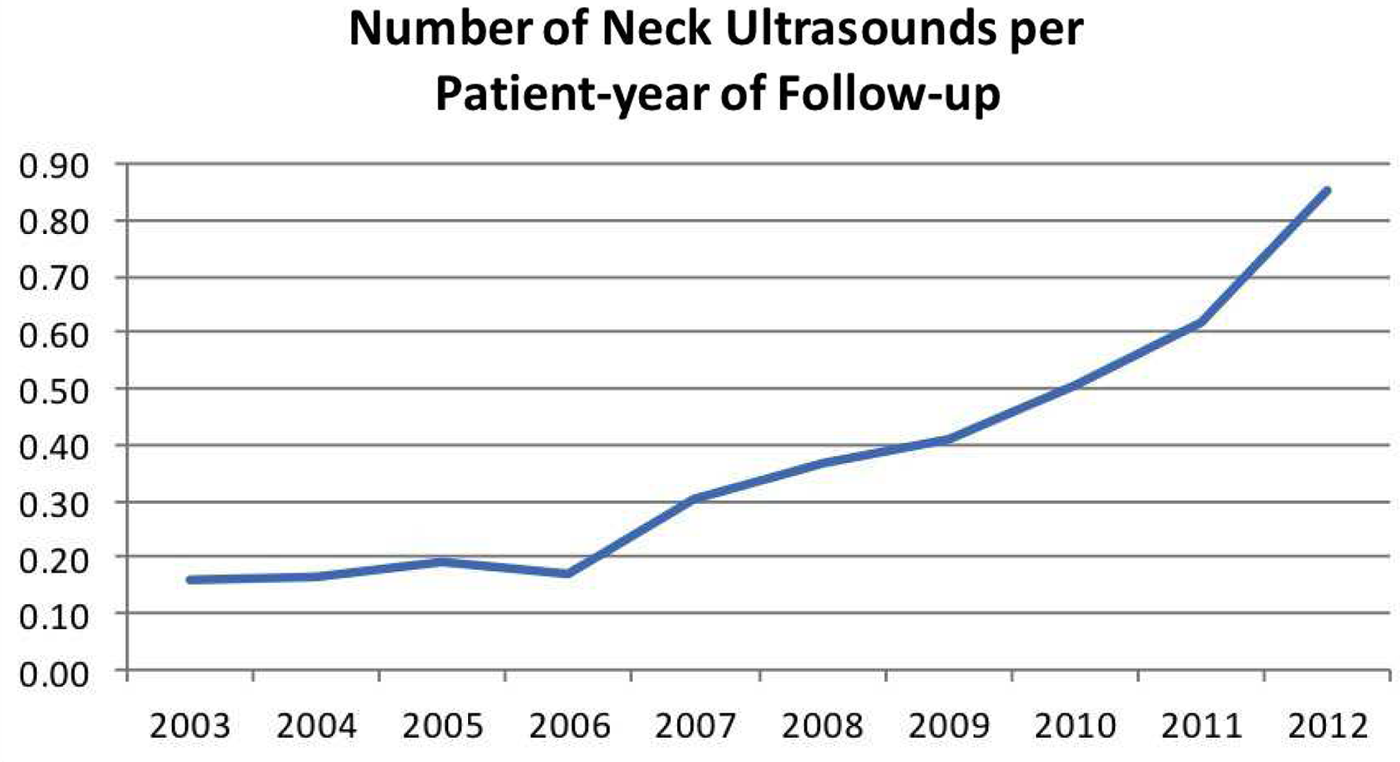
Number of neck ultrasounds per patient-year of follow-up
At our institution, the annual use of neck ultrasounds increased 5.3-fold per low-risk PTC patient over a decade. With only 3 structural recurrences detected, the routine use of neck ultrasounds for surveillance of these patients may not be justified.
Thyroid Cancer Friday Poster Clinical
It is not uncommon for patients with low-risk papillary thyroid cancer, managed with thyroid lobectomy, to have microscopic multifocal tumors. For these patients, the American Thyroid Association management guideline advocates completion thyroidectomy (Recommendation 29). The aim of this study is to determine if multifocal disease managed with lobectomy alone is associated with poorer outcomes.
An institutional database of 3364 previously untreated patients with differentiated thyroid cancer operated between 1993 and 2010 was reviewed. Patients with non-papillary histologies, more than lobectomy, unresectable disease, distant metastases at presentation, and those in whom multifocality could not be determined were excluded. This left 551 lobectomy patients for analysis, of whom 400 (72.6%) had unifocal disease (UFD) and 151 (27.4%) had multifocal disease (MFD) (Figure 1). The rates of immediate completion thyroidectomy, overall recurrences and disease related deaths were compared between the 2 groups.
The median ages of the UFD and MFD groups were 44 years (range 4–91) and 45 years (range 19–86) respectively. The median follow-up times for each group were 53 months (range 1–244) and 51 months (range 1–232) respectively. The rate of immediate completion thyroidectomy were similar between the MFD and UFD groups (12 (7.9%) vs. 32 (8.0%)) (Figure 1). There were no disease specific deaths in either group. The rates of recurrence in the observed lobectomy patients were similar between the 2 groups; 1 patient developed regional lymph node recurrence in each MFD and UFD group. The 5 yr RFS was 100% for both MFD and UFD groups. Univariate analysis showed that multifocality was not a predictor for recurrence (p=0.456).
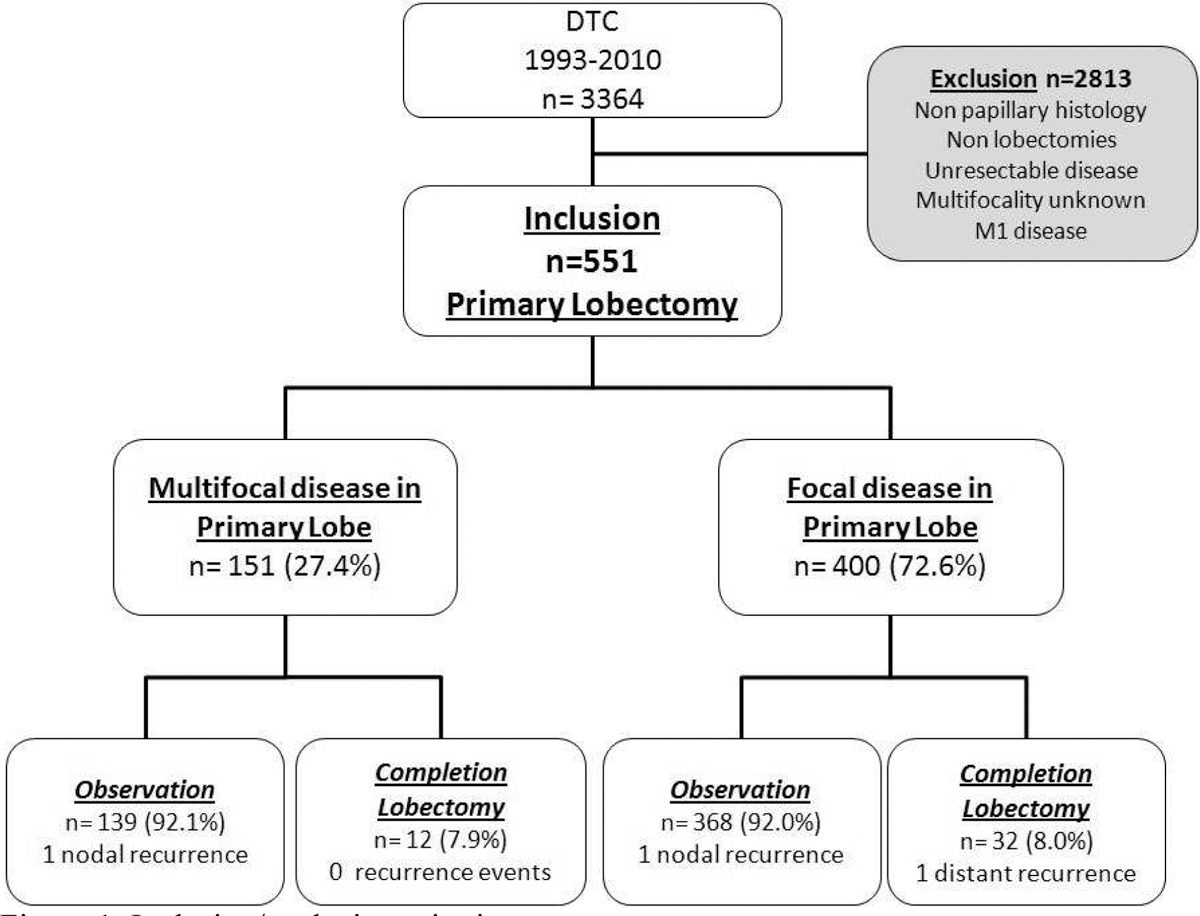
Inclusion/exclusion criteria
Patients with MFD managed with lobectomy alone have similar recurrence rates compared to patients with UFD. This data suggests that multifocality should not be considered as an indication for completion thyroidectomy.
Thyroid Cancer Friday Poster Clinical
Following total thyroidectomy (TT) for clinically low-risk papillary thyroid cancer (PTC), pathological assessment can occasionally report incidental perithyroidal lymph nodes (LNs) with occult metastases. These cN0pN1a patients often receive radioiodine (RAI) therapy for this indication alone. The aim of this study was to determine if a select group of N1a patients can be safely treated without RAI therapy.
An institutional database of 3664 previously untreated patients with differentiated thyroid cancer operated between 1986 and 2010 was reviewed. 232 pT1-3 patients managed with TT and no neck dissection were subsequently found to have incidental level 6 LNs on pathology. Patients with other indications for RAI such as extrathyroidal extension, close or positive margins were excluded leaving 104 patients for analysis. Patient demographics, pathological features and outcomes were recorded. Kaplan-Meier method was used to determine central neck LN recurrence free survival (RFS).
The median age of the cohort was 40 years (range 17–83). The median follow up was 45 months (range 1–190). The median number of positive LNs removed and maximal LN diameter was 1 (range 1–8) and 5 mm (range 1–16 mm) respectively. There were no statistically significant differences between the RAI (64.4%) and no RAI (35.6%) groups in terms of age (p=0.355), primary tumor size (p=0.234), multicentricity (p=0.659), presence of microscopic LN foci (≤0.2 cm) (p=0.072), LN extracapsular spread (p=0.373), and number of positive LNs (p=0.072). Male patients (p=0.049), those with vascular invasion (p=0.010) and LNs>5 mm (p=0.037) were more likely to be selected for adjuvant RAI therapy. Central neck recurrence occurred in 5 patients; 4 patients in the RAI group and 1 patient in the no RAI group. Patients with and without RAI therapy had similar 5 year central neck LN RFS of 94.6% and 96.2%, respectively (p=0.915). No patient, tumor, or treatment variables were predictive of neck RFS.
Select, low-risk PTC patients with incidental N1a and LNs smaller than 5 mm may be safely managed without adjuvant RAI.
Thyroid Cancer Friday Poster Clinical
Multifocality is commonly encountered in patients with papillary thyroid cancer (PTC). However its prognostic significance is unclear.
An institutional database of 3364 previously untreated patients with differentiated thyroid cancer operated between 1986 and 2010 was reviewed. Patients with non-papillary histology, less than total thyroidectomy, unresectable disease and those in whom multicentricity could not be determined were excluded s. 2505 patients were included for analysis; 1384 (55.2%) had multifocal disease (MFD) and 1121 (44.8%) had unifocal disease (UFD). Patient and tumor characteristics were compared for each group using the Pearson Chi square test. Recurrence free survival (RFS) was determined for MFD and FD patients using the Kaplan Meier method. Cox proportional hazards was used for multivariate analysis.
The median age of the cohort was 48 years (range 12–91). The median follow up time was 50 months (range 1–242). In MFD patients, the secondary tumor focus was most likely 1 cm or less (90.0%), with the majority involving both lobes (72.8%). Comparison of MFD and UFD patients showed that MFD patients were more likely to be female (p<0.001), display vascular invasion (p=0.001), histological positive margins (p<0.001), extrathyroidal extension (p<0.001), higher T stage (p<0.001), higher nodal stage (p<0.001), present with distant metastases (p=0.031), and were more likely to receive adjuvant RAI (p<0.001). MFD patients had slightly poorer 5 year RFS compared to UFD patients (93.4% vs. 94.8%, p=0.008). The unadjusted hazard ratio for multifocality was 1.655 (95%CI; 1.134–2.417, p=0.009). However, when adjusting for other variables predictive of recurrence (vascular invasion, T, N, and M status) and the use of adjuvant RAI, multifocality was not independently predictive of RFS (HR;1.218, 95% CI; 0.822–1.805, p=0.326).
In our series, multifocality was reported in greater than 50% of PTC patients. Multifocality is associated with aggressive histological features. However, multifocality does not appear to be independently associated with decreased RFS.
Thyroid Cancer Friday Poster Clinical
There is a lack of health related quality of life (HRQOL) research in thyroid cancer (TC) survivors. This study aims to assess the sociodemographic and clinical factors that most influence TC-specific QOL domains and estimate the impact of different health conditions on HRQOL in a large cohort of TC survivors.
TC survivors ≥17 years of age were recruited through the thyroid cancer survivor (ThyCa) website. Mean scores for the 7 domains and 6 items of THYCA-QoL, MCS and PCS of SF-12, and derived health utility index (HUI) were compared between factors. Regression analyses estimated the relationship between the sociodemographic, clinical, and THYCA-QoL measures and HRQOL (HUI).
All 1028 survivors reported their entire thyroid was removed. Most were female (90.3%), white (92.6%), <65 years (90.2%), insured (96.5%) and had papillary carcinoma (97.0%). Average survivorship time was 55.06 months (SD 63.2). Almost every sociodemographic and clinical factor significantly influenced ≥1 domain of THYCA-QoL. Age, education, employment, age at menopause, and co-morbidities affected 6-7/7 of the main domains, MCS and PCS (all p<0.05). Significantly lower THYCA-QoL scores (less complaints) were experienced in survivors >65 years, male, without co-morbidities, with higher education, were on T4 replacement, diagnosed with hypoparathyroidism, and were ≤1 year from diagnosis (all p<.05). Significantly higher scores (more complaints) were seen in survivors with a comorbidity, unemployed, and went into menopause at a younger age if female (all p<.05). Many of these differences were not identified in MCS and PCS scores. Average HUI was .69 (SD .14) and approximated a normal curve (skewness .13). Co-morbidities as well as increased neuromuscular, sympathetic, concentration, and throat/mouth complaints had the strongest association with worsening health status (adj R2>.2). The simplest, best regression model (adj R2=.48) included neuromuscular, concentration, and anxiety complaints predicting lower HRQOL.
TC-specific QOL is significantly influenced by many sociodemographic and clinical factors and is best measured by THYCA-QoL. Neuromuscular, concentration, and anxiety complaints had the greatest impact on HRQOL in TC survivors.
Thyroid Cancer Friday Poster Clinical
Current ATA guidelines recommend that thyroid ultrasound be performed preoperatively in patients with thyroid cancer. Previous studies demonstrate improved outcomes and fewer errors when guidelines are followed. Objectives: 1. Determine adherence rate of preoperative US for thyroid cancer. 2. Determine sensitivity of preoperative US in assessing extent of disease.
340 cases of thyroid cancer from 2009–2011 were reviewed at our academic medical center. 146 unique pathology reports were identified as at least stage T2 or node-positive. These cases were assessed for pathology findings (size, capsular invasion, extrathyroidal extension [ETE]) and US findings (size, echogenicity, calcifications, and ETE). Study Design: Retrospective chart review 63/146 thyroidectomies had an US completed or formally reviewed at our institution. Of the 83 that did not have an US at Emory, 59 had outside US reports referenced or uploaded. 24 (16%) had no US reported at thyroidectomy, thus adherence rate was 84% (increasing from 78% in 2009 to 88% in 2011). Calcifications were noted in 24/63 (sensitivity: 38%) of Emory US reports, and 39/63 (sensitivity: 62%) noted mixed/heterogenous or hypoechoic echogenicity; malignant features were reported in 83% of cases. 12/63 demonstrated ETE on pathology, and two of these were noted on ultrasound (NPV=84%). From 2009–2010, 15/39 (38%) of pathology reports did not reference capsular invasion-this decreased to 3/24 (13%) in 2011. Ultrasound-suspicious nodules correlated in size with T1 and T2 carcinomas by 46% and 12% overestimation, respectively, and T3+ carcinomas by 2% underestimation.
Our adherence rate to preoperative US is improving, as is the frequency of detection of malignant findings. Reporting of pathology became standardized with implementation of CAP synoptic reporting. We plan to develop a clinical pathway to standardize our preoperative imaging evaluation of our thyroid cancer patients to reduce error and variation in care.
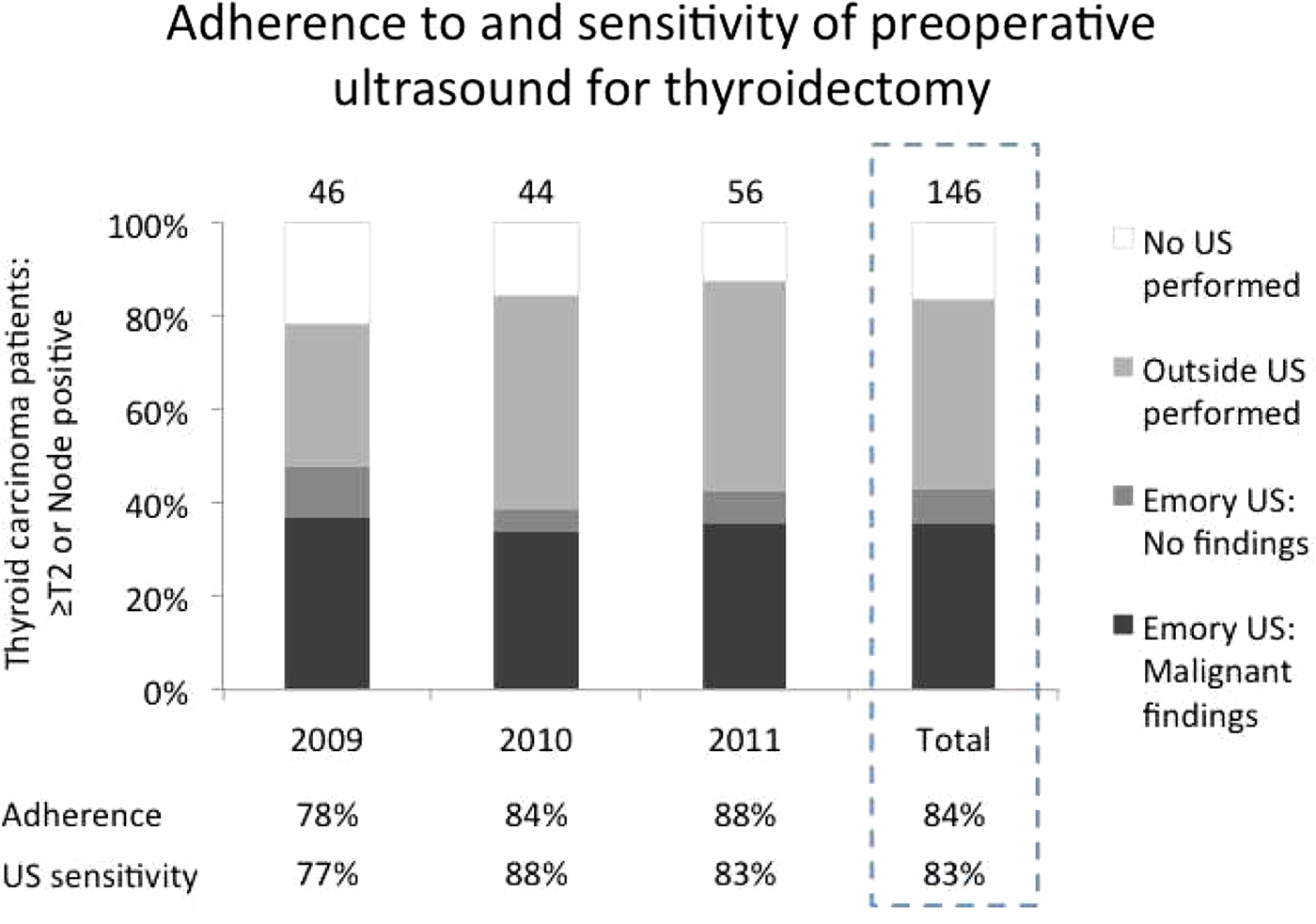
Thyroid Cancer Friday Poster Clinical
MTC related diarrhea can be debilitating, reduces QOL and occasionally is the only indication for initiating systemic therapy. Conventional anti-diarrheal drugs are not always helpful and may have side effects. CASAD, a natural calcium montmorrilonite clay, safely adsorbs toxins and inflammatory proteins associated with diarrhea. We hypothesized that CASAD will reduce the severity of diarrhea and improve QOL in MTC pts.
This is a prospective pilot trial (NCT01739634) of MTC pts not on systemic therapy with self-reported diarrhea of ≥3 bowel movements (BMs)/day for ≥1 wk. Study design included a 1 wk run-in period followed by 1 wk of CASAD +/− 2 wks optional continuation period. The primary endpoint was efficacy of 1 wk of CASAD treatment in decreasing the number of BMs/day by ≥20% when compared with baseline run-in period. Secondary objectives included tolerability and safety and the impact on QOL using MD Anderson Symptom Inventory-Thyroid questionnaire (MDASI-THY).
10 MTC pts (median age 52, 70% female, 80% white) were enrolled. All had distant metastases and median calcitonin was 5,088 ng/mL(1,817–42,007). 90% received prior anti-diarrheals, of whom 40% used ≥2 drugs, including tincture of opium (30%), imodium (50%), lomotil (20%), colestid (10%), cholestyramine (10%). 7/10 pts were evaluable (excluded: consent withdrawal(1), noncompliance(1), and concurrent C. difficile(1)). 6/7 pts discontinued their prior anti-diarrheals. 4/7 (56%) met the primary endpoint. Best response ranged from −7% to −99% (Fig. 1). 5/7 pts considered CASAD a success and they opted for 2 wk extension. Improvement in diarrhea symptom and all 6 interference items (QOL) assessed by MDASI-THY was noted at wks 1 and 3 (Fig. 2 and 3). Total interference score was significantly improved at 3 wks compare with baseline (p=0.05). Thyroid absorption test was performed in 1 patient; malabsorption of levothyroxine was not observed. Adverse events included flatulence (40%), bloating (10%), heartburn (10%), and constipation (10%).
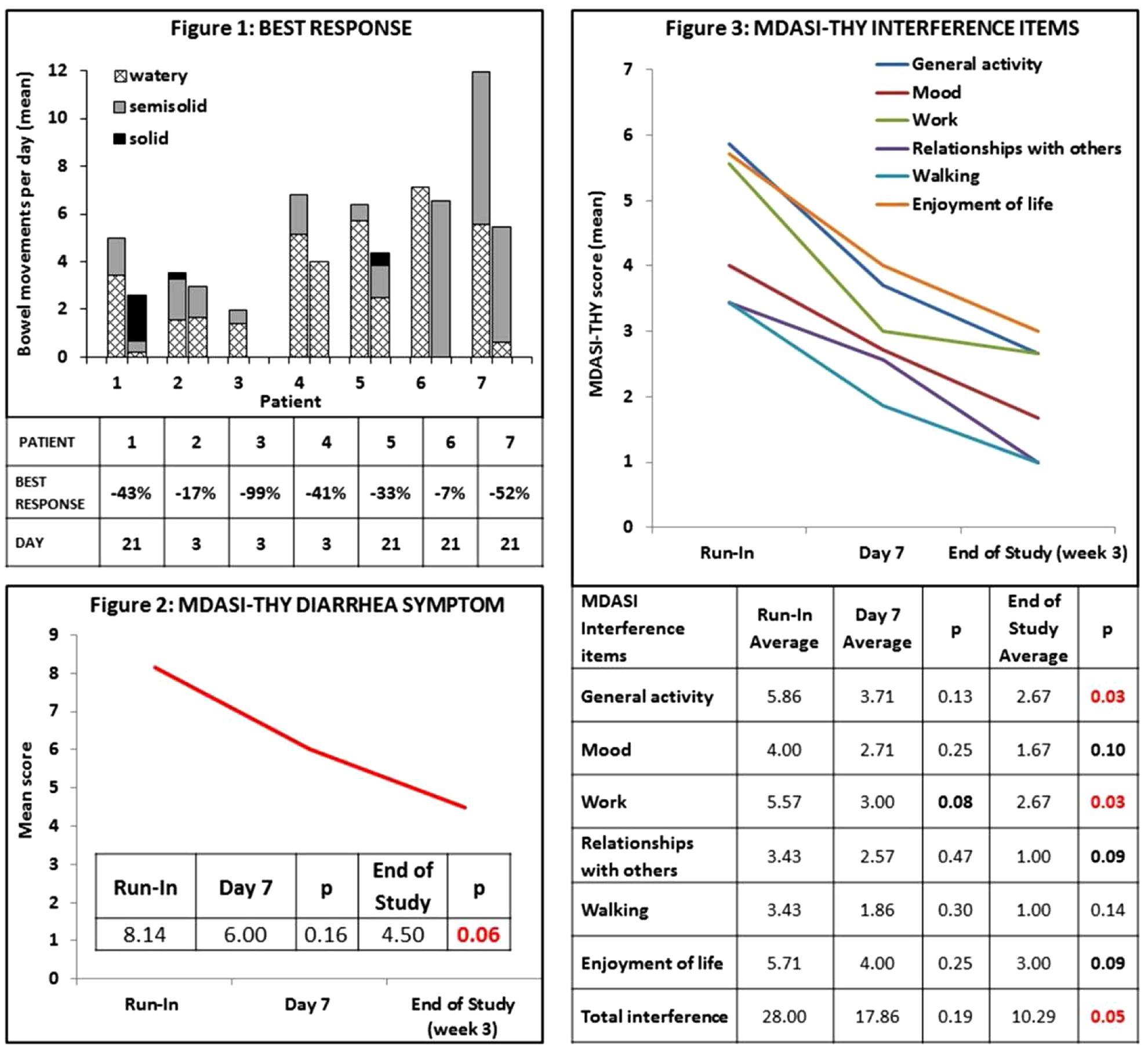
CASAD is a promising strategy for treatment of MTC related diarrhea. In this small pilot study, an improvement in frequency and quality of diarrhea, and QOL was noted. Further studies in this population are warranted.
Thyroid Cancer Friday Poster Clinical
Regional as well as national series show an increasing incidence of thyroid cancer due largely to papillary thyroid carcinoma of minor size. Prognostic scoring systems have been developed, but these do not take into account the rapidly changing case mix, and adjustments may be required. The purposes of this study were to evaluate treatment outcome and to analyze the value of older prognostic scoring systems tested on a relatively new, unselected national cohort of papillary thyroid carcinoma patients.
National prospective cohort study. Denmark; population 5.5 million.
1,350 patients were diagnosed with papillary thyroid carcinoma during 1996–2008, and the median follow-up time was 7.9 years. The ten-year recurrence free survival rate was 90.2%, and the ten-year crude and cause-specific survival rates were, 83.7% and 93.8%, respectively. By multivariate Cox regression, it was possible to confirm age, metastases (distant and nodal), extra thyroidal extension and tumor size as predictors of mortality, whereas only nodal metastases, extra thyroidal extension and tumor size were predictors of recurrence. In analyses of older prognostic scoring systems, a significant correlation between the risk group ranks was found for survival as well as recurrence. The c-index for cause-specific survival was highest for MACIS (0.92) and lowest for AMES (0.80). In the TNM, MACIS and EORTC systems, most patients were classified as stage 1, and for these patients, the 10-year cause-specific survival rate was approximately 99.5%, confirming the generally excellent survival.
This national study provides further evidence that a favorable prognosis is to be expected for patients diagnosed with papillary carcinoma. Also, it was possible to confirm age, metastases, extra thyroidal extension and tumor size as predictors of mortality, whereas only nodal metastases, extra thyroidal extension and tumor size were predictors of recurrence. All the scoring systems evaluated were able to produce a highly significant risk group stratification, showing that in spite of the changes in case mix of papillary carcinomas, these systems are still applicable, and in fact contain valuable prognostic information useable for treatment planning.
Thyroid Cancer Friday Poster Clinical
Fibroblast is an important component of the malignant tumor stroma. Most tumors incorporate an obvious biologically active, fibroblastic cell type known variously as carcinoma-associated fibroblasts (CAF). These cells have received increased attention because of their participation in tumor development, including invasion and lymph node metastasis and their ability to act as markers of patient prognosis in colorectal and thyroid epithelial neoplasm. Papillary thyroid carcinoma (PTC) is by far the most common thyroid malignancy with frequent cervical lymph node metastases up to 90% of cases. However, there were few studies that found the predictive marker for cervical lymph node metastases in PTC. The purposes of this study were to investigate the presence of CAF in PTC with or without lateral cervical lymph node metastases (LCLM) and to verify the correlation between CAF and LCLM through the immunohistochemical study.
Human progenitor cell antigen, CD34, and α-smooth muscle actin (SMA) were used for marker of CAF. The presence of CAF was investigated prospectively for verifying the correlations between the presence of CAF and LCLM in 65 PTC patients. Other clinicopathological charateristics including age and tumor size were compared to the result of immunohistochemical stain to CAF.
Among 39 specimens of PTC without LCLM, 7.7% showed immunoreactivity to CAF. In contrast, 92.3% of 26 specimen of PTC with LCLM showed CAF. The expression of CAF and tumor size revealed significant differences between PTC with LCLM and without LCLM (p<0.05).
This study revealed the presence of the CAF in PTC. Furthermore, PTC presenting CAF showed significantly more LCLM than that of PTC without CAF. Therefore, the CAF could be used as predictive marker for LCLM of PTC.
Thyroid Cancer Friday Poster Clinical
Current ATA guidelines recommend that ultrasound of the cervical lymph nodes be performed preoperatively in patients with thyroid cancer. Previous studies demonstrate improved outcomes and fewer errors when guidelines are followed. Objectives: 1. Determine adherence rate to preoperative US in patients with metastatic lymph nodes removed for thyroid cancer. 2. Determine sensitivity of preoperative US in assessing extent of nodal disease.
340 cases of thyroid cancer from 2009–2011 were reviewed at our academic medical center. 120 unique pathology reports were identified in which metastatic lymph nodes were removed. These cases were assessed for pathology findings (size, extranodal extension) and US findings (size, node shape, echogenicity, or hypervascularity). Study Design: Retrospective chart review 49/120 had an US completed or formally reviewed at our institution. Of the 71 that did not have an US at Emory, 47 had outside US reports referenced or uploaded. 24 (20%) had no US reported at time of surgery, thus overall adherence rate was 80% (increasing from 70% in 2009 to 83% in 2010 to 88% in 2011). Hypervascularity was noted in 26/49 (sens: 53%) of Emory US. Mixed/heterogenous or hypoechoic echogenicity was noted in 22/49 (sens: 45%), calcifications were noted in 13/49 (sens: 27%), and round shape in 7/49 (sens: 14%). Overall, malignant features were reported in 73% of cases. Extranodal extension was noted in 19/49 pathology reports, of which 95% had malignant features on US. Ultrasound-suspicious nodes overestimated the size of metastatic nodes on pathology by 6%.
Our adherence rate to preoperative US is improving, as is the frequency of detection of malignant findings. Reporting of pathology became standardized with implementation of CAP synoptic reporting. We plan to develop a clinical pathway to standardize our preoperative imaging evaluation of our thyroid cancer patients to reduce error and variation in care.

Thyroid Cancer Friday Poster Clinical
Right paraesophageal lymph node (RPELN), located posterior to the right recurrent laryngeal nerve, requires advanced surgical skill and expertise to dissect. Indication for RPELN dissection is unclear. The aim of this study was to identify the risk factors of RPELN metastasis in papillary thyroid carcinoma (PTC).
Two hundred and forty-six consecutive PTC patients (194 female, 52 male) who underwent total thyroidectomy (244 patients)or right lobectomy (2 patients) with central lymph node (CLN) dissection (13 ipsilateral and 233 bilateral) were observed between September 2010 and August 2013 at the General Surgery Department, Peking Union Medical College Hospital. Clinical and pathological data were collected and analyzed to identify the risk factors for RPELN metastasis.
RPELN metastasis was detected in 33 (13.4%) out of 246 patients. CLN metastasis occurred in 133 patients (54.1%). All 33 RPELN metastasis patients also had CLN metastasis (31 right-CLN and 2 left-CLN). Patients with right-CLN metastasis were more likely to have RPELN metastasis (34.4%, 31/90). Among the 54 patients with lateral lymph node metastasis, 18 patients (33.3%) had RPELN metastasis. In univariate analysis, gender, mean age, past medical history of thyroid and family history were not correlated with the possibility of RPELN metastasis. However, large tumor size, right lobe tumor, multifocality, right-CLN metastasis, Delphian lymph node metastasis, increased number of metastatic lymph node in central and lateral compartment were significantly associated with RPELN metastasis. In multivariate analysis, number of right central metastatic lymph nodes (1–2 metastatic lymph nodes: OR 13.58, 95%CI 2.73–67.52; ≧3 metastatic lymph nodes: OR 39.44, 95%CI 7.74–200.96), right side tumor (OR 6.35, 95%CI 1.13–36.61) and 3 or more lateral metastatic lymph nodes (OR 3.53, 95%CI 1.22–10.24) were significantly associated with high risk of RPELN metastasis.
RPELN dissection is suggested for all right side PTC patients, especially for patients with potential right CLN metastasis.
Clinical and pathologic features of patients with or without right paraesophageal lymph node metastasis.
a: In patients with multifocal tumors, the diameter of the largest one was defined as “diameter”. b: Right side tumor means 1 or more tumors in right lobe, none right side tumor means no tumor in right lobe. c: CLN didn't include RPELN. d: In patients without clinical lateral lymph node metastasis, No. of LLNs was defined as “zero”. Abbreviation: LN: Lymph node; Meta: Metastatic; CLN: Central lymph node, rCLN: Right central lymph node, LLN: Lateral lymph node.
Thyroid Cancer Friday Poster Clinical
Papillary Thyroid Microcarcinoma (PTMC) is increasingly recognized during thyroid surgery for both benign and malignant disease. The clinical significance of incidental PTMC is unknown. It is not clear if PTMC is a benign phenomenon or if it is associated with clinically significant cancer.
After obtaining IRB approval, we performed a retrospective analysis of 234 consecutive thyroidectomies from January 2009 to September 2011. The sectioning of all samples was standardized with 20 sections per specimen followed by 3 mm thick slicing of each section. Patients with known PTMC, history of previous head and neck radiation and familial syndromes were excluded. Univariant and multivariant analysis comparing patient age, gender, BMI, thyroid gland weight, size and foci of PTMC was performed in patients with benign disease and thyroid cancer.
The patient population consisted of 184 females and 50 males (F:78.6%, M:21.4%). On final pathology 74.8% of patients had benign disease and 25.2% had thyroid cancer. In patients with benign disease the rate of incidental PTMC was 38% versus 76% for patients with thyroid cancer (P<0.05). There was no statistically significant difference in mean age, gender, BMI, gland weight, size or number of foci of PTMC in benign versus thyroid cancer. There was also no correlation between gland weight, size or patient age with the number of foci of PTMC. The rate of incidental PTMC was significantly higher in patients with Multi Nodular Goiter (MNG) as compared to patients with thyroiditis (44% versus 21%, p<0.05).
The incidence of PTMC in MNG is similar to the background rate found in autopsy studies of normal thyroid glands. However, patients with clinical thyroid cancer are twice as likely to have PTMC where as inflammatory thyroid disorders have a protective effect. The lack of correlation of PTMC with age, gender, BMI, thyroid gland weight, size and number of foci of PTMC only further obscures its etiology and clinical significance and emphasizes the need for further evaluation.
Thyroid Cancer Friday Poster Clinical
Differentiated thyroid cancer (DTC) is amongst the most common malignancies in the adolescent and young adult (age 15–39) population and its incidence is rising. Younger age (<45) is an important prognostic indicator and is incorporated into the TNM classification system for DTC. We hypothesized that this would result in distinct treatment patterns for younger and older patients with DTC.
Using the California Cancer Registry, we identified 23,629 patients with DTC from 2004 to 2011 and divided them into younger (<45) and older (45+) cohorts. We tabulated demographic and clinical variables and compared them using Chi-square tests. Treatment variables included total or near total thyroidectomy (TT), other types of thyroid surgery, and the administration of radioiodine (RAI) as part of the initial treatment. We used multivariable logistic regression to identify independent clinical and demographic predictors of treatment administered.
Younger patients were more likely to be Hispanic (32.8% vs 21.5%), female (82.8% vs. 74.8%), have papillary carcinoma (92.9% vs 90.8%) and lymph node involvement (32.2% vs 19.6%; all p<0.0001). While the majority of patients underwent TT, it was slightly more common in the younger population (87.6% vs 85.1%, p<0.0001). RAI administration was also more frequent in those younger than 45 (54.6% vs 48.5%, p<0.0001). On multivariate analysis, younger patients (OR 1.193; 95% CI 1.099 – 1.294), higher T stage tumors, higher socioeconomic status (SES) and papillary carcinoma were predictors of undergoing TT versus other thyroid surgery. After adjustment, predictors of RAI administration included younger age (OR 1.116; 95% CI 1.053 – 1.183), prior TT, higher T stage, higher SES and lymph node positivity.
Younger patients with DTC in California are more likely to be female and Hispanic with papillary histology. After adjustment for disease and demographic characteristics, younger patients are more likely to undergo TT as their initial surgery and are more likely to receive RAI. Given their excellent prognosis and the potential for adverse sequelae from initial treatment for DTC, these findings warrant consideration when managing younger patients with DTC.
Thyroid Cancer Friday Poster Clinical
Preoperative distinction between benign and malignant follicular or Hürthle cell neoplasms based on cytologic examination of a fine-needle aspiration biopsy specimen is not possible. Preoperative measurement of serum thyroglobulin (Tg) is not recommended for initial evaluation of thyroid nodules, even though Tg concentrations are higher in follicular as well as Hürthle cell carcinomas than in benign follicular or Hürthle cell tumors. The aim of this study was to establish the cut-off value of the preoperative serum Tg concentration as a predictive factor of malignant disease in patients with a follicular or Hürthle cell neoplasm with diameter 2 cm or less.
Altogether, 244 patients (214 females, 30 males, age range 9–82 years, median age 52 years) had surgical procedure at out Institute from 1988 to 2013 because of follicular or Hürthle cell neoplasms with a tumor diameter 2 cm or less. In all patients a preoperative concentration of thyroglobulin was determined and Tg-autoantibodies were negative. The risk factors for malignancy were identified by the chi-square test and multivariate logistic regression.
The histopathological diagnoses were carcinoma, adenoma and benign goiter in 62 (25.5%), 115 (47%) and 67 (27.5%) patients, respectively. The median preoperative Tg concentration in benign tumors, papillary carcinomas, follicular carcinomas and Hürthle cell carcinomas was 41, 87, 72 and 106 ng/mL (p=0.05), respectively. The predictive factors for carcinoma shown by the chi-square test were: gender, thyroid volume and preoperative Tg concentration. The independent predictors of malignancy as shown by multivariate logistic regression were: male gender (OR 2.57 P=0.02), and Tg concentration of more than 80 ng/mL (OR 2.35, P=0.005).
The independent predictors of malignancy in follicular or Hürthle cell neoplasms are male gender and preoperative Tg concentration more than 80 ng/mL.
Thyroid Cancer Friday Poster Clinical
Pemetrexed is a second generation folate antimetabolite approved in the US for use in mesothelioma and in lung and ovarian cancers, believed to exert anti-tumor effects principally by inhibiting folate dependent enzymes including thymidylate synthetase. Preclinical studies have shown that pemetrexed inhibits in vitro growth of thyroid cancer cell lines; moreover, several patients with thyroid cancer have attained beneficial clinical responses in phase I pemetrexed clinical trials.
We now report a case series of pemetrexed use in thyroid cancer.
We first incidentally observed beneficial responses to pemetrexed and carboplatin therapy in two thyroid cancer patients treated with this regimen for coexisting more imminently threatening other cancers. One patient with recurrent metastatic lung adenocarcinoma coexistent with unresected primary Hürthle cell thyroid cancer experienced decreased thyroid primary FDG uptake after 6 cycles of treatment, with only benign cytology demonstrated upon later re-biopsy. A second patient with aggressive pelvic mesothelioma coexistent with poorly differentiated thyroid cancer (PDTC) associated with lung metastases attained durable RECIST partial response in parallel with marked decline in thyroglobulin (932 to 103 ng/ml) after only 2 cycles of pemetrexed and carboplatin therapy. Based on these encouraging outcomes, we subsequently treated two additional patients with metastatic rapidly progressive PDTC (who were deemed unsuitable for therapy using kinase inhibitors) with pemetrexed and carboplatin. A patient with rapidly progressive extensive lung and nodal metastatic disease received 7 cycles, attaining stable disease and alive more than one year after therapy initiation; a second patient attained a mixed RECIST response after 2 cycles, with decrease in size of lung nodules, stable disease in the liver and disease progression in the spleen.
Our experience suggests that pemetrexed-based therapy has clinical activity in follicular cell derived thyroid cancers and is perhaps of consideration in patients who are otherwise unsuitable for or who have progressed through kinase inhibitor therapy. We propose former clinical trials to further and more critically assess this approach.
RECIST partial response in metastatic poorly differentiated thyroid cancer with pemetrexed and carboplatin therapy
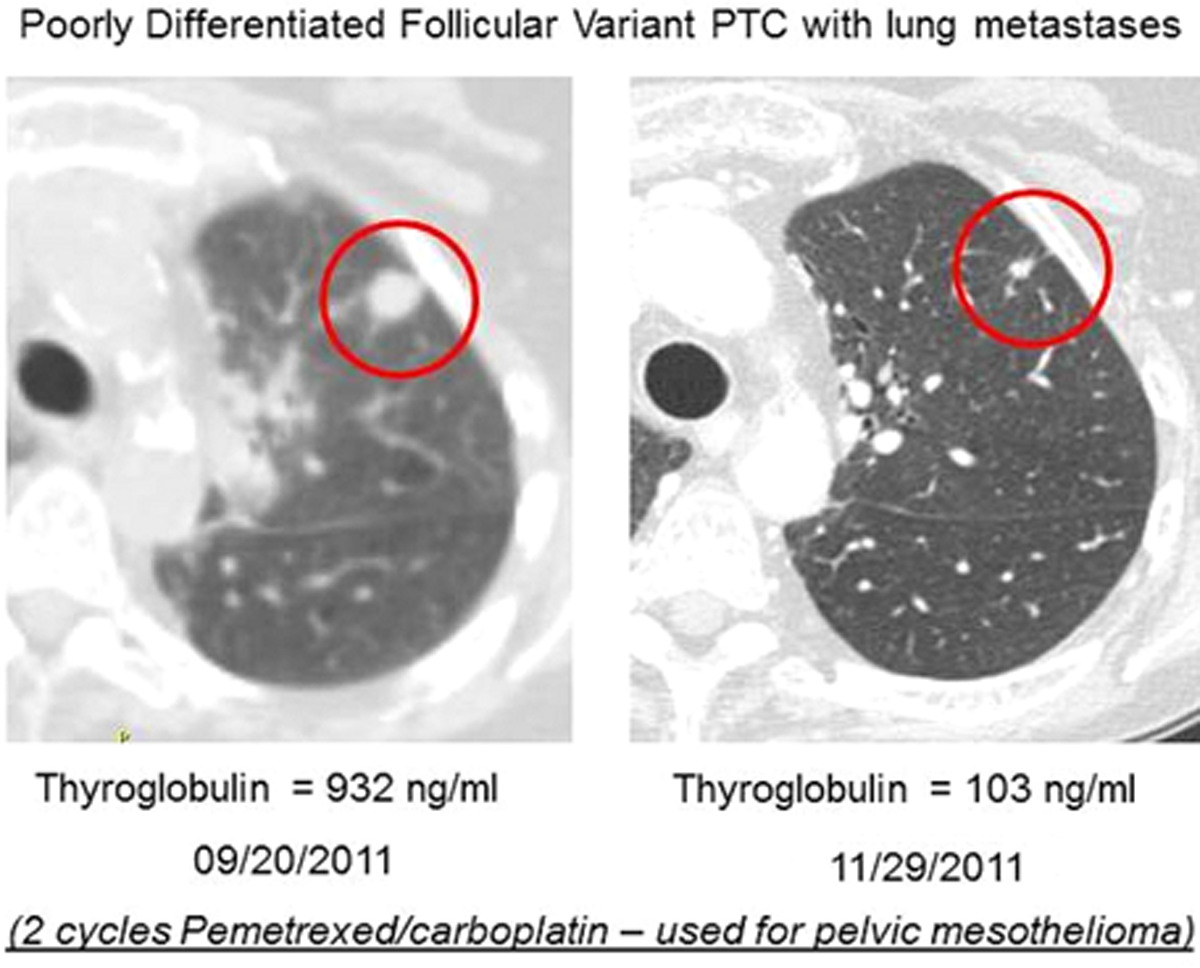
Thyroid Cancer Friday Poster Clinical
The universal endorsement in 1990 of the goal of virtual elimination of iodine deficiency (ID) by the year 2000 has still not been achieved in several signatory countries. Two billion people worldwide (over two million school age children), remain ID. In Europe there are still countries with no national population data on iodine nutrition, amongst which, Portugal. The current study aims at evaluating the iodine nutrition in the inland mountainous region of Beira Interior (BI), in Portugal.
Determination of urinary iodine concentration (UIC) from a general population sample of 192 volunteers from BI (2012/2013/2014), measurements of the iodine content of the largest water reservoir of the region of BI and evaluation of the thyroid histology pattern (6 year period). Urinary iodine excretion measurements: 91.7% of the general population was iodine deficient with a median UIC 63.50 μg/L. The mean iodine content of the main surface water reservoir for BI was 0.584 μg/mL. From 279 histology reports available the incidence of the different types of thyroid nodular pathology in BI was established. There were 60 histologic diagnoses of malignancy: 31 papillary carcinomas, 22 follicular cancers (18 follicular carcinoma and 4 Hürthle cell tumour), 3 medullary carcinomas, and 4 anaplastic carcinomas. The papillary to follicular carcinoma ratio was 31/22=1.41. The findings in what is, to our knowledge, the first general population study from the inland region of BI, in Portugal, demonstrate significant ID. Ample public information combined with educational programs as to the negative consequences of ID, availability of iodized salt at affordable prices and the promotion of seafood consumption would assist in solving the problem.

Thyroid Cancer Friday Poster Clinical
Sensitive (second-generation) Tg tests (Tg2GIMA) used to monitor DTC patients for persistent/recurrent(P/R) disease are prone to TgAb interference causing underestimation. Typically, laboratories limit Tg2GIMA to TgAb-neg. sera and TgAb+ sera are reflexed to a TgAb-resistant Tg method (radioimmunoassay(TgRIA) or mass spectrometry(TgLC-MS/MS). Previous Tg method correlations have not involved clinical samples. This study compared Tg2GIMA(Beckman), TgRIA(USC) and TgLC-MS/MS(Mayo) measurements for TgAb+ versus TgAb-neg. patients with P/R DTC.
Serum Tg was measured for 66 DTC patients prior (median 3, range 0–115 days) to P/R disease detection by biopsy or anatomic imaging. 34 patients were TgAb-neg. (using Kronus/RSR and Roche) and 32 patients were TgAb+.
TgAb-neg. sera displayed strong correlations between methods: Tg2GIMA versus TgRIA (r=0.98); TgIMA versus TgLC-MS/MS (r=0.98); and TgRIA versus TgLC-MS/MS (r=0.97). Between-method CVs were higher (median=20, range 5–86%) than within-method CVs (<10%). 4 patients had severe between-method discordances, (0.04/3.5/2.9; 16.6/39.4/25.4; 2.0/6.1/1.8 and 14.1/6.4/39.6 μg/L for Tg2GIMA/TgLC-MS/MS/TgRIA, resp.) suggesting methods recognized some tumor Tgs differently. One TgAb-neg. patient had no Tg detected by any method. TgAb+ sera had undetectable (<0.10 μg/L) Tg2GIMA in 13/32 (41%) and lower Tg2GIMA than either TgRIA or TgLC-MS/MS in 14/32 (44%). Both Tg2GIMA and TgLC-MS/MS were undetectable in 5/32 (16%) despite TgRIA of 1.0,2.5,2.6,2.7 and 10.5 μg/L, resp. The paradoxically undetectable/low Tg2GIMA values most likely reflected underestimation secondary to TgAb interference, whereas the cause of the undetectable TgLC-MS/MS in TgAb+ patients with disease could reflect TgLC-MS/MS insensitivity coupled with TgAb interference causing TgRIA overestimation, a polymorphic tumor Tg unable to generate the tryptic peptide for TgLC-MS/MS detection, or increased clearance of Tg-TgAb complexes.
There are differences between Tg2GIMA, TgRIA and TgLC-MS/MS measurements made for DTC patients with disease that result both from TgAb interference and different method specificities for detecting tumor-derived thyroglobulins, affirming the need for Tg method continuity.
Thyroid Cancer Friday Poster Clinical
Patients with metastatic differentiated thyroid cancer (DTC) often become refractory to radioactive iodine (RAI) (RAI refractory DTC; RRDTC) and have limited treatment options. The objective of this study was to investigate the treatment patterns of metastatic RRDTC patients.
Data were collected by performing a retrospective chart review study in the US and 5EU (France, Germany, Italy, Spain, UK) with physicians recruited from an online panel. Physicians provided demographics, disease history, and treatment information on 1 to 4 of their RRDTC patients in an online survey.
231 physicians participated. Of all RRDTC patients managed by these physicians, 24.4% had been in a watch and wait period in the past year. 700 patient charts were included in the chart review portion (44.1% from the US, 11–12% from each 5EU country). 45.0% of patients were male with a mean age at diagnosis of 55.1 years (SD=12.4). Patients had been diagnosed with DTC for a mean of 10.6 months (SD=22.5) prior to RAI initiation; patients were considered RAI refractory a mean of 24.2 months (SD=36.8) after initial DTC diagnosis. 52.0% of patients were on systemic therapy (from 34.6% in Germany to 58.3% in the US, p<.05); patients initiated systemic therapy 3.5 months (SD=4.5) after diagnosis. Of patients on systemic therapy, 74.2% were on 1st line, 19.5% were on 2nd line, and the remaining 6.3% were on 3rd/4th line. TKIs were the overall most common 1st line treatment (59.9%), though significantly more common in the US (78.3%) compared with 5EU (from 21.4% in Italy to 59.0% in Spain; p<.05). Chemotherapy was the next most common 1st line treatment option overall (37.4%), though significantly less common in the US (19.4%) compared with 5EU (from 38.5% in Spain to 69.0% in Italy; p<.05). TKIs and chemotherapy had similar usage as 2nd line treatment options.
Among patients diagnosed with RRDTC, watch and wait is a common management strategy. Both TKIs and chemotherapy were the most common treatment options in 1st and 2nd line, though patients in the US were more likely to be treated with TKIs while patients in the 5EU were more likely to be treated with cytotoxic chemotherapy.
Thyroid Cancer Friday Poster Clinical
It has been stated that thyroid carcinoma is an increasingly serious issue in many parts of the world. The aim of our study was to determine a possible relationship between Forkhead box E1 (FOXE1) gene variants and histopatholocigal features of papillary thyroid carcinoma.
We investigated the FOXE1 rs894673, rs1867277 and rs3758249 variations in 57 Papillary thyroid carcinoma patients and 51 age matched healthy control subjects. This study was performed with the polymerase chain reaction based restriction fragment length polymorphism (RF LP) techniques.
According to study results, there was a significant difference in the distribution of FOXE1 rs894673 genotypes in Papillary thyroid carcinoma cases (p=0.01). The presence of FOXE1 rs1867277 AA genotype was more significantly associated with several histopathological parameters such as focal and diffuse capsular invasion, lymphatic invasion, P3 with P4 tumor grade and surgical margins. The presence of the AA genotype of FOXE1 rs1867277 variation was more significantly associated with the classic variant in papillary thyroid carcinoma cases. Furthermore, the presence of the A allel was found to be related with lymph node invasion risk by 2.46 fold, capsular invasion risk by 2.97 fold, and pT3 with pT4 pathological stage risk by 4.13 fold and the presence of FOXE1 rs1867277 A allele was more significantly associated with classic variants. The presence of FOXE1 rs1867277 A allel was more significantly associated with several histopathological parameters in classic variant in papillary thyroid carcinoma cases such as, the presence of the A allel was found relationship with lymph node invasion risk by 2.0 fold, capsular invasion risk by 2.39 fold, and pT3 with pT4 pathological stage risk by 3.57 fold. In addition, AATT, AAAA and GATT haplotypes (rs1867277 and rs894673) were evaluated for association with papillary thyroid carcinoma cases. Our study results showed a significant difference according to two-allele haplotype distribution between papillary thyroid carcinoma cases and control groups.
Our findings suggest that FOXE1 variations generate a higher risk for poor histopatological features of papillary thyroid carcinoma.

Thyroid Cancer Friday Poster Clinical
The majority of thyroid fine-needle aspirations (FNA) are definitively diagnosed on cytologic evaluation; however, a significant proportion of cases show atypical cells of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS) and thus represent an atypical category difficult to clinically treat. The extent to which molecular profiling (MP) can aid clinical decision making in the category of AUS/FLUS thyroid FNA is explored.
The Metropolitan FNA clinic database was searched between April 2011 and May 2013 for AUS/FLUS thyroid aspirations with accompanying MP and as available, a second opinion consultant report and/or relevant follow up. Aspirations were performed by a single aspirator with 20-plus years of dedicated FNA experience. Molecular profiling was accomplished by the miRInform™ test (Asuragen, inc., Austin, TX) that analyzes 17 DNA mutations and RNA fusion transcripts that mark for thyroid neoplasia. A total of 34 AUS/FLUS FNA cases with MP were identified, all with adequate cellularity, with a subset of 15 cases with surgical follow-up and an additional 3 cases with repeat, follow up aspirations. Eleven of the 34 cases had consultant reports.
Of the 15 AUS/FLUS cases with histologic follow up, 11 (73.3%) were malignant. Molecular profiling identified a mutation or translocation in 6 of these 11 (54.5%) malignant cases; the remaining 5 malignant cases (45.5%) had a negative MP result. Molecular profiling had a positive result in 7 of 34 (20.6%) total AUS/FLUS cases. Six of the 7 (85.7%) positive MP results correlated with malignancy on follow up. A single case of AUS/FLUS with a RAS mutation was adenomatoid nodule (AN) on histology. Of 12 cases sent for a second opinion there was an interobserver agreement of AUS/FLUS in 7 cases (54.5%). Table 1 summarizes the results.
Table 1: Correlation of AUS/FLUS aspirates with second opinion consultant diagnosis, molecular profile result and relevant follow up, as available. Cases without follow-up are not listed.
PTC-Papillary thyroid carcinoma, AUS/FLUS- Atypical cells of undetermined significance/follicular lesion of undetermined significance, AN-Adenomatoid nodule
Although AUS/FLUS is a challenging diagnostic category and has a high inter-observer variability, in our experience a cytologic diagnosis of AUS/FLUS is concordant with malignancy in the majority of cases (73.3%). Molecular profiling was less sensitive in detecting malignancy (54.5%), but is highly specific.
Thyroid Cancer Friday Poster Clinical
Increasingly, Afirma gene expression classifier analysis is being used to guide decision making in FNA samples with indeterminate cytology. While validated as a diagnostic tool, the clinical application of Afirma is still being explored given a high negative predictive value (96%) but a low positive predictive value (40–44%), often leading to surgical intervention for GEC suspicious lesions that are ultimately benign. Given the low PPV of GEC suspicious nodules, we hypothesized that analyzing TSH, TPO, and lymphocytic thyroiditis status could reveal factors that would allow us to better predict the likelihood of malignant pathology for GEC suspicious thyroid lesions.
We retrospectively examined the pre-operative TSH, TPO and evidence of lymphocytic thyroiditis on histopathology in patients with suspicious Afirma who underwent NTT at the University of Colorado Hospital between 10/2010 and 11/2013. Data was obtained for 69 patients.
Results were analyzed primarily for TSH relationship; there was a non-significant association between malignancy and TSH with mean TSH being 0.399 mU/L higher in malignancy (benign - 1.67, malignant - 2.00; p=.204). The odds of a patient with malignant pathology having lymphocytic thyroiditis were 1.973 times the odds of a non-cancer patient (p=0.213). TPO status was only available for 24 patients and there was no significant difference between TPO antibody positivity in benign vs malignant lesions.
Our study was limited by a small sample size, especially with TPO antibody assessment as the majority of patients had a normal TSH and did not clinically warrant thyroid antibody evaluation. Given the trends seen with higher TSH and presence of lymphocytic thyroiditis being associated with malignancy in GEC suspicious thyroid nodules, a larger, prospective analysis of TSH and TPO antibody status may yield significant findings. These factors may aid in clinical decision making for patients when considering a hemi-thyroidectomy versus total thyroidectomy as a surgical intervention for GEC suspicious thyroid nodules.
Thyroid Cancer Friday Poster Clinical
The purpose of this study was to demonstrate the predictive value of tumor volume measured by ultrasonography for occult central neck metastasis (OCNM) of clinically N0 PTC.
From March 2009 to May 2013, a total of 264 patients with PTC who underwent total thyroidectomy with at least ipsilateral prophylactic central neck dissection (CND) were enrolled in this study. All patients were clinically N0 by preoperative ultrasonography and CT. We retrospectively evaluated the demographics, preoperative ultrasonographic features (tumor size, volume, and multiplicity) and pathologic results.
The OCNM rate was 35.6%. Tumor volume measurement facilitated prediction of occult metastasis (p=0.035). At 0.385 mm3, the sensitivity and specificity were 51.1% and 66.5%, and the area under the curve was 0.610. In multivariate analysis, the tumor volume was an independent predictive factor for OCNM (odds ratio (OR)=1.83, p=0.029). The other predictive factors were extrathyroidal extension (OR=2.39, p=0.004) and male gender (OR=3.90, p<0.001).
The PTC tumor volume measured by ultrasonography could be a preoperative factor predictive of occult central neck metastasis.
Ultrasonographic volume measurement.
Tumor volume=A×B×C×0.524 (A: width, B: length, C: height).
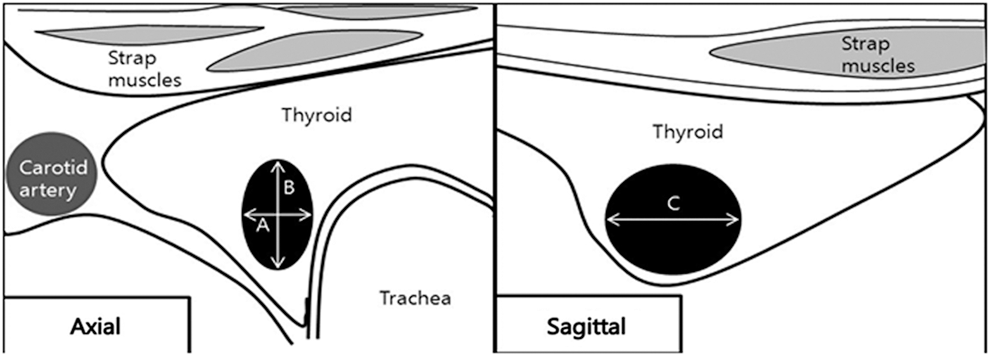
Thyroid Cancer Friday Poster Clinical
Papillary thyroid cancer (PTC) invading surrounding organs presents relatively worse prognosis than confined or minimally invasive tumor. PTC involving the recurrent laryngeal nerve (RLN), trachea, larynx, or esophagus is regarded as T4a which is resectable at length. The treatment outcome and complications after surgical resection of T4a lesion may differ. This study was designed to analyze the treatment outcome of T4a-staged PTC according to the involved sites.
Clinical data of 54 patients who were treated between 2006 and 2010 for T4a-staged PTC were reviewed. Age, gender, lymph node metastasis, and involving sites were used as clinical factors. Survival analysis was performed by the life table method; comparison among/between groups was performed using the log-rank test and multivariate analysis was carried out using the Cox proportional hazard model.
Multiple organs (n=26, 48.2%) were involved more frequently than isolated RLN (n=14, 25.9%) or isolated tracheal invasion (n=14, 25.9%). Multiple organs invasion showed increased risk of lymph node metastasis (odds ratio=4.44, p=0.031) compared to isolated tracheal invasion. In addition, multiple involvements of tumor showed significant impact on disease-free survival and overall survival (p=0.029 and p=0.029, respectively). Independent predictors of disease progression or recurrence was the presence of tracheal and/or esophageal invasion (odds ratio=5.14, p=0.011). Distant metastasis at diagnosis was statically associated with multiple organ invasion (odds ratio=8.10, p=0.04).
The presence of tracheal and/or esophageal invasion is related to lymph node metastasis, which is associated with disease progression and worse survival rate. Elective lateral lymph node dissection should be considered for the treatment of these patients. Tumor involving only the RLN showed better prognosis if it is adequately resected compared to tumor involving multiple organs.
Thyroid Cancer Friday Poster Clinical
Thyroid tumors represents only 1 to 1.5% of all malignant tumors in humans; however they are the most common malignant tumors of the endocrine organs. Histologically they are divided into differentiated (DTC), medullary thyroid carcinoma (MTC), anaplastic thyroid carcinoma (ATC) and less frequently lymphomas or metastases of other malignant tumors. The annual incidence of thyroid cancer varies considerably by geographic area, age and sex. Objective: We aimed to evaluate the incidence of thyroid cancer during 2013 in Tucumán province, a territory with a population of 1448200 inhabitants (women=737565, men 710635) from Argentina.
Subjects and Methods: we reviewed all the pathological examinations from thyroidectomies performed in the whole province from January 2013 to December 2013 in eight private and four public centers. We included those cases with a diagnosis of thyroid cancer from patients living in this province and we excluded those cases that were referred from other provinces to Tucumán for the surgical procedure.
In 2013, 116 new cases of thyroid cancer were diagnosed, 13 males and 103 females. The calculated incidence was 8.01/100000 inhabitants (men: 1.8/100000 and women 13.9/100000). Mean age at diagnosis was 45 years (range 15–86 y). The incidence for differentiated thyroid cancer (DTC; n=112) was 7.7/100000; medullary thyroid cancer 0.14/100000 and others (anaplastic and lymphoma) 0.14/100000. Mean size of DTC was 17.7 mm, 37% were microcarcinomas.
The incidence of thyroid cancer seems to be higher in Tucumán province than previously reported in other áreas from Argentina.
Thyroid Cancer Friday Poster Translational
MicroRNAs (miRNAs) are small non-coding RNA molecules which negatively regulate gene expression. Their levels are altered in tumors compared to normal tissues, therefore miRNAs are likely to be highly useful as biomarkers for cancer diagnosis. The aim of this study was to evaluate the expression profile of miRNAs in the serum of a cohort of Caucasian patients with thyroid nodules.
We used a stepwise approach. In step 1 we assessed the miRNA profile, by TaqMan® Array Human MicroRNA A Cards v2.0, in pooled sera from 12 healthy subjects (HS), 12 nodular goiter (NG) and 12 papillary thyroid cancer (PTC) patients (first cohort). We found 8 miRNAs with different expression levels in PTC patients, which were validated in step 2, by qRT-PCR, in each sample of the first cohort of patients. Four out of these 8 miRNAs were confirmed to have a different expression in PTC. In step 3 these 4 miRNAs were analyzed, by qRT-PCR, in a second cohort of subjects including 79 PTC, 80 NG and 41 HS.
In step 1 we found 8 miRNAs differentially expressed in PTC compared to NG and HS. In detail, miRNA579, −95, −29b, −501-3p and miRNA-548d-5p were down-regulated while miR190, −362-3p, −518a-5p were up-regulated. In step 2, only 4 miRNAs (miRNA579, miRNA95, miRNA29b and miRNA190) were validated and when evaluated in a second cohort of sera (step 3), miRNA95 combined with miRNA190, in a multivariate risk model, showed a sensitivity of 98.7% for PTC diagnosis.
The combination of serum miRNA190 and miRNA95 levels is a powerful and non invasive tool for the differential diagnosis of thyroid nodules.
Thyroid Cancer Friday Poster Translational
Metformin is a widely used antidiabetic agent, which regulates glucose metabolism. Recent studies suggest that metformin may reduce the risk of cancer, including papillary thyroid cancer (PTC), but its mode of action in cancer remains not elucidated. Our previous study revealed that overexpression of pyruvate kinase M2 (PKM2), a key enzyme involved in the glycolysis pathway, provide a selective growth advantage for PTC cells through activation of glycolysis, which accounts for the major source of energy production. Aims of this study are to investigate whether metformin inhibits the proliferation of PTC in vitro and in vivo, and to determine whether metformin causes alterations of both PKM2 levels and energy metabolism in PTC cells.
After treating with metformin, the viability of PTC cell lines (BCPAP, K1 and TPC-1) was analyzed by 3-(4, 5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide (MTT) at various concentrations; cell cycle analysis was performed by flow cytometry; real-time polymerase chain reaction and Western Blotting were performed to determine the expression of PKM2; energy utilization in living cells was measured by Seahorse XF instruments, simultaneously quantifying mitochondrial respiration and glycolysis in real time. Moreover, xenograft tumors were challenged in nude mice to establish the murine model; tumor growth was monitored after metformin administration orally.
MTT assays showed that the proliferation of PTC cell lines was inhibited in a concentration- and time-dependent manner after treating with metformin; moreover, metformin induced apoptosis of the PTC cell lines. The expression of PKM2 in PTC cells was decreased by metformin. Furthermore, metformin changed the pattern of cell energy metabolism, manifested with a significant decrease in basal respiration, basal glycolysis, ATP production and glycolytic capacity of PTC cells. Metformin inhibited tumor growth in mouse xenograft models.
Metformin provides an antitumoral effect in PTC cells. This effect may be mediated through a decrease of PKM2 expression and an alteration of cell energy metabolism, which leading to an energy crisis in cancer cells.
Thyroid Cancer Friday Poster Translational
Cystic papillary thyroid cancer (cPTC) is a type of well-differentiated PTC exhibiting classical histopathological features, but different morphological properties due to its common presentation as mural nodule in thyroid cystic mass. The diagnosis of cPTC is challenged because the fine needle aspiration biopsy (FNAB) usually reveals cystic fluid with insufficient amount of representative follicular cells resulting in low-informative cytological reports. The aim of this study was to identify potential diagnostic markers for discrimination of cPTC from benign cystic thyroid neoplasms.
We identified patients who were surgically treated for cystic thyroid neoplasms. The cystic fluid from these cases was collected from post-operative specimens. Seven cPTC and seven cystic benign controls were selected for proteomics profiling by liquid chromatography tandem mass spectrometry (LC MS/MS). The depletion was performed to remove high-abundant proteins followed by labeling by iTRAQ. To validate LC MS/MS data, we performed immunohistochemistry (IHC) and western blot (WB) using tissue and fluid from depleted samples, respectively; ELISA was applied on non-depleted 17 cPTC and 55 benign fluid samples and receiver operating characteristics (ROC) curve was used to determine optimal cut-off value.
Out of all 1,581 identified proteins, 841 contained labels in both iTRAQ pools and 41 proteins were differently expressed in cPTC (p<0.05). Of these, cytokeratin 19 (CK-19) showed significant up-regulation in cPTC as compared to benign controls (p=0.002). This finding was validated by IHC and WB showing overexpression of CK-19 in cPTC. By ELISA (CYFRA 21-1 assay) we detected higher concentrations of CK-19 in cyst fluids from cPTCs (59 ng/ml) as compared to benign controls (36 ng/ml), p<0.001. ROC curve analysis revealed 55 ng/ml or more as optimal cut-off value. Area under the ROC curve was 0.86 (p<0.0001).
To our knowledge this is the first extensive catalogue of the protein content in fluid from the thyroid cystic neoplasms. Based on the LC-MS/MS, IHC, WB and ELISA data we hypothesize that CK-19 could be determined in fluid of thyroid cyst lesions by ELISA and potentially used as diagnostic marker of cPTC complementary to FNAB.
Thyroid Cancer Friday Poster Translational
Heme oxygenase-1 (HO-1) is a stress-inducible intracellular enzyme. In response to various stress factors and proinflammatory cytokines, expression of HO-1 increases to maintain cellular homeostasis. Recent studies indicate that HO-1 expression is upregulated in cancer cells and may promote tumor development and progression. A previous study demonstrated that HO-1 reduced the sensitivity of papillary thyroid cancer cells to apoptotic stimuli. However, the expression pattern of HO-1 in thyroid cancer tissues has not been investigated.
In this study, we analyzed HO-1 expression by Western blot in paired papillary thyroid cancer tissues. Papillary thyroid cancer consistently showed an increased HO-1 expression. Immunohistochemical analysis of a tissue microarray revealed positive HO-1 expression in 55/115 (48%) papillary, 5/14 (36%) follicular, 2/7 (29%) poorly differentiated, and 1/2 (50%) anaplastic thyroid cancers. In addition, BRAF V600E expression was evaluated by immunohistochemical VE1 staining. In 18 papillary cancers, Sanger sequencing of genomic DNA was performed to detect BRAF c.1799T>A mutation. The results of sequencing were consistent with immunohistochemical VE1 staining.
In differentiated thyroid cancer, HO-1 expression correlated positively with patient age (P=0.001), TNM stage (P=0.001), and MACIS score (P=0.001). There was a trend towards a more frequent extrathyroidal invasion (P=0.061) and a higher ATA risk of recurrence (P=0.054) in patients with HO-1-positive tumors. BRAF V600E expression was associated with patient age, extrathyroidal invasion, TNM stage, MACIS score, and ATA risk of recurrence. There was a strong association between HO-1 and BRAF V600E expression (P=0.002).
In conclusion, we found that HO-1 expression is upregulated in thyroid cancer, and HO-1 expression correlates with tumor aggressiveness and BRAF V600E expression. Our findings may provide a novel prognostic biomarker and a potential therapeutic target in the management of thyroid cancer.
Thyroid Cancer Friday Poster Translational
Papillary thyroid cancer (PTC) is the most common type of differentiated thyroid cancer. MicroRNA 146b (miR-146b) has been suggested as a potentially useful diagnostic marker of malignancy and has been associated with aggressive clinicopathologic features of PTC. In this systematic review, we provide an overview of the expression of miR-146b and the possible association with lymph-node metastases (LNM), an important clinicopathologic feature of aggressive PTC.
A literature search was performed within the PubMed, Embase, Cochrane, Web of Science and Scopus databases selecting papers published prior to April 4, 2014. We searched by combining the concepts “thyroid tumor” with “micro-RNA” by using “and” as the Boolean operator. From a total of 830 unique studies identified by our search terms, 48 met our inclusion criteria and 20 examined miR-146b, among which a total of 7 studies examined relationships between miR-146b and cervical LNM.
Seven studies from 6 unique authors including 447 patients, among whom 217 demonstrated LNM, were reviewed. All seven studies reported positive association between the expression of miR-146b and LNM. Substantial methodological, statistical and reporting differences make interpretation across studies unreliable.
Our systematic review of currently available studies suggests that there may be a meaningful relationship between expression levels of miR-146b and the occurrence of LNM in patients with PTC. These findings may be biased because none of the studies reported that patients had undergone routine central lymph node dissection. Our findings emphasize the need for well-designed prospective studies involving routine central lymph node dissection prior to considering miR-146b expression as a factor in clinical decision-making.
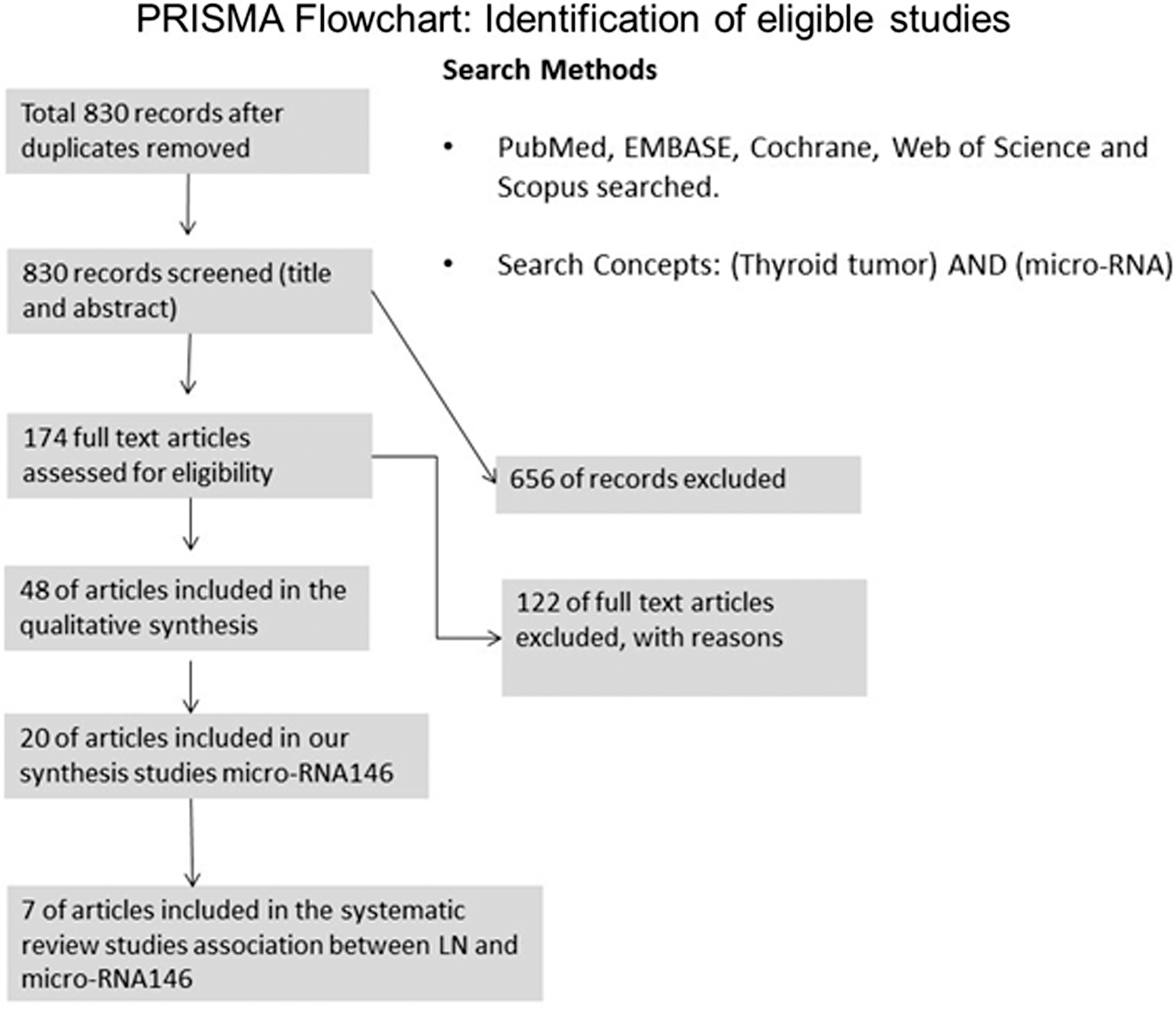
Thyroid Hormone Action Friday Poster Basic
Thyroid hormones (THs) act mainly through their nuclear receptors (TRs). T3 is considered the primary bioactive TH because of its high affinity for TRs. However, results from our group in teleosts have shown that 3,5-T2 (T2) can also regulate gene expression as well as promote the recruitment of a different transcription factor population to the TR bound to TH-response elements. In these vertebrates, the effects of T2 are mediated by a long (L-) TRβ1 isoform that contains a 9 amino acid insert in its ligand-binding domain. In contrast, the short (S-) TRβ1 lacks this insert and is only activated by T3. In concert, T3 and T2 differentially regulate the expression of S- and L-TRβ1, respectively in vivo. Furthermore, liver expression of L-TRβ1 is 10^6-fold higher than that of S-TRβ1, reflecting the functional relevance of this signaling pathway. These studies however have only been performed in tilapia liver and no information regarding any other tissue is available. On this regard, it is well known that THs mediate cellular proliferation and neural differentiation in the nervous system of vertebrates.
With the aim of starting to explore the functional role of the two TRβ1 isoforms in tilapia brain, we treated tilapia juveniles with 25 nM of T2 or T3 for 24 h in the culture water and measured the absolute levels of expression of S- and L-TRβ1, as well as those of two T3-responsive genes: GH and IGF-1 in four different areas of the brain: telencephalon; thalamus/hypophysis; optical lobe and cerebellum.
All these brain regions expressed the four genes predominantly in thalamus/hypophysis and cerebellum in control fish. IGF-1 expression slightly varied between regions, being more abundant in cerebellum. The expression levels of GH and S-TRβ1 were more abundant in thalamus/hypophysis, while those of L-TRβ1 were prominently abundant in the four regions, suggesting their important role in teleost brain physiology.
In treated animals, the patterns of expression of the four analyzed genes were different between treatments (T2 or T3) and brain regions, suggesting a different role for T2 and T3, depending on the specific areas of the brain.
Thyroid Hormone Action Friday Poster Basic
Thyroid hormones (THs) are involved in important body functions. Iron is a very important element to all cells playing roles such as oxygen transportation. Its homeostasis is performed by specialized proteins (ferritin, transferrin, ferroportin, hepcidin). Some studies show that THs can regulate iron homeostasis mRNA and protein expression, such as ferritin and transferrin. This study aimed to evaluate the action of THs in mRNA expression of those proteins.
The animals were made hypothyroid (Tx) and subclinical hypothyroid (HS) surgically. Surgical sham animals were used as control. Part of Tx animals were treated during 5 d with triiodotironine, 5 and 10 times physiologic dose, part of HS animals were treated with tiroxine. Rats were killed by decapitation and duodenum and liver were excised and total mRNA was extracted with Trizol and evaluated by Real Time PCR.
In HS animals liver high ferritin was increased (P<0.0001) compared to control, TX, 5XT3, 10XT3; ferroportin was increased in TX (P=0.0207) compared to control; hepcidin was increased (P<0.0001) in TX animal compared to control, 5XT3 and 10XT3, in HS was decreased (P<0.05) compared to TX, control, 5XT3, 10XT3, HS+T4 was decreased (P<0.0001) compared to TX. Transferrin receptor in TX was increased (P=0.0389) compared to 10XT3, and transferrin was increased (P=0.0188) in TX compared to 5XT3. In duodenum HT have not changed mRNA expression.
We have shown that HT can play a role in mRNA expression of proteins involved with iron homeostasis and they act in a tissue specific way.
Expression of proteins related with iron homeostasis after treatment with TH or without TH.
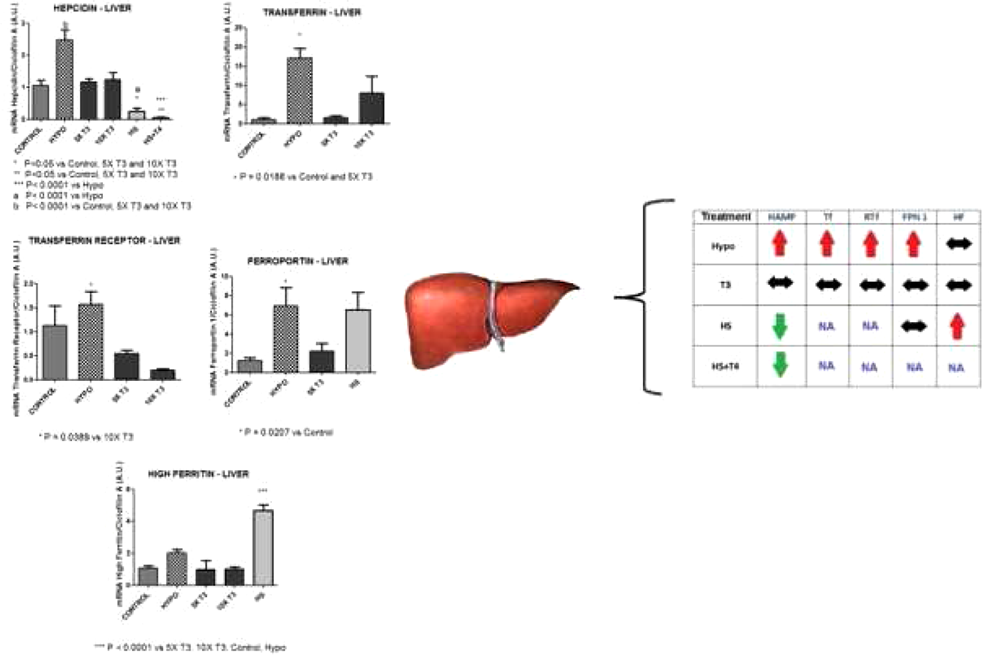
Thyroid Hormone Metabolism & Regulation Friday Poster Basic
TH is important to ensure central nervous system development. Non-treated hypothyroidism causes thermoregulatory system defects and irreversible mental retardation. The concept that exists a critical period for TH action on the brain during development was the reason to us to evaluate several genes that regulate TH action during neuron differentiation, using from human iPSC until neurons differentiation.
Stem cells generated from fibroblast of normal patient (WT83) and from Rett syndrome patient (Q83X) were differentiated into neurons at their respective culture media. Total RNA were extract with Trizol from iPSC, embryoid bodies (EB), neural progenitor cells (NPC) and neurons (N) and were evaluated by Real Time PCR using the respective primers for TH transporters (MCT8 and LAT2), deiodinases (Dio 1, 2 and 3), and thyroid receptors (TRα1 and TRβ 1 and 2), and IGF-1 (TH regulated gene).
In both kind of cells (WT83 and Q83X), the Dio1, Dio 2 and Dio 3 expressions in iPSCs were very low. Gene expression of all deiodinases was found on N, but Dio 3 gene expression were diminished on Q83X cells when compared with the control (WT83). TH transporters were found in all differentiations phases with higher expression of LAT2 on iPCS and EB and diminished on the NPC and N with the opposite pattern occurring with MCT8 gene expression in both cell types. All types of TRs had a diminished expression during iPSCs, EB and NPC phases and a significant increase when the cells became neurons. The IGF-1 expression was found just on neurons with higher expression on Q83X cells.
TH action occurs since the early stage of the development, and when it is already differentiated as neuron TH became more important as reflected in IGF-1 higher expression. Cells derived from Rett syndrome patient had a diminished Dio3 expression and higher IGF-1 expression.

Thyroid Hormone Action Friday Poster Clinical
Introduction: Resistance to thyroid hormone (RTH) is characterized by decreased tissue responsiveness to thyroid hormone, due to mutation of the thyroid hormone receptor. Goiter, learning disabilities, psychological abnormalities, sinus tachycardia, hearing deficits, short stature, and growth delay are among the most common symptoms in patients with RTH.
Methods: Here, we present three patients between 4–14 years old (two males) with RTH (Table) TSH and thyroid hormones were obtained. Thyroid ultrasonography were performed. L-T3 suppression tests were performed to patient with application of daily 50 μg L-T3 on 0-3rd days, 100 μg on 4-6th days, 200 μg on 7–9th days. Thyroid receptor beta (TR-β) gene mutation analyses were performed in our patients.
Clinical features of patients with Resistance to Thyroid Hormones
After L-T3 suppression test, all patients treated with L-T3. All patients have known mutations in TR-β (Table).
Conclusions: Three patients with variable clinical features of RTH, still receiving supra-physiological dose L-T3 treatment. Recognition of disease is of great importance for avoiding diagnostic mistakes that may lead to incorrect and potentially dangerous treatments. Generalized RTH should be considered in patients presenting with elevated free thyroid hormone levels and normal or increased TSH concentrations, especially if these patients appear clinically euthyroid, hypothyroid or hyperthyroid
Thyroid Hormone Action Friday Poster Translational
Prior clinical studies have shown that lowering serum free thyroxine[FT4] was associated with extended survival in patients with terminal cancers. In-vitro, L-tri-iodothyronine (T3) is significantly less pro-oncogenic (mitogenic) at physiological concentrations than L-thyroxine (T4). The objectives of this study were (a) to substitute L-tri-iodothyronine [T3] for L-thyroxine[T4] as replacement therapy for pre-existent hypothyroidism and (b) in euthyroid patients, to use methimazole to induce hypothyroxinemia while adding L-T3 to maintain eumetabolism and prevent the compensatory rise in TSH. Patients from internationally dispersed locations were either self-referred or recommended by attending physicians to the principal investigator.
Patients (n=23)) had advanced, incurable cancer of brain, ovary, lung, pancreas, salivary glands, breast, pulmonary mesothelioma and soft tissue sarcoma. Serum FT4 and TSH were serially monitored at 2-4-weekly intervals to guide adjustments to drug therapy as follows: 1. Passive FT4 depletion following discontinuation of T4 replacement for hypothyroidism [n=9]. Patients were converted abruptly from T4 (50–88 mcg daily) and after a week's ‘washout’, gradually started on exogenous T3 15–37.5 mcg/day in three divided doses. 2. Active T4 depletion with methimazole 40–50 mg/day in a single or divided doses and T3 at 5–12.5 mcg three times/day [n=12] continued until FT4 was below reference range. 3. Two patients were on unchanged L-T3 supplementation at diagnosis with advanced disease.
The difference between the actual vs. expected survival was significant at the p<0.01 level for comparisons of the total population [8 males and 15 females]. The expected odds of surviving for at least 12 months for 19/23 patients was estimated at 15–20% while 20/23 from the FT4 depleted group[90%] survived more than 12 months and 12/23 [52%] survived more than 24 months vs. an expected 2/23 [4.4%].
These preliminary results suggest a clinically measurable outcome of a significant divergence of a pro-proliferative action of T4 from a less proliferative T3 effect on tumor cells and may represent a novel, non-toxic approach for improving outcomes in patients with advanced solid tumors.
Thyroid Hormone Metabolism & Regulation Friday Poster Clinical
Low T3 syndrome is related to inflammatory activity in many diseases. In type 2 diabetes (T2DM), it has been linked only with poor glycemic control. Our objective was to verify if the presence of low T3 syndrome in patients with T2DM is related to glycemic control and/or inflammatory activity.
We selected 140 individuals separated in 2 groups: 70 patients with T2DM and 70 healthy individuals paired by age, sex and body mass index. We evaluated clinical parameters as well as total (T) and free (F) T4, T3, reverse T3 (rT3), TSH, and the relations TT3/rT3, FT4/rT3 and FT4/FT3, high-sensitivity C reactive protein (hs-CRP), serum amyloid protein (SAA) and interleukin-6 (IL-6). We excluded patients with T2DM and conditions associated to low T3. Statistical analysis was performed by non-parametric methods. Linear regression analysis was used to assess the influence of inflammatory variables in thyroid hormone levels adjusted by sex, age, BMI, waist/hip ratio (WHR) and HbA1c with all variables log transformed.
Patients with T2DM had higher WHR (p<0.001), SAA (p=0.04), IL-6 (p=0.01) and FT4 levels (p<0.001); and lower levels of TT4 (p=0.012), TT3 (P<0.001) and FT3 (p<0.001) than control group individuals. FT4/FT3 was higher and FT3/rT3 lower in the T2DM group (p<0.001). IL-6 correlated with T4, rT3, FT3/rT3 and FT4/rT3; SAA with FT3, rT3 and FT4/rT3 and hs-CRP with T4 (Table 1). IL-6 (p=0.042) and SAA (0.048) were positively associated with WHR. In adjusted linear regression, SAA (p<0.001) and hs-CRP (p=0.03) predicted FT3 levels. FT4/FT3 was predicted by SAA (p=0.02) and IL-6 (p=0.041). All associations occurred only in the T2DM group. No associations were found between hormonal variables and HbA1c.
Table 1
Correlation coefficients (r; Spearman's) and significance level (p) of hormonal and inflammatory variables in patients with type 2 diabetes. *p<0.05; **p<0.01.
Hormonal evaluation indicates the presence of low T3 syndrome in patients with T2DM. Abnormalities typical of low T3 were associated with inflammatory activity only in the T2DM group. Lower T3 and higher FT4/FT3 were possibly related to lower type 1 deiodinase activity, probably mediated by subclinical inflammation, which was associated to the central adiposity of T2DM in this study. In conclusion, the physiopathology of low T3 in T2DM was more related to a higher degree of inflammatory activity than glycemic control.
Thyroid Imaging Friday Poster Clinical
The use of hemostatic agents in thyroid surgery has been widely reported in the literature. The aim of this study is to assess the safety and efficacy of hemostatic agents in comparison to conventional technique hemostasis by meta-analysis of the current literature.
Articles were identified from PubMed and EMBASE using the following keyword searches: hemostatic agent thyroid surgery and hemostatic agent thyroidectomy. Outcomes included total operative time, estimated blood loss, length of hospital stay, and intraoperative and postoperative complications. Data were extracted following review of appropriate studies by two independent authors, and outcome differences were calculated using analysis of variance and the Bonferroni method.
Thirty-four publications were identified and 10 studies met our inclusion criteria, totaling 941 patients, 519 (55.1%) of which received a hemostatic agent during a thyroid surgery. Of these patients who had hemostatic agents, 369 (71%) received a hemostatic gel and 150 (29%) received an oxidized cellulose patch. Outcome measures in each of these groups were compared with the patients receiving only conventional methods of hemostasis. The mean operative time in the conventional group 114.95±21.8 minutes was comparable to the operative time in patients who received hemostatic gel 113.75±14.5 minutes (95%CI:-28.634, 8.427). The risk of hematoma formation in the hemostatic gel group was comparable to conventional hemostatic methods (95%CI: 0.330, 2.586). This was also true when comparing conventional hemostasis to the patch (95%CI: 0.642, 15.242). No difference in the risk for seroma formation was found between the conventional and hemostatic gel groups (95%CI: 0.259, 3.951). Drain output was significantly less in the gel group 40.75 mL±35.6 mL compared to 66.26±31.2 mL in the conventional group 95%CI (−23.422, −7.460). Patients who received hemostatic agents had shorter hospital stay when compared to the conventional group 95%CI (−1.057, −0.203).
Our meta-analysis suggests that the use of a hemostatic agent in thyroid surgery yields minimal advantages for the management of perioperative bleeding risk.
Thyroid Nodules & Goiter Friday Poster Basic
Many genetic and environmental factors contribute to the development of multinodular goiter (MNG). Xb130 is an adaptor protein for signal transduction that is highly expressed in thyroid glands. It participates in the regulation of cell proliferation, survival and motility. Investigation of Xb130's role in spontaneous tumorigenesis using old mice revealed that Xb130 knockout (KO) mice developed MNG late in life.
The thyroid glands were dissected from aged (17 to 20 month-old) Xb130 KO (n=45), Xb130 heterozygous (HZ) (n=36), and wild-type (Wt) (n=45) mice and were subjected to histological examination. Serum TSH and T4 levels were measured by radioimmunoassay.
A significantly higher number (60%) of KO mice developed enlarged thyroids, whereas none of the HZ and Wt mice exhibited this abnormality (p<0.01). Histological analysis indicated that the KO mice developed moderate to severe MNG, which is characterized by asymmetrically enlarged glands containing dilated colloid-rich follicles with flattened hyperplastic epithelium. Most (91%) of the Wt mice exhibited normal sized thyroids with normal histology, in contrast to 18% of the KO mice (p<0.01). Only Xb130 KO mice showed severe forms of MNG (45%; p<0.0001). Interestingly, Xb130 HZ group exhibited the intermediate phenotype between the Wt and KO groups, such that nearly 40% of these mice developed moderate forms of MNG (p<0.01). Development of MNG is associated with hypothyroidism caused by dishormonogenesis. We found that younger (6 month) KO mice were hypothyroid with significantly elevated (2.8-fold) TSH (563.0±93.1 mU/L; p<0.01) and relatively lower (1.1-fold) T4 (4.0±0.1 μg/dL; p<0.05) in serum. In contrast, the old (18 month) KO mice had euthyroid MNG with similar serum levels of TSH (112.0±38.6 mU/L) and T4 (3.3±0.2 μg/dL) to those of Wt mice. However, in thyroid tissue, the protein level of total thyroglobulin (Tg) was significantly higher, but iodinated Tg was significantly lower in old Xb130 KO mice, as determined by western blotting.
Xb130 may play important roles in the regulation of thyroid hormone synthesis, and the loss of Xb130 may lead to a permanent defect in iodide organification, which leads to the development of MNG during aging.
Thyroid Nodules & Goiter Friday Poster Clinical
The University HealthSystem Consortium (UHC) database was interrogated to generate a descriptive report of trends in robotic thyroidectomy in the US surrounding the announcement of FDA restrictions for the use of the robot in thyroid surgery in the fall of 2011. UHC represents 90% of non-profit academic medical centers in the US, consisting of 120 university medical centers and more than 300 of their affiliated hospitals (
Data from UHC and another North American institution not included in the UHC database from 1st Q 2009 to 4th Q 2013 (a total of 20 quarters) was compiled. 484 patients undergoing robotic thyroidectomy were identified. Data on age, sex, race, insurance, comorbidities, complications, discharge status, length of stay, and ICU admission were collected. Data on outpatient discharge type, surgeon cost, OR time, and total cost, although incomplete, was also collected.
Mean age of patients was 42 for outpatients and 48.8 for inpatients (p<0.001). There were significant differences in gender, race and insurance status between outpatients and inpatients (p<0.005, 0.001, 0.014 respectively). Comorbidities were significantly more present in inpatients (p<0.001) as were complications (p=0.005). The median hospital length of stay was one day (range: 1–31 days) for inpatients and 57% of outpatients stayed overnight. 8.4% of inpatients required an ICU stay. 99% of outpatients and 97% of inpatients were discharged to home. The highest volume institution did most of the outpatient cases and had a lower rate of complications. There was a clear drop in the number of cases after FDA restrictions release date.
This dataset represents the largest US series of robotic thyroidectomy. Robotic thyroid surgery performed by higher volume surgeons is associated with lower complications and shorter hospital stay. The FDA restrictions impacted the expected growth of robotic thyroid surgery cases in the US. Further studies are warranted to further investigate these important findings.
Thyroid Nodules & Goiter Friday Poster Clinical
Appropriate management of large thyroid (≥3 cm) nodules remains a topic of debate. One of ultrasound guided fine-needle aspiration biopsy (US-FNAB) limitations is that 5–20% of results are nondiagnostic. False-negative (FN) rate of cytology is thus especially problematic, which can result in delayed treatment and, may adversely affect patient outcome. This study evaluate the accuracy, nondiagnostic cytology and false-negative rates of US-FNAB for resected thyroid nodules 3 cm or larger.
We retrospectively studied 242 resected thyroid nodules in a single center, resulting in 94 (42.4%) large nodules (≥3 cm). Preoperative cytological results were correlated with final histological data. The US-FNAB results were reported in accordance with Bethesda cytological system. Histopathology was the standard reference used to calculate accuracy and FN rates of US-FNAB in these large nodules.
Histopathology identified 44.6% malignant (42/94) thyroid nodules over 3 cm vs. 49.6% (69/139) in small nodules (P>0.05). The accuracy of cut-of 3 cm to discriminate malignant and benign lesions was 51.9%, not statically significant. When considering malignant and suspicious for malignancy readings as positive and benign cytology as negative, the sensitivity of Bethesda system was 76.7%; 78.9% of specificity, negative predictive value (NPV) of 82.2% and, 78% of accuracy. For large and small thyroid nodules, we respectively verified: 84.2% vs. 71.8% of sensitivity, 88.4% vs. 80.4% of NPV and 76.5% vs. 76.9% of accuracy. The proportion of Bethesda I (nondiagnostic) result was significant higher in large versus small nodules (9.5% vs. 3.5%). The FN rates were 28.1% for small nodules (<3 cm) versus 36% for large thyroid nodules. Among thyroid nodules 3 cm or larger with Bethesda I results, the risk of malignancy was 55.5%.
This study demonstrated a major proportion of Bethesda I results and false-negative rates of US-FNAB results in thyroid nodules 3 cm or larger. Furthermore, those patients with a nondiagnostic cytology display a high risk of malignancy. Much larger series would be required to determine its utility to guide surgical decision-making referred to nodules 3 cm or larger.
Thyroid Nodules & Goiter Friday Poster Clinical
The thyroid imaging reporting and data systems (TI-RADS) scores do not consider the nodule vascularity as major criteria to stratify malignancy. Both American and European thyroid associations consensus statement considered the increased nodular vascularity as suspicious criteria for fine-needle aspiration biopsy (FNAB) recommendation. This study aimed to evaluate the impact of Doppler study by ultrasound (US) on the TI-RADS results and estimates the improvement of FNAB recommendations and cancer diagnosis.
Retrospective data were available for 243 resected thyroid nodules, including 123 cases with Doppler analysis. The flow pattern seen via power Doppler examination was ranked for each nodule on a scale of 1–5: absent, perinodular, mixed with perinodular prominence, mixed with intranodular prominence, and exclusively intranodular, respectively. The hypervascularity was defined as peripheral and central vascularization, predominant or isolated central flow. All nodules submitted to Doppler study were re-classified by TI-RADS including the vascular analysis by the same author, blinded to histopathological results. The number of FNAB recommendations and malignancy rate were compared between TI-RADS and TI-RADS with Doppler analysis.
The histopathological findings identified 57 (46.3%) malignant and 66 (53.7%) benign cases. Nodular hypervascularity was detected in 49/123 (39.8%) cases, 28.5% of nodules were avascular and 31.7% showed only peripheral flow. The majority of malignant cases showed mixed and predominant central flow (57.8%) in contrast to 24.2% of benign nodules (P=0.01). US-guided FNAB recommendation increased from 89 to 98 cases (7.4%) after Doppler analysis detecting nodules TI-RADS 4 or 5 scores, which resulted in 4 (44.4%) new malignant cases. The misdiagnosis of cancer based on TI-RADS (without Doppler) represented 8.3% of total malignant cases.
The thyroid nodule vascularity determined by Doppler-US contributed to better score TI-RADS, which resulted in improvement in the number of FNAB procedures and cancer detection. Combination of Doppler study to classical TI-RADS score could be used as simple tools to better stratify thyroid malignancy.
Thyroid Nodules & Goiter Friday Poster Translational
The molecular mechanisms regulating cell growth and death in thyroid lesions, such as papillary thyroid carcinomas (PTCs), follicular adenomas (FAs) and Hashimoto's thyroiditis (HT), are still poorly understood. The Mcl-1 (myeloid cell leucemia-1) protein expression is frequently upregulated in various human cancers, such as prostate, lung, and colon cancer. Downregulation of suppressor tumoral gene p27, a cell cycle control, has been found in most cases of thyroid malignancy. Data on these markers in relation to thyroid malignancy are still very limited. Objectives: To investigate the expression of a panel of angiogenic, proliferative cell, and apoptotic markers in normal tissue, benign and malignant thyroid lesions in humans.
Thyroid tissues were evaluated by immunochemistry for angiogenesis (VEGF), proliferative cell (Ki-67, p27), and apoptotic (Fas, FasL, Bcl-2, Mcl-1) markers. We used tissue arrays containing 138 thyroid samples, including 24 neoplastic (10 FAs, 14 PTC) and 114 non-neoplastic specimens (45 adenomatoid nodules (AN), 17 HT, and 52 normal thyroid samples). The positivity for monoclonal anti-Mcl-1 antibody and p27 were considered when at least 20% and 50% of the cells were clearly stained, respectively.
Expression of VEGF stained more strongly positive in FAs, non-neoplastic (AN), and malignant specimens (PTC) than in normal tissue. Ki-67 overexpression was predominant in ANs (17.8%) than in neoplastic lesions (FAs, 10%; PTCs, 0%). The p27 stain was downregulated in 57.2% of PTCs when compared with benign lesions. Mcl-1 protein was robust expressed in PTCs (71.4%) than in HT (35.2%), ANs (31.8%), FAs (20%), and normal tissue (23.5%). Mcl-1 overexpression and p27 downregulation were verified in just PTCs (30%), resulting in a 90.4% negative predictive value. Fas, FasL, and Bcl-2 staining were strongly observed in non-neoplastic and normal tissues.
Mcl-1 upregulation was an important marker for thyroid malignancy, especially in association with p27 underexpression. The pathogenetic differences between normal, malignant and benign thyroid specimens were related to antiapoptotic Mcl-1 overexpression and p27 downregulation in PTCs.
Thyroid Nodules & Goiter Friday Poster Clinical
Thyroid nodules are very common and mostly represent benign lesions. FNA is part of routine patient evaluation in conjunction with clinical-sonographic findings. Current standard of care is to perform a rFNA if there is documented growth during follow-up. However, there is no clear evidence that growth is a surrogate marker for malignancy especially since the traumatic effects of FNA can lead to organizing hemorrhage that may impact size estimates, leading to rFNA' s that add little clinical value. Our objective was to evaluate the clinical relevance of rFNA in patients with previously documented benign thyroid nodules (BTN).
Retrospective chart review of all patients seen at Mayo Clinic between January of 2003 and December of 2013 who had undergone rFNA. We selected the group of patients with an initial benign FNA (iFNA).
A total of 334 initially BTN underwent a rFNA. Patients mean age was 52.3 years and the majority were women (81.1%). Mean follow up was 4 years (range 0.1–10.2 years). The mean time to rFNA was 3.1 years and the most common reason for rFNA was growth during follow up (63.8%). There was a change from iFNA in 49 cases (14.7%). This corresponded to 5.4% reported as suspicious for neoplasm, suspicious for papillary cancer (1.5%) and one case of renal cell carcinoma. We had 19 (5.7%) non diagnostic cases and 6 (1.8%) malignant. These changes resulted in a change in clinical management in 33 cases (10%) including surgical intervention in 30 and medical management of non-thyroid malignancy in another 3. Surgery was performed in 98 patients after a mean follow up of 3.5 years, the most common indication being the presence of compressive symptoms (41%). Histologic diagnosis confirmed thyroid cancer in the index nodule in 3 cases (3.1%), and non-thyroid cancer in 3 cases, which represents a false negative rate of 1.8% when using clinical follow up as a gold standard.
We analyzed 334 initially BTN that underwent rFNA during a 10 year period. The repeat FNA changed management in 10% of the cases and a final histologic diagnosis of thyroid cancer in the index nodule was found in 3 patients. This suggest that a rFNAB might be useful in selected patients.
Thyroid Nodules & Goiter Friday Poster Clinical
Rayan et al. (Eur J Endocrinol 2014, 170:593–599) recently reported that many nodular goiter cases have an autonomously functioning thyroid nodule (AFTN). To our knowledge, there have been no previous reports of AFTN cases with a normal thyroid-stimulating hormone (TSH) level treated with radioisotope therapy (RIT). Herein, we report our investigation of AFTN cases with a normal TSH level treated with RIT.
The subjects were 13 patients (1 man and 12 women) diagnosed as having AFTN with a normal TSH level and treated with RIT. The median age was 69 (interquartile range [IQR]: 58–72) years. Of these 13 patients, 9 had a solitary nodule and 4 had multinodular goiters. All but one patient received a radioisotope at a fixed dose of 481 MBq once, the exception being a patient receiving this treatment twice. The TSH and free thyroxine (FT4) levels at the onset of hypothyroidism and the AFTN volume before and two years after treatment were evaluated.
Thyroid function test results at the onset of hypothyroidism were: TSH, 19.41 (IQR: 2.6–84.89) mIU/L and FT4, 0.85 (IQR: 0.59–0.94) ng/dL. Of the 13 patients, 9 started taking levothyroxine and one had been on this medication since before treatment. The AFTN volume was reduced from 9.73 (IQR: 5.48–12.53) mL to 3.28 (IQR: 0.88–6.45) mL (p<0.05).
RIT significantly reduced the nodule volume in patients with AFTN with a normal TSH level. However, as many patients undergoing RIT experience hypothyroidism, sufficient patient explanation and careful follow-up are required. Our results suggest that the diagnosis of AFTN with a normal TSH level can provide more treatment options to patients with nodular goiter who do not wish to undergo an operation.
Thyroid Nodules & Goiter Friday Poster Clinical
Thyroid ultrasound guided fine needle aspiration (FNA) biopsy is the cornerstone in clinical evaluation of thyroid nodules and enables the number of surgical operations to be reduced. Endocrinologists perform thyroid ultrasound study and FNA biopsy at bedside has become a standard care in American. The present study presents data of FNA biopsy of thyroid nodules by using the Bethesda system for reporting thyroid aspiration cytology from a single endocrine institution in a rural setting mostly serving Appalachian southeastern Ohio.
We reviewed all thyroid FNA biopsy reports that were performed by a single endocrine practitioner in a referral endocrine/diabetes center in Athens City, Ohio, between 05/2012 and 05/2014. Follow-up surgical pathology reports were obtained for all patients known to have undergone thyroid surgery.
There were total 158 cases of thyroid FNA biopsies performed. Of them, according to the Bethesda system for reporting thyroid aspiration cytology, 69% were benign, 3% malignant, 6% follicular lesion of undetermined significance, 11% follicular neoplasm, and 5% non-diagnostic. In the vast majority of cases, FNA biopsy influences subsequent clinical decisions. Correlation of surgical pathology, rates of thyroid dysfunction and Hashimoto's thyroiditis in this series will be also presented (ongoing analysis).
In coupling with clinical and biochemical evaluation, ultrasound guided FNA biopsy remains the first-line diagnostic in the management of thyroid nodules in our practice. FNA biopsy of thyroid nodules can substantially reduce unnecessary thyroid surgeries and subsequently the cost from thyroid surgeries. At present, clinical studies to evaluate potential association of thyroid nodules/cancers with Hashimoto's thyroiditis and/or thyroid dysfunction are desirable to provide further insights into unknown causes of thyroid nodules/cancers in most cases.
Autoimmunity Friday Poster
IgG4-related thyroiditis is newly recognized disease that is characterized by infiltration of lymphocytes and IgG4 positive plasmacytes, and extensive fibrosis in thyroid. IgG4-related thyroiditis is clinically different from non-IgG4-related thyroiditis. IgG4-related thyroiditis is clinically characterized by younger age, a lower female to male, a more rapid and aggressive course, and a higher level of circulating thyroid autoantibodies. Although subacute thyroiditis is the most common cause of thyroid pain, painful IgG4-related thyroiditis should be considered as one of differential diagnosis.
A 35-years old female patient with hypothyroidism complained of recurrent thyroid pain dependent on change of steroid dose. She had soft, diffuse goiter of about 50 g with minimal tenderness. Laboratory testing revealed: T3 0.72 nmol/L, free T4 0.36 ng/dl, TSH>100 IU/ml, anti-TPO 258.3 IU/ml, anti-Tg>4000 IU/ml, TBII 1.25 IU/L. Thyroid scan showed diffuse goiter with increased radionuclide uptake. Thyroid ultrasound showed that hypoechoic area occupied nearly entire thyroid. Thyroid fine-needle aspiration cytology revealed follicular cell clusters with oncocytic change in lymphoplasma-cell background. She underwent total thyroidectomy because of failure of steroid tapering and appearance of iatrogenic Cushing feature.
The tissue pathology revealed severe inflammation and fibrosis. The inflammatory infiltrates were predominantly plasmacytoid cells. Also there were many foci of phlebitis. Thyroid capsule thickened with extracapsular fibrosis. IgG4 immunohistochemistry revealed that the infiltrative plasmacytoid cells were mainly IgG4-positive cells. She discontinued prednisolone through tapering, and her thyroid function was normal on the treatment of synthyroid 150 ug per day.
Our case is the first case report of IgG4-related thyroiditis in patient suffering from recurrent pain in Korea. The identification of painful IgG4-related thyroiditis opens new insights not only for patient's treatment with painful thyroid but also for the development of new diagnostic and therapeutic approaches for this rapidly progressing destructive subtype of thyroiditis.
Autoimmunity Friday Poster
Human anti-mouse antibody (HAMA), the most commonly encountered heterophile antibody, can cause interference in immunological assays; leading to either falsely elevated or depressed values. Here we report a case of a euthyroid patient who had suppressed TSH values for more than a decade, later found to have elevated HAMA levels.
A 69 year old African American male with medical history of cocaine abuse and depression was admitted for suicide ideation. He denied palpitations, tremors, heat intolerance, or visual changes. On physical exam, thyroid was palpable but not enlarged. There were no eye signs, tremors, or thyroid bruit and deep tendon reflexes were intact.
He has had persistently suppressed TSH with normal free T4 and total T3, dating back 14 years in our records. His radioiodine uptake done 14 years ago was 34% with homogenous distribution on the scan. He received a brief trial of methimazole therapy on repeat evaluation a few years later, which he self discontinued after a few weeks, he didn't feel any different while on therapy. He presented several years later with similar thyroid function as before; however, a HAMA level was checked which was found to be >600 ng/ml along with a thyroid stimulating Ig level of 436%. Because the patient was clinically euthyroid, treatment with anti-thyroid medications was not considered.
The patient's suppressed TSH could likely be falsely low due to HAMA; however, considering elevated TSI, Grave's disease cannot be ruled out. To the best of our knowledge, this is the first case of a patient with suppressed TSH levels with both significantly elevated HAMA and TSI Ab. Our case suggests that HAMA interference should be strongly considered if there is any discrepancy between clinical features and lab results to prevent extensive work up, misdiagnosis, or inappropriate treatment.
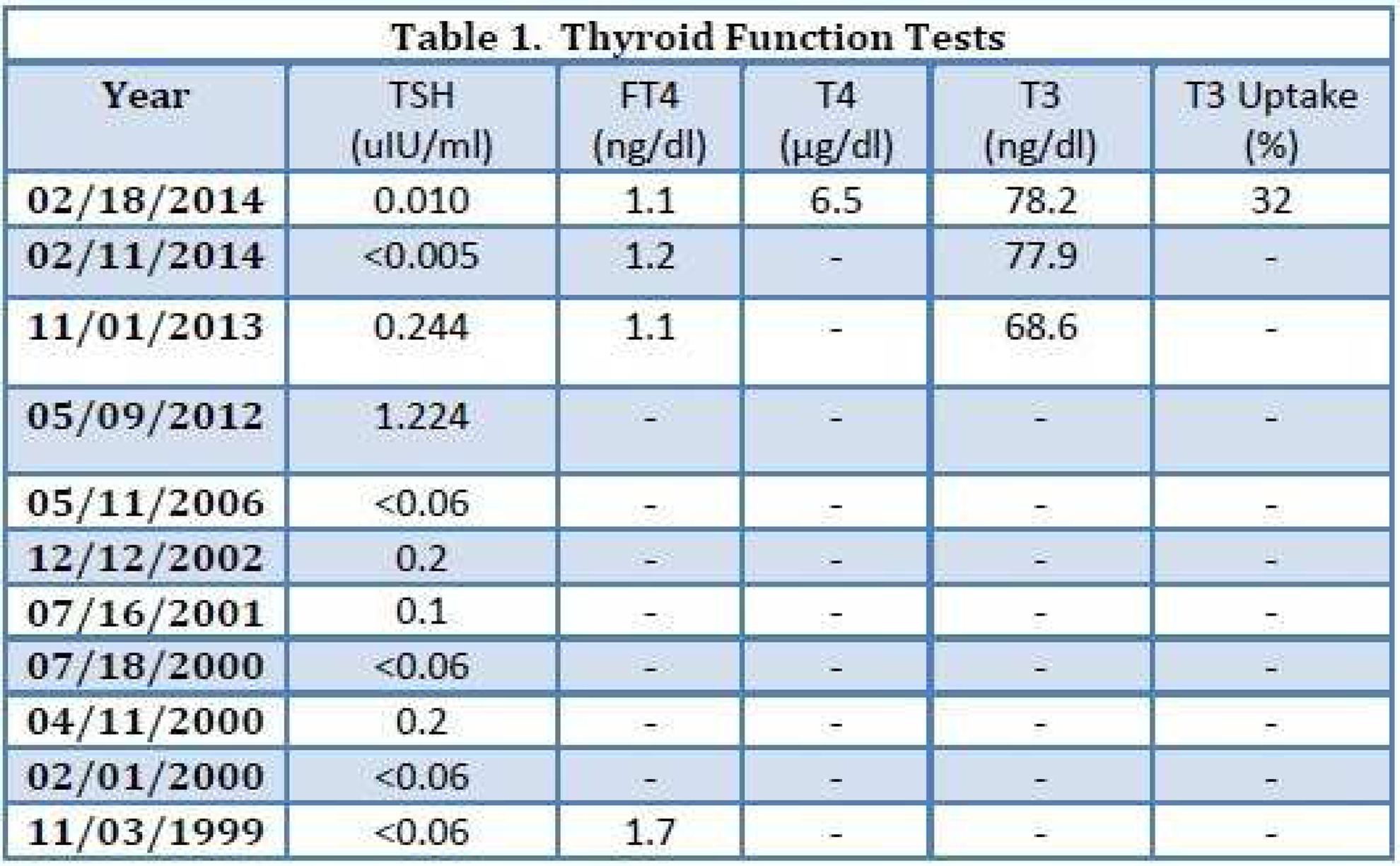
Disorders of Thyroid Function Friday Poster
Thyrotoxic patients who fail thionamide therapy and who are not candidates for radioactive iodine therapy are managed with thyroidectomy. Preoperative normalization of thyroid function is imperative in these patients to decrease the risk of postoperative thyroid storm.
We report three cases of Graves' disease that required rapid preoperative preparation due to unsuccessful therapy with thionamides.
Two patients developed hepatotoxicity during treatment with methimazole (MMI), necessitating discontinuation. When switched to a regimen of propranolol 60–80 mg BID, dexamethasone 2 mg QID, cholestyramine 4 gm QID, and saturated solution of potassium iodide (SSKI) 2 drops TID, both patients became euthyroid in seven days and total thyroidectomies were successfully completed (Figure 1). A third patient started on MMI and metoprolol developed hepatotoxicity, and was then found to be pregnant. She was started on propylthiouracil 100 mg TID, but remained thyrotoxic even when titrated to 600 mg per day. In preparation for definitive therapy with surgery during the second trimester, cholestyramine 4 mg BID, hydrocortisone 100 mg IV BID and SSKI 2 drops BID were started. After 2 days the patient was euthyroid and underwent total thyroidectomy.
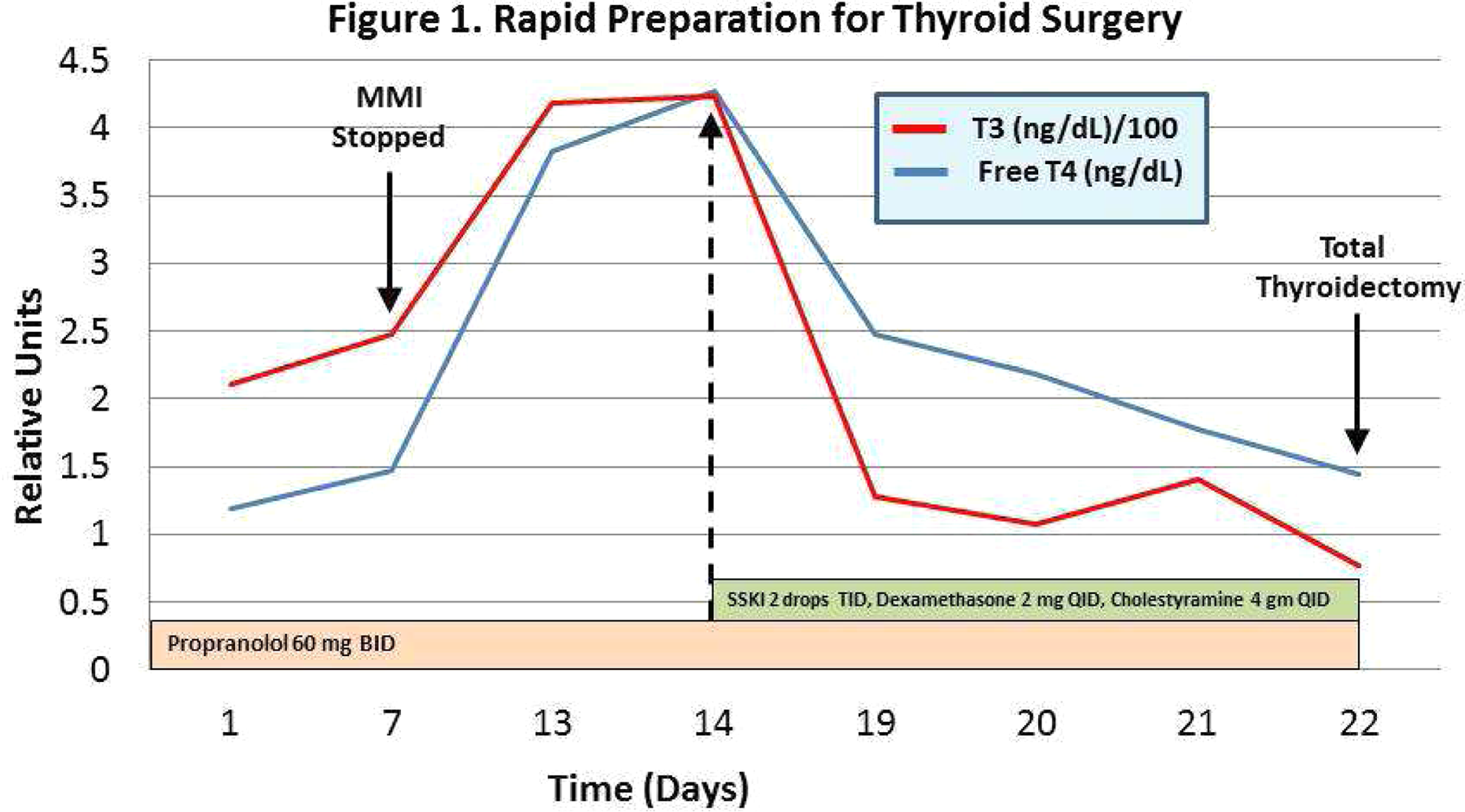
When rapid correction of thyrotoxicosis is necessary for surgery, a combination of medications with various antithyroid mechanisms are essential. β-blockers reduce cardiovascular instability and at high doses, propranolol can inhibit peripheral conversion of thyroxine (T4) to triiodothyronine (T3). Bile acid sequestrants bind thyroid hormone metabolites in the gastrointestinal tract, thereby interrupting the recycling of these metabolites through the enterohepatic pathway. Glucocorticoids at high doses also impair peripheral conversion of T4 to T3. Inorganic iodine inhibits thyroid hormone synthesis and release, but without concurrent thionamides, escape occurs in 1–2 weeks. In cases where neither radioiodine nor thionamides can be used, we present an approach to safely and rapidly prepare Graves' disease patients for thyroid surgery.
Disorders of Thyroid Function Friday Poster
Central hypothyroidism is commonly associated with impaired secretion of other pituitary hormones. Isolated impairment of TRH-TSH-thyroid hormone axis is rare and was mostly identified in children due to genetic mutations or in adults due to morphological changes of pituitary gland.
We present one patient who was diagnosed with central hypothyroidism as an adult. She had no family history of hypothyroidism or apparent morphological changes of pituitary gland on MRI. Other anterior pituitary hormones including FSH, LH, prolactin, cortisol and IGF-1 were normal. She was not taking any medication that can impact thyroid function and she was not in critical illness at the time of thyroid function tests. We did not find clear etiology for her hypothyroidism.
Our patient had “adult-onset idiopathic isolated central hypothyroidism”. There have been five reports involving a total of eight patients with the same disease and a few possible cases in the literature. It might be an autoimmune disease with auto-antibodies that only target TRH/TSH secreting cells. Direct measurement of TRH level may provide more information regarding the location of the lesion.
“Adult-onset idiopathic isolated central hypothyroidism” may not be as rare as previously believed. Patients with this disease present with similar clinical findings as peripheral hypothyroidism. Symptomatic patients responded well to levothyroxine with good prognosis.
Other anterior pituitary hormones (or substitute markers) in the two cases
1. Follicle-stimulating hormone 2. Luteinizing hormone 3. Insulin-like growth factor 1 4. The patient was in follicular phase of menstrual cycle at the time of measurement 5. Afternoon value 6. Morning value 7. Normal range 92–190 ng/ml
Disorders of Thyroid Function Friday Poster
Acute suppurative thyroiditis (AST) due to bacterial infection is a serious, but rare endocrine emergency. There are limited reports of AST in immunocompromised patients and only one prior case specifically in a renal transplant patient (1). The diagnosis can be challenging especially in these patients where the clinical cues of infection may be blunted. We present a case of AST arising in an immunosuppressed patient with a history of renal transplant and myasthenia gravis (MG) with a concomitant urinary tract infection.
A 54-year-old woman with a history of polycystic kidney disease status post bilateral nephrectomy and right renal transplant had been on prednisone (10 mg/day) and tacrolimus (1 mg twice a day) since 1994. She also had a history of MG on azathioprine. She presented with three weeks of dyspnea on exertion and generalized weakness, as well as an enlarging painful neck mass, palpitations, weight loss, tremors, and diarrhea.
On admission she was tachycardic and febrile and started empirically on ertapenem. CT scan of the neck without contrast revealed a large right neck mass, with deviation of the subglottic trachea and mass effect on the right internal jugular and common carotid artery. Labs confirmed hyperthyroidism with a thyroid stimulating hormone (TSH) of 0.01 Uiu/ml (0.27–4.2 Uiu/ml), free thyroxine 5.15 ng/Dl (0.9–1.8 ng/Dl), total thyroxine 18.26 ug/dL (15.1–13 ug/Dl). Physical exam revealed a non-toxic cushingoid woman with a firm asymmetrically enlarged thyroid with tenderness to palpation on the right, and a resting tremor. There was no evidence of lid lag, proptosis, or hypereflexia. Thyroid ultrasound revealed a right 5.5×5.8×5.4 cm complex collection. Thyroid antibodies were negative. Erythrocyte sedimentation rate was 121 mm/hr (0–15 mm/hr). I-123 thyroid scan revealed 2% uptake in the left lobe and a non-functioning right thyroid lobe.
Culture from an aspiration grew E.coli, the same as her urine culture. She was started on imipenem, and went for further incision and drainage with improvement in symptoms. Two weeks later her TSH was 5.68 Uiu/ml and free thyroxine 1.1 ng/dL with subsequent normal thyroid function testing 1 month after her initial diagnosis.
Disorders of Thyroid Function Friday Poster
A 37 year-old Vietnamese man was admitted to the Emergency Room with muscle weakness after working overnight in a factory. He had little oral intake at work and was unable to move his legs or sit upright. He was found to have a low potassium and a suppressed TSH. His only medical history was recently diagnosed Graves' disease.
He had labs drawn and had the following levels:TSH 0.05 uIU/mL, Free T4 4.61 ng/dL, TSI 374, and TSH receptor ab 85.9%. He was found to have a K+ level of 2.6 mmol/L. Thyroid scans previously done had a 6-hr uptake of 77.9% and 24-hr uptake of 80.6%.
He was given 40 mEq of PO KCl and 40 mEq of IV KCl, which increased his K+ to 4.3 mmol/L and improved his muscle weakness. He was started on methimazole 40 mg daily and propranolol 40 mg twice a day then discharged home. On follow up with Endocrinology, his hyperthyroidism was improving and potassium remained in normal ranges.
Thyrotoxic periodic paralysis (TPP) is a sporadic form of hypokalemic periodic paralysis that can occur in patients with uncontrolled hyperthyroidism. While it has been reported in non-Asians, there seems to be a 10-fold increase in incidence in those of Asian descent, particularly men. While the mechanism of action is not clear, it is thought to be related to an increase in β-adrenergic stimulation. This increases Na+/K+/ATPase activity, which results in an influx of potassium into cells. It is thought that those with TPP may have an ion channel defect, which does not manifest in the euthyroid state. We present a case of a man with an unusual complication of uncontrolled Graves' disease. TPP can be precipitated by heavy exercise and while TPP is usually not associated with fasting, the patient had not had much in the way of oral intake during work the night prior to admission. The euthyroid state eliminates episodes of TPP and non-selective β-blockers can be used to help prevent TPP until a euthyroid state is achieved. This case demonstrates the importance of discussing unusual complications of uncontrolled hyperthyroidism that can occur in patients of Asian descent. TPP can be life threatening with the development of bulbar weakness, respiratory weakness, and severe arrthymias.
Laboratory Values
Thyroid Cancer Friday Poster
Brain metastases from differentiated thyroid carcinoma can cause acute life-threatening complications, but their management remains unresolved. Sorafenib is an emerging therapeutic option for radioiodine-refractory differentiated thyroid carcinoma. However, the effects of sorafenib as an adjuvant treatment following surgery or radiation on brain metastases from poorly differentiated thyroid carcinoma have never been reported.
A 52-year-old female patient who underwent total thyroidectomy two months prior for follicular thyroid carcinoma was referred to our clinic for radioactive iodine therapy. Despite high-dose radioactive iodine therapy, radiologic imaging showed a newly developed anterior neck mass and multiple lung metastases. Poorly differentiated carcinoma was diagnosed by mass removal and biopsy. During adjuvant external beam radiation therapy to the neck, brain metastases developed, for which she received palliative external beam radiation therapy for brain metastases. The brain tumor size decreased but lung metastases markedly progressed.
Off-label sorafenib was used to treat progressive multiple metastatic lesions. Over five months of sorafenib treatment, the sum of the longest diameters for target lesions was decreased by 45% in brain and 13% in lung. Unfortunately, mediastinal lymph nodes had progressed over one month of therapy, and most metastatic lesions including brain lesions were aggravated after withdrawal of sorafenib.
Sorafenib can be considered a new adjuvant therapeutic option for metastatic brain lesions from poorly differentiated thyroid carcinoma after external beam radiation therapy. Further clinical trials are needed to completely elucidate the adjuvant role of sorafenib in highly aggressive thyroid cancer, after surgery or radiotherapy.

Thyroid Cancer Friday Poster
Common sites of metastases for papillary thyroid cancer (PTC) include the lungs and bones. Adrenal metastasis is rare and reported in only a few case reports. We describe three patients with this unusual presentation.
A 77-year-old man with T3N1MX BRAFV600E mutated PTC with clear cell features underwent total thyroidectomy and radioactive iodine (RAI) ablation. Post ablation whole body scan (WBS) showed uptake only in the thyroid bed. Two years later thyroglobulin increased from 1.9 to 13 ng/ml in 10 months. Thyrogen stimulated WBS and PET-CT showed metastatic disease in the chest, rib and bilateral adrenal glands [3.2 cm right and 1.2 cm left]. Biopsy of the rib and right adrenal gland showed PTC. He is undergoing further RAI followed by anti-VEGF therapy. A 66-year-old man was initially evaluated for left lower abdominal pain and chronic cough. CT scan revealed cervical and right paratracheal lymphadenopathy and a 10 cm left adrenal mass. Biopsy of paratracheal nodes showed PTC. Thyroid ultrasound revealed a right lobe 2.2 cm mass. Subsequent biopsy of the adrenal mass was consistent with poorly differentiated PTC, positive for BRAFV600E mutation. Thyroidectomy and adrenalectomy were considered but he not a surgical candidate. Carboplatin and paclitaxel was initiated, but after two cycles he has disease progression, with the adrenal mass doubling in size to 20 cm. Vemurafenib, a selective BRAF inhibitor, was started but patient died a few months later.
64 year-old man with Hurthle cell cancer s/p total thyroidectomy and RAI at initial diagnosis. Nine years later he was found to have widely metastatic disease including a right adrenal (6.2×3.5 cm) in addition to lung, bones, liver, kidney, brain, pancreatic metastases, which were all RAI non-avid. No mutations were identified. He has received treatment with 6 systemic therapies to date.
DTC with metastasis to the adrenal glands is rare and portends a poor prognosis. Adrenal nodules in these patients needs to be considered as potential metastasis and worked up. Although the BRAFV600E mutation was present in two of these patients it remains unclear whether this denotes an association with progression to adrenal metastatic disease. Long term surveillance with serial cross-sectional imaging, tissue sampling with molecular profiling and Tg measurement remain key in monitoring patients with advanced disease.
Large [6.2×3.5 cm] right adrenal hypermetabolic metastasis
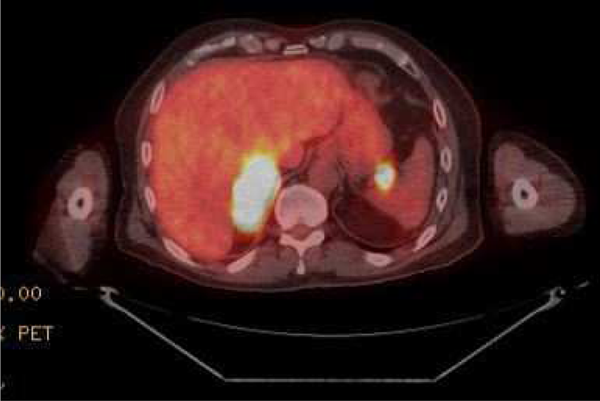
Thyroid Cancer Friday Poster
Thyroid cancer accounts for 1–2% of all malignancies. Papillary carcinoma (PTC) is the most common thyroid cancer (75–80%), whereas medullary carcinoma (MTC) occurs infrequently (5–8%). PTC and MTC co-exist in <0.5% of thyroid cancers. Most of these patients are symptomatic and show lymph node metastases at the time of diagnosis. We present a rare case of an asymptomatic and non-metastatic patient with this combined entity.
A 43-year-old white female was evaluated in the endocrinology office for thyroid cancer due to a positive family history of medullary thyroid cancer (MEN 2A) in her cousin. Her physical exam was normal. Genetic testing for RET proto-oncogene was positive. Further blood work showed an elevated calcitonin level - 72 pg/mL. The remaining tests were normal: TSH - 0.66 mIU/L, Free T4 - 1.4 ng/dL, thyroglobulin −<2 ng/mL, PTH - 26 pg/mL, urine metanephrine −88 mcg/24 hours, norepinephrine - 32 mcg/24 hours and normetanephrine - 243 mcg/24 hours. Thyroid ultrasound revealed a diffuse, nonhomogeneous texture with no definite cyst or nodules. A CT scan of neck, chest and abdomen were negative for metastases. Subsequently, she had total thyroidectomy; histopathology report revealed simultaneous micromedullary (0.8 cm) and micropapillary (0.8 cm) thyroid cancer with lymphocytic thyroiditis. Post-operative PET scan was unremarkable
Thyroid cancer is a neoplastic growth of the follicular or parafollicular thyroid cells. It is divided into papillary, medullary, follicular and anaplastic types. Despite different embryonic cell origins, simultaneous papillary and medullary thyroid cancer can, rarely, co-exist. Although many different theories have emerged for this co-existence, their simultaneous presence is thought by most to be a coincidence. Radiation exposure and family history are the two most common risk factors. RET proto-oncogene mutation has been associated with the familial type of MTC as well as MEN 2A and 2B
Our case highlights the importance of genetic screening, early diagnosis and adequate treatment in those with a positive family history of a genetic mutation. This may facilitate recognition of familial cases of thyroid cancer at an asymptomatic stage.
Thyroid Cancer Friday Poster
Malignant tumors of the thyroid gland account for 0.5–1% of all malignancies. According to the tumor classification of the World Health Organization (WHO), thyroid tumors are classified as epithelial or nonepithelial, benign or malignant, primary or metastatic. The prevalence of intrathyroid metastases of nonthyroid origin ranges from 1.9% to 2.5%. We report a rare case of metastatic sarcoma diagnosed in the thyroid gland by fine needle aspiration (FNA) biopsy.
Our patient is a 49 year old male with a past medical history of melanoma and an intermediate grade sarcoma of probable peripheral nerve sheath origin in the small bowel two years prior. The most recent imaging of the chest for the surveillance of his disease detected a 1.2×0.9 cm hypoechoic nodule in the right lobe of the thyroid. His TSH was within normal limits at 2.28. He denied any symptoms suggestive of hypo or hyperthyroidism, hoarseness, dysphagia, positional shortness of breath, or neck pressure.
An FNA was performed with 25 gauge needles. Air-dried slides were stained with Diff-Quik and methanol fixed slides with Papanicolaou stain. Smears showed numerous loosely cohesive pleomorphic spindle cells. The nuclei were oval or spindle, with hyperchromatic chromatin and inconspicuous nucleoli. The cytoplasm was moderate in amount, and delicate. Normal follicular cells and colloid were present in the background (Figure 1). Subsecuently he underwent a total thyroidectomy. The specimen demonstrated a white-pink lobulated mass measuring, 1.7×1.2 cm (Figure 1). The tissue was formalin fixed, paraffin embedded, and stained with hematoxylin and eosin (H&E). The tumor was composed of sheets of pleomorphic spindle cells. High mitotic rate (8-10/10 high power fields) was noted (Figure 1). The histology was similar to that seen of resected small intestine sarcoma, confirming the cytologic diagnosis.
FNA smears were stained with Diff quik (A and C) and papanicolaou stain (B and D) (low and high power fields), which demonstrates slight loosely cohesive tissue fragments containing short fascicles of spindle cells with scant to moderate delicate cytoplasm, round to spindle nuclei with hyperchromatic granular chromatin and smooth nuclear membrane, apoptosis, and crushing artifact.
Tissue sections from thyroidectomy (E) and small intestine (F) were stained with H&E stain (high power field), which showed short fascicles of pleomorphic spindle cells with cytomorphologic features similar to those seen in the FNA cytology, high mitotic rate (8-10/10 high power fields). The tumor cells from thyroid and small intestine were immunoreactive to S-100 (G and H).

The FNA is useful and safe procedure with low morbidity and can also help avoid unnecessary thyroidectomy in patients with a poor prognosis. The cytomorphology can be compared to the original tumor and a cell block used for immunohistochemical studies. Metastasis should be considered in any patient with a previous history of malignancy and a new thyroid mass.
Thyroid Nodules & Goiter Friday Poster
Primary thyroid lymphoma accounts for <5% of thyroid malignancies. It usually presents with a rapidly enlarging neck mass causing compressive symptoms. On the other hand, cancers metastatic to the thyroid are generally discovered in the setting of a known primary malignancy (eg, breast, renal, lung). We present an unusual case of lymphoma diagnosed by FNA of a thyroid nodule.
Clinical Case: This is a 65 year old man who was noted to have right inguinal lymphadenopathy during a visit with his primary doctor for right knee pain. The lymph nodes were rubbery, mobile and tender. He denied fever, weight loss, night sweats, or pruritis. PET/CT showed inguinal and axillary lymph nodes as well as bilateral thyroid nodules which were all FDG avid. FNA and excisional biopsy of a groin lymph node showed atypical lymphocytes but no evidence of lymphoma. Thyroid ultrasound showed bilateral thyroid nodules and he was referred to Endocrine. In Endocrine clinic he denied change in his neck, dyphagia, dyspnea or dysphonia. The physical exam did not show thyromegaly or distinct thyroid nodules. FNA of the right thyroid nodule showed atypical lymphocytes without normal follicular cells. Flow cytometry was suspicious for large B cell lymphoma but molecular studies for B cell rearrangements were indeterminate. At that time Oncology did not feel there was sufficient data to warrant treatment. On repeat ultrasound, there was an increase in size of the left thyroid nodule and FNA of that nodule was performed. Cytology and flow cytometry were consistent with B cell lymphoma, large cell type.
Patient underwent 6 cycles of R-CHOP chemotherapy and post-treatment PET showed no FDG avid lesions. Additionally, repeat ultrasound showed resolution of the thyroid nodules.
This man's lymphoma was diagnosed by FNA of a thyroid nodule. This case is not typical of primary thyroid lymphoma due to his presentation. However, it is also unusual to detect thyroid metastases of lymphoma in a patient where excisional lymph node biopsy was negative. Fortunately, this patient did well with chemotherapy and serves as a reminder to consider extranodal lymphoma in the differential diagnosis of thyroid nodules.
Saturday, November 1, 2014
Thyroid Hormone Action Saturday Oral Basic 2:20 PM
Amphibian metamorphosis is totally dependent on thyroid hormone (T3) and offers a unique opportunity to study how T3 controls postembryonic development in vertebrates. TR mediates the effects of T3 during Xenopus metamorphosis. Liganded TR recruits histone modifying coactivator complexes to target genes during metamorphosis. This leads to nucleosomal removal and histone modifications, including methylation of histone H3 lysine (K) 79, and the activation of T3-inducible genes.
We have studied the regulation of the only known methyltransferase for histone H3K79, the evolutionally conserved Dot1L, by T3 and used a Dot1L-specific TALEN to knockout endogenous Dot1L in order to determine the role of Dot1L during development.
We have shown that DotlL is regulated by T3 directly at the transcription level during intestinal remodeling when adult intestinal stem cells are formed de novo. We demonstrate that the activation of Dot1L is directly through TR binding to a T3 response element in the promoter region during metamorphosis. We show that Dot1L can be efficiently knockout with a TALEN, resulting in the loss of H3K79 methylations in animals. Importantly, Dot1L knockdown has no apparent effect on embryogenesis since normal feeding tadpoles are formed. The availability of such Dot1L knockdown tadpoles should allow us to investigate whether Dot1L plays a role in the response of premetamorphic tadpoles to exogenous T3. Interestingly, Dot1L knockdown severely retards the growth of the tadpoles and leads to tadpole lethality prior to metamorphosis.
Our findings together with the lack of maternal Dot1L indicate that Dot1L and H3K79 methylation are dispensable for embryogenesis but essential for tadpole growth and development prior to metamorphosing into a frog. They further reveal interesting similarities and differences between Xenopus and mouse development and suggest the existence of two separate phases of vertebrate development with distinct requirements for epigenetic modifications. Finally, the regulation of DotlL by T3 suggests that TR activates Dot1L and the latter in turn participates in adult intestinal stem cell development through a positive feedback to enhance H3K79 methylation and gene activation.
Thyroid & Development Saturday Oral Basic 2:35 PM
The stem cells governing formation of the intestinal epithelium undergo molecular changes around birth corresponding to the initiation of milk consumption to weaning, a postembryonic developmental time period when thyroid hormone (TH) levels peak. Surprisingly, very few studies have examined mechanisms governing the transition of embryonic into adult intestinal stem cells or the effects of thyroid hormone on stem cell maturation. During Xenopus (X.) laevis metamorphosis, a remodeling of the larval intestinal epithelium occurs which is analogous the postembryonic maturation of the mammalian intestine. Thyroid hormone is critical for the formation of adult epithelium in the intestine for both mammals and amphibians but the tadpole provides an opportunity to examine the molecular mechanisms of TH action independent of maternal influences.
Genome-wide analysis of X. laevis revealed an expressed sequence tag (EST) of an unknown gene was upregulated in the intestinal epithelium during stem cell formation. Rapid amplification of cDNA ends was used to identify the gene and then qPCR, in situ hybridization and immunohistochemical analyses were utilized to analyze its role during intestinal stem cell development.
The EST was determined to be a part of the 3' UTR of the Mxd1 gene that encodes for the Mad protein, a bHLH/Zip transcription factor that competes with cMyc to heterodimerize with Max. Previous studies have shown that Mad/Max dimers inhibit transcription leading to differentiation while cMyc/Max binding induces proliferation. Mad expression was confirmed to be epithelial specific during metamorphosis. In both naturally and TH induced metamorphosing intestines there is strong induction of Mad just prior to cMyc expression and adult stem cell formation. High levels of Mad expression is localized to apoptotic larval cells while cMyc expression is in newly forming adult stem cells.
Our findings suggest TH induced Mad plays a novel role of inducing apoptosis in the maturing intestine, which was further supported by high levels of Mad in other apoptotic tissue. Thus cMyc/Mad balance is likely critical for cell fate determination during TH-dependent postembryonic adult stem cell development.
Thyroid & Development Saturday Oral Basic 2:50 PM
Adult organ-specific stem cells are essential for tissue homeostasis and repair. Since the intestinal epithelium is constantly renewed every 2–6 days throughout adulthood and uncontrolled proliferation of ISC can lead to intestinal cancer, the intestinal epithelial stem cells (ISC) are often used as a stem cell model system. Indeed, elucidating the molecular mechanisms regulating the formation of adult stem cells during development is important to determine how stem cell activity leads from normal renewal to cancer development, yet poorly understood. During mouse development, formation of adult ISC takes place around birth when plasma thyroid hormone (TH) levels peak. TH is essential for postembryonic development in several species and functions by binding to nuclear TH receptors (TRs), which in turn recruit coactivators and promotes gene transcription. One of these coactivators is the protein arginine N-methyltransferase 1 (PRMT1) that mediates post-transcriptional modification of target proteins and is upregulated around birth in the developing stem cells. Thus, we hypothesize that PRMT1 is involved in TH-dependent intestinal stem cell formation.
As the homozygous knockout (KO) of PRMT1 in the whole mouse is embryonic lethal, we generated a conditional KO to investigate the participation of PRMT1 in ISC development via the Cre-Flox System using Villin-Cre as a specific intestinal promoter. The phenotypes were analyzed via Immunohistochemistry.
Our results indicate that conditional PRMT1 KO animals had altered intestinal crypt development by the time the adult intestine is developed. The crypts were elongated and thinner compared to wild type control. Further, proliferation in this crypt area was significantly reduced, indicative of a reduction in stem cell activity. In addition, when TH was administered around birth to promote adult stem cell development, we observed similar effects in the PRMT1 KO juveniles.
These findings indicate that PRMT1 is important for TH-dependent formation of adult intestinal stem cell development during mouse intestinal maturation and therefore, PRMT1 dysregulation may play an important role in intestinal diseases and cancer.
Disorders of Thyroid Function Saturday Oral 3:05 PM
The molecular mechanisms of thyroid hormone synthesis have been extensively studied with unexpected discoveries. XB130, also known as actin filament associate protein 1 like 2 (AFAP1L2), is an adaptor protein that regulates cell proliferation, survival, migration and gene expression. It is highly expressed in both human and mouse thyroid glands.
Newly generated Xb130 knockout (KO) mice were used and compared with their wild type (WT) littermates.
Xb130 KO mice showed growth retardation starting from postnatal week (PW) 2 to 3 with most significance at PW 4. This growth delay was mostly compensated at PW 8. Adult Xb130 KO mice developed severe goiter. Histological assessments revealed enlarged colloid with significantly higher number of Ki67 positive thyroid follicular cells in Xb130 KO mice, and thyroidectomy cells in the pituitary. At PW 2, Xb130 KO mice had significantly lower serum concentrations of T3; 21.5±3.2 (mean±SE) ng/dl (WT 39.0±5.8 ng/dl) and T4; 0.4±0.05 μg/dl (WT 7.3±0.2 μg/dl), and the TSH was 11176.9±553.5 mU/L or approximately 50-fold higher than WT mice (250.4±64.7 mU/L). Furthermore, the T4 content in thyroid tissue of Xb130 KO mice was 7-fold lower than WT mice with similar thyroid weight. At PW 14, Xb130 KO mice had similar serum concentration of T3; 46.7±7.6 ng/dl (WT 46.0±7.1 ng/dl); however still significantly lower T4; 3.5±0.1 μg/dl (WT 4.9±0.2 μg/dl) and 10-fold higher TSH in Xb130 KO mice. In contrast, the T4 content in Xb130 KO mice thyroid tissue reversed to approximately 5-fold higher than WT mice; the Xb130 KO mice thyroid weight is 3-fold higher than WT mice. The mRNA levels of Tshr, Slc5a5, and Slc26a4 were significantly up-regulated at PW 2, 4, and 12, and Duox1 and Tpo at PW 4 and 12 in Xb130 KO mice; whereas Duox2 and Tg mRNA expressions were not changed at all time points. Furthermore, the iodination of thyroglobulin was defected in Xb130 KO mice.
Xb130 KO mice showed compensatory hypothyroidism with an apparent defect in thyroid hormone synthesis and also possibly secretion.
Thyroid & Development Saturday Oral Clinical 2:20 PM
This study aimed to determine whether the prevalence of an anomaly called “methimazole (MMI) embryopathy (single or multiple existence of choanal atresia, esophageal atresia, aplasia cutis, umbilical defects, or omphalocele)” increases with MMI exposure in the first 12 gestational weeks.
We performed a prospective, multicenter, observational study. Since 2008, women with Graves' disease who became pregnant were registered from several thyroid clinics at the Japan Drug Information Institute in Pregnancy. The MMI group comprised pregnant women with Graves' disease who took any dose of MMI and/or propylthiouracil (PTU) during the first trimester. The PTU group comprised women who took any dose of PTU, but not MMI, during the first trimester. The non-antithyroidal drug (ATD) group comprised women who did not take any dose of PTU or MMI during the first trimester. Pregnancy outcomes were collected from participants and related medical institutes by mail or phone.
When the fifth case of MMI-related anomalies was reported in 2011, an interim analysis was performed because an extremely high incidence of embryopathy was anticipated. The collection rate of pregnancy outcomes was 90.1%. In the MMI group, there were five cases of MMI-related embryopathy in 85 live births (95% confidence interval: 1.9–13.2%), which was higher than the general incidence, estimated as 0.1%. However, no cases of MMI-related embryopathy were found among 121 (0.0–2.4%) PTU group live births and 83 (0.0–3.5%) non-ATD group live births. The five cases of MMI embryopathy had exposure to MMI during the whole pregnancy period and had patent omphalomesenteric ducts with or without omphalocele. One of the cases was also complicated by aplasia cutis.
We recommend avoiding continuation of MMI during the organogenesis period in women with Graves' disease. We have prospectively collected approximately 1000 outcomes of pregnancies complicated by Graves' disease. The final report will be made by 2015 to clarify whether cession of MMI in early pregnancy (i.e., 4 or 5 gestational weeks) is safe.
Thyroid & Development Saturday Oral Translational 2:35 PM
Introduction: Despite early detection and treatment of congenital hypothyroidism (CH), affected children still show persisting cognitive deficits. Prior studies have found degree and type of deficit reflects CH severity at time of diagnosis. We previously described abnormalities in cortical morphology among children with CH (Rovet et al, ATA 2012), consistent with animal evidence showing the cortex needs an adequate supply of thyroid hormone (TH) to develop properly. Not known, however, is whether cortical abnormalities in CH reflect severity of neonatal hypothyroidism at diagnosis.
Methods: Participants were 41 children with CH identified and treated early in life and continuously followed at Toronto's Hospital for Sick Children. At 10–14 years, all underwent neuropsychological testing and received MRI scanning. Scans were analyzed in FreeSurfer, which provided measurements of cortical thickness (CT). Correlations were performed between CT values and diagnostic TSH and T4 levels, etiologic subgroups were compared, and CT findings were correlated with IQ levels.
Results: Lower T4 and higher TSH values at diagnoses were correlated with thinning or thickening throughout cortex (Figure). Regions that were thinner when CH was more severe were the right superior and middle frontal gyrus, left superior temporal gyrus and lateral fissure; right inferior parietal gyrus and parieto-occipital sulcus. Regions that were thicker were left superior frontal gyrus, middle frontal sulcus, and calcarine sulcus; right postcentral gyrus and inferior temporal sulcus. Relative to ectopic etiology, children with athyrosis showed thinning in right occipital gyrus and thickening in left middle frontal and inferior parietal gyri. Lower IQ was associated with thickening of left middle frontal gyrus and superior frontal gyrus.
Brain Regions Correlating with T4 Levels at Diagnosis. Upper panels show significant clusters in lateral views (positive correlations in red, negative in blue). Lower panels show sample correlations for two regions.
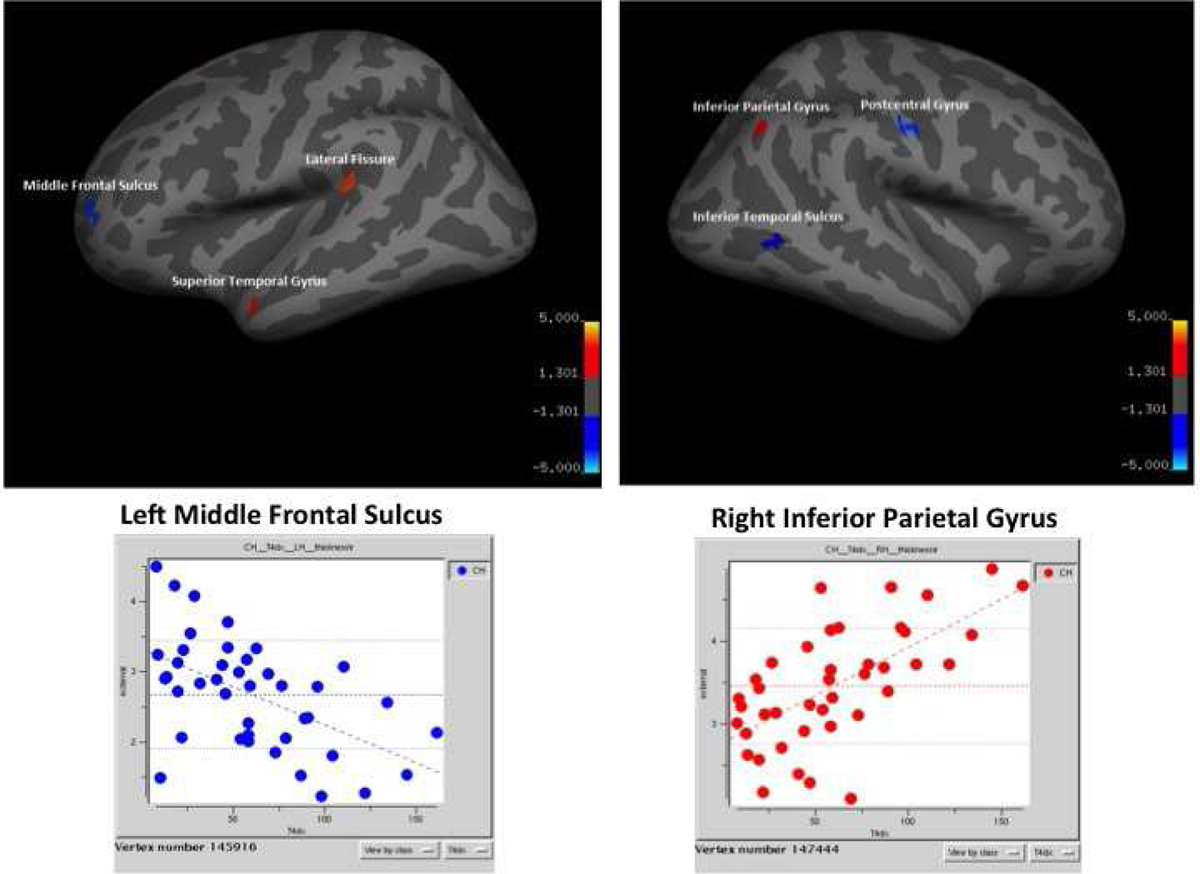
Conclusions: Abnormalities in cortical morphology in CH reflect severity of hypothyroidism prior to diagnosis signifying TH is needed in late gestation and early infancy for human cortical development. Moreover, as some brain regions affected by a lack of TH are associated with later intellectual functioning, this may explain some of the cognitive weaknesses children with CH still experience.
Disorders of Thyroid Function Saturday Oral Clinical 2:50 PM
Myxedema coma (MC), a rare form of decompensated hypothyroidism, can be fatal if not diagnosed and treated promptly. The goal of this study is to characterize the diagnosis of MC and evaluate the efficacy and safety of treatment with 500 mcg IV L-thyroxine.
A case series of 45 patients with MC at LAC+USC Medical Center in Los Angeles from 2004 through 2014 were evaluated. The diagnosis of MC was made based on the presence of signs and symptoms of hypothyroidism (hT) and altered mental status (AMS), defined as A&O <3, +/− a precipitating event (PE) and low serum FT4 and/or high TSH values (in primary hT). Biochemical evidence of hT was generally present but not necessary for initiation of treatment. All patients were given 500 mcg IV L-thyroxine (LT4 load). Patients' demographic information, treatment outcome, and mortality were evaluated.
Forty-five patients (27 women; 60%) of 58.7 +/− 16.9 years of age (range, 26 to 97 years) with 56% Latino ethnicity were evaluated. Thirty (66.7%) patients presented in fall and winter with sepsis as the most common PE (17 of 40 patients; 42.5%). The majority of patients were admitted to the ICU (30 of 39 patients; 76.9%). The median FT4 value was 0.39 ng/L (IQR 0.083-0.5). The median TSH for 38 patients with primary hT was 69.28 mIU/mL (IQR 54.27-130.1). Average time from presentation to treatment with LT4 load was 27.3 +/− 18.9 hours with 20 of 29 (69%) patients showing improvement in AMS within 24 hours. No acute cardiovascular complications following LT4 load were noted. Three (6.7%) patients died with sepsis being the predominant cause of death.
To the best of our knowledge, this is the largest case series of MC patients described. The diagnostic criteria of hT symptoms/signs and AMS +/− a PE and low serum FT4 and/or high TSH values should be used to identify patients with MC. LT4 load is safe and effective at reversing symptoms, particularly AMS, within a short period of time (<24 hrs) and should be the standard of care. The majority of patients had good outcome except for a small percentage of patients who were septic and had significant comorbidities, highlighting the importance of supportive care for successful treatment.
Disorders of Thyroid Function Saturday Oral Clinical 3:05 PM
Hyperthyroidism in women of reproductive age is predominantly caused by Graves' disease. Pregnancy may influence the time of disease onset, but population-based estimates on the incidence in and around pregnancy have not been reported.
Population-based cohort study using Danish nationwide registers. All women who gave birth to ≥1 singleton live-born child in Denmark from 1999–2008 (n=403,468) were identified, and information on maternal hospital diagnosis/surgical treatment of hyperthyroidism and redeemed prescriptions of antithyroid drugs (ATDs) was obtained. Incident cases of hyperthyroidism in the period from 1997–2010 were defined as a) no previous hospital diagnosis or treatment of thyroid disease and b) ≥2 redeemed prescriptions of ATDs within a period of more than one month. The incidence rate (IR) of hyperthyroidism was calculated in three-month intervals before, during and after the mother's first pregnancy in the study period. Secondly, the risk of early pregnancy (first trimester) and postpartum onset (4–15 months after giving birth) of hyperthyroidism in first vs. subsequent pregnancies was evaluated in multivariate (e.g. maternal age, smoking) logistic regression.
Altogether 3,743 mothers (0.9%) were identified with onset of hyperthyroidism from 1997–2010, and the overall IR of hyperthyroidism was 66.3/100,000/year (horizontal line in Fig. 1). The IR of hyperthyroidism in and around pregnancy varied widely (Fig. 1) and was high in the first trimester of pregnancy (incidence rate ratio (IRR) vs. the overall IR: 1.44 (95%CI 1.05–1.97)), very low in the third trimester (IRR 0.25 (0.15–0.43)), and reached the highest level 6–9 months postpartum (IRR 3.53 (2.67–4.66)). Compared with first-time pregnancies, the risk of early pregnancy onset of hyperthyroidism was higher in subsequent pregnancies (adjusted odds ratio (aOR) 1.65 (95%CI 1.19–2.28)) whereas the risk of postpartum onset was lower (aOR 0.69 (0.60–0.79).
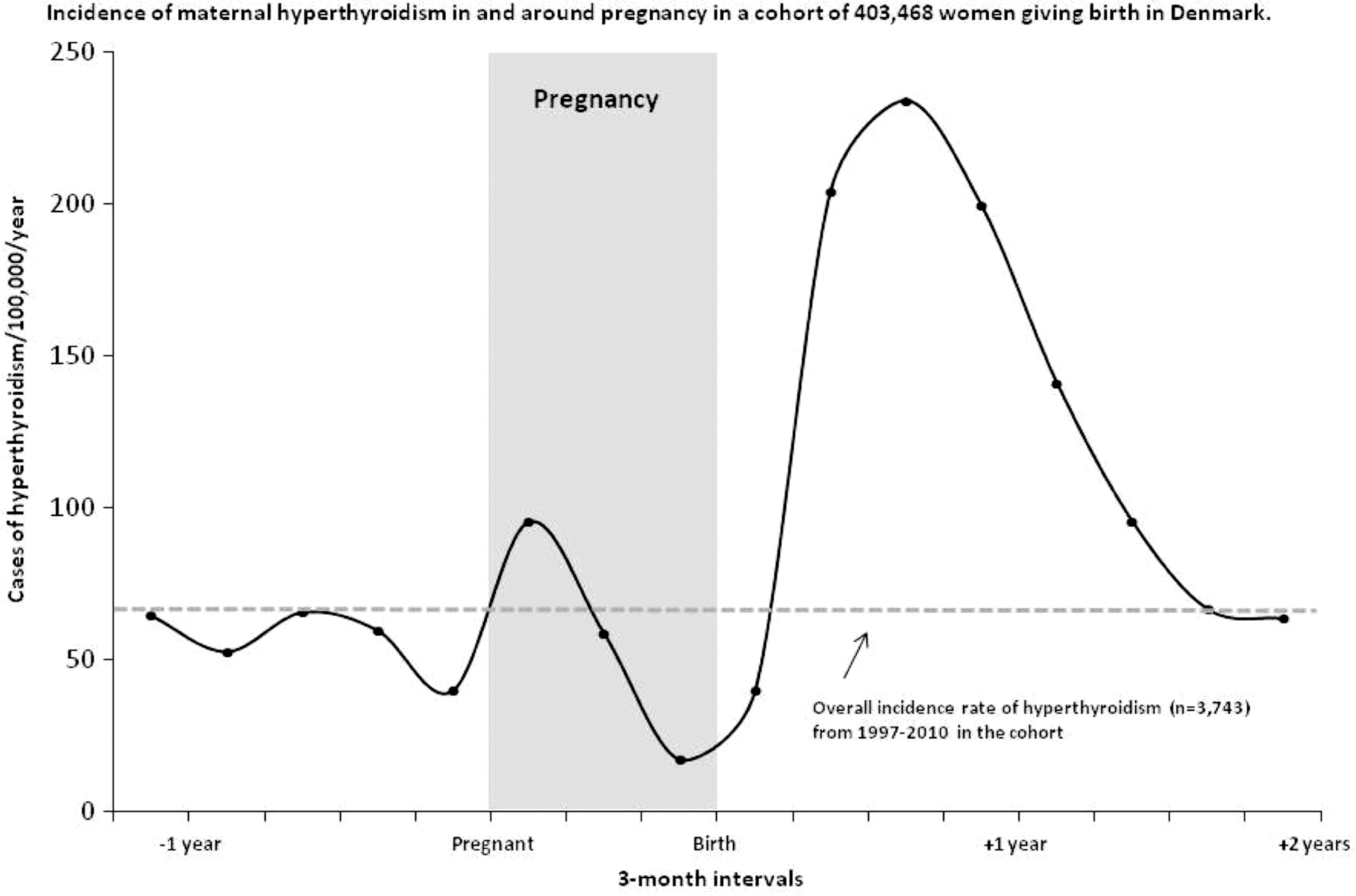
These are the first population-based data on the incidence of hyperthyroidism in and around pregnancy. A wide incidence variation was observed, and the risk of early pregnancy and postpartum onset was differently influenced by maternal parity.
Withdrawn
Autoimmunity Saturday Poster Basic
Hashimoto's thyroiditis (HT) is the most prevalent autoimmune thyroid disorder. Apoptosis plays a pivotal role in the pathogenesis of autoimmune diseases. D7S6440 microsatellite is a short tandem repeat of ca-nucleotide motif, located inside the HIPK2 gene. HIPK2 may induce cell cycle arrest and apoptosis via p53 phosphorylation at specific residues, and its loss is frequent in well differentiated thyroid tumors. Aim of the present study is to assess whether haplotype distribution of D7S6440 has characteristics consistent with molecular markers of HT disease.
Using the simple sequence length polymorphism (SSLP) analysis, we studied 108 genomic DNA samples taken from leukocytes of 78 HT patients and 30 healthy controls subjects.
Five D7S6440 haplotypes were detected, namely O14, O15, O14/15, O15/16, O14/16. Haplotypes O14 and O14/15 were found in both HT and control samples (O14=69 vs 73%; O14/15=21 vs 27%). In contrast, the other haplotypes were detected in the HT group only (O15=7 vs. 0%, O15/16=1 vs. 0%, O14/16=2 vs. 0%). Statistical significance was observed for O15 haplotype only (P<0,005).
The specific intragenic microsatellite haplotypes O15, O15/16, O14/16 are present only in patients HT. The specific intragenic microsatellite haplotypes O15 could represent a useful genetic marker to identify HT.
Autoimmunity Saturday Poster Basic
p53, which is encoded by the tumor suppressor gene TP53, plays a crucial role in the regulation of mechanisms of cell cycle arrest and apoptosis. Some SNPs of TP53 have been associated with increased susceptibility to develop autoimmune diseases as well as cancer. Up to now, five SNPs have been recognized in the coding region of exon 4.
By direct sequencing of exon 4, we investigated the genotypic distribution of such SNPs in a cohort of Caucasian HT patients (n=79, 11 M and 68 F; mean age±SD: 45±15 yr) and 30 age- and sex-matched healthy subjects (5 M and 25 F, mean age±SD: 40±17 yr).
For the Pro72Arg SNP we found these rates in HT patients: 11.4% (wild-type Pro72Pro), 24.0% (heterozygous Pro72Arg), 64.6% (homozygous Arg72Arg). The corresponding rates in healthy controls were 10%, 46.7% e 43.3%, respectively. Thus, significantly different were heterozygosity (24.0% vs 46.7%, P=0.02) and homozygosity 64.6% vs 43.3%, P=0.04). The genotypic distribution for the other SNPs (Pro34Pro, Pro36Pro, Pro47Ser, and Arg110Leu) was the same in HT patients as compared to controls: 100% wild-type, 0% heterozygous, 0% homozygous vs 100% wild-type, 0% heterozygous, 0% homozygous. Similarly for the SNP Pro36Pro the distribution was: 99% wild-type, 1% heterozygous, 0% homozygous in patients vs 99% wild-type, 1% heterozygous, 0% homozygous in controls.
Our data, the first on a Caucasian population, indicate an increased prevalence of the homozygous genotype Arg/Arg and a decreased prevalence of heterozygous genotype Arg/Pro of Pro72Arg SNPs in HT patients compared to controls, suggesting that such SNPs may confer susceptibility to HT. The other SNPs are rare or absent in our population.
Thyroid Nodules & Goiter Saturday Poster Basic
P53 isoforms, namely Δ133 include α, β and γ forms. These spring from alternative initiation of P53 translation through use of an internal promoter (P2) located in intron 4. Δ133p53 isoforms initiate at codon 133 of P53 protein, modulating cell proliferation and cell fate outcome in response to DNA damage. Our aim was to examine immunoexpressions of Δ133 in benign proliferative lesions occurring in multinodular thyroids and to assess the subcellular phenotype of Δ133p53 distribution in follicular lesions.
We examined 38 thyroid glands showing a goitrous appearance associated with one single lesion in 12 cases and with two in the remaining 26 cases. By immunohistochemistry and transmission electron microscopy (TEM) a total number of 102 lesions was analyzed, including 38 nodular goiters (NG) of which 20 colloid and 18 parenchimatous types, 52 follicular adenomas (FA) and 12 Hashimoto thyroditis-associated oncocytic hyperplasias (OHHT). FA were classified in normo-follicular (NF-FA, n=10), macro-follicular (MaF-FA, n=9), micro-follicular (MiF-FA, n=28) and solid (S-FA, n=5) variants.
50% of multinodular glands reacted to Δ133 isoforms. Colloid and parenchimatous NG expressed Δ133 isoforms in 60% and 56% of cases, respectively. Reactive NG showed increased irregularity of nuclear membrane, dispersed chromatin, increased amount of cytoplasmic organelles and rough endoplasmic reticulum, at TEM. Cell basal borders were infolded. Δ133 isoforms were found in 50% NF-FA, 33,4% MaF-FA, 57,1% MiF-FA and 60% S-FA. All the reactive FA - but N-FA - showed irregular nuclear membrane. Cromatin was dispersed in all cases. Subcellular organelles and RER were increased in all cases but N-FAs. Cell basal borders were infolded in 50% of reactive FA. 42% of OOHT expressed Δ133 isoforms. The ultrastructural phenotype was quite similarly to FA.
Immonodistributions of Δ133p53 isoforms in NG, FA and OHHT suggests a role in these lesions. Ultrastructural findings indicate that Δ133p53 immunoexpressions may be associated with proliferate changes.
Withdrawn
Autoimmunity Saturday Poster
Patient options for primary definitive treatment of Graves' disease include radioactive iodine (RAI) and thyroidectomy, but their utilization varies. We previously reported that socioeconomic factors and clinical manifestations of disease influence whether a patient undergoes thyroidectomy or RAI for definitive treatment, and we hypothesize that thyroid-specific autoantibody levels, though useful for diagnosis, cannot help patients decide between surgery or RAI.
Retrospective review of patients treated with RAI or thyroidectomy for Graves' disease between 8/2007 and 9/2013 at our university hospital. Patients with contraindications to RAI or other indications for surgery were excluded, as were patients who previously underwent either treatment.
469 patients underwent definitive treatment for Graves' disease: 335 (71%) underwent RAI while 134 (29%) underwent surgery. The number and percent of patients who underwent surgery increased each year of the study, from 14% in the first year to 52% in the final year (p<0.01). 244 patients (52%) had thyroid perioxidase (TPO) measured prior to treatment, 208 (44%) had thyroglobulin (TgAb), and 212 (45%) had either thyroid stimulating immunoglobulin (TSIg) or thyrotropin receptor antibody (TRAb) measured. Patients who underwent surgery were more likely to have measurements of any of the antibodies than those who underwent RAI (p<0.01). Patients with a positive TSIg or TRAb were more likely to have eye disease (40% vs 25%, p=0.04), and patients with positive TgAb were more likely to have goiter (70% vs. 55%, p=0.03) on bivariate analysis. On multivariate analysis, however, antibody positivity did not predict ophthalmopathy or goiter.
Total thyroidectomy is being offered to patients as initial treatment for Graves' disease with increasing frequency in recent years. Clinical features such as ophthalmopathy or compressive goiter are often the driving factors behind patients' treatment choices, and measurement of thyroid-specific autoantibodies does not appear to be predictive of these clinical features.
Autoimmunity Saturday Poster Clinical
Euthyroid Graves' disease (EGD) is a rare condition that is characterized by thyroid-associated ophthalmopathy (TAO) in the absence of thyroid dysfunction. Some reports have suggested a correlation between the presence of thyrotropin receptor antibodies and TAO, but the long-term course of EGD itself is still unknown. The aim of this retrospective review was to determine the long-term course of thyroid function and TAO in patients diagnosed with EGD.
We selected the patients diagnosed with EGD on initial presentation between March 1987 and July 2013 as subjects of this study and reviewed their medical records, thyroid function, TRAb values, and ophthalmic symptoms. Their eyes were examined by ophthalmologists.
Eighty-five patients had been diagnosed with EGD. Twelve of the 85 patients (14.1%, 9 female and 3 male) subsequently developed hyperthyroidism, and 2(2.4%, both female) of the 85 patients subsequently developed hypothyroidism, while 68 patients of the 85 patients (80.0%, 56 female and 6 male) remained euthyroid throughout the follow-up period (mean 3.9 years, range 0.1–25.7 years). Eighteen of the 85 patients had been followed up for more than 5 years, and 17 of them remained euthyroid, but the other patient had developed subclinical hypothyroidism by the time of their most recent examination. According to the ophthalmic medical records, 35.7% of the patients had received ophthalmic treatment, including radiation therapy, surgery, and local injection of triamcinolone or botulinum toxin type A. There were no significant changes in the ophthalmic symptoms of the patients who did not receive ophthalmic treatment.
There was no significant deterioration in either the thyroid function or ophthalmic symptoms of the subjects of this review who had been followed up for more than 5 years. The results suggested that TRAb and TSAb may be related to the development of EGD, but not to the long-term course of EGD.
Autoimmunity Saturday Poster Clinical
The association between Hashimoto's Thyroiditis (HT) and Well-Differentiated Thyroid Carcinoma (WDTC) has been a subject of long and ongoing debate. As the incidence of HT is increased in WDTC patients, the histopathologic evaluation of surgical specimens from these patients are required.
Objectives: To determine the frequency and degree of severity of HT in patients with WDTC and managed with total thyroidectomy. Materials and methods: We analyzed 70 cases with WDTC based on diagnostic criterion described in the literature; we also evaluated the presence of HT based on universals diagnostic standards. The histological criteria for diagnostic and severity of HT were: I. Degree of lymphoid follicle formation: 0. No formation, 1. Rare, 2. Occasional, 3. Frequent. II. Stromal fibrosis: 0. No fibrosis, 1. Less than 1/3 of the thyroid stroma, 2. Fibrosis between 1/3 and 1/2 of the tissue, 3. More than 1/2 of the parenchyma were replaced for fibrotic tissue. III. Follicular size: 1. Macrofollicular: >500 μm, 2. Normofollicular: 200–400 μm, 3. Microfollicular: <100 μm. IV. Follicular degeneration: 0. No degeneration, 1. Mild or <33% of the tissue, 2. Moderate or 33–50%, 3. Severe or >50%. V. Degree of lymphoplasmacytic infiltration: 0. No infiltration, 1. Mild or <5 hpf, 2. Moderate or >5 hpf, 3. Severe or >10 hpf. We obtain the degree of severity of HT as follows: Severe: Score 10 to 15, Moderate: Score 7 to 9, Mild: Score ≤6.
49 patients (70%) had WDTC, but no HT, the remaining 21 cases (30%) were diagnosed with WDTC and HT, its distribution was: a. Score 10–15: Severe Thyroiditis: 7 cases. b. Score 7 to 9: Moderate Thyroiditis: 10 cases. c. Score <6: Mild Thyroiditis: 4 cases.
The frequency of HT in WDTC in this series is high, with a severity score ≥7 in more of 80% of the cases. As the incidence of HT is increased in WDTC patients, histopathological analysis meticulous surgical specimens from these patients are required.
Thyroid & Development Saturday Poster
Ectopic thyroid tissue is usually found anywhere along the embryonic descent pathway of the medial thyroid anlage from the tongue to the trachea. However, ectopic thyroid tissue in the adrenal gland (ETTAG) is not easy to understand on the basis of thyroid embryology; because it is so rare, the possibility of metastasis should first be considered. ETTAG is a rare finding, with only seven cases reported on literature; women are much more frequently affected than men, and it usually presents in the fifth decade.
We described two cases of ETTAG presented as incidental cystic adrenal masses in adult females.
Two cases of ETTAG presented as incidental cystic adrenal masses incidentally discovered on abdominal ultrasonography and/or in computed tomography images in adult females, one having a congenital hernia of Morgagni. The ETTAG was histologically indistinguishable from normal orthotopic thyroid tissue, and its follicular nature was confirmed by immunohistochemical positivity for thyroglobulin (Tg), thyroperoxidase (TPO), thyroid transcription factor-1 (TTF-1/Titf-1/Nkx2.1), cytokeratin AE1/AE3, cytokeratin 7, pendrin, human sodium iodide symporter (NIS), paired box gene 8, and forkhead box E1 (TTF-2), as well as positivity for the messenger RNA of the thyroglobulin gene by in situ hybridization analysis. No C cells (negativity for calcitonin, chromogranin, and synaptophysin) were present. Neither BRAF nor KRAS mutations were detected with real-time polymerase chain reaction analysis. Further work-up did not show evidence of thyroid malignancy.
In our two patients, ETTAG is composed of normal follicular cells without C cells. The expression of some transcription factors (TTF-1, paired box gene 8, and FOXE1) involved in development and/or migration of the medial thyroid anlage is preserved. Although ETTAG pathogenesis remains unknown, the lack of C cells together with the coexistence of a congenital defect of the anterior diaphragm (hernia of Morgagni) in one of our patients could suggest an overdescent of medial thyroid anlage-derived cells in the origin of this heterotopia.
Thyroid Nodules & Goiter Saturday Poster Clinical
Thyroid Nodules (TN) in children are less prevalent, but may have a greater risk of malignancy than in adults. The prevalence of palpable TN in childhood being about 1,5%. In children, 26% of TN is malignant, most are asymptomatic because they are associated with normal thyroid function. Risk factors for developing TN in children are female sex, post-pubertal age, previous or co-existing thyroid disease, previous irradiation of the neck, and a family history of thyroid disease.
Objectives: To analyze the cytological characteristics of fine-needle aspiration biopsy (FNAB) of 41 children diagnosed with TN, and the prevalence of autoantibodies to thyroid peroxidase (TPOAb) and thyroglobulin (TgAb) in this patients. Between 2008 and 2012 we evaluated 41 children with TN (F/M: 33/8; age: 8–12 years) of an initial group of 126 with diagnosis of thyromegaly, to which was performed thyroid ultrasonography, TSH/FT4, TPOAb and TgAb levels. The FNAB was performed in all 41 patients and was guided by ultrasonography (US).
Thirty-tree patients were females (80,48%). Overall they had mean age of 10,17±1,8 years (8–12 years). Thyroid function was normal in 31 females (93,93%) and in 7 males (87,5%), with remaining having subclinic hypothyroidism. Mean TSH was 3,01±0,8 mIU/mL (normal value: 0,4–4,0), FT4 was 0,97±0,12 ng/dL (normal value: 0,7–1,48). TPOAb was positive -mean: 64,7 IU/mL- (normal value: <35 IU/mL) in 20 females (60,6%) and in 6 males (75%) -mean: 57,9 IU/mL-. TgAb was positive -mean 7,9 IU/mL (normal value: 0–4,0 IU/mL)- in 21 females (63,63%) and in 5 males (62,5%) -mean 8,8 IU/mL. 54,54% of females and 50% of males were positive both TPOAb and TgAb. FNA revealed findings consistent with lymphocytic thyroiditis in 31 females (91,93%) and 7 males (87,5%), papillary carcinoma (follicular variant) in 1 female (3,03%) and follicular lesion of undetermined significance in 1 male (12,5%), but in the latter case, histology was reported “goiter.”
The prevalence of thyroid autoimmunity is high in TN of children with normal thyroid function; moreover, the prevalence of malignancy in our sample was low that reported in others studies.
Autoimmunity Saturday Poster Clinical
Addison's disease is a rare and potentially lethal disease if untreated. Autoimmune Addison's disease (AAD) is the main reason of primary adrenal failure. More than a half of patients display additional autoimmune conditions, such as Hashimoto's thyroiditis, which represent a considerable clinical concern.
In this study we describe a 23-year-old patient who presents to the hospital with severe abdominal pain, weakness, adynamia, pigmentation of skin, especially in skin creases and in areas subject to friction, anorexia, confusion, weight loss, salt craving. Patient with severe abdominal pain transferred to the surgical clinic. There during investigations hyponatremia, hyperkalemia, hypotonia (BP 70/45 mmHG) and hypoglycemia (30 mg%) were revealed. Abdominal ultrasound did not reveal any abnormalities. Cortisol and ACTH levels were checked and the patient was transferred to the department of Endocrinology with the diagnosis of Adrenal crisis.
Laboratory findings revealed: hyponatriemia (133 mmol/l), hyperkalemia (6,0 mmol/l), hypoglycemia (30 mg/dl, 66 mg/dl), low cortisol level - 0,1 mg/dl /N 3.7–19,4/, high ACTH level->1250.0 pg/ml /N till 46/. ACTH stimulation test was also performed: serum cortisol levels fail to rise after ACTH administration. Thyroid function tests revealed autoimmune thyroiditis with hypothyroidism: TSH 10,30 IU/ml, fT4 0,8 ng/dl, anti-thyroid peroxidase (anti-TPO) antibodies were elevated 200 IU/ml. The patient was treated with intravenous Hydrocortisone, later Hydrocortisone tablets, intravenous fluids, Fludrocortisone (Florinef) tablets, intravenous glucose, Euthyrox 50 mcg/day. It was mentioned improvement of both clinical signs and laboratory datas after treatment. She was discharged from the hospital with Hydrocortisone 20 mg 1-1/2-0 Tbl., Euthyrox 50 mcg/day prescription and with later regular follow-up.
Current study confirms particular tendency of AAD patients to develop other autoimmune disorders in a pattern of autoimmune polyglandular syndrome. Active search for concomitant conditions is warranted to prevent serious complications.
Autoimmunity Saturday Poster Translational
Graves' ophthalmopathy (GO) is one of the major clinical issues that remain unresolved. Antibodies against thyrotropin receptor (TSHR) may play important roles in pathogenesis of GO. However, additional mechanism should be involved in the inflammation and extracellular matrix deposition of affected tissues. In these respect we investigated the effects of IGF-I and IGF1 receptor (R) kinase inhibitors on cytokine production stimulated LPS and cyclic AMP analogue using GO fibroblasts in order to establish a new therapeutic strategy.
IGF-1 receptor kinase inhibitor, PQ401, and human IGF-1 were obtained from Sigma Aldrich. Orbital tissues were obtained as surgical waste during decompression surgery for Graves' ophthalmopathy conducted in Olympia Eye Hospital. The establishment of cell culture was carried out by a standard method. Cell proliferation was measured by MTS method. IL-6 secretion and mRNA were estimated by ELIA and RT-PCR using commercial kits.
IGF-1 potentiated 8-bromo-cAMP stimulated cell proliferation estimated by MTS assay. IGF-I also potentiated 8-bromo-cAMP stimulated IL-6 mRNA expression and IL-6 secretion. LPS also stimulated IL-6 secretion and both IGF-I and 8-bromo-cAMP also potentiated IL-6 secretion stimulated by LPS. These observations suggested that IGF-I R signaling is interacting not only with cAMP signaling but also with LPS induced cytokine production by innate immune system. Then we investigated the effects of IGF-I receptor kinase inhibitor, PQ401. It inhibited IL-6 secretion stimulated by both 8-bromo-cAMP and LPS. It suppressed proliferation of cells in basal conditions and in cells treated with IGF-I.
The observations suggested that inhibition of IGF-I R system in affected tissues can be a potential therapeutic strategy for GO.
Disorders of Thyroid Function Saturday Poster Basic
Selenium (Se), which has an antioxidant feature and contributes to protein and DNA synthesis, is an essential mineral for a healthy life. There are various studies demonstrating its positive effects in prostate, lung, colorectal, bladder and thyroid cancers, strengthening the immune system and also ensure the well-functioning of thyroid gland. In this study, we aimed to investigate 24 hours urinary Se levels in healthy women.
Istanbul (Iodine sufficient) and Kayseri (Iodine insufficient) were chosen in order to reflect different iodine (I) intake regions in Turkey based on our previous published data. Urine samples (24 h) were taken from 141 healthy women aged 17–62, who were not pregnant or lactating. Participants were randomly selected from Acibadem Hospitals in Istanbul (n=49) and from Erciyes University Hospital in Kayseri (n=92). Volunteers are selected by age, body-mass index, smoking status, history of diabetes, thyroid history, use of iodized salt with a questionnaire. Se levels in urine samples were analyzed by a selective and sensitive method ICP-MS (inductively coupled plasma-mass spectrometry).
Urinary Se levels were found below normal reference intervals in both cities. Se values compared in Kayseri (10,9[5,3–17,6]ppb) and Istanbul (12,7 [7,8–18,4] ppb) were not statistically significant (U=1921; p=0,15). A weak negative correlation was determined between age and Se values (spermanr=−0, 19; p=0.02). There was no correlation between body mass index (BMI) and Se values (p=0,17). When age groups (17–25; 26–35; 36–45; 46–62) were compared, Se values in age group of 17–25 (16,44±1,76) was significantly higher than in 36–45 (10,95±1,11; t=2,956; p=0,03) (Figure). There was no difference in Se values when smoking habits were compared (p=0,84).
Se levels (ppb) and age histogram (on the left); Se values (ppb) based on age groups (17–25; 26–35; 36–45; 46–62). Se levels significantly lower in 36–45 group compared to 17–25.
Data is shown as mean±SEM.
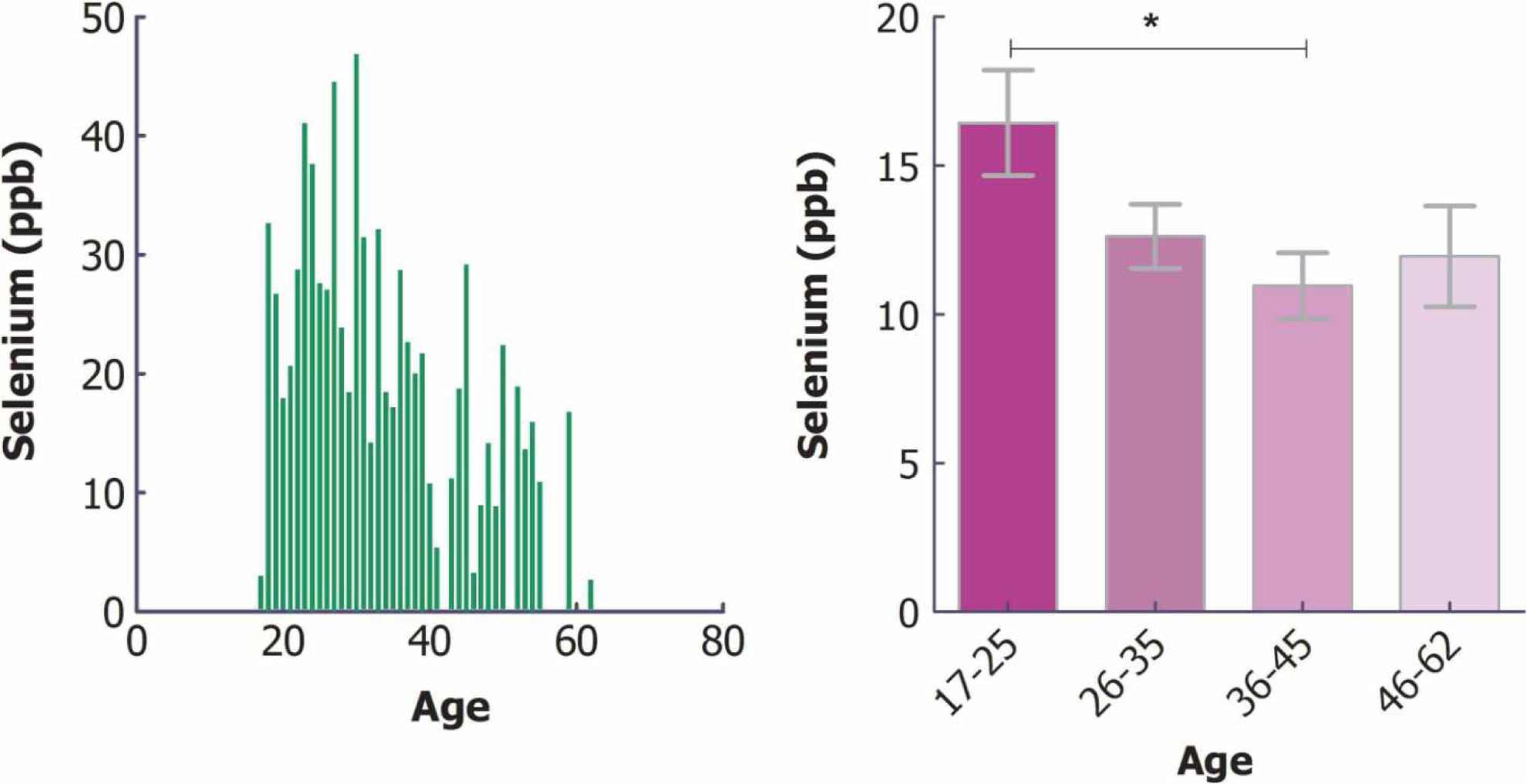
Since close relation between I and Se is known, in Turkey as a moderate I insufficient country, women seems to have also Se deficiency, concomitant treatment of deficiencies in I and Se should be considered in Turkish women.
Disorders of Thyroid Function Saturday Poster
Primary Congenital Hypothyroidism (PCH) affects 1 in 2,000 live births in California and Hawaii. Without early detection and ongoing treatment, PCH can cause severe developmental delay. We assessed the diagnostic procedures, management patterns, and developmental outcomes of patients with PCH in California and Hawaii.
We conducted a cross-sectional survey among 770 primary care providers (PCPs) who were listed as contact doctor of ≥1 confirmed PCH patient identified through the Newborn Screening Programs (NBSP) in California (n=748) and Hawaii (n=22) between 2009–2013. We collected data on diagnostics, clinical management, and developmental outcomes for patients with PCH. We restricted analysis to patients identified through NBSP.
Two hundred and six (27%) PCPs completed the survey, 79% of which reported currently having ≥1 patient with PCH. Of these PCPs, 17% reported taking primary responsibility for their patients' PCH management; 63% were involved, but not taking primary responsibility and 19% were not involved at all. PCPs provided clinical information on 125 patients, 117 of whom were identified through NBSP (39% male and 61% female; 39% Hispanic, 20% White, 22% Asian, 2% Black, 16% mixed race/ethnicity or other). Median age of starting levothyroxine treatment was 7 days (range: 2–28). Median dose at treatment initiation was 37.5 ug/day (range: 25–50). During diagnosis and follow-up, 43% of patients had hearing tests, 23% had thyroid scans, 37% had TSH receptor antibody testing, 24% had thyroid ultrasounds, and 11% had X-rays of the knees for bone age. About 80% of patients received developmental evaluations during each of the first 4 years of life. Of these (patients with Down syndrome or preterm birth were excluded), 21% had developmental delays including cognitive/mental (8%), language (20%), gross (8%) and fine (3%) motor skills delays.
The majority of patients with PCH identified through NBSP are diagnosed and treated in a timely manner. Use of thyroid scan and ultrasound was low. Most patients are co-managed by both PCPs and endocrinologists. Developmental delay is common in the first 4 years of life.
Disorders of Thyroid Function Saturday Poster Clinical
Thyroid storm (TS) is a syndrome of decompensated thyrotoxicosis requiring prompt therapy. Even with optimal therapy, mortality is 10% or more. Because of its rarity, diagnostic and prognostic aspects of TS remain incompletely understood. Identifying independent predictors of diagnosis and outcome could improve the clinical assessment and treatment of TS.
Retrospective cohort study of patients admitted to Los Angeles County Hospital with TSH<0.01 mIU/L from 2008–2014. Data collected included demographics, clinical findings, laboratory data, and outcomes [hospital and ICU length of stay (LOS), intubation, ventilator days, and mortality]. TS patients were compared to patients without TS, defined as compensated thyrotoxicosis (CT), and retrospectively stratified by Burch-Wartofsky score (BWS).
There were 25 TS and 125 CT patients identified and analyzed. The diagnosis of TS was made clinically and 24/25 TS patients received thionamides, beta-blockade, steroids, and SSKI within 24 hr of diagnosis; CT patients received thionamides and beta-blockade alone. Of CT patients, 24 had BWS>45, 50 had BWS 25–44, and 51 had BWS<25. No TS patient had a BWS<25. In the acute hospital setting, fever (>100.4°F), heart rate (>100 bpm), altered mentation, and precipitating event distinguished TS from CT (p<0.05 for all); altered mentation was the sole distinguisher for TS versus CT patients with BWS>45 (p<0.001). Regression analysis also identified CHF and elevated serum AST as independent predictors of TS. TS patients had significantly higher in-patient mortality, rate of ICU admission, and longer hospital and ICU LOS than CT patients or the subset of CT patients with BWS>45. For TS and CT patients, BWS correlated directly with hospital LOS and ICU LOS. Multiple regression analysis identified fever and atrial fibrillation as independent predictors of longer hospital LOS and ICU LOS in TS patients.
In acutely hospitalized, thyrotoxic patients, the presence of fever, tachycardia, altered mentation, and a precipitating event predicted the clinical diagnosis of thyroid storm and identified those with poor hospital outcomes who may require the most aggressive therapy.
Withdrawn
Disorders of Thyroid Function Saturday Poster Clinical
In the treatment of Graves' disease in pregnancy, MMI is usually used as the first-line drug after the critical period of organogenesis on the basis of the report of severe liver dysfunction due to propylthiouracil. From the standpoint of brain development, it has been recommended to maintain maternal fT4 in a mildly thyrotoxic range (at or slightly above normal for non-pregnant women) to avoid low fT4 in the fetus, which is based on the close relationship between maternal and fetal fT4. In this situation, maternal fT3 is frequently high predominantly, which may affect pregnancy outcomes. On the other hand, mild intrauterine hypothyroidism may not have adverse effect on brain development as long as mothers are euthyroid during pregnancy and neonates recover from hypothyroidism within a short time, as it is shown in sporadic congenital hypothyroidism. In order to investigate preferable treatment, we studied maternal and fetal thyroid status at term in women with Graves' disease who continued MMI through delivery taking fT3 into account.
Thyroid function was examined using maternal and cord blood at term. Excluding two women with low fT4, 148 women were classified into 3 groups: 58 with fT4 normal for women at term (0.60–1.20 ng/dL) (Group 1), 69 with fT4 above normal for women at term but below the upper limit of non-pregnant subjects (1.21–1.90 ng/dL) (Group 2) and 21 with fT4 above the upper limit of non-pregnant subjects (>1.91 ng/dL) (Group 3).
There was a close correlation between maternal fT4 and cord fT4 or cord TSH, and low cord fT4 was not seen only in Group 3. In Group 1, 2 and 3, maternal fT3 was above normal in 33, 77 and 100% respectively. While maternal fT4 was not correlated with cord fT3, correlation of maternal fT3 with cord fT3 was statistically significant, and cord fT3 was above normal in 38, 45 and 57%, respectively.
Normal maternal fT4 may be preferable to mildly high maternal fT4 both for the mother and the fetus. Studies on the effects of high fT3 in the fetus as well as thyrotoxic state in the mother during antithyroid drug therapy are necessary.
Disorders of Thyroid Function Saturday Poster Clinical
Well recognized risk factors for stroke include age, hypertension, renal disease and diabetes mellitus. Our prior studies show strong correlation of stroke risk and a corrected cerebral flow reserve index (FRi). The contribution of thyroid disease to stroke risk has been less studied.
Patients from a single endocrinology practice had cognitive complaints evaluated with cortical metabolic indices (CMi) derived from basal SPECT or FDG PET. Perfusion-stimulated SPECT determined cortical perfusion indices (CPi) and FRi=CPi - CMi. Statistical and graphical analysis used Excel 2013. Thyroid patients were treated and clinically euthyroid when scanned.
Among 201 thyroid patients, 18.4% (37/201) had history of hyperthyroidism and 81.6% (164/201) had other thyroid diseases. The regression line relating stroke prevalence, SP, to FRi for patients age 53 +− 14 with stroke risk factors was: SP=16.2 – 1.79(FRi) with r=0.96. Thyroid patients, age 48 +− 12 years, had SP of 8.1% (6/74) slightly less than predicted for their FRi 2.7 +− 5.5, but greater than SP of 1.8% (1/56) for 56 near normal patients age 55 +− 14 years. To study the effect of thyroid disease and other risk factors, additional plots included patients with both thyroid disease and other risk factors. Stroke risk among thyroid patients was approximately linear for more common combinations such as thyroid disease and hypertensive diabetes, with SP 22.2% (10/45), nearly equal to the sum of SP of 8.1% (6/74) for younger thyroid patients and SP of 14.4% (37/256) for hypertensive diabetics alone. Older thyroid patients, age 65 +− 16 years, including more with atrial fibrillation or other heart disease, had higher SP of 39.1% (18/46).
Thus, particularly when thyroid disease is combined with other stroke risk factors, stroke prevalence among thyroid patients with cognitive complaints is significant and higher than commonly appreciated.
Disorders of Thyroid Function Saturday Poster Clinical
Acute short-term hypothyroidism induced by thyroid hormone withdrawal (THW) could impact patient's life physically or psychologically. The aim of the study was to quantify deterioration in physical or mental health and to look at changes in brain function by resting functional magnetic resonance imaging (fMRI).
We recruited 62 DTC patients who are scheduled for surveillance of disease after THW. Patients visited before THW and two-week period of THW. Patients completed three forms of questionnaires (Short Form 12 Health Survey (SF-12), Symptom Checklist-90-Revision (SCL-90-R), Patient Health Questionnaire-9 (PHQ-9)). Twenty patients performed resting fMRI and 10 patients performed cognitive test (Cambridge Neuropsychological Test Automated Battery (“CANTAB”)). We compared the intrapersonal changes of these measurements before and after THW.
In SF-12, mental component summary (p=0.003) and its four subdomains (role functioning (emotional), vitality, mental health, and social functioning) were worsened. But, physical component summary and its four subdomains (general health, physical functioning, role functioning (physical), bodily pain) did not change. In SCL-90-R, total score increased (p=0.003). In subdomain analysis, parameters for obsession-compulsion, depression, anxiety, and hostility increased significantly, but those for somatization, interpersonal sensitivity, phobic anxiety, paranoid and psychosis did not change. In PHQ-9, the proportion of subjects who showed over 10 points suggesting moderate depression increased (p=0.047). “CANTAB” results did not show any differences. fMRI showed any significant change in basal activities across whole brain. Functional connectivity which was evaluated among 264 regions of interest (ROI)'s by analyzing the correlation of time-dependent changes in activity between two points tended to increase after THW.
Acute short-term hypothyroidism significantly deteriorated mental health and increased proportion of patients with moderate depression. THW does not alter resting cortical activities across whole brain but appears to increase the functional brain network and may contribute to psychopathological changes associated with alterations in thyroid function.
Disorders of Thyroid Function Saturday Poster Clinical
The relationship between subclinical hypothyroidism and increased mortality in elderly adults is controversial. We investigated the association of thyroid function and 6-year mortality in the elderly population living in a iodine sufficient area.
This study was conducted as a part of the KLoSHA study, which was designed as a population-based prospective cohort study on health, aging, and common geriatric diseases in Korean elders aged 65 years and older. A total of 917 participants aged 65 and older (male to female ratio, 415/502) with euthyroid or subclinical hypothyroid status were analyzed in the present study. Metabolic parameters including plasma thyrotropin and free thyroxine concentrations and demographic features were evaluated in the participants. Cox proportional hazards models adjusted for confounders were used in the analysis.
At baseline evaluation, 769 subjects (male to female ratio. 345/424) showed normal thyroid function, and 148 subjects (male to female ratio, 70/78) had subclinical hypothyroidism. During a median of 6.7 years of follow-up, 202 deaths occurred (22.0%), 50 (24.8%) of which were from cardiovascular causes. Cox regression analysis revealed no significant association between subclinical hypothyroidism and all-cause and cardiovascular mortality after adjusting age, sex, body mass index (BMI), and cumulative illness. In euthyroid subjects, free T4 and TSH were not associated with all-cause and cardiovascular mortality. In this cohort, age and sex were associated with all-cause and cardiovascular mortality.
Subclinical hypothyroidism was not associated with mortality in the elderly population living in a iodine sufficient area.
Disorders of Thyroid Function Saturday Poster Clinical
We have previously reported that tyrosine kinase inhibitor (TKI) therapy, specifically axitinib, can cause inappropriate elevations in TSH relative to thyroid hormone levels (Ohba, et al., Thyroid, 2013). Similar results are reported in patients with a macro thyrotropin-IgG complex (macro-TSH), or coexistent reduced sensitivity to thyroid hormone and Hashimoto's thyroiditis (RSTH+HT). Currently, little is known about the range of inappropriate TSH elevation. To define its tentative range, we analyzed the TSH:FT4 relationship in patients with thyroid disorders.
We abstracted a total of 48,126 concurrent TSH and FT4 results, determined by chemiluminescent immunoassays (Abbott Japan Co.), from patients who presented to Kuma Hospital in December 2012. Reference ranges of log-transferred TSH (log TSH) against each FT4 concentration were calculated, and compared to TSH and FT4 levels obtained from recent case reports describing macro-TSH or RSTH+HT. A MEDLINE search revealed 10 cases of macro-TSH and 3 cases of RSTH+HT. We also analyzed 4 cases of axitinib-induced thyroid dysfunction and 1 case of macro-TSH diagnosed at Hamamatsu University School of Medicine.
Reference ranges of log TSH levels against each FT4 were established from the 2.5th to 97.5th percentile of the measurements, because the distribution of log TSH was non-Gaussian. The area above the 97.5th percentiles was tentatively defined as the range of inappropriate TSH elevation as shown in the Figure. Thyroid function tests obtained from 17 out of 18 reported cases of macro-TSH (10), RSTH+HT (3), and axitinib-induced thyroid dysfunction (4) were included in the proposed range. This tentative range also included most area of inappropriate secretion of TSH where FT4 is elevated with non-suppressed TSH (shaded region in the Figure). We also calculated the medians of log TSH values, which were not log-linear but resembled 2 negative sigmoid curves in agreement with a recent study (Hadlow, et al., J Clin Endocrinol Metab, 2013).
Inappropriate TSH elevation was tentatively defined as the area above the 97.5th percentile of log TSH against each FT4 level.
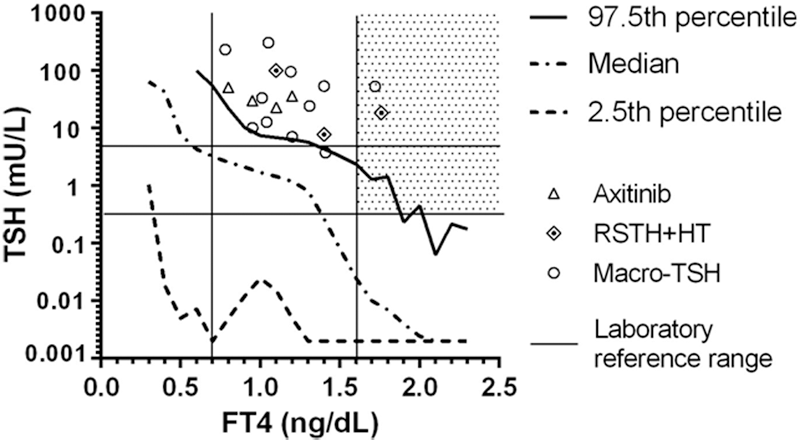
We tentatively define the range for inappropriate TSH elevation, which may contribute to the different diagnosis of thyroid disorders.
Withdrawn
Iodine Uptake & Metabolism Saturday Poster Clinical
Iodinated contrast media (ICM) for CT scans contain many thousand times the recommended daily iodine allowance. This prospective study assessed the effects of ICM on urinary iodine concentrations (UIC) and thyroid function in healthy adults.
Spot UIC and serum thyroid function tests were obtained in adults ≥18 yrs following an ICM dose weekly for at least 4 weeks, until normal levels were achieved. Subjects with ICM use ≤6 months, self-reported thyroid dysfunction, thyroid hormone or anti-thyroid medication use, amiodarone use ≤2 years, lithium use ≤6 months, pregnancy, or lactation were excluded. Ultrasound was performed to detect thyroid nodules. Multivariable regression models assessed associations between covariates and peak UIC, time for UIC to peak and normalize, and thyroid dysfunction risk.
53 subjects (age 50.8±12.4 [mean±SD] yrs, 58% men, 47% White, 77% U.S.-born, 45% smokers, 1 with positive TPO Ab) were studied. 15% had a thyroid nodule >1 cm. Administered iodine in ICM was 34.5±6.1 g (mean±SD). Baseline median (range) UIC was 105.6 (17–866.1) μg/L and TSH was 1.43 (0.28–29.14) mIU/L. Mean±SD time to achieve peak UIC [median (range): 3,430 (233–157,500) μg/L] was 1.1±0.5 weeks. Mean±SD time for UIC to normalize (within 1.5 times baseline level or <NHANES median of 164 μg/L) was 5.2±4.0 weeks. 13 subjects had abnormal baseline TSH (range: 0.3–29.1 mIU/L; 1 hyperthyroidism and 12 hypothyroidism); of the remaining subjects, 6 (15%) developed an abnormal TSH within 1–3 weeks (range 0.05–5.6 mIU/L; 1 hyperthyroidism and 5 hypothyroidism). ICM iodine content predicted peak UIC (p<0.01). Age, sex, race, smoking status, family history of thyroid disease, personal or family history of autoimmunity, thyroid volume, presence of thyroid nodules >1 cm, ICM iodine content, baseline UIC, and baseline serum TSH were not predictive of times to achieve peak and normalized UIC, or thyroid dysfunction risk.
Peak UIC occurred at 1.1 weeks and normalized by 5.2 weeks in healthy adults who received ICM. As thyroid dysfunction developed in 15% following a single ICM dose, monitoring of thyroid function should be considered in at-risk patients.
Thyroid Cancer Saturday Poster Basic
Notch1 is a trans-membrane receptor which aids in the determination of thyroid cell fate. Recently, we have found that patients with lower Notch1 expression in their thyroid cancer tissue have a significantly higher recurrence rate. However, little is known about the possible underlying mechanisms. The purpose of this study was to investigate the biological function of Notch1 in metastatic thyroid cancer and the potential downstream effector(s).
A doxycycline-inducible system for Notch1 intracellular domain (NICD) was established in a metastatic thyroid cancer cell line FTC 236 (FTC-N1 cells) to characterize the effects by gain-of-function assays both in vitro and in vivo. The potential downstream effectors were first screened by DNA microarray and the most significant one was further validated in multiple cell lines by loss-of-function assays.
Induction of NICD in FTC-N1 cells significantly decreased cell migration observed by Boyden chamber assay (35 cells/field vs. 86 cells/field in control, p<0.01). Using an in vivo orthotopic thyroid cancer model, the growth of the primary thyroid tumor was reduced by 73% with NICD induction (p=0.012). Impressively, lung metastasis developed in 80% of tumors without NICD induction compared to only 20% in the NICD-induction group (p=0.007). Among the top 50 most significant sequences from the microarrays, 8 hits represented the same gene: Serpine1. Induction of NICD reduced both mRNA and protein levels of Serpine1 in a dose-dependent manner while withdraw of doxycycline treatment in FTC-N1 cells resulted in reduced expression of NICD back to minimal level and restoration of a relative higher level of Serpine1. Inverse correlation between basal expression of NICD and Serpine1 was observed in five representative thyroid cancer cell lines including papillary, follicular and anaplastic lines. Serpine1 was then knocked down using specific siRNA. Significantly less migrated cells were observed with the Serpine1 siRNA transfected thyroid cancer cells compared with those only with control siRNA.
Induction of NICD inhibits thyroid cancer cell migration and tumor metastases, which may be mediated by down-regulation of Serpine1.
Thyroid Cancer Saturday Poster Basic
The thyroid transcription factor Forkhead Box E1 (FOXE1) is part of a network of factors that help maintain thyroid differentiation via transcriptional regulation of thyroid specific genes including thyroglobulin and thyroid peroxidase. Germline inactivating mutations in the DNA-binding or forkhead domain (FHD) of FOXE1 result in Bamforth syndrome, characterised by thyroid agenesis, cleft palate and choanal atresia. Population-based studies have demonstrated an association of single nucleotide polymorphisms close to FOXE1 with thyroid cancer. The objective of the study was to identify novel mutations in FOXE1 in papillary thyroid cancer (PTC) and to assess the effect of these mutations on protein expression and transcriptional function on FOXE1 responsive promoters.
The coding region of FOXE1 was sequenced in 120 patients with PTC and 110 patients with multinodular goitre (MNG). In vitro studies were performed to examine the protein expression and transcriptional function of wild-type and mutant FOXE1. A molecular model of the FHD of FOXE1 was generated using the SWISS-MODEL online server with the three-dimensional structure of FOXD3 as a template.
Three somatic missense mutations in the FHD of FOXE1 were detected in PTC resulting in the following amino acid substitutions: P54Q, K95Q and L112F. One additional mutation was detected in MNG: G140R. Two of the PTC were clinically recurrent tumours also positive for BRAFV600E mutation while one was a BRAF mutation-negative microPTC. In vitro studies demonstrated significant impairment in transcriptional activation by all four FOXE1 mutants which was not due to differences in protein expression. Molecular modelling localised three of the mutations to highly conserved regions of the FHD.
We have identified novel somatic mutations of FOXE1 in PTC. Mutational inactivation of FOXE1 is an uncommon event in thyroid tumours but may contribute to thyroid carcinogenesis and dedifferentiation in concert with other oncogenic drivers.
Thyroid Cancer Saturday Poster Basic
Anaplastic Thyroid Cancer (ATC) is one of the most lethal malignancy with very short survival and extremely poor treatment outcome, and the mean survival is approximately 6 months. The most effective therapy for ATC is multimodal treatment protocol that include surgery, chemotherapy (in particular doxorubicin and cisplatin), and hyperfractionated accelerated external beam radiotherapy, with a median patient survival of 10 months. Testing the sensitivity of “primary anaplastic thyroid cancer cells” (pATC) obtained from each subject, to different drugs, could determinate an increase in the effectiveness of the treatment avoiding the administration of inactive therapeutics.
In this study we tested the in vitro antineoplastic effect of two new “pyrazolo[3,4-d]pyrimidine” compounds (CLM3, CLM29; 1, 10, 30, 50 μM) in pATC obtained from biopsy (biop-pATC), or from fine needle aspiration (FNA-pATC) both established from 5 patients.
WST-1 assay (a 3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide, used in the MTT assay) shows a significant reduction of proliferation in FNA-pATC, or biop-pATC cells respect to the control, in particular with CLM29, and slightly with CLM3, while both compounds increased the percentage of apoptotic cells in FNA-pATC, or biop-pATC, dose-dependently. No significant differences in sensitivity to CLM29 or CLM3 between the tested ATC cells from FNA, or biopsy were demonstrated in our study.
Our results show that: 1) primary FNA-pATC cells have a sensitivity to tyrosine kinase inhibitors (TKIs) agents quite similar to that observed in primary cells from biopsy (biop-pATC), and for this reason the use of primary FNA-pATC cells for the tests can reduce the time needed for biopsy; 2) CLM29 and CLM3 reduce cell growth, increasing apoptosis in ATC; 3) the possibility to test sensitivity to different TKIs in each patient is able to increase the efficacy of treatments, avoiding the administration of ineffective drugs.
Thyroid Hormone Metabolism & Regulation Saturday Poster Clinical
Lactose intolerance is associated with L-T4 malabsorption, and the need to use high L-T4 doses in the substitutional treatment of hypothyroidism.
We report reversible normalisation of serum TSH levels in four patients with Lactose intolerance who received L-T4 in tablet form after switching to an oral liquid formulation lactose free.
TSH was significantly reduced after switching (with the same dosage, 30 minutes before breakfast) from oral tablets to a liquid formulation (TSH, evaluated 1–3 months after the switch, decreased: from 7.2±3.4 to 3.1±1.9 μIU/mL, p<0.05). The switch back to tablets (with the same dosage, 30 minutes before breakfast) caused thyrotropin levels to worsen. This fact leads us to believe that absorption of thyroxine is greater with oral liquid formulations in these patients. The fact that the change from tablets to liquid oral formulation normalised serum TSH levels, and that switching back to tablets caused thyrotropin levels to worsen, leads us to believe that absorption of thyroxine is greater with oral liquid formulations in these patients.
These results suggest that the L-T4 oral liquid formulation could circumvent malabsorption in patients with lactose intolerance.
Thyroid Cancer Saturday Poster Basic
Scent detection by canines has been investigated in melanoma, ovarian, bladder, and colorectal cancer with promising results. In a prior study, we showed that canines imprinted on conventional papillary thyroid cancer were able to discriminate between urine samples (N=58) from subjects with metastatic (n=19) or benign disease (n=39) with a sensitivity of 97.2% and specificity of 97.3%.
In the present study, two dogs, previously trained in search and rescue for human remains detection, were imprinted with tissue, blood and urine from pathologically verified papillary thyroid cancer (conventional type). Following imprinting, discrimination training involving the random presentation of cancer and non-cancer samples was performed over a period of six months. Correct answers were rewarded with positive reinforcement. Following training, urine specimens were prospectively collected from 22 subjects presenting to our thyroid clinic with >1 thyroid nodule(s). A gloved handler, blinded to the sample status, presented the samples to each dog. The dogs' responses were relayed to the study coordinator. When correct, the dog was rewarded with verbal excitement and a high-value treat. Only samples from surgically confirmed conventional papillary thyroid cancer were included in the final data set.
Correct responses were given in 21 of 22 urine samples, resulting in a sensitivity of 90.9% and specificity of 100.0% (1 false negative).
Scent detection by trained dogs to aid in the evaluation of thyroid nodules may serve as a non-invasive adjunct to current diagnostic practices. Ongoing expansion of our dataset will determine final accuracy of these trained canines.
Thyroid Cancer Saturday Poster Basic
The HIV protease inhibitor Nelfinavir (NFV) disrupts Heat Shock Protein 90 (HSP90) activity and induces apoptosis in medullary thyroid cancer (MTC) cells. HSP90 is abundantly present in the mitochondria of tumor cells and treatment with HSP90 inhibitors affects mitochondrial morphology. Our current study sought to determine the effects of NFV on mitochondrial clients for HSP90 in MTC cells.
Two human MTC cell lines, TT and MZ-CRC-1, which harbor endogenous C634W or M918T RET mutations, respectively, were exposed to clinically achievable concentrations of NFV (5–10 microM). The mRNA levels of mitochondrial genes were examined using Mitochondrial and Mitochondrial-Energy quantitative RT-PCR arrays. The effect of NFV on mitochondrial proteins was determined by Western Blot. The mitochondrial membrane potential was measured by JC-1 staining.
NFV induced expression of genes regulating superoxide production (NADH dehydrogenases, cytochrome-c-oxidases, superoxide dismutase and uncoupling protein), increased expression of genes coding for Solute carrier family 25, and increased expression of the pro-apoptotic genes PUMA and NOXA. The mRNA level of ATP synthase (ATP5C1) was inhibited by treatment with NFV. Western blot analysis with anti-COXIV demonstrated that NFV affected electrophoretic mobility of the COXIV protein in TT cells, and increased COXIV protein level in MZ-CRC-1 cells. NFV-inducible changes in genes coding for mitochondrial respiratory chain were associated with loss of JC-1 staining indicating mitochondrial membrane depolarization in both cell lines. Induction of apoptosis was demonstrated by Western blot with anti-cleaved caspase-3 and anti-PARP in MTC cells treated with NFV (10 microM). Treatment with NFV at 5 microM affected expression of mitochondrial proteins, but did not induce caspase-3 cleavage. Time course experiments indicate that NFV-inducible mitochondrial damage preceded induction of apoptosis in MTC cells.
NFV targets mitochondria in MTC-derived cells. Mitochondrial damage is an early event in the NFV-inducible apoptotic cascade in MTC cells.
Thyroid Cancer Saturday Poster Basic
Microtubule-associated protein-2 (MAP-2) belongs to a family of proteins involved in microtubule assembly. It had been illustrated as a useful marker for neural or neuroendocrine tumor differentiation. MAP-2 is expressed in normal and neoplastic cells of neural crest origin. Medullary carcinoma of thyroid (MTC) originates from neural crest-derived parafollicular C cells, which makes MAP-2 a potential diagnostic marker for this neoplasm.
Formalin fixed paraffin embedded material of 19 MTC cases was examined by immunoperoxidase staining using MAP-2 monoclonal antibody. All the cases included both primary tumor from thyroidectomy/lobectomy specimen, and metastatic lymph nodes from neck dissection; in two cases the histological material from distant metastasis (liver and bone) was also available. A semiquantitative score was used to evaluate the percentage of positively stained cells: 0 (0–1%); 1 (1–10%); 2 (11% to 50%); 3 (above 50%).
The staining pattern for MAP-2 is cytoplasmatic. The evaluation of primary thyroid neoplasm demonstrated: score 3 (figure) in 12 cases (63.2%); score 2 in three cases (15.8%); score 1 in two cases (10.5%); score 0 in two cases (10.5%). The score in the primary tumor and the respective regional lymph node metastasis in each patient showed similar results, except of one case with a thyroid lesion score 1 and nodal metastasis score 0. Distant metastases, available in two cases, demonstrated the same result as the primary tumor and nodal metastasis (score 3). The normal thyroid tissue in all the cases showed negative stain.

1. The majority of MTCs had been shown to express MAP-2 in both primary and metastatic tumor in more than 50% of the cells. 2. MAP-2 may be used as an additional diagnostic tool for MTC, especially in the workup on MAP-2-positive metastatic tumors of unknown primary origin. 3. The presence of both MAP-2-positive and negative cases, with similar staining pattern in primary and metastatic tumor in the same patient, raises the possibility of different subsets of MTC. 4. The differences in expression of MAP-2 in MTCs might have a potential prognostic and therapeutic implication.
Thyroid Cancer Saturday Poster
The prognostic significance of various features of cervical lymph node metastases from papillary thyroid carcinoma (PTC) is gaining recognition. Recently, the risk of recurrence in patients with nodal metastases was shown be related to clinically apparent lymph node metastasis size, the number of positive nodes and the presence of extranodal extension (ENE). The College of American Pathologists recommends that the presence of ENE should be reported, but does not define criteria as clearly as in protocols for reporting metastatic head and neck squamous cell carcinoma. The degree of reliability among expert pathologists for the identification of ENE has heretofore not been evaluated.
This is an IRB-approved retrospective review of 61 permanent section slides of nodal metastases from PTC. A blinded review was performed by 7 expert pathologists. Each slide was categorized as demonstrating ENE or no evidence of ENE, and the intraclass correlation coefficient (ICC) was computed to assess consistency in ratings. The specific criteria used by each pathologist for determining the presence of minimal ETE was delineated.
The average measures ICC, representing the absolute agreement among the raters, was 0.669 with a p-value of 0.000. The closer the ICC value is to 1, the better the agreement. The criteria for minimal ETE used by each of the participating pathologists were incompletely concordant, especially regarding invasion of nerves as a criterion.
The inter-observer concordance for the identification of ENE between expert pathologists is fair. The presence of ENE could potentially be reliably used to further stratify metastatic nodal disease based on risk. However, recognition of variation in pathologic interpretation provides an impetus for the standardization of criteria of ENE to achieve greater consistency between pathologists and institutions.
Thyroid Cancer Saturday Poster Clinical
Extrathyroidal extension (ETE) is a recognized negative prognostic factor in papillary thyroid carcinoma (PTC) and is universally used to upstage thyroid cancers. The accurate determination of disease stage is important not only for selecting appropriate therapy, but also to predict outcomes, communicate between clinicians and to be able to effectively compare end results. However, the College of American Pathologists describes the definition of ETE as problematic and subjective, and the degree of reliability among expert pathologists for the identification of minimal ETE has heretofore not been evaluated.
This is an IRB-approved retrospective review of 69 representative permanent section slides of PTC tumors. A blinded review was performed by 7 expert pathologists. Each slide was categorized as demonstrating evidence of or no evidence of minimal ETE, and the intraclass correlation coefficient (ICC) was computed to assess consistency in ratings. The specific criteria used by each pathologist for determining the presence of minimal ETE was delineated.
The average measures ICC, representing the absolute agreement among the raters, was 0.492 with a p-value of 0.000. The closer the ICC value is to 1, the better the agreement. The specific criteria for minimal ETE used by each of the participating pathologists were inconsistent, especially regarding invasion of adipose tissue, nerves, vascular structures as criteria.
The importance of minimal ETE as a prognostic feature has been challenged in the literature. However it is apparent that with the moderate to poor inter-observer concordance for the identification of minimal ETE between expert pathologists, the populations of patients identified with minimal ETE is likely heterogeneous with respect to this variable. Recognition of this variation in pathologic interpretation is important for clinicians to understand when reviewing the literature related to this feature and provides an impetus for the standardization of criteria of minimal ETE to achieve greater consistency between pathologists and across institutions.
Thyroid Cancer Saturday Poster Clinical
Thyroid nodules are less common in patients ≤18 years of age. The Bethesda System for Reporting Thyroid Cytopathology allows for individual risk stratification, but a significant number of samples are classified as indeterminate. The incorporation of gene mutation panels and gene expression classifiers has led to improved pre-operative diagnosis. The aim of this study was to assess the diagnostic utility of the Asuragen miRInform® panel in the pediatric population.
Descriptive, retrospective evaluation of 114 archived FFPE samples, including; 48 benign (thyroiditis×8, autonomous nodule×6, FA×24, other×10), 6 FTCs, 20 fvPTC, 31 classic-PTC (cPTC), and 9 diffuse sclerosing variant-PTC (dsvPTC). All slides were reviewed to ensure adequacy of sample and accuracy of diagnosis.
Either a mutation or rearrangement/translocation in one of the 17 molecular markers was found in; 19/31 (61%) cPTC, 2/6 (33%) FTC, 5/20 (25%) fvPTC, and 5/9 (56%) dsvPTC. BRAF was the most common mutation in cPTC (12/31; 39%), and RET/PTC1 was the only translocation associated with dsvPTC. Mutations in RAS or PAX8/PPARγ were exclusive to FTC and fvPTC. A mutation or rearrangement was found in 21/26 samples (81%) with malignant cytology and histology. One case of follicular adenoma showed a PAX8/PPARγ rearrangement. In samples with indeterminate cytology and malignant histology, a mutation was found in 5/15 (33%) of cases. In cPTC, BRAF mutation did not predict a more invasive phenotype.
A detectable mutation or rearrangement with the Asuragen miRInform® panel is highly suggestive of differentiated thyroid cancer. The panel confirmed the role of RAS in FTC tumorigenesis, RET/PTC rearrangements in dsvPTC, and identified BRAF as the most common mutation in pediatric cPTC. In contrast to adults, BRAF did not predict invasiveness. These results suggest a clinical role for molecular analysis of pediatric FNA samples with indeterminate cytology.
Thyroid Cancer Saturday Poster Clinical
In the SELECT trial, lenvatinib (an oral, multikinase inhibitor of VEGFR1-3, FGFR1-4, PDGFRα, RET, and KIT) significantly prolonged median progression-free survival (PFS) in patients with 131I-refractory differentiated thyroid cancer (RR-DTC) compared with placebo. This prespecified subgroup analysis examined PFS and safety for North American (NAmer) patients in SELECT compared with the overall trial population.
SELECT was a phase 3, randomized, double-blind, multicenter trial that enrolled 392 patients with progressive RR-DTC. Independently reviewed tumor assessments were performed at baseline and every 8 weeks using RECIST v1.1 criteria. Safety assessments were conducted throughout the trial.
In the overall study population (lenvatinib, n=261; placebo, n=131), lenvatinib demonstrated a significant PFS benefit vs placebo: median PFS was 18.3 vs 3.6 months (hazard ratio [HR] 0.21; 99% confidence interval [CI] 0.14–0.31; P<0.0001). PFS results were similar in NAmer patients (lenvatinib, n=77; placebo, n=39): median PFS was 18.3 and 3.5 months for lenvatinib and placebo, respectively (HR 0.15; 95% CI 0.08–0.26). Median overall survival was not reached in either arm in the overall trial nor in the NAmer subgroup. Grade ≥3 treatment-related adverse events (AEs) were experienced by 75.9% of lenvatinib-treated patients overall, which is comparable to 75.3% in the NAmer lenvatinib arm. Dose modifications in NAmer patients were also similar to rates in the overall trial: dose reductions, interruptions, and study-drug discontinuations, respectively, occurred in 68.8%, 85.7%, and 18.2% of NAmer patients. Serious treatment-emergent AEs occurred in 51.0% of overall lenvatinib-treated patients (vs NAmer lenvatinib arm, 55.8%). Out of 20 lenvatinib-emergent deaths in the overall study (3 NAmer), 6 were considered treatment-related, including pulmonary embolism (n=1) and hemorrhagic stroke (n=1).
The efficacy and safety profile of lenvatinib in NAmer patients with RR-DTC was similar to that of the overall study population.
Thyroid Cancer Saturday Poster Clinical
Thyroid cancer incidence has increased sharply in the last several decades, and it is unclear whether this represents a true incidence increase or increased diagnosis and screening. The purpose of this study is to examine the association between thyroid cancer incidence and utilization of thyroid ultrasound (US) and fine needle aspiration (FNA) in the Veterans Affairs (VA) healthcare system. We hypothesize that increases in thyroid cancer incidence rates correspond to increases in use of these diagnostic modalities.
Nationwide multi-year cross-sectional study using VA administrative data from 2000 to 2012. Joinpoint regression analysis was used to identify trends in thyroid cancer incidence and the utilization of thyroid US and FNA.
Thyroid cancer incidence increased from 10.3/100,000 in 2000 to 21.5/100,000 in 2012. Utilization of thyroid US increased from 123.1/100,000 in 2001 to 572.1/100,000 in 2012, while rates of thyroid FNA increased from 7.0/100,000 in 2000 to 46.2/100,000 in 2012. On joinpoint regression analysis, a statistically significant increase in thyroid cancer incidence between 2000 and 2008 (Annual Percent Change (APC)=3.81, p<0.05) was followed by a more pronounced increase between 2008 and 2012 (APC=10.32, p<0.05). A statistically significant increase in thyroid US occurred between 2002 and 2012 (APC=15.48, p<0.05) and in thyroid FNA between 2000 and 2012 (APC=18.36, p<0.05).
This is the first study to demonstrate a direct association between thyroid cancer incidence and utilization of thyroid US and FNA within a single integrated healthcare system. While thyroid cancer incidence nearly doubled, a nearly fivefold increase in utilization of thyroid US and a nearly sevenfold increase in use of FNA occurred between 2000 and 2012. These findings suggest that the increase in thyroid cancer incidence in the VA population may reflect an over-diagnosis of subclinical disease as a result of overutilization of thyroid US screening and FNA.
Thyroid Cancer Saturday Poster Clinical
The current management of thyroid nodules with indeterminate FNA cytology may be improved by testing that further preoperatively differentiates benign from malignant lesions, or predicts cancer extent and prognosis (e.g. tumor invasion/metastasis/recurrence risk). Tumor immune tolerance, such as suppressor cell accumulation, is a universal feature of malignancy that distinguishes cancer patients from healthy individuals and may correlate with disease status. This proof-of-concept study evaluates the diagnostic and prognostic utility of peripheral blood myeloid suppressor cell (MSC) measurement for differentiated thyroid cancer (DTC) using a novel, minimally-invasive clinical assay.
Consecutive adult patients undergoing surgery for a solitary thyroid nodule were prospectively enrolled at the LA County and USC Keck hospitals. Exclusion criteria: concurrent non-thyroidal cancer, immune deficiency, autoimmune disease, active infection. Peripheral blood leukocytes (PBL) were isolated from venous blood, stained with fluorescently-labeled monoclonal antibodies identifying two MSC subsets (MSC Clinical Assay) or regulatory T cells (Treg), and analyzed by flow cytometry.
Blood specimens, surgical pathology, and clinical course were evaluated in 44 patients (12 benign, 32 DTC). The percent CD11bintHLA-DRlowHIF1a+ MSC of PBL (%MSC11b) was higher in DTC cases compared to benign lesions (mean 13.9±6.2 vs 7.9±3.6, respectively, p<0.005). A %MSC11b value of >12% was present in 21/32 DTC cases and 1/12 benign cases (specificity=91%, sensitivity=65%, p<0.001). Within this set, 12/13 nodules with indeterminate cytology were correctly classified. Mean %MSC11b increased linearly with advancing ATA recurrence risk (p<0.01), and was higher in cases of persistent DTC versus those without evidence of disease during follow up (20±6.5 vs 13.2±6.7, p<0.05). Treg frequency did not vary significantly among groups.
Peripheral blood %MSC11b potentially discriminates benign from malignant thyroid lesions, including those with indeterminate cytology. The correlation between %MSC11b and recurrence risk suggests that preoperative %MSC11b may differentiate clinically aggressive from indolent DTC.
Thyroid Cancer Saturday Poster Clinical
Widely invasive Follicular thyroid carcinoma (FTC) is associated with grave prognosis. The basis of dividing FTC into minimally and widely invasive groups based on number of foci of vascular invasion is clearly defined however the same is not true for capsular invasion. The aim of this study was to establish the prognostic significance of the number of foci of capsular invasion in FTC.
This retrospective study consists of 119 FTC patients treated between 1990 and 2011. Two pathologists independently reviewed the histology slides. Clinical and follow-up details were noted. Different prognostic factors and overall survival (OS) were correlated with number of foci of capsular invasion.
The mean age of the patients was 48.4+13.4 years (M:F=1:2.5). 11, 33, 51, and 05%, patients had T1, T2, T3 and T4 tumors. Mean tumor size was 5.1+2.6 cm. Lymphadenopathy was noted in 13.4% and distant metastases in 56.3% patients. The distribution of capsular invasion was: <2 foci: 15.1%, 2–5: 35.3%, 6–10:33.6%, >10: 16.0%. Based on ROC analysis a cut- off of 5 foci was decided and 49.6% patients had more than 5 foci of capsular invasion. It was significantly associated with distant metastases (p=0.005). These patients had less albeit non-significant overall survival. The 10 year OS of these patients was (53.6% vs 64.2%, p value=0.12) and the mean survival of these patients was 141.2 +/− 24.9 months vs 179.2 +/− 14.9 months respectively.
Number of foci of capsular invasion has significant prognostic value in FTC.
Kaplan-Meier survival plot for capsular invasion up to five and more

Thyroid Cancer Saturday Poster Clinical
Pediatric patients make up 1.8% of the total incidence of thyroid malignancies. It is recognized that pediatric thyroid cancers (TC) tend to have advanced presentation yet maintain favorable survival outcomes. This study examines our institution's experience as a major referral center for pediatric TC.
10-year retrospective review (2005–2014) of all pediatric thyroid malignancies treated at our institution. Clinical characteristics of 60 patients <18 years old undergoing thyroid surgery were analyzed, identifying our study cohort of 25 patients with TC.
Median age at TC diagnosis was 14 years (range 6–18 years) and 44% were adolescents. A palpable neck mass was evident in 72%. Histology was papillary TC in 22 patients (88%), and 1 each follicular, medullary and anaplastic TC. Neck irradiation or family TC history were risk factors present in 16%; nearly half also had personal/family history of autoimmune thyroiditis. Total thyroidectomy was completed in 23/25 patients. Sixteen patients (64%) required lateral neck dissection; half of these were bilateral. 3 patients (12%) underwent multiple operations, 12% have permanent hypocalcemia and 8% vocal cord paralysis. Compared to adolescents, patients <10 years old had significantly greater rates of N1b disease, distant metastases, extrathyroidal extension, and transient hypocalcemia (p<0.05). Although Hispanics comprised a higher proportion (32%) of our cohort than represented in state (12%) and national (17%) demographics, their TC-related clinical characteristics were similar to our other patients. Outcomes at median follow-up time of 14 months (range 2–129 months) revealed that 10 patients (40%) completely responded to therapy, while 7 (28%) have thyroglobulin elevation, 1 stable lung metastases, 5 unknown status, and 1 death from anaplastic TC.
Our study represents one of the largest contemporary surgical series of pediatric thyroid cancers. It confirms the significant burden of disease appreciated in young patients who present at advanced TC stages, but documents trends towards even more regional metastases than in other published reports. Extensive surgery aimed at cure also predisposes to high complication rates, despite care by specialists.
Thyroid Cancer Saturday Poster Clinical
Well-differentiated thyroid cancer in pediatric patients has a high rate of lymph node metastasis at presentation and recurrence. Developing an effective management method for metastatic adenopathy is critical. We present a case series detailing intraoperative ultrasound-guided localization and methylene blue injection of suspicious lymph nodes for selective neck dissections of pediatric patients with papillary thyroid cancer and metastatic lymphadenopathy.
Retrospective chart review of patients with differentiated thyroid cancer referred to a dedicated pediatric thyroid center. Selected patients underwent intraoperative lymph node mapping using US guided methylene blue injection of suspicious lymphadenopathy. The procedure was performed by a single Interventional Radiologist along with a single pediatric otolaryngologist.
Six patients over a one-year period completed the procedure with injection of suspicious lymph nodes. All patients had a diagnosis of biopsy proven papillary thyroid carcinoma including 4 females and 2 males, (mean age 18±2.4 years). 3/6 cases involved a primary total thyroidectomy and selective, compartmental neck dissection and 3/6 were for recurrent or residual/staged disease. In revision neck dissection cases, intraoperative dye administration eased nodal identification. In 5/6 cases, metastatic lymph nodes were identified and appropriately marked with methylene blue injection. In one case, false positive results were obtained based on final pathological review of marked nodes. Surgical plans based on pre-operative imaging were modified in 5/6 patients with additional nodal involvement identified based on intraoperative US characteristics.
Intraoperative lymph node localization using ultrasound and selective methylene blue injection is an effective method and adjunct to surgical management of metastatic lymph nodes in pediatric patients with well differentiated thyroid cancer.
Thyroid Cancer Saturday Poster Clinical
Thyroid cancer incidence is increasing faster than any other cancer, particularly in early stage tumors. Little is known about the consequences of interventions and the effects of diagnosis on the health-related quality of life (HRQoL) of the large population of thyroid cancer survivors. Herein, we assess which of four well-validated preference-based survey instruments are most sensitive to clinical intervention and to obtain vital descriptive quality of life data for future comparative effectiveness research.
We recruited patients with biopsy-positive papillary thyroid carcinoma. The EQ-5D, SF6D, and Health Utilities Index Mark 2/3 (HUI2/3), were all administered by phone 1) preoperatively; 2) one month post-operatively; and 3) six months post-operatively. Survey responses were catalogued and translated into interval scale utilities (0=dead to 1=perfect health). A minimal clinically important difference (MID) of 0.03 was used.
To date, 107 responses were collected from 55 patients. 33 patients completed both pre-op and post-op surveys, and 19 completed all three surveys. 71% of respondents were female with a median age of 52 (IQR 15). Consistent across the different instruments used, more patients got worse (range: 38–58%), 13–31% stayed the same and 29–33% got better at 2 weeks post-operatively. By six months 26–47% had improved from post-op, 16–26% had gotten worse, and 26–53% had stayed the same. In comparison to pre-op scores, 21–47% had lower HRQoL scores, 22–47% had similar scores, and 21–44% had higher scores. 51% of EQ5D responses were the maximum score (ceiling effect), versus only 3% of SF6D.
This HRQoL analysis of thyroid cancer patients reflects the general good health of the study population; however, a large proportion of patients did not return to baseline quality of life. Of the indices assessed, the SF-6D is the most responsive (Table). Continued work will provide essential data for comparative effectiveness research and assess the need for a thyroid-cancer specific preference-based utility instrument. With the continued growth of the thyroid cancer survivor population, inclusion of quality of life measures in both research and clinical decision-making will be essential.
SD: standard deviation; MID: minimal clinically important difference.
Mean change in utility per patient between the three time points measured and proportion of patients exceeding the minimal clinically important difference for each of the four indices.
Thyroid Cancer Saturday Poster Clinical
The clinical importance of papillary thyroid microcarcinoma (PTMC) is debatable. PTMC is being diagnosed with increasing frequency, it is important to describe the characteristics of this cancer. This study was carried out to evaluate the clinical and histological features and long-term outcomes of PTMC patients treated at a single institution of Korea during 27 years.
A total 14,045 patients who underwent thyroidectomy between 1986 and 2013 identified from a database were assessed. Clinicopathological profile, overall and disease free survival outcomes were noted.
A total 14,045 patients, initial operative procedure of total thyroidectomy performed in 47.0% and less than total thyroidectomy performed in 53.0% patients. Central lymph node metastasis observed in 27.4% and lateral neck node in 4.9%. Of these, 86% patients followed up completely. The 10-year and 20-year overall survivals were 98.0% and 91.3%, respectively, while disease free survivals were 97.0% and 94.1%. Disease recurred in 0.9% patients. No significant differences between the total thyroidectomy and less than total thyroidectomy groups in the risk of locoregional recurrence.
The incidence of PTMCs increased progressively over the study period. The present study showed excellent prognosis of PTMC patients. Future long-term follow up of patients diagnosed in the most recent decade is needed to confirm the prognostic characteristics of Korean PTMC patients.
Thyroid Cancer Saturday Poster Clinical
This study was to evaluate time trend of characteristics of anaplastic carcinoma (ATC) and clinicopathologic factors correlated with its prognosis.
A total of 140 patients who were diagnosed anaplastic thyroid carcinoma between 1980 and 2013 from the database of Seoul National University Hospital were included in this study. Patients were divided into 3 groups based on histology: ATC (54 patients), ATC arising from DTC (31 patients), and DTC (differentiated thyroid carcinoma) with anaplastic foci (55 patients). The histology, treatment and survival were compared between the patients who were diagnosed before and after 2005 (73 and 67 patients, respectively). We analyzed the difference of survival outcomes in patients with ATC and ATC arising from DTC according to clincopathologic factors.
Median age was 58.4 years (range, 22–88) and male to female ratio was 1:2.13. The median follow-up duration was 79.3 months (range, 1–131). The 1 year overall survival rate was 32.9%, 48.2%, and 87.4% in ATC, ATC arising from DTC, and DTC with anaplastic foci, respectively (p<0.001). Survival rates were significantly different among 3 groups after 2005 (27.8%, 44.4%, and 91.9%, respectively). The frequency of cases with DTC with anaplastic foci increased; 23.3% before 2005 and 56.7% after 2005, while ATC and ATC arising from DTC decreased from 46.6% to 29.9%, from 30.1% to 13.4%, respectively (p=0.002). Treatment modalities were not different between the groups before 2005 and after 2005 (p=0.682). T-stage, overall stage, lymphatic invasion and vascular invasion were significantly different between survivors and non-survivors of ATC and ATC arising from DTC. Multivariate analysis showed that lymphvascular invasion was an only prognostic factor. (p=0.027).
Time trend of ATC showed increasing relative incidence and survival of DTC with anaplastic foci. Lymphovascular invasion is the significant prognostic factor of ATC and ATC arising from DTC.
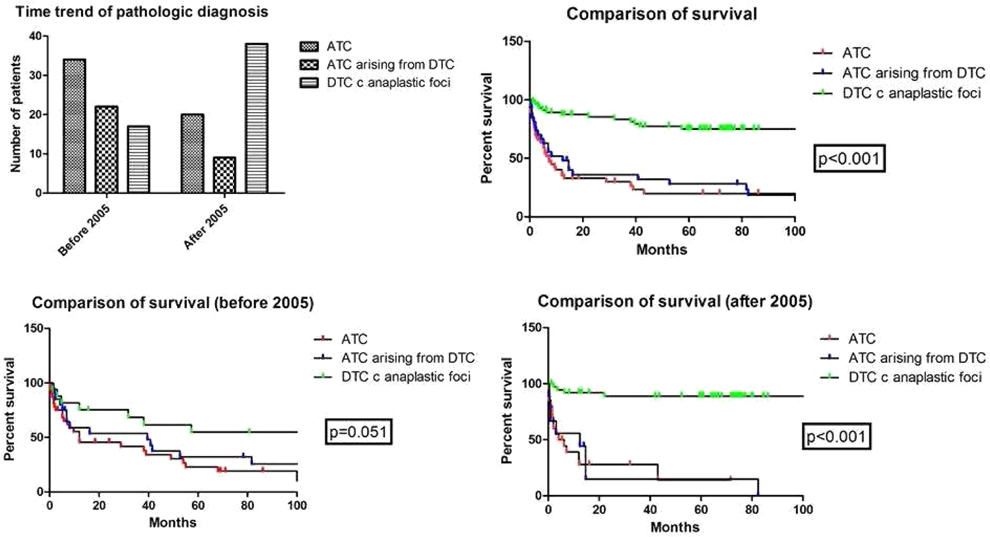
Thyroid Cancer Saturday Poster Clinical
Approximately 15% to 25% of patients with thyroid nodules subjected to fine-needle aspiration (FNA) cytology have indeterminate results and lack well-defined guidelines, resulting in either observation, repeat FNA, or thyroidectomy. We hypothesized that a standardized ultrasound scoring system and nuclear grooves on cytology may improve the ability to identify patients with thyroid cancer.
We performed a retrospective analysis of all patients with indeterminate thyroid cytology from 2007 to 2011 subsequently managed with thyroidectomy. Ultrasound images were reviewed in a blinded fashion, assigning ultrasonographic risk scores (T-score, range 1–5) based upon objective features (Table 1). T-score and cytological features were correlated with malignancy using IBM Corp. SPSS statistical software.
Ultrasound T-scoring of thyroid nodules
Of 132 indeterminate nodules, 54 (42%) were malignant with 91% papillary carcinoma histology. A T-score of 4 or 5 (n=41, cancer 26, p=0.002, specificity 81%, sensitivity 48%) and nuclear grooves (n=68, cancer 37, p=0.002, specificity 60%, sensitivity 68%) were associated with malignancy. Presence of both of these features (n=21) was predictive of malignancy (n=17) with a specificity of 95% and sensitivity of 31%. Positive predictive value (PPV) of high T-score alone was 63% while presence of both features had a PPV of 81%.
T-score and nuclear grooves are predictors of thyroid cancer in patients with indeterminate thyroid nodules. The combination of a high T-score and the presence of nuclear grooves on cytology predicts cancer in 81% of patients. The use of standardized ultrasound scoring and the presence of nuclear grooves should be used to determine the management of patients with indeterminate thyroid nodules.
Thyroid Cancer Saturday Poster Clinical
In some cases papillary thyroid cancer (PTC) patients do not need a total thyroidectomy. The American Thyroid Association recommends that a lobectomy may be sufficient treatment for small (<1 cm), unifocal, intrathyroidal PTC in the absence of prior head/neck irradiation or evidently involved cervical nodal metastases. The decision to perform a lobectomy may be based off preoperative ultrasound findings. However when adverse features are identified on permanent section, completion thyroidectomy may be required. Ideally, more informed decisions could be made based on intraoperative frozen section analysis, if it was determined that frozen section could reliably identify adverse features. Our study aims to understand how well we can identify these specific factors on frozen section relative to permanent section analysis.
IRB approval was obtained. 42 thyroid specimens from 42 patients were submitted for intraoperative frozen section analysis and were reviewed by a senior pathologist to identify the presence/absence of the following characteristics: malignancy, aggressive histology, extrathyroidal extension(ETE), multifocality, and positive lymph nodes. Samples were submitted for permanent section analysis and the same features were recorded. Statistical analysis was performed to compute agreement between frozen and permanent results.
The average measurement of agreement between frozen and permanent for malignancy was .777 with a .000 p-value; .257 with a p-value of .089 for adverse factors; .549 with a p-value of .000 for multifocal disease; .842 with a p-value of .000 for positive nodes. PPV, NPV, sensitivity and specificity values were also computed (Table 1).
The Positive Predictive Value (PPV), Negative Predictive Value (NPV), Specificity and Sensitivity were computed for the accurate identification of each adverse feature on frozen section analysis
The data suggests that concordance between frozen and permanent sections is excellent for identification of malignancy and positive nodes, fair to good for multifocality, and poor for adverse factors (ETE, lymphovascular invasion, and perineural invasion). This small sample population of 42 patients is a preliminary pilot study. It does show promise regarding the fundamental premise that potentially important adverse features can be consistently identified on frozen section and used to determine whether a completion thyroidectomy should be performed.
Thyroid Cancer Saturday Poster Clinical
The incidence of well differentiated thyroid cancer (WDTC) is increasing rapidly. Many authors feel that this increase is due to over-diagnosis and that one of the contributing factors is the increasing use of various imaging studies. The rate of obesity has also been increasing in the United States. It has been suggested that patients with an increased body mass index (BMI) have a higher incidence of WDTC than patients with normal BMI. One might hypothesize that thyroid nodules are more difficult to palpate in obese patients and that as more cancers are detected by imaging the apparent rate of increase in WDTC in obese patients would appear to be greater than in non-obese patients. This study was undertaken to evaluate this hypothesis by determining if there is any difference in the way thyroid cancers are initially detected in obese and non-obese patients.
The medical records of all 519 patients with a postoperative diagnosis of WDTC at NYU Langone Medical Center from January 1, 2007 through August 31, 2010 by the three members of NYU Endocrine Surgery Associates were reviewed. Patients were divided into Non-obese (BMI<30) and Obese (BMI≥30) groups. Patients were also divided by the initial method of detection of their tumor into Palpation, Imaging, and Incidental groups.
The final study group contained 270 patients, 181(67%) of whom were in the Non-obese Group and 89 (33%) were in the Obese Group. In the Non-obese group, 81(45%) of tumors were found by palpation, 72 (40%) were found by imaging, and 28(16%) were found incidentally. In the Obese group, 40 (45%) were found by palpation, 38(43%) were found by imaging, and 11 (12%) were found incidentally. These differences were not statistically significant (p-value 0.769).
We show that BMI does not play a role in the method of initial detection in patients with WDTC. This suggests that the prevalence of WDTC detected by imaging is not an artifact caused by an increasingly obese population and that any association of WDTC and obesity is not related to the way in which these tumors are detected.
Thyroid Cancer Saturday Poster Clinical
Pediatric and adolescent PTC is an uncommon malignancy, the issues of optimal initial treatment remain controversial due to its slow progression and good prognosis. Our study is to evaluate the optimal initial treatment for pediatric and adolescent papillary thyroid carcinomas (PTC).
In this largely retrospective study, we enrolled 140 consecutive pediatric and adolescent patients. Among them, 107 were primarily managed at our institution (primary surgery group), while the rest of 33 underwent primary surgery at other institutions and came to us for recurrence or improper primary treatment (secondary surgery group).
In primary surgery patients, 54 had undergone a total thyroidectomy (TT). The maximal tumor size of the TT group was significantly larger, and the proportion of multifocal and extrathyroidal extension was also higher. Postoperative radioiodine (RAI) therapy was administered to 10 of the patients in the TT group. Extrathyroidal extension and central neck lymph node metastasis (CLNM) were significantly associated with lateral neck lymph node metastasis (LLNM). The frequency of postoperative complications was significantly higher in the secondary surgery group, and, the mean length of the recurrence-free interval was significantly shorter.
The initial treatment is of great importance for pediatric and adolescent patients with PTC. TT is recommended for patients with large tumor sizes (more than 2 cm), multifocal tumors, and tumors with extrathyroidal extension. Prophylactic lateral neck dissection is suggested for clinically negative patients with extrathyroidal extension and CLNM. RAI is not routine but is necessary for certain cases.
Thyroid Cancer Saturday Poster Clinical
Genetic testing of FNA specimens with atypical cytology results has held the promise of subjecting fewer thyroid nodule patients to surgery for histologic confirmation of diagnosis. A commercially available gene expression classifier (Afirma) designed to have a high negative predictive value of malignancy has been available in the United States since early 2011. Biopsy material with indeterminate cytology from FNA specimens is subjected to molecular analysis, and results are reported as benign or suspicious. Suspicious specimens are referred for surgery, and benign specimens are usually observed per ATA guidelines. Little long term follow up information is available regarding the outcomes of patients evaluated in this manner, and there is no published data regarding actual cost savings to the system to date. I report the follow up outcome data available in a single clinical practice.
UGFNA material was collected using standard technique between Jan 2011 and March 2014 on 447 patients. 44 GEC was successfully run on 44 patients with indeterminate cytology. 28 GEC suspicious specimens were referred for surgery. These results have been reported elsewhere. 16 GEC benign patients were evaluated for long term follow up. This is the subject group of the study.
3 of the benign GEC patients underwent surgery (18%) Two had large symptomatic nodules. One had 2 GEC nodules evaluated with one suspicious and one benign. GEC was correct on histologic confirmation in each case. The remaining 13 GEC benign patients (82%) have been followed since initial biopsy with physical exam and ultrasound. 6 patients have been followed 2.5–3 years, 4 patients for 1–2.5 years, and 3 patients have been followed for 6–12 months. All have shown no significant change in nodules by exam or serial sonography.
Long term follow up of GEC benign thyroid nodules for a time period up to 3 years by physical exam and ultrasound seems to be a viable option in many cases. In this relatively small sample, 13 patients who would have previously been referred for surgery (30% of indeterminate cytology reports) have shown stable physical and ultrasound findings. Potential savings to the medical system in this group are estimated at $91000.
Thyroid Cancer Saturday Poster Clinical
Fluorodeoxyglucose (FDG)-avid lesion is known to show low radioiodine uptake and poor therapeutic response in radioiodine therpay (RIT) for differentiated thyroid cancer. We evaluated high-risk features related to FDG-avid lymph node metastasis (FALM) before RIT.
Patients with PTC who underwent preablative F-18 FDG PET-CT (PETpreab) before the first RIT were retrospectively enrolled. We defined the FALM as FDG-avid lymph node metastases on PETpreab which were not detected on preoperative US, CECT or postablative I-131 whole body scan. We compared the clinicopathologic factors of patients with and without FALM and performed multivariate analysis to find the factors independently related to FALM before RIT.
Seventeen out of 346 patients (4.9%) were considered as FALM. Patients with FALM showed significantly more advanced T (p=0.002) and N (p=0.002) stages, and higher frequency of patients with elevated preoperative thyroglobulin (Tg, p=0.007). Co-existence of Hashimoto's thyroiditis (HT) was more frequent in patients without FALM, although not statistically significant (p=0.094). Multivariate analysis revealed that only advanced (≥T3) T stage, N1b stage, and elevated preoperative Tg were independently related to FALM.
Advanced T, N stages, and elevated preoperative Tg are high-risk features for FALM. Preablative F-18 FDG PET-CT should be performed in those patients, and change of treatment options should be considered.
Thyroid Cancer Saturday Poster Clinical
The diffuse sclerosing variant of papillary thyroid carcinoma (DSV-PTC) is a rare subtype of PTC which has a unique clinical feature compared to classic PTC. Few studies have shown that prevalence of RET/PTC rearrangements is higher than BRAFV600E mutation in DSV-PTC. However, previous studies had limitation of small sample size. Therefore, we investigated genetic alterations in DSV-PTC and analyzed the associations between mutation status and clinicopathological characteristics.
We retrospectively reviewed 38 consecutive patients with DSV-PTC who underwent surgery between 1999 and 2009 at Samsung Medical Center. Of 38 cases, 23 cases were investigated for mutation. The BRAFV600E mutation was studies by DNA sequencing in tumor samples and RET/PTC rearrangements were determined by RT-PCR-sequencing of tumor cDNA. The relationships between mutation status and clinicopathological characteristic at the time of diagnosis and the prognosis of the patients were also analyzed.
Of 23 DSV-PTC, RET/PTC rearrangements were detected in 14 of 23 (61%): RET/PTC1 and PET/PTC3 were detected in 9 (39%) and 5 (22%), retrospectively. In contrast, BRAFV600E mutation was detected in 5 of 23 (22%). There was no case with concomitant BRAF mutation and RET/PTC rearrangements. The RET/PTC3 rearrangement was significantly associated with distant metastasis and poor outcome. (distant metastasis 3/5, alive with disease at last follow up 5/5). The RET/PTC1 rearrangement was significantly associated with favorable outcome (alive with no disease at last follow up 2/9). Coexistent Hashimoto's thyroiditis was significantly more prevalent in the PET/PTC1 rearrangement group. (8/9, p<0.05).
The RET/PTC rearrangements is the most prevalent genetic alteration in DSV-PTC. DSV-PTC harboring RET/PTC3 rearrangement is associated with a poor prognosis while those RET/PTC1 rearrangement may be a more favorable prognosis. Furthermore, the PET/PTC1 rearrangement had a higher prevalence of Hashimoto's thyroiditis in DSV-PTC.
Withdrawn
Thyroid Cancer Saturday Poster Clinical
The fine needle aspiration cytology (FNAC) and thyroglobulin measurement in needle washout (FNA-Tg) are recommended for diagnosis of metastatic or recurrent lymph nodes (LN) in thyroid cancer. However, determination of FNA-Tg cutoff values for diagnosis of metastasis LN and final outcome of discordant results between FNA-Tg and FNAC in thyroid cancer still remain unclear.
This retrospective observational hospital-cohort study enrolled consecutive 661 thyroid cancer patients with single or multiple suspicious cervical LNs (1050 lesions) from May 2011 to December 2013 in whom both FNA-Tg measurement and FNAC had been performed. The clinical parameters included patient demographics, primary tumor pathology, thyroidectomy status, radioiodine therapy, thyroid function test, Tg/anti-Tg antibody levels, and cancer persistence/recurrence. The ultrasonographic features, FNA-Tg levels, and FNAC results, and final outcome of individual suspicious LN were also reviewed.
FNA-Tg levels were significantly lower in LNs from serum TgAb-positive patients than in those from TgAb-negative patients. There were 60 discordant cases, 2 were revealed lung cancer metastasis which were initially showed papillary thyroid cancer in FNAC with low FNA-Tg and negative serum Tg, 26 lesions were finally diagnosed malignant which showed high FNA-Tg and negative FNAC, 3 cased showed malignancy in FNAC with low FNA-Tg but final histologic diagnosis were benign. And there was 17 case exhibiting non diagnostic result in FNAC with high FNA-Tg, it eventually become diagnosed malignant in final histopathology.
FNA-Tg measurement is highly reliable in the diagnosis of neck metastases in PTC patients. FNA-Tg levels combined with FNAC results in suspicious LN of thyroid cancer could guide various clinical decision.
Thyroid Cancer Saturday Poster Clinical
The risk for recurrence and mortality in thyroid carcinoma is determined by multiple factors, including age at diagnosis, completeness of resection, local invasion, and distant metastasis. Locally aggressive differentiated thyroid carcinoma, which is typically indolent, is an exception to this general rule, although there is little information on outcomes related to management in such patients, who are at high risk for local recurrence.
We reviewed 80 cases with differentiated locally invasive thyroid carcinoma (T4), previously diagnosed between 1987 and 2013, and restaged them according to the current AJCC to identify factors predicating survival/mortality. 51 cases were excluded because of histology (poorly differentiated or anaplastic) or downgraded based on localized soft tissue involvement (T3). Patient records in the remaining 29 cases (17 females, 12 males) were reviewed to determine age at diagnosis, tumor size, histology, nodal involvement, extra-nodal extension, completeness of resection, metastasis, local structures invaded/involved, and MACIS score.
The mean age at diagnosis was 58.2 (±15.6) years, and the median duration of follow up was 42 months (IQR 10–101). The five-year mortality was 27.6% (8/29). Approximately 50% of the patients died after diagnosis (15/29). Nine patients had at least one local recurrence (4 with multiple), 5 developed distant metastases. Kaplan-Meier survival analysis showed that age at diagnosis (HR 1.063/unit increase in age [CI 1.01–1.114, p=0.011) and tumor diameter (HR=1.288 [CI 1.04–1.6], p=0.02) were associated with a higher all-cause mortality. The mean tumor diameter was 4.12 (±2.7) cm. A higher MACIS score at diagnosis was significantly associated with mortality (9.47 in deceased patients vs. 7.49 in survivors), (p=0.024), whereas aggressive resection with recurrent laryngeal nerve sacrifice was protective (HR 0.26 [CI 0.08–0.9], p=0.023).
Survival in differentiated locally invasive thyroid carcinoma (T4), related to age, tumor size, and MACIS score can be prolonged with aggressive resection.
Thyroid Cancer Saturday Poster Clinical
Ultrasonographic calcification is one of most important ultrasonographic(US) findings to diagnosis malignant thyroid nodules. Especially, microcalcification is well known to be highly associated with papillary thyroid carcinoma. However, US calcification could be a pathological prognostic factor has not evaluated as much. The aim of this study was to evaluate postoperative histological prognostic factors according to the presence and types of US calcification.
A total of 1,297 thyroid nodules which were diagnosed as papillary thyroid carcinoma(PTC) of 901 patients who underwent thyroidectomy. US calcification was classified in to fine stippled psammomatous (FSP) and non-FSP types.
A total 40.5% (525 of 1297) of PTC nodules had US calcification. Among of them, 42.9% (225 of 525) was FSP type. The nodules with US calcification is larger than without US calcification (11.7 vs 7.9 mm, p<0.001). However, there was no significant difference of size between FSP and non-FSP. PTC with FSP type calcification showed higher incidences of N1 staging (57.0 vs 47.5%, p=0.02), lymphovascular invasion (32.1 vs 23.7%, p=0.045) and metastasis (38.4 vs 34.1%, p=0.05) than non-FSP type. Underlying thyroiditis higher existed in PTC with FSP than non-FSP (32.0 vs 22.7, p=0.022).
The present study suggest that US finding of FSP type calcification may be a useful prognostic indicator of aggressive PTC behaviors. Therefore preoperative US FSP type calcification would be a useful indicator for preoperative or intraoperative decision-making.
Thyroid Cancer Saturday Poster Clinical
Parathyroid carcinoma is estimated to account for 0.005% of all reported cancers or 5.73 cases per million persons. Surgery remains the initial treatment of choice, with most operations including en bloc resection. It is unclear, however, whether central neck dissection is necessary. The incidence of positive lymph nodes in patients who have undergone central neck dissection for parathyroid carcinoma was examined in this study using data from the Surveillance, Epidemiology, and End Results (SEER) cancer registry.
SEER data were used to identify patients who were diagnosed with parathyroid carcinoma from 1998 through 2011. The study period was selected because of more extensive details on surgery and lymph node dissection starting in 1998. The frequency of cases with positive lymph nodes and its impact on survival were determined.
From 1998 through 2011, 404 patients with parathyroid carcinoma were reported. Surgery was performed and documented in 374 (92.6%) cases. Of these, 77 (19%) had documented lymph nodes removed and in 15 cases (3.7%) positive lymph nodes were found. The median survival of patients with positive nodes was 56.7 (CI 82.4 to 29.9) months and the median survival with negative or undocumented nodes was 66.1 (CI 102.3 to 21.9) months (p=0.49).
Lymph node involvement is uncommon in parathyroid carcinoma. Although en bloc resection is recommended during surgery, the added benefit of lymph node dissection is not clear. Further prospective studies may need to be done to define the optimal surgical approach for these patients.
Thyroid Cancer Saturday Poster Clinical
Hypocalcemia is one of the most common complications of thyroid surgery, but its optimal protocol for the prediction of development of hypocalcemia is still controversial. We investigated this study to determine the clinico-pathological risk factors and reliable biochemical predictors of the development or non-development of hypocalcemic symptoms after total thyroidectomy on the basis of serum calcium and intact parathyroid hormone (PTH) levels measured 1 hour after surgery.
A prospective study was performed of 817 patients who underwent a total thyroidectomy with central compartment node dissection (CCND) due to well-differentiated thyroid cancer. We evaluated the correlations between hypocalcemic symptom development and clinico-pathological factors. And the predictability for hypocalcemic symptom development of intact PTH cut-offs (<10 pg/mL and <20 pg/mL, respectively) according to serum calcium level subgroup were analyzed.
Female gender (P<0.001) was the only independent risk factor for hypocalcemic symptom development in multivariate regression analysis. The negative predictive value (NPV) of intact PTH, signifying non-development of hypocalcemic symptoms, was higher than the positive predictive value (PPV) which was signified development of hypocalcemic symptoms. In addition, when we applied the different adoption of the intact PTH cut-off according to serum calcium level, we could obtain more increased NPVs.
A female gender and the application of more specific cut-offs for intact PTH according to the serum calcium levels measured 1 hour after surgery may help thyroid cancer patients who undergo a total thyroidectomy with CCND to be more safely discharged.
Thyroid Cancer Saturday Poster Clinical
Patients with thyroid carcinoma typically present with an enlarging neck mass. Distant metastasis without a history of neck swelling as the initial presentation of thyroid carcinoma is extremely rare. We retrospectively reviewed patients seen at our center over the last 12 years, who did not have a history of neck swelling and presented with distant metastases as the initial manifestation of thyroid carcinoma.
Case records of patients with thyroid carcinoma seen at the National Cancer Centre Singapore from 2002 to 2013 were retrospectively reviewed. Patients with no prior complaint of neck swelling and whose initial presentations were that of distant metastases histologically-confirmed to be metastatic thyroid carcinoma were included. Loco-regional metastasis such as cervical nodal disease was excluded.
A total of 15 cases fulfilled inclusion criteria. The median age at presentation was 63 (range 34–81) years. No gender preponderance was found (46.7% female vs 53.3% male). All 15 patients presented with osseous (40%), pulmonary (33.3%), cerebral metastases (6.7%) or a combination of two out of three aforementioned sites (20%). Axial (n=4) and appendicular (n=3) skeletal metastases were equally common in patients with osseous metastases. Two patients had metastases at both axial and appendicular skeletal sites. Follicular thyroid carcinoma (FTC) was the most common (46.7%) followed by papillary (33.3%) and medullary (20%). Ten out of 15 patients (66.7%) underwent total thyroidectomy after metastatic disease was confirmed while the rest declined or were unfit for surgery. The median size of the largest tumour focus on histopathological examination was 27 (range 3–80) mm. Lymphovascular and extrathyroidal extension was present in 90% and 60% of thyroidectomy specimens respectively.
Distant metastasis without neck swelling as the initial presentation of thyroid carcinoma is extremely rare. When present, osseous metastasis and FTC are the most common site and etiology respectively. We recommend long term follow-up to evaluate the prognosis of these patients. Histopathological studies should be considered to identify risk factors that predisposed this rare and unfortunate group of patients to distant metastases.
Thyroid Cancer Saturday Poster Clinical
Unlike Western countries, few data document clinical characteristics of well differentiated thyroid carcinoma in South Africa or the African continent. Lesions <10 mm at presentation have a favourable prognosis, but we have observed some patients with advanced disease, despite small primary lesions. We wished to describe the clinical characteristics of patients attending a tertiary referral centre in South Africa, hypothesising that a subset with small primary lesions has more aggressive disease.
Folders were reviewed of all patients with differentiated thyroid carcinoma, referred for radioiodine ablation at a tertiary centre from January 2007 until January 2013. Demographic and clinical data were collected and patients were divided into two groups, based on the size of the primary lesion. Clinical characteristics of these two groups were compared (<10 mm and >10 mm). Staging used TNM pathological system, histology, radiology and scintigraphy
There were 103 patients, 90 (87%) female, whose median and interquartile range (IQR) age at presentation was 45.0 (32.5–56.5) years. Primary histology was papillary in 73 (71%). Initial presenting stage was (15.5%) stage1, (47.5%) stage2, (22%) stage3 and (13.5%) stage4, but this did not correlate with traditional risk factors. The subgroup defined as having metastases, despite a small primary lesion (n=8; 7.8%) was compared to the group with primary lesions >10 mm with metastases (n=53; 51.5%). Median age, gender, extent of surgery, primary histology and poor prognostic histological features, did not differ between these two groups. In the entire cohort, there were 6 patients with multifocal dual pathology; 5 (papillary and follicular carcinoma) and 1 patient with papillary and Hurtle cell carcinoma.
Our patients had predominantly papillary carcinoma, but traditional risk factors did not consistently explain a more advanced stage. We identified small groups of patients with multifocal dual histology and small primary lesions with metastases. Genetics analyses are warranted to characterise our patients.
Thyroid Cancer Saturday Poster Clinical
There is a dilemma for clinicians to decide management of atypia of follicular lesion of undetermined significance (AUS/FLUS). We evaluated what factors afftect decision making of follow-up of AUS/FLUS thyroid nodule when they were done a repeated-fine needle aspiration (FNA) in clinical setting.
We prospective enrolled 102 patients who underwent repeated FNA due to previously diagnosed with AUS/FLUS. Ultrasonography (US) and BRAFV600E mutation were analyzed at the time of repeated-FNA.
The rate of thyroidectomy after repeating FNA was 15.7% (16/102). Total 12.7% (13/102) patients were diagnosed with malignancy after operation. Five (4.9%) patients were diagnosed with malignancy cytology at repeated FNA. Further three patients were decided to surgery and confirmed malignancy according to the BRAFV600E mutation. The positive rate of BRAFV600E mutation was higher in the nodule with suspicious malignant US findings than non suspicious malignant (29.2% vs. 0%, P<0.05).
The present findings demonstrate that BRAFV600E mutation showed a complementary role in the repeat FNA of thyroid nodules with AUS/FLUS when the US findings of AUS/FLUS have suspicious malignant. Therefore BRAFV600E mutation analysis might be considered when repeated FNA was planned in AUS/FLUS cytology with malignant US findings.
Thyroid Cancer Saturday Poster Clinical
Thyroglossal duct cysts (TGDC) are the most common congenital anomaly in the development of the thyroid gland. Seventy percent of midline masses diagnosed during childhood and 7% in adults are TDGC. Thyroid carcinomas can arise from thyroglossal duct cysts and comprise 1% of thyroid cancer cases.
A 30-year-old female presented with a 6-month history of an anterior midline neck mass. Physical examination revealed a 2-cm midline cystic mass at the level of the hyoid bone. The thyroid gland was normal with no palpable cervical lymph nodes. Thyroid function tests were normal. Thyroid ultrasound showed benign appearing subcentimeter thyroid nodules. There was no history of radiation or family history of thyroid cancer. Neck CT scan showed a heterogeneous 2.1×1.2×1.3 cm nodule in the left infrahyoid region, compatible with a thyroglossal duct cyst remnant; a 6-mm enhancing nodule was also seen within the posterior aspect of this lesion. Ultrasound-guided FNA of the TGDC was consistent with cystic papillary thyroid carcinoma (PTC). Histopathological examination after a Sistrunk operation was positive for a 0.8×0.6×0.4 cm PTC. Patient underwent total thyroidectomy and central neck dissection which revealed no evidence of malignancy in the thyroid gland or lymph nodes.
TGDC carcinoma typically presents as a midline palpable neck mass. The median age at presentation is usually 40 years with female predominance. It is usually diagnosed after histologic study with the majority of cases being papillary type. The surgical treatment of TGDC carcinoma is controversial. Some authors consider the Sistrunk procedure alone to be sufficient (cure rate of 95%), but recent reports recommend additional total thyroidectomy.
PTC arising in a TGDC is rare and highlights the importance of a thorough clinical and pathological examination. Given the excellent prognosis, rendering a correct diagnosis is crucial to proper patient management.
Thyroid Cancer Saturday Poster Translational
LGR5 is an orphan G-coupled protein receptor expressed on cancer stem cells (CSCs) that potentiates Wnt/B-catenin signaling. Dysregulation of Wnt/B-catenin signaling contributes to the aggressiveness of human papillary thyroid cancer (PTC), potentiating CSC proliferation and promoting metastases. The ligand for this receptor, R-spondin (RSPO), has recently been described. Objectives: To demonstrate that RSPO and LGR5 are up-regulated in PTC. To demonstrate that LGR5 expression is associated with nodal metastases and tumor aggressiveness.
Using two well-established human PTC cell lines (TPC-1, KTC-1) and a normal thyroid cell line (NThy-ori 3-1), we pharmacologically and genetically manipulated LGR5 to evaluate its effect on Wnt/B-catenin, cellular proliferation, and cancer invasion/migration. We performed clinical analysis of Duke PTC patients from 2003–2013 (n=275 patients) and studied effects of LGR5 tumor expression on tumor histology, TNM stage, locoregional metastasis, and BRAFV600E status.
LGR5 and RSPO3 are 1500-fold and 20-fold higher, respectively, in PTC cell lines and 20 to 60-fold higher in human frozen thyroid tissue as compared to normal controls. R-spondin potentiates B-catenin/LGR5 expression whereas Wnt pathway inhibitor, niclosamide, significantly decreases expression. Overexpression of LGR5 had no effect in PTC cell growth or viability, where is it already highly expressed. Conversely, silencing LGR5 expression by RNA interference dramatically reduced cellular proliferation and migration. In humans, LGR5 overexpression was strongly associated with lymph node metastases (p<0.001), vascular invasion (p=0.015), and male gender (p=0.009). There was no correlation of LGR5 positivity with tumor size, histologic variant, capsular invasion, or extrathyroidal extension. For patients with at least 5 nodes sampled, tumor LGR5-positivity predicted lymph node metastases with a sensitivity of 100% and specificity of 75%. BRAFV600E mutation-positive tumors demonstrated highest expression of LGR5.
LGR5 potentiates Wnt/B-catenin signaling and tumor invasion in human PTC. Patients with LGR5-positive tumors have a high probability of loco-regional metastases.
Thyroid Cancer Saturday Poster Translational
BRAF V600E mutation is associated with poor prognosis in patients with papillary thyroid carcinoma (PTC). PTC is often multifocal, however, and there are no guidelines on how many tumors to test for BRAF mutation in multifocal PTC.
This retrospective study was approved by Tulane's IRB. Twenty-five separate formalin-fixed and paraffin-embedded thyroid tumors from eleven patients were manually microdissected and tested for five point mutations in BRAF codon 600: V600E, V600K, V600R, V600D, and V600M. This was done using a commercial allele-specific real time polymerase chain reaction-based assay (Entrogen, Woodland Hills, CA) that can detect a mutation present in as little as 1% of the DNA. Data related to histologic characteristics, patient demographics and outcomes were collected.
All mutations detected were BRAF V600E. Eight patients (73%) were BRAF-positive in the largest tumor (mean size 1.4 cm±0.8 cm), and three patients (27%) were BRAF-negative in the largest tumor (mean size 1.9 cm±0.8 cm, p=0.2). For all three patients whose largest tumor was BRAF-negative, their next-largest tumor (mean size 0.5 cm±0.1 cm) was BRAF-positive. The next-largest tumors were all of the same histologic variant as their corresponding larger tumors, and only one of the next-largest tumors had histologically aggressive features (location near the capsule and irregular borders). None of the three patients whose largest tumor was BRAF-negative presented with positive lymph nodes or distant metastases. One of these patients had a positive stimulated thyroglobulin with radioiodine uptake in the mediastinum post-total thyroidectomy, which may have been residual tumor (vs. ectopic thyroid tissue); otherwise, none of the three have had recurrence.
Patients with multifocal PTC whose largest tumor is BRAF-negative can have additional BRAF-positive tumors, and molecular testing of multiple foci should therefore be considered. Future prospective studies are warranted to establish whether BRAF mutation in a smaller tumor correlates with disease progression and poorer clinical outcomes.
Thyroid Cancer Saturday Poster Translational
Thyroid nodules are extremely common, yet thyroid cancer is a relatively rare condition. The identification of a nodule as benign or malignant has important surgical and therapeutic implications. However, in a significant number of cases, this distinction is challenging. Many of these difficult cases are diagnosed as indeterminate and often result in unnecessary surgical procedures. MicroRNAs constitute a class of short, non-coding RNAs that play key roles in the regulation of gene expression. MicroRNA expression profiling has been shown to be a reliable method for cancer subtype classification. In the present study, we screened over 2000 microRNAs to identify microRNA biomarkers that can stratify thyroid lesions as “benign” or “malignant” in pre-operative Fine Needle Aspirate (FNA) samples. We show that microRNA expression profiling is a promising new strategy for the precise classification of thyroid nodules.
Over one hundred thyroid FNA samples representing various histological subtypes were collected, most of which were indeterminate. Using proprietary protocols, high-quality RNA was extracted from the samples and hybridized to custom-made microarrays measuring the expression of over 2000 microRNAs. Next generation sequencing was run on an additional set of over 20 thyroid resection samples in order to find novel microRNA biomarkers.
Differential expression of microRNAs was found between benign lesions and malignant neoplasms based on FNA samples. Importantly, a combination of a small number of microRNAs was able to successfully differentiate benign from malignant neoplasms with accuracy exceeding 85%. In addition, microRNAs were able to distinguish between specific subtypes of thyroid tumors, including morphologically similar nodules. Novel microRNAs were found using next generation sequencing which may further improve the classification accuracy.
MicroRNAs are promising biomarkers for the classification of pre-operative thyroid nodules. These findings form the basis for the development of a simple and reliable diagnostic assay, which will offer an accurate tool for classification of surgical and pre-operative thyroid samples, including those that presently fail cytological evaluation.
Table 1: Clinicopathologic characteristics of the study patients
All patients were M0. T=tall cell variant, H=hobnail variant, C=classic variant, F=follicular variant, W=Warthin's variant, *=invasive borders, **=invasive border with extrathyroidal extension, ^=near capsule, RAI=radioiodine
Thyroid Cancer Saturday Poster Translational
Recently, we reported that the expression of ABI3 is down-regulated in thyroid carcinomas while it was expressed in benign lesions. We further demonstrated that ectopic expression of ABI3 significantly inhibited cell growth, invasiveness and migration in vitro and tumor growth in vivo, accompanied by an increased of senescence, suggesting that ABI3 is a potential tumor suppressor gene. However, the mechanism involved in the loss of ABI3 expression in thyroid carcinomas has not been fully elucidated. We here investigated the potential role of ABI3' promoter methylation in the transcriptional silencing of ABI3.
We evaluated gene expression by RT-qPCR and methylation degree by bisulfite-sequencing in two follicular thyroid carcinoma cell lines(WRO and FTC238) treated with 5-azacytidine(5-AZA) and 14 follicular thyroid adenomas (FTAs) and follicular thyroid carcinomas (FTCs) samples.
As re-expression of ABI3 was observed in both cell lines after 5-AZA treatment (p<0.001), we evaluated the methylation degree of ABI3 promoter in these cell lines and in FTAs and FTCs. We detected three CpG rich areas that did not qualify as CpG islands. Although all three regions (R1-R3) were methylated in thyroid carcinoma cell lines, only R1 showed an association between methylation degree and loss of ABI3 expression in thyroid cell lines (p<0.05). We additionally observed that R1 were hypermethylated in FTC samples when compared to FTA (p<0.001). Indeed, negative correlation between R1 methylation and ABI3 expression was also observed in FTA and FTC samples (p<0,001). Further analysis revealed a NKX2-1 binding site present in the R1 of ABI3 promoter. Importantly, we observed that ABI3 was re-expressed only when NKX2-1 was present and R1 hipomethylated.
We here demonstrate that hypermethylation of ABI3 promoter is a potential mechanism associated with the loss of ABI3 expression in FTCs and that ABI3 expression in FTA seems to be dependent on the presence of NKX2-1. These findings not only reinforce the potential roll of ABI3 as a tumor suppressor gene but also may help to understand the molecular basis involved in thyroid tumorigenesis and highlights the potential use of ABI3 as a new target for epigenetic therapeutic strategies.
Thyroid Hormone Action Saturday Poster Basic
Thyroid hormones (THs) exert their biological effects through their binding to thyroid hormone receptors (TRs). These TRs interact with the TH-response elements located at the promoter regions of TH-dependent genes and recruit coregulators to induce or inhibit their expression. In teleosts, we have shown that 3,5-diiodothyronine (3,5-T2 or T2) regulates the expression of TH-dependent genes in the same way as T3, but through the binding and activation of a specific isoform of the TRβ1, different from that activated by T3. These isoforms differ in the presence (long or L-TRβ1) or absence (short or S-TRβ1) of a 9 aminoacid insert in the ligand binding domain (LBD) of the receptor. Furthermore, T3 and T2 seem to promote the recruitment of a different coregulator population to the ligated S- or L-TRβ1 isoforms, respectively. In order to identify possible coregulator S- or L-TRβ1 binding partners, we initially looked for coregulators that interacted with the T2+L-TRβ1 complex using a yeast 2-hybrid screen. Jab1 was identified as an interacting partner of the full L-TRβ1+T2 complex.
To study the interaction mechanisms and the transcriptional effects of Jab1 bound to the TRβ1 isoforms, we performed: 1) yeast 2-hybrid assays with the L-TRβ1 LBD plus Jab1; and 2) transactivation assays with L-TRβ1, S-TRβ1 or delta NTD L-TRβ1 plus increasing concentrations of Jab1, in the presence or absence of T2 or T3.
Our results showed that Jab1 does not bind to the LBD of L-TRβ1, but it enhances T2 and T3-dependent L-TRβ1 mediated transcription; however, the presence of the NTD is necessary for T2 but not T3-dependent transcription. Surprisingly, Jab1 repressed T3-dependent S-TRβ1 mediated transcription, suggesting an opposite role as a corepresor when interacting with this TRβ1 isoform.
These results postulate Jab1 as a specific coactivator of the L-TRβ1+T2 complex and a corepressor of the S-TRβ1+T3 complex. The possibility of isoform- and ligand-specific TRβ1 partner protein interactions that result in opposite functional outcomes may explain, at least in part their divergent biological functions, and their target gene regulatory properties. (Supported by PAPIIT: IN201614-25).
Thyroid Hormone Metabolism & Regulation Saturday Poster Basic
Abnormal thyroid system function is increasingly common in premature and compromised newborns. This includes elevated thyroid stimulating hormone (TSH) in the presence of normal thyroid hormone (TH) levels reflecting an altered TSH/TH set point. Mechanisms underlying this thyroid system dysfunction remain largely unknown. We have established the zebrafish as an evolutionarily conserved model for the study of hypothalamic pituitary thyroid (HPT) axis development. Here we characterize thyrotrope sensitivity to TH levels through development, providing a new model to study the impacts of embryonic conditions on thyrotrope development and the maturation of TSH regulation.
We exposed 7- and 14-day post fertilization (dpf) zebrafish larvae to a range of T4 concentrations (1; 2.5; 12.5; 25 nM) for 2 days. We then assessed relative gene expression of tshβ, dio2, dio3, and trβ by RT-qPCR as a read-out of thyroid axis regulation by TH.
Tshβ gene expression was reduced by 40–60% in the presence of T4 in both 7 and 14 dpf larvae. At 7 dpf the threshold for tshβ suppression was 2.5 nM T4 (p<0.01), with no change in tshβ expression seen following exposure to 1 nM T4. In contrast, at 14 dpf, tshβ gene expression was reduced (by ∼50%) in the presence of 1 nM T4 (p<0.01). Similarly, TH exposure led to increased trβ and dio3 expression at both 7 and 14 dpf. At 7 dpf expression of both genes doubled following exposure to 12.5 nM T4 (p<0.01) but was unaffected by lower TH concentrations. Again, 14 dpf larvae displayed increased sensitivity to TH, with expression of both trβ and dio3 doubling following exposure to only 1 nM T4 (p<0.01).
Tshβ, trβ and dio3 gene expression levels reflect HPT responsiveness to TH and provide an assay for changes in HPT sensitivity to TH in zebrafish. We show that tshβ gene regulation becomes increasingly sensitivity to TH through larval development, and that TH-regulated trβ and dio3 expression might contribute to changes in the TSH set point. These studies of thyrotrope sensitivity maturation under normal conditions will allow us to examine how abnormal embryonic environments affect the ontogeny of the TSH set point in vertebrates.
Thyroid Hormone Action Saturday Poster Basic
We have recently shown that the biological effects of 3,5-T2 (T2) are mediated by a different TRβ1 isoform that contains a 9 amino acid insert in its ligand binding domain, and which we have denominated long TRB1 (L-TRB1). Furthermore, in-vivo and ex-vivo, T2 specifically down-regulates L-TRB1 expression, whereas T3 down-regulates the short TRB1 isoform (S-TRB1) which lacks this insert. In addition to their independent activities, thyroid hormones (THs) and cortisol (C) have co-regulatory interactions in numerus vertebrates including fish. Both, THs and C mediate their actions through their corresponding nuclear receptors (NRs). The present study was designed to evaluate a possible cross-talk between cortisol and the two bioactive THs by evaluating the cross-regulation of each others receptor expression.
To this end, a series of time- and dose-response curves were performed in organotypic tilapia liver cultures to establish treatment conditions for C, T3 and T2. Hepatic slices were then treated with 1 nM of T3, T2 and/or C in culture media for 12 and 24 hours, and the mRNA expression of their corresponding NRs was quantified: (T3: S-TRB1; T2: L-TRB1; C: GR and MR). The expression levels of GH and IGF-1, genes that are inversly regulated by C and THs was also analyzed.
Our results showed that all studied NRs were down-regulated by their cognate ligands, while a cross and opposite (positive) regulation was observed for both TRs by C, and for MR and GR by both THs. Furthermore, only T2 blunted the up-regulatory effect of C upon L-TRB1 expression. However, C effect upon S-TRB1 expression was only partially reverted by T3, suggesting a stronger regulatory effect of C upon this TR isoform. As expected, GH and IGF-1 expressions were increased by T3 and T2, and decreased by C, and co-treatment of C+T3 or T2 reversed C inhibition to control levels.
So far, these results show cross-regulation of cortisol and the T3 and T2 signalling pathways, providing elements for understanding the interactive functions of these two endocrine systems in non-mammalian species. (Supported by PAPIIT IN201614-25)
Thyroid Hormone Action Saturday Poster Translational
The goal of this prospective study is to evaluate the effect of thyroid hormone (TH) on brown adipose tissue (BAT) in adult humans, specifically whether hyperthyroidism increases, while hypothyroidism decreases, BAT mass and activity.
We studied 8 patients diagnosed with differentiated thyroid cancer who underwent thyroidectomy and were scheduled to receive radioactive iodine treatment after TH withdrawal (age 41 +/− 3.9, F:M=5:3, weight 80.7 +/− 6.6 kg, BMI 27 +/− 2.2 kg/m2). The subjects participated in two study visits, first in the hypothyroid state after TH withdrawal at the time of the radioactive iodine treatment and then in the hyperthyroid state three to six months after starting TH suppressive treatment. We measured the whole-body BAT volume and activity via 18F-FDG PET/CT after 120 min of cold exposure using a cooling vest set to 15–16°C during both study visits. We performed indirect calorimetry at baseline and after 60 min of cold exposure during each study visit.
Six out of the 8 enrolled subjects completed the study. The baseline resting metabolic rate was higher in the hyperthyroid compared to the hypothyroid phase (1334 +/− 50 vs. 1470 +/− 82 Kcal/day, p=0.046) and after 60 min of cold exposure during the hyperthyroid but not the hypothyroid phase. Thyroid function test results were different between the hypothyroid and hyperthyroid phase (free T4 0.59 +/− 0.33 vs. 3.78 +/− 0.27 ng/dL, p=0.03) but not after 60 min of cold exposure during each phase. All patients showed detectable BAT in both hypothyroid and hyperthyroid phase (total BAT volume: 68.10 +/− 15.69 vs. 87.70 +/− 16.47 mL, p=0.25; total BAT activity 137.12 +/− 55.07 vs. 188.99 +/− 55.54 SUV*g/mL, p=0.34). There was a correlation between the BAT mass and activity in the hypothyroid and hyperthyroid phase. The majority but not all (4 out of 6) subjects showed an increase in BAT volume and activity between the hypothyroid and hyperthyroid phase.
Thyroid hormone seems to play a role in the growth and activity of BAT. Further studies to investigate factors that potentiate the effect of TH on BAT mass and activity are needed.
Thyroid Hormone Metabolism & Regulation Saturday Poster Basic
Ghrelin is an orexigenic peptide hormone that stimulates appetite and is involved in energy homeostasis. It is secreted in the gastrointestinal tract and affects multiple organs. In thyroid dysfunction, ghrelin levels are changed and hence may play a role in energy homeostasis in these disorders. However, little is known about ghrelin's direct effect on the thyroid gland. Thus, the aim of the study was to describe the direct effects of ghrelin on primary human thyroid cells.
Human thyrocytes from thyroidectomies were cultured to confluent monolayers, and exposed to varying concentrations of TSH and ghrelin for 72 hours. Activity was measured by quantifying thyroglobulin (Tg) and cAMP production in supernatants by ELISA and RIA, respectively. Initially, the maximum ghrelin effect on thyroid function was established by varying ghrelin concentration (10-11 to 10-6 M) at 0.1 IU/l TSH. Cells were stimulated by varying concentrations (0.1, 0.5 and 1 IU/l) of TSH at maximum ghrelin inhibitory concentration (10-7 M) or vehicle. In addition, Tg, thyroid peroxidase (TPO), thyroid stimulating hormone receptor (TSHR), sodium iodide transporter (NIS) and (interleukin-6) IL-6 mRNA expression levels were estimated by qRT-PCR.
TSH induced a concentration dependent increase of Tg and cAMP production during 72 h. Ghrelin in contrast, inhibited the TSH mediated induction, in a concentration dependent manner at 0.1 IU/l TSH with the greatest inhibition at 10-7 M ghrelin. The ghrelin induced inhibition of Tg secretion was 65%, 52% and 41% of the full response (n=6, 3 and 3) at 0.1, 0.5, and 1 IU/l of TSH, respectively. Similarly, ghrelin decreased the TSH induced cAMP accumulation 22%, 14% and 26% at 0.1, 0.5 and 1 mU/l of TSH, respectively (n=5, 3 and 4). In addition, a tendency of a corresponding ghrelin mediated inhibition of NIS, TPO and TSHR mRNA expression levels was observed.
Ghrelin induced a decrease in Tg and cAMP in TSH stimulated primary human thyrocytes, possibly mediated by inhibition of TSH-R, NIS and TPO mRNA expression. Ghrelin-induced decrease in thyroid function may be important for energy preservation during fasting.
Thyroid Hormone Metabolism & Regulation Saturday Poster Clinical
Congenital hypothyroidism (CH), detected by newborn screen (NBS) is most commonly caused by thyroid dysgenesis or dyshormonogenesis and results in permanent hypothyroidism. Consumptive hypothyroidism is caused by excessive type 3 deiodinase (D3) activity that inactivates circulating thyroid hormones at rates which exceed the secretory capacity of the normal hypothalamic-pituitary-thyroid axis. This has been reported in patients with large D3-expressing vascular tumors (most commonly infantile hepatic hemangiomas), fibrous tumors, or gastrointestinal stromal tumors. We report the case of a neonate with CH detected on NBS that resolved after resection of a D3-expressing fibrosarcoma.
A full term infant was born with a large solid tumor of the hand. NBS at 2 days of life showed T4=12.59; TSH=20.50. Serum testing at 14 days confirmed primary hypothyroidism (free T4 0.6 ng/dL [0.6–1.2]; TSH 36.61 mIU/mL [0.34–5.6]). Levothyroxine (LT4), 37.5 mcg daily restored euthyroidism. The tumor was surgically removed at 2 months of age and diagnosed as a fibrosarcoma. Thyroid function tests obtained 1 week after this surgery showed hypothyrotropinemia (TSH 0.88 mIU/ml [1.7–9.1]), suggesting overtreatment. Subsequent thyroid tests showed recurrent hypothyrotropinemia (TSH as low as 0.37 mIU/ml [1.12–8.21]) and hyperthyroxinemia (free T4 as high as 1.7 ng/dl [0.6–1.2]) that resolved after discontinuation of LT4. The resolution of hypothyroidism after tumor resection led us to hypothesize that this infant had consumptive hypothyroidism.
To test this, we used high-performance liquid chromatography to assay deiodinase activity in this patient's frozen tumor tissue. This revealed authentic D3 activity in the tumor, evidenced by a low nanomolar Km for T3 and a maximal velocity of 0.8 fmol T3 deiodinated per mg of tissue per minute.
The documentation of tumoral D3 activity and resolution of hypothyroidism following resection implicates consumptive hypothyroidism as the cause of this child's CH. Although the specific D3 activity in this tissue was only moderate, this is to our knowledge the first report of D3 expression in human fibrosarcoma and warrants further study of D3 expression and clinical thyroid status in this cancer.
Large fibrosarcoma of the hand, prior to surgical resection

Thyroid Hormone Metabolism & Regulation Saturday Poster Clinical
Absorption of oral L-thyroxine (L-T4) therapy is influenced by several factors, including the age of the patient, adherence to therapy, dietary habits, absorption kinetics, malabsorption, and interference of other drugs. A potential concern in patients with autoimmune atrophic gastritis is the drug malabsorption.
In this work, we show reversible normalisation of serum thyroid-stimulating hormone (TSH) levels in five patients with autoimmune atrophic gastritis, previously treated with L-thyroxine in tablet formulation, switched to the therapy with L-T4 in oral liquid formulation.
TSH was significantly reduced after switching (with the same dosage, 30 minutes before breakfast) from oral tablets to a liquid formulation (TSH, evaluated 1–3 months after the switch, decreased: from 6.1±4.2 to 2.9±2.7 mcIU/mL, p<0.05). The switch back to tablets (with the same dosage, 30 minutes before breakfast) caused thyrotropin levels to worsen. This fact leads us to believe that absorption of thyroxine is greater with oral liquid formulations in these patients.
In conclusion, we report five patients with autoimmune gastritis, in whom oral liquid L-thyroxine induced a reversible normalisation of thyrotropin levels. The obtained results suggest that the L-T4 oral liquid formulation could circumvent the pH alteration resulting from autoimmune atrophic gastritis.
Thyroid Hormone Metabolism & Regulation Saturday Poster Clinical
Drug malabsorption is a potential concern after bariatric surgery.
Here, we present 10 cases of hypothyroid patients (7 females, 3 males; age 34–57 years) who were well replaced with thyroxine tablets (for >1 year) to euthyroid thyrotropin (TSH) levels prior to surgery (seven Roux-en-Y gastric bypass; three biliary pancreatic diversions). These patients developed elevated TSH levels after the surgery (from 2 to 7 months later).
TSH was significantly reduced after switching (with the same dosage, 30 minutes before breakfast) from oral tablets to a liquid formulation (TSH, evaluated 1–3 months after the switch, decreased: a- gastric bypass, from 5.2±3.9 to 2.4±2.5 μIU/mL, p<0.05; b- biliary pancreatic diversion, from 7.7±1.7 to 4.1±1.8 μIU/mL, p<0.05).
These results suggest that the L-T4 oral liquid formulation could circumvent the malabsorption after bariatric surgery.
Autoimmunity Saturday Poster Basic
Interferons (IFNs) and tumor necrosis factor-α (TNF-α) cooperate in activating several inflammation-related gene in chronic inflammation in autoimmune thyroid diseases (AITD). The positive signaling of IFNs to activate gene expression in AITD is known, while the mechanisms by which IFNs negatively regulate genes remain less studied. While IFNs inhibit (C-X-C motif) ligand 8 (CXCL8) chemokine secretion in several human cell types, their effects on thyroid and orbital cells in Graves' disease were not evaluated. We aimed to investigate the interplay between TNF-α and type I or type II IFNs on CXCL8 secretion by these cells.
The CXCL8 secretion was tested in supernatants of primary cultures of thyroid cells, and orbital fibroblasts and preadipocytes both basally and after a 24 h incubation with TNF-α.
CXCL8 was detected in all cell types supernatants in basal conditions being significantly increased by TNF-α. Twenty-four hours incubation with IFN-γ or IFN-β or IFN-α dose dependently and significantly inhibited both basal and TNF-α-induced CXCL8 secretion. The degree of the inhibitory effect was IFN-γ>IFN-β>IFN-α.
We demonstrate that type I and type II IFNs downregulate both basal and TNF-α-induced CXCL8 secretion in human thyroid and orbital cells in Graves' disease, IFN-γ being the most powerful inhibitor.
Thyroid Hormone Metabolism & Regulation Saturday Poster Clinical
Assess metformin treatment effects on thyroid function, and its impact on serum TSH and Thyroid hormones value in patients with PCOS diagnosis and no previous treatment of comorbidities.
A total of 31 patients, over the age of 18, attended the Hospital Universitario de Caracas (July-October 2013), with PCOS diagnosis. TSH, fT4 and fT3 serum levels were quantified before and after giving metformin: 1 gr daily dose for 2 months.
All patients included in our study presented mean TSH values of 2,15±1,16 UI/L before starting treatment, with significant reduction on TSH after using 1 gr of metformin during 2 months (TSH: 1,50±0,63 UI/L, p<0,001). Likewise, changes in fT4 and fT3 were observed after treatment with metformin (fT4: before treatment: 1,05±0,14 ng/dL vs after treatment: 0,93±0,09 ng/dL, p<0,0001, and f3T: before treatment: 3,21±0,56 pg/dl vs. after treatment 2,67±0,37 pg/dl; p<0,0001). No significant changes were observed in thyroid antibody (anti-TPO) values.
Apparently, metformin enhances thyroid hormones actions not only in peripheral tissues but also in the pituitary. The contributions of this study must be considered when giving pharmacological treatment to patients with PCOS and overt or subclinical hypothyroidism, where metformin, one of the most used drugs, could diminish TSH without prescribing levothyroxine. It is also important to note that this is the first study that describes a reduction of TSH in euthyroid patients with PCOS and also to observe a diminishment in free TH. This could be related to ethnicity, duration of treatment and requires further investigation on larger cohorts and different populations.
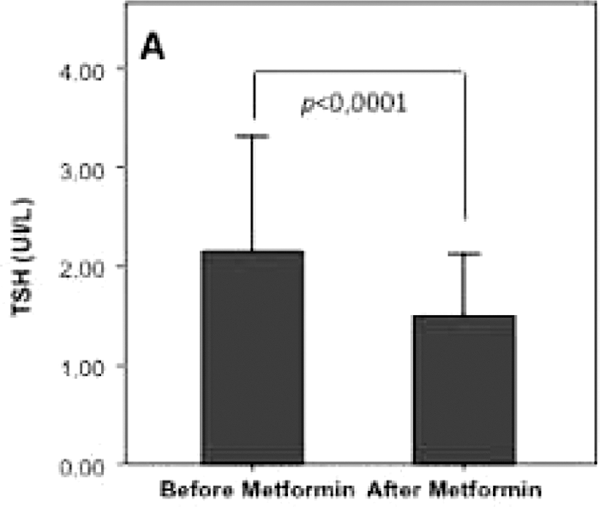
Thyroid Imaging Saturday Poster Clinical
To assess the presence of contralateral malignancy in preoperative papillary thyroid microcarcinoma (PTMC) patients, no other study has employed a prospective ultrasound (US)-based diagnosis. We aimed to assess the usefulness of US-based diagnosis to predict whether contralaterally located, dominant thyroid nodules are malignant or benign in known PTMC patients.
We studied 143 primary PTMC patients who underwent preoperative thyroid US. Each dominant thyroid nodule was prospectively classified into 1 of 5 diagnostic categories by a single radiologist: benign, probably benign, borderline, possibly malignant, and malignant. We calculated the efficacy of US diagnosis for contralateral malignancy by using the histopathological or long-term US follow-up results as a reference standard.
Of the 143 primary PTMCs, 17 displayed satellite PTMCs; hence, bilaterality of all PTMC patients was 11.9% (17/143). Real-time US of the contralateral thyroid yielded no thyroid nodule (n=55) and benign (n=52), probably benign (n=10), borderline (n=13), possibly malignant (n=4), and malignant (n=9) nodules. When the borderline US class was excluded, the sensitivity, specificity, positive and negative predictive values, and accuracy of US diagnosis for detecting contralateral malignancy were 86.7%, 100%, 100%, 98.3%, and 98.5%, respectively. Within individual US classes for the dominant thyroid nodules, the diagnostic accuracies of US class IV and V were higher than those of other US classes.
The US-based diagnosis may be helpful for detection of contralateral malignancy in preoperative PTMC patients.
Thyroid Imaging Saturday Poster Clinical
As the gold standard surgical treatment of primary hyperparathyroidism (PHPT), bilateral neck exploration (BNE) has a cure rate reported between 94% and 98%. After the introduction of localizing imaging modalities and with the use of intraoperative parathyroid hormone monitoring (IoPTH), minimally invasive parathyroidectomy (MIP) has become more popular with cure rates approaching BNE levels. Although IoPTH can prevent missing multiple adenomas and help the surgeon confirm intraoperative cure, it is an added cost and often extends surgical times. To our knowledge, MIP utilizing preoperative imaging with sestamibi scintigraphy (MIBI) and multidetector computed tomography (MDCT) without the use of IoPTH has not been previously reported.
We present a retrospective cohort study from prospectively collected patient data at a tertiary care endocrine surgery unit in Canada. One hundred fifteen consecutive patients with a first diagnosis of PHPT were included. Patients were booked for MIP if either MIBI or MDCT localized an adenoma but converted to BNE if a false positive was encountered. Demographics, preoperative imaging and investigations, surgical care, final pathology and cure were compared. GraphPad Prism was used to carry out statistical analyses.
Overall cure rate one year from surgery was 98.3%. Of the 115 patients, 71% underwent MIP. When only MDCT was positive (66%), 80% of patients avoided a BNE (p<0.0001, CI 47.9–73.2). In cases where only MIBI was positive (35%), 93% of patients avoided BNE (p<0.0001, CI 73.5–96.5).
In a tertiary care endocrine surgery unit in Canada, MIP without IoPTH is an effective operation with an acceptable cure rate of over 98%. While MDCT and MIBI are both employed for localization, MDCT remains more sensitive and predictive. In the cost-aware culture of the Canadian health care system, carefully selected MIP without IoPTH should be considered an established treatment option for patients with PHPT.
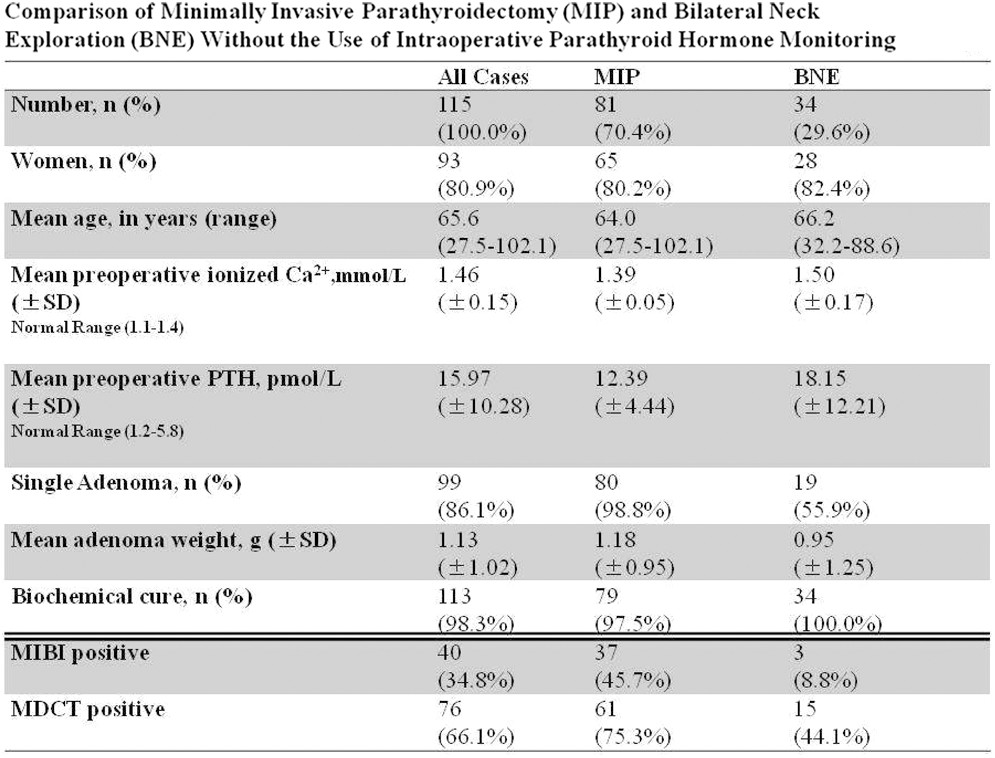
Thyroid Imaging Saturday Poster Clinical
Biochemically confirmed primary hyperparathyroidism (PHPT) can be treated with the gold standard bilateral neck exploration (BNE) for a cure rate of 94% to 98%. Currently, this more invasive approach has been largely avoided with the preferred modality being a focused approach using preoperative imaging to confirm disease localization. In order to minimize dissection in the neck, the surgeon must have reliable evidence of the location of parathyroid disease within the neck before completing a minimally invasive parathyroidectomy.
We present a retrospective cohort study of 115 consecutive patients from a prospectively collected database in a tertiary care endocrine surgery referral center in Canada. Patients had both Sestamibi scintigraphy (MIBI) and Multidetector Computed Tomography (MDCT) for preoperative localization of a parathyroid adenoma. Patients with a diagnosis of PHPT were included and exclusion criteria included previous parathyroid surgery. Demographics, surgical outcome and pathology were correlated with imaging. Intra-operative parathyroid hormone assay was not employed. GraphPad Prism was used to carry out statistical analyses.
The sensitivity of MDCT and MIBI were 84% and 40%, respectively (p=0.00012). Overall cure rate was 98% at 1 year follow-up; 98% when preoperative MIBI was positive and 99% when MDCT was positive. MDCT localized a correct pathological adenoma in 66% of cases independent of MIBI. MIBI was positive in 38.4% of cases and was associated with finding a significantly heavier adenoma at surgery (1.42 g vs 0.92 g, p<0.05).
In our center, MDCT is objectively more valuable than MIBI in localizing parathyroid adenomas upon initial evaluation of patients with PHPT. MIBI is helpful when positive, although this is rarely the case. Within the context of a high throughput endocrine surgery center, further investigation into preoperative localization using only MDCT should be explored.
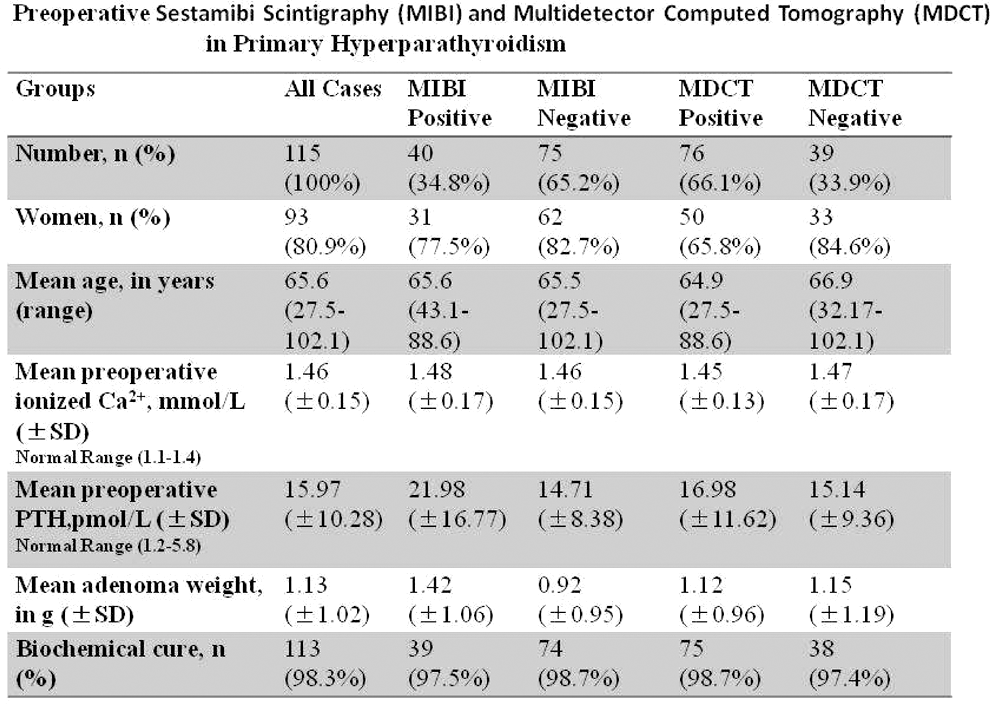
Thyroid Imaging Saturday Poster Translational
Poorly differentiated thyroid cancers (PDTC) that lose iodine uptake ability, in most cases still express TSH receptors (TSHR). Aim of our study was to radiolabel superagonist recombinant human TSH (rhTSH) analogues for imaging PDTC. In particular, we performed a comparison between TR1401 and TR1402 analogues with higher affinity for the TSHR respect to endogenous TSH.
Both analogues were labeled with 99 mTc using an indirect method via HYNIC conjugation. In vitro quality controls included SDS-PAGE, cysteine challenge and cell binding assay on TSHR positive cell lines JP09 and ML-1 human thyroid cancer cells lacking Na/I symporter. In vivo studies included tumor-targeting experiments in 40 athymic nude CD-1 mice bearing TSHR+ xenografts and TSHR- cells (JP02) as control. Additionally, we performed a comparison among labeled TR1401, TR1402, 131I and 18F-FDG in 2 dogs with spontaneous thyroid cancer.
Superagonist rhTSH analogues TR1401 and TR1402 were labeled with high labelling efficiency (>95%) and high specific activity (9250 MBq/mg). The labeled molecules retained biological activity and structural integrity. Calculated Kd constants confirmed an affinity for the TSHR from 10 to 50 times higher than endogenous TSH. In tumor targeting experiments, a focal uptake of radiolabeled analogues was observed in TSHR+ cells with a target-to-background ratio up to 3 at 3 h p.i., whereas no significant uptake was observed in mice bearing TSHR- cells. Similar observations were made in dogs with spontaneous intra-glandular papillary thyroid cancer, in which TSHR expression was confirmed by immunohistochemistry.
We were able to efficiently radiolabel novel rhTSH analogues with 99 mTc with retention of in vitro and in vivo binding capacity to TSHR. These new radiopharmaceuticals open new perspectives for pre-surgical TSHR-based staging of thyroid cancer, for diagnosis of radioiodine negative cancer remnants, local relapses and/or distant metastases, as well as for diagnosis of differentiated intra-thyroidal thyroid cancer. In addition these data suggest for the first time that the TSHR may be initially upregulated in thyroid cancer in response to loss of the most labile symporter function.
Thyroid Nodules & Goiter Saturday Poster Clinical
In the case of a non-diagnostic fine-needle aspiration (FNA) biopsy result, recent guidelines from the Bethesda System recommend repeat FNA after three months to prevent false-positive results. We aimed to examine our data to determine whether the three-month period affects the diagnostic yield of repeat biopsies.
A retrospective review of patient records over a six-year period at our institution was performed. Patients who required repeat FNA due to non-diagnostic yield were included. The time between the FNA biopsies, adequacy of the FNA specimens, as well as the surgical pathology diagnosis, were analyzed.
We identified 323 patients who required a repeat FNA. 100 (31%) patients had a repeat FNA less than three months apart; while 223 (69%) patients had a repeat FNA greater than three months apart. 105 patients were referred to our clinic with an initial inadequate biopsy result from an outside source. Repeat FNA was non-diagnostic in 36 patients (11.15%) of the total study population. There was no difference in satisfactory diagnostic yield between repeat FNAs performed greater than three months (91.03%) or less than three months (84.00%) after the initial biopsy (p=0.0634). Of the 36 patients with repeat non-diagnostic biopsy, 17 patients underwent diagnostic lobectomy, 3 (17.6%) of them found to have malignant disease.
The timing of repeat sampling of FNAs does not affect diagnostic yield of the repeat FNA. Patients with suspicious thyroid nodules could therefore receive a repeat FNA as soon as needed, rather than waiting three months. This could alleviate stress on patients with benign nodules and expedite surgical intervention in patients with proven malignancy on repeat biopsy.
Thyroid Nodules & Goiter Saturday Poster Clinical
The Bethesda criteria are proposed for appropriate stratification of malignancy risk in thyroid nodules, but controversy exists regarding their accuracy and reliability in decision making. Additionally, previous studies have suggested higher rates of both malignancy and false negative FNA's associated with increasing nodule size. This study aims to determine the accuracy of ultrasound (US)-guided fine needle aspiration biopsy (FNA) using the current Bethesda criteria in surgical practice. We also aimed to investigate the relationship between nodule size and malignancy.
A retrospective analysis of US-guided FNAs by a single surgeon during a 6 year period. FNA results using Bethesda criteria were compared to final surgical pathology.
611 patients with thyroid nodules underwent US-guided FNA. FNA results in 375 subsequently excised thyroid nodules were recorded according to the Bethesda criteria: 192 (51%) benign, 65 (17%) atypia of unknown significance (AUS), 42 (11%), suspicious for follicular neoplasm (SFN), 17 (5%) suspicious for malignancy (SM), 28 (8%) malignancy, and 31 (8%) non-diagnostic. Malignancy was confirmed by surgical pathology in 17%, 34%, 50%, 88%, 100%, and 39% of the above groups respectively. Sensitivity, specificity, and false-negative rate were 67%, 90%, and 17% respectively. No correlation existed between indeterminate nodule size and malignancy rate (p=0.72), or non-diagnostic nodule size and malignancy rate (p=0.72).
The proposed Bethesda risk stratification system underestimated malignancy rates in these cytopathologic categories: benign, AUS/FLUS, non-diagnostic and SFN. There was no positive correlation between nodule size and malignancy rate in any of the cytopathologic categories.
Withdrawn
Thyroid Nodules & Goiter Saturday Poster Clinical
The purpose of this study was to evaluate character of histological changes after the applying of bipolar radiofrequency ablation (RFA) on different thyroid lesions, surgically removed in Belarus and Ukraine.
Surgically removed thyroid gland was routinely processed and nodules were sliced in two parts - one was the subject for histological diagnosis according to the principles that universally applied in surgical pathology, the other one was used for the RFA procedure. Eighty-eight lesions with hyperplastic nodule (40), follicular adenoma (36), and papillary carcinoma (12) were subjected to RFA of certain power of current and exposure time. The study has been done using thyrablator bipolar handpiece and Elmed BC 50 Bipolar Coagulator. The volume of the nodules and ablated tissue were calculated by the formula V=(3.14*A*B*C)/6)/taking A and B sizes directly from histology and C was an approximated third size of the nodule.
Optimal result vaporization without carbonation was achieved with a power of 25 watts applied for 10 seconds. Gross examination revealed a whitish focus, rather dry, tight, or flabby. Microscopic changes varied but shrinkage of follicles, necrotic foci, karyolysis or karyopyknosis of thyrocytes, connective tissue thickening were usual. Contracture of blood vessels was also revealed. Such changes were more manifested in cellular than in colloid lesions. Complete destruction was achieved between electrodes whereas a few millimeters apart, necrobiotic cell changes prevailed and stromal reaction was mild. In general group, after the RFA procedure, the volume of ablated tissue was 0.12 ml (41.2%). The volume of ablated tissue in cellular lesions vs colloid lesions was a same: 0,12 (41,9%), and 0,12 ml (40,7%) respectively. The volume of ablated tissue in lesions sized up to 1 cm in diameter vs. such one more than 1 cm was 0,08 ml, (56,6%), 0,15 (30,5%) respectively (P<0.05).
Therefore, morphological features of the effectiveness of RFA were more significant for thyroid lesions sized up to 1 cm in diameter than for ones bigger size.
Thyroid Nodules & Goiter Saturday Poster Clinical
An association between insulin resistance or the Metabolic Syndrome (MS) and thyroid nodular disease has been recently described. Our hypothesis is that MS, highly frequent in elderly population, could be a risk factor for proliferation activity of the thyroid gland in aged population. Therefore our aim was to evaluate which metabolic parameters in elderly patients with MS are associated to thyroid enlargement or increased prevalence of thyroid nodules.
Seventy seven patients >65 years with MS were included. We evaluated the presence of thyroid nodules and thyroid volume by ultrasonography and several biochemical, metabolic and anthropometric parameters. Only patients with TSH between 0.3–6 mU/L were included. We further divided subjects into 2 groups: DM2 and Non DM2 and established comparisons between them. For statistical analysis we used Linear Correlation, Spearman correlation, Student t test, and ANOVA.
Among all parameters analysed we found a significant correlation between HbA1C and volume (r=0.261, p=0.027) or number of nodules (r=0.266, p=0.023). As expected HbA1C also correlated with glycemia, log-HOMA, Quicki and microalbuminuria (r=0.644, p=0.000; r=0.238, p=0.037; r=−0.253, p=0.026; r=0,456, p=0.000 respectively). Neither sex, age, BMI, metformin nor levothyroxine use were associated to thyroid volume or nodularity. Regarding TSH levels, surprisingly, a negative correlation between TSH and thyroid volume was observed (r=−2.81, p=0.013). Within the whole cohort, those patients with DM2 had larger thyroid volumes compared to non DM2 (Median (CI): 6.976 (5.220–10.789) vs 5.034 (3.796–6.034) ml, p<0.008). Furthermore, a larger proportion of DM2 patients presented thyroid volumes >5.8 ml (69 vs 23%, p<0.001; Odds ratio: 7.25 (CI: 2.04–25.56)).
In elderly patients with MS, worse metabolic control, represented by higher HbA1C levels, was found associated to increased prevalence of thyroid nodules and larger thyroid volume. Moreover, within the whole MS group, patients with DM2 had the largest thyroid volumes.
Levels of HbA1c correlated significantly with thyroid volume and number of nodules
Thyroid Nodules & Goiter Saturday Poster Clinical
Primary hyperparathyroidism is a systematic disease of calcium metabolism due to primary cause of parathyroid gland. Commonly it occurs due to chief cell adenoma and less common due to hyperplasia. In this report we are describing very rare causes of primary hyperparathyroidism.
The files of Department of Pathology, Farwaniya Hospital were searched for the cases; the pathology reports and histological slides were reviewed. The clinical records of all patients we reviewed for clinical
Four female patients were identified. All patients were adults and the age range was 39–62. One patient presented with peptic ulcer disease with bone pain. Laboratory tests revealed high levels of parathyroid, Gastrin and Prolactin hormones in keeping with MEN I. Pathological examination showed a parathyroid cyst. A second patient presented with severe bone pain involving the knees and legs. Laboratory tests showed hypercalcemia with very high level of parathyroid hormone (62.8 pmol/L). The parathyroid examination revealed 6.0 cm mass with vascular and capsular invasion diagnostic of a parathyroid carcinoma. The other two patients presented also with asymptomatic hypercalcemia with elevated parathyroid hormone. Pathological examination uncovered a diagnosis of oncocytic adenoma in one patient and lipoadenoma in the other.
This report describes very rare causes of primary hyperparathyroidism. Functional parathyroid cyst is very rare and to arise in context of MEN I is extremely rare with one previous case report. Parathyroid carcinoma also is extremely rare cause of hyperparathyroidism. Lipoadenoma and oncocytic adenoma are arising from cells, physiologically not secret parathyroid hormone.
Thyroid Cancer Saturday Poster Clinical
Thyroid cancer is the fifth most common cancer in Kuwait, estimated to be 5.6% of all cancers. Farwaniya Health Region reported the highest incidence of thyroid cancer among Kuwaiti nationals approximately 23% of all cases in Kuwait and the second for non-Kuwaiti. Clinico-pathological analysis for these cases is not available; hence, we conducted this study.
Cases of well differentiated thyroid cancercinoma more than 1.0 cm in size and diagnosed between 2006 and 2013 were retrieved from the electronic files of the Department of Pathology, Farwaniya Hospital. Pathology reports and histological slides were reviewed to confirm the diagnosis and to identify prognostic factors. Clinical charts and electronic files of patients were analyzed for demographic features, clinical presentation, imaging studies, surgical procedures and complications.
Seventy-six cases of WDTC were identified, 53 cases (69.7%) were females and the patients' age ranged 24–59. The most common clinical presentation was neck swelling, documented in 54 cases (87%) followed by incidental diagnosis (6.4%). Thyroid function was normal in majority of cases (93%). The majority of patients underwent total thyroidectomy (59%) followed by lobectomy (23%). Fourteen patients (18.4%) developed post-operative complications; the most common complication was transient hypocalcemia detected in 10 patients. Pathological diagnosis revealed 73 cases to be papillary carcinoma (96%) and 3 cases as follicular carcinoma (4%). Fourty eight cases (63%) were uni-focal tumors. Follicular variant of papillary carcinoma was the most common histological variant, seen in 45 cases (59%) followed by the classical variant seen in 23 cases (30%). The most frequent pathological stage was pT2 NXMX.
Analysis of WDTC cases in Kuwait revealed that WDTC is more common in females and neck swelling is the most common clinical presentation. Incidence of thyroid follicular carcinoma is markedly decreased, reflecting the awareness of nuclear morphology of papillary carcinoma. Post-operative complications are not uncommon and hypocalcemia is the most common.
Disorders of Thyroid Function Saturday Poster
We present a case of severe thyrotoxicosis in a patient with chronic lymphocytic leukemia.
A 60 year old male with CLL presented to the emergency department with fatigue, weakness, and fever to 102.5 degree Fahrenheit. He had received recent chemotherapy with bendamustine and rituximab. He described weight loss of 20 pounds over 2 months. He developed neck pain one week prior to admission. On presentation, he had left-sided neck swelling that was painful to touch. The patient was admitted to the hospital with neutropenic fever.
Due to worsening tachycardia and ongoing hyperthermia, thyroid function tests were ordered and the patient was found to have an elevated free T4 level of 6.73 ng/dL and a TSH level was 0.007 mIU/L. Endocrine was consulted and he was started on hydrocortisone, methimazole, and propranolol. A repeat free T4 level was more than 8 ng/dl, and a total T3 level, after steroids had already been started, was 244 ng/dL. An I-123 thyroid scan and uptake was requested, but contrast CT imaging was necessary, and ultimately the patient became too unstable to complete the study. CT imaging showed lymphomatous nodules throughout the lungs, spleen, liver, kidney and thyroid gland. On repeat CT scan to investigate for a neck abscess, new hypoattenuating lesions/infiltration within the thyroid gland were seen bilaterally. Methimazole therapy did not lower the patient's free T4 level (>8.0 ng/dL), although the T3 levels remained stable at 220 ng/dL (normal 60–180 ng/dL). In addition to the lack of response to thionamides, the patient developed a severe transaminitis (ALT and AST >500 U/L). A serum thyroglobulin level returned at 4880 ng/ml. Charcoal hemoperfusion or plasmapheresis was recommended instead of methimazole. Unfortunately, the patient suffered a fatal cardiac arrest. An autopsy was not performed.
This case likely illustrates a rare consequence of CLL, namely thyroiditis due to infiltration of the thyroid gland by leukemia cells. Other potential etiologies for the patient's thyrotoxicosis were suppurative thyroiditis and chemotherapy induced thyroiditis. Discordance between free T4 and T3 levels and failure to lower free T4 levels with thionamides were indications of thyroiditis.
Free T4, Total T3 and TSH trend

Disorders of Thyroid Function Saturday Poster
Thyrotoxic hypokalemic periodic paralysis (THPP) is an uncommon condition characterized by the triad of hyperthyroidism, flaccid paralysis and hypokalemia.
We report 2 cases of THPP with different etiology for their hyperthyroidism and precipitant for their hypokalemia.
Case 1 is a 33 y Philippino male with proven first presentation of Grave's disease (fT4 36.5 pmol/l, TSH<0.005 mIU/l, TRAB 2.7) presenting with acute weakness of both legs following a period of intensive exercise and with a serum potassium of 2.5 mmol/l. After correction of acute hypokalemia, his thyroid was controlled medically before definitive treatment with radioactive iodine. Case 2 is a 27 y Chinese man presenting with acute quadriparesis and severe hypokalemia (1.5 mmol/l). His drug history was significant for anabolic steroids, Triiodothyronine (125 mcg/d) and Clenbuterol (oral Beta 2 agonist). His biochemistry was in keeping with thyrotoxicosis factisia (fT4 1.8 pmol/l, fT3 7.1 pmol/l and TSH<0.005 mIU/l) and THPP was felt likely from a combination of T3, Clenbuterol and recent increase in carbohydrate content of his meals. He made a full recovery after correction of his hypokalemia and withholding of drugs although has defaulted from further follow up since.
We discuss the multiple postulated mechanisms that underlie the stimulation of skeletal muscle cell Na+/K+ ATP'ase that leads to acute and severe hypokalemia from intracellular shift in patients with hyperthyroidism irrespective of etiology. We also discuss novel genetic mechanisms that may underlie the prelediction of this condition to Asian males.
Disorders of Thyroid Function Saturday Poster
Radioactive iodine therapy (RAI) and thyroid replacement is the standard treatment for Grave's disease. Patients treated with RAI ultimately become hypothyroid despite differences in dosing regimens. Several factors such as age, gender, thyroid size, thyroid hormone levels, and pre-treatment antithyroid medication use, determine treatment effect.
We present a case of a 41 year-old patient with Grave's disease who required 3 doses totaling 116 mCi (4292 Mbq) of I-131 to obtain normal thyroid levels and symptom relief. The patient was diagnosed three years prior to his visit to our clinic in October 2012. He was taking Tapazole 30 mg twice daily and Atenolol 100 mg a day. The patient reported daily palpitations, excessive sweating, increased heat sensitivity, photophobia, and weight loss (45.3 kg over 1 ½ years). His blood pressure and heart rate were normal. He had an upper extremity tremor and anterior leg muscle weakness, slight periorbital edema, bilateral positive lid lag and stare. Thyroid exam revealed a symmetrical gland which was 4 times larger than normal. Initial labs were FT4 4.39 ng/dL and TSH 0.05 μIU/mL. Thyroid scan revealed diffuse homogenous Iodine-123 uptake of 51.6% at 24 hours. Patient was given 31.4 mCi of I-131 orally for therapy.
After several follow up visits the thyroid levels remained elevated at 2 to 3 times the normal range. The patient required two additional doses of 31 mCi and 54 mCi at 5 months and 13 months after the initial dose. 4 months after the last dose, thyroid levels were normal (FT4 0.53 ng/dL, FT3 2.3 pg/mL) but the TSH remained suppressed at 0.05 μIU/mL. Patient has had no complaints and remains clinically asymptomatic.
This is a unique case because of the unusually high amount of I-131 required for treatment. Patient characteristics that indicate reduced dose effect may have contributed to the need for higher dose. Identifying these factors at diagnosis may help guide dose determination for more effective and prompt treatment of hyperthyroidism. Abbreviations and Normal Values: FT4 (Free T4) 0.58–1.64 ng/dL; FT3 (Free T3) 2.5–3.9 pg/mL; TSH (Thyroid Stimulating Hormone) 0.34–5.6 μIU/mL.
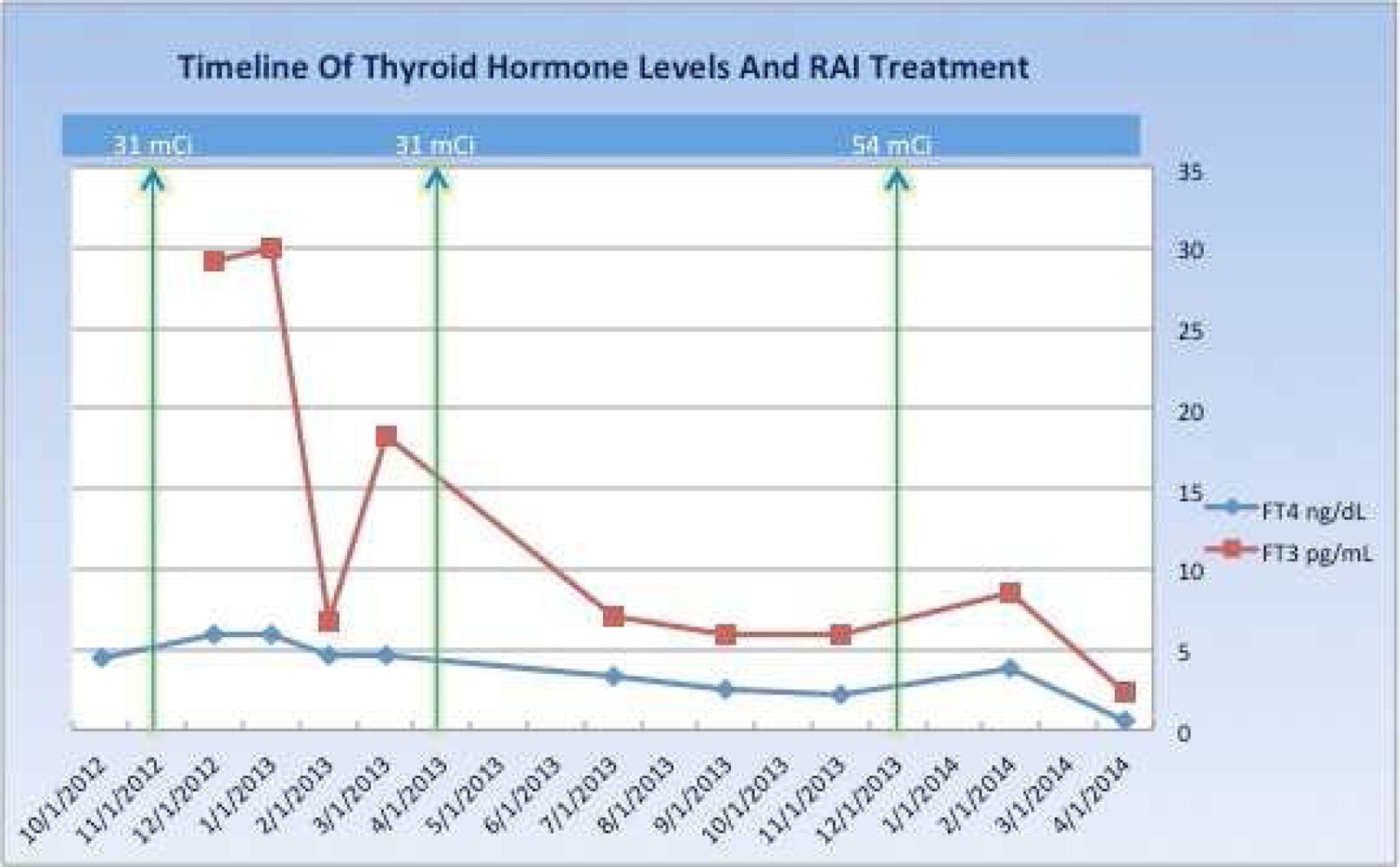
Thyroid & Development Saturday Poster
Ectopic thyroid tissue is a rare developmental defect of the thyroid gland embryogenesis, during its passage from the floor of the primitive foregut to its final pre-tracheal position. Lingual thyroid is the most common presentation of thyroid ectopy. Ectopic thyroid tissue in other locations, including the anterior mediastinum, is rare. It is more common in females and especially in Asian origin. There is no consensus on the management of ectopic thyroid tissue.
51 year old African American female presented to endocrinology clinic with an incidentally found anterior mediastinal mass and biopsy proven thyroid tissue. CTA was done initially for workup of SOB and chest pain which showed 3.3×4.4 cm anterior mediastinal mass. She denied radiation exposure, personal or family history of breast, colon or thyroid cancer, or thyroid disease. TSH 0.489 (0.400–4.00 uIU/ml), free T4 1.03 (0.71–1.51 ng/dl), TPO<6.0 IU/mL, and TSI <89. Thyroid Ultrasound showed non- enlarged normal cervical thyroid gland. Mediastinoscopy with biopsy revealed benign thyroid parenchyma consisting of thyroid follicles lined by benign cuboidal follicle lining cells, containing homogeneous eosinophilic colloid material. No atypia or malignancy. PET CT showed a heterogeneous, anterior mediastinal mass with similar activity as the remainder of mediastinum. In reviewing the literature, most incidental anterior mediastinal thyroid masses were removed by sternotomy, most of them are benign. When malignant, most are papillary carcinoma but follicular, hurthle cell and medullary have been described. After a discussion with the patient and our surgical team, the decision was to closely observe patient clinically and reimage periodically or if symptoms develop.
N/A
Ectopic thyroid tissue in the anterior mediastinum is rare, often found incidentally; can present with dyspnea, cough or hemoptysis. Very few cases are reported in American literature. Most of the mediastinal ectopic thyroids were surgically resected, with a very low malignancy rate so we opted for a conservative clinical approach. There is no consensus for management of ectopic thyroid tissue. We support FNA and imaging studies such as PET-CT, US to guide the management.
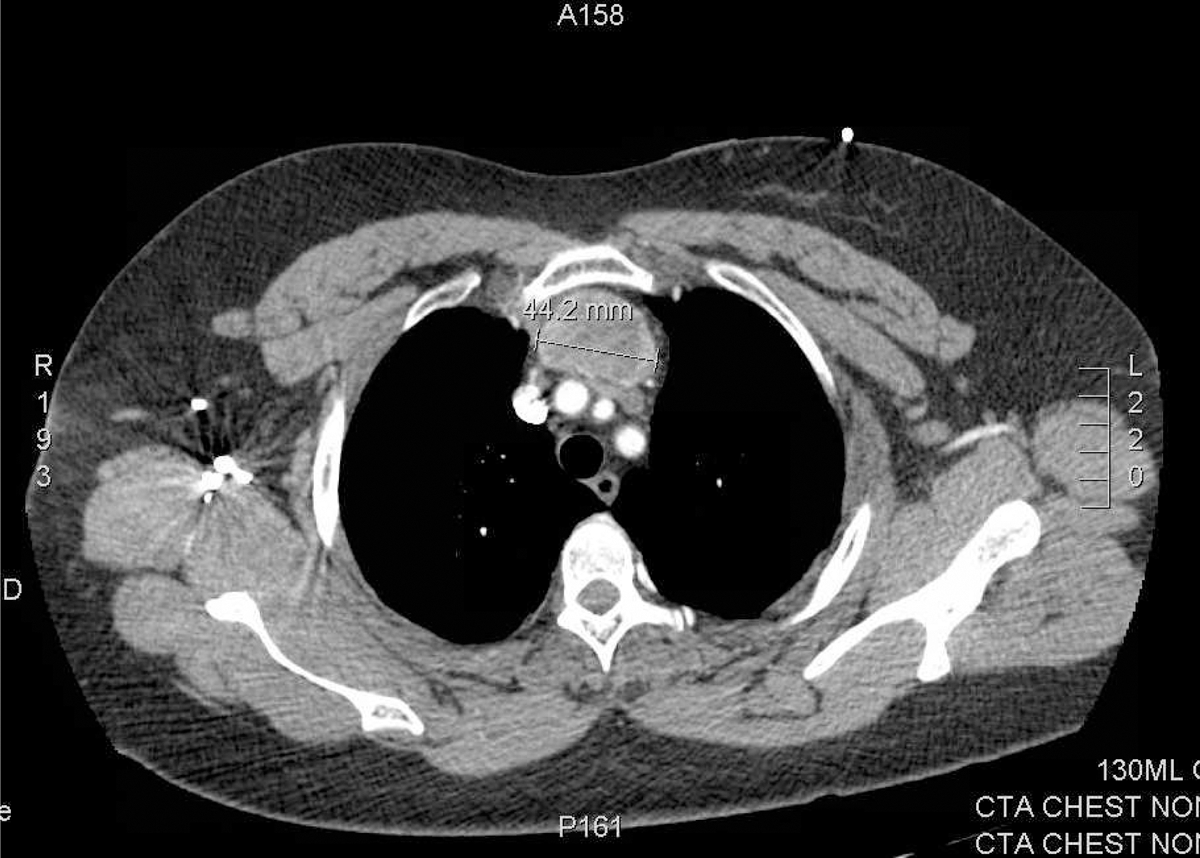
Thyroid Cancer Saturday Poster
Radioactive scintigraphy is used to establish the presence of local regional or metastatic disease in patients with well-differentiated thyroid carcinomas following radioactive iodine ablation. False positive I-131 scans post treatment have been described. Cases of false positive uptake due to inflammatory processes, other neoplasms, infections, meckels diverticulum or secretions have been reported. We present an unusual case of a 64 year old female with a history of a well-differentiated papillary thyroid carcinoma (T3N1aMx) with a 3.9 cm, right-sided classical and follicular variant lesion with capsular and lymphovascular invasion as well as a left 0.1 cm follicular variant microcarcinoma with 1/1 positive right central neck lymph nodes with extracapsular extension. The patient underwent a total thyroidectomy and radioiodine remnant ablation (RA-I-131; with 155.5 mCi). TSH was greater than 200 following recombinant TSH administration with undetectable thyroglobulin and thyroglobulin antibody levels. Post-treatment whole body scintigraphy demonstrated T9 spinal tracer uptake. (figure 1a). Further investigation of the spinal lesion with CT scan revealed a probable hemangioma (figure 1b), which was definitively confirmed with MRI (figure 1c). There are two previously reported cases of false positive uptake in spinal hemangiomas, one using I-131 and one using I-123. Previous reports alluded to intravascular blood pooling and/or transcapillary escape into the interstitial space as possible causes. When found, metastatic bone lesions alter staging as well as the therapeutic approach to patients with thyroid carcinoma. Given the high incidence of benign vertebral hemangiomas, present in 11% of the population, and the potential for false positives on scintigraphy, complete evaluation of lesions prior to restaging is imperative.
Figure 1a: NM Post-uptake scan Figure 1b: Above: Sag CT, Below: Axial CT Figure 1c: Above: Sag MRI, Below: Axial MRI
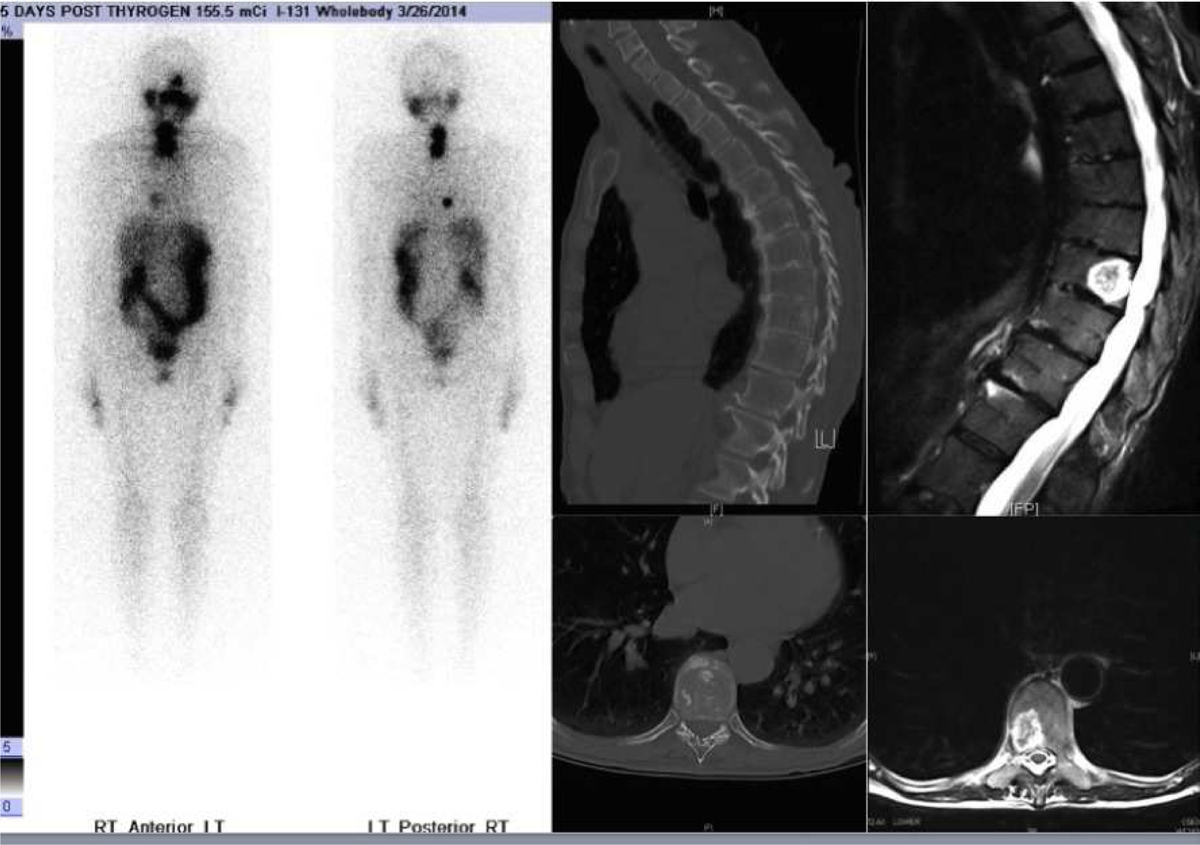
Thyroid Cancer Saturday Poster
Medulloblastoma is the most common brain tumor in children, but only 1% of those in adults. Treatment consists of surgery and radiation, with or without chemotherapy. Though the risk of thyroid disease after radiation therapy in childhood is well established, few studies discuss thyroid cancer in those treated for medulloblastoma as adults.
A 48 year old asymptomatic man presented with a painless neck mass for 6 months. At 37 he was treated with surgery and radiation for a medulloblastoma in the cerebellum. There was no family history of malignancy or thyroid disease. A hard mass was palpable in the right lobe of the thyroid gland. On ultrasound a 2 cm hypoechoic hypervascular nodule with microcalcifications in the right lobe had suspicious lymphadenopathy at level 3.
FNA of the right sided nodule showed hurthle cell features and architectural atypia. Cytopathology was non-diagnostic but gene expression classifier analysis reported a 40% risk of malignancy. He underwent total thyroidectomy and lymph node dissection, demonstrating pT1bN1bM0 papillary carcinoma up to 1.8 cm, followed by 30 mCi I-131 completion ablation. One year later there is no recurrence.
Children are more sensitive to carcinogenic effects of ionizing radiation, with a relative risk of developing radio-induced thyroid cancer decreasing with increasing age at exposure. The risk for thyroid malignancy after irradiation in adulthood is 9 times lower than in childhood. Among 27 adults with irradiated medulloblastoma, 1 developed thyroid carcinoma. A 28 year old treated with radiation for medulloblastoma died 14 years later of a brainstem infarct, with papillary thyroid carcinoma found at autopsy. A study of 37 children with medulloblastoma used I-thyroxine to suppress TSH before and during craniospinal irradiation; 70% of those adequately suppressed had hypothyroidism-free survival rates vs. 20% of those inadequately suppressed, indicating a protective effect. Future research should evaluate if TSH suppression decreases the risk of future malignancy. We present a rare case of thyroid carcinoma after radiation therapy for adult onset medulloblastoma. Routine surveillance for thyroid carcinoma should include yearly hormonal and ultrasound evaluation.
Pre-Operative Laboratory Studies
Thyroid Cancer Saturday Poster
A 40 year old previously healthy woman presented with one week history of neck mass, swelling, dyspnea, dysphagia, and ear pain. She denied family history of thyroid disease. On physical exam she had a soft but clear voice. There were no ocular abnormalities. Palpation of the thyroid revealed an anterior, edematous, nonerythematous, nontender, right sided 3.5 cm mass. The remainder of the exam was normal. Thyroid function panel was normal (TSH 2.130 mcunit/mL and FT4 1.04 ng/dL).
Neck ultrasound showed an enlarged right lobe containing a complex 4.0×3.6 cm heterogeneous cyst. Another 2.1×2.1×2.2 cm hypoechoic complex cyst was also noted in the same lobe. The left lobe had an homogenous echotexture and sub-centimeter nodule without worrisome features. Soft tissue CT scan of the neck showed severe edema surrounding the right thyroid extending to the superior mediastinum. There was a 3.4 cm cystic fluid collection along the inferior margin of the right thryoid lobe. There was evidence of mass effect with prominent shift of the airway to the left.
The patient underwent right thyroid lobectomy for compressive symptoms. Pathology showed a 2.5 cm clear cell neoplasm with immunostaining profile suggestive of metastatic renal cell carcinoma as well as a 1.8 cm follicular oncocytic adenoma. One month later, the patient underwent CT scan of the chest, abdomen, and pelvis with IV contrast which returned negative for any renal mass.
Metastases to the thyroid gland are rare. When they do occur, most cases are secondary to metastatic implants of renal carcinoma (50%). Here we described an unusual case of renal cell carcinoma metastasis to thyroid gland, with a CT scan negative for any renal mass and found to have a concomitant thyroid oncocytic follicular adenoma.
Thyroid Hormone Action Saturday Poster
Resistance to thyroid hormone is a rare condition caused by tissue refractoriness to the effects of circulating thyroid hormone, and may be misdiagnosed as hyperthyroidism. This syndrome is characterized by elevated circulating thyroid hormones, and unsuppressed TSH levels. Although most patients are euthyroid, rarely they may present with clinical hyperthyroidism, if the pituitary gland is more insensitive than other tissues to thyroid hormones. In this study we present a case of thyroid hormone resistance with clinical evidence of hyperthyroidism.
We present a case of 58 year old male who suffered from thyrotoxicosis for many years.
A 58 year old male who had diarrhea for many years and had been under treatment for atrial fibrillation with rate control medications. He had been tested for thyroid function in the past which revealed elevated fT3 and fT4 with slightly elevated TSH concentration. Pituitary adenoma was excluded as magnetic resonance imaging showed normal pituitary gland, alpha subunit was within normal range and TSH concentration increased after TRH administration. Sonography revealed normoechogenic, slightly enlarged thyroid gland. Methimazole had been tried in the past without any significant improvement. The diagnosis of thyroid hormone resistance was made and he was started on bromocriptine at a dose of 10 mg per day. After 2 months of treatment he achieved a state of constant euthyrosis and following next few months thyroid volume diminished.
In this case report we emphasize the importance of timely diagnosis of thyroid hormone resistance, which prevents many patients from being wrongly diagnosed as Graves disease and therefore various inappropriate treatments. Also, we present a successful treatment of this rare condition with bromocripten.
Thyroid Nodules & Goiter Saturday Poster
We describe the case of a 38 year-old woman with history of suprasellar mass complicated by diabetes insipidus (DI), hypogonadotropic hypogonadism, and central hypothyroidism who presented with subacute onset of goiter associated with dysphagia. Work-up for goiter lead to diagnosis of systemic Langerhans cell histiocytosis (LCH).
Patient has been followed at our institution with physical exams, blood work, imaging and biopsies.
On physical exam, she was euthyroid, and a bilaterally enlarged non-tender thyroid was palpable. On thyroid ultrasound the right lobe measured 7.3×2.9×3.4 cm and the left lobe measured 5.8×2.3×2.5 cm; replacement of almost the entire thyroid with an abnormal hypoechoic tissue with increased vascularity was identified. Thyroid FNA showed atypical mononuclear cells of histiocytic origin raising the possibility of LCH. An open thyroid biopsy confirmed the diagnosis of LCH. Pathology from prior suprasellar mass biopsy was revised and showed cells suspicious for LCH. Oncologic evaluation was negative for skeletal, bone marrow, and gingival involvement. A PET/CT scan showed a markedly enlarged, FDG-avid thyroid (SUV 14.7) with increased FDG activity in the superior mediastinum likely due to thyroid extension, and FDG-avid level IIB lymph nodes. Her course was complicated by fungation of the tumor into the skin of the neck. She began two 6-week courses of induction therapy with vinblastine and prednisone followed by three cycles of vinblastine, methotrexate, 6-mercaptopurine and steroids. Follow-up PET/CT showed improvement of FDG-avid disease and decrease in thyroid size. Brain MRI also showed interval improvement in size of suprasellar lesion. She remains on stable doses of desmopressin and levothyroxine.
LCH is a rare disease with highly variable clinical presentation. Thyroid infiltration, especially associated with compressive symptoms, is an infrequent complication of this condition in adults. The association of new onset goiter in a patient with hypothalamic-pituitary disease, particularly DI, should prompt evaluation for this unusual condition. Diffuse FDG-avidity of the thyroid on PET/CT scan should be concerning for thyroid involvement in patients with LHC.
Thyroid Nodules & Goiter Saturday Poster
Approximately 23,500 cases of differentiated thyroid cancer are diagnosed each year in the United States with increasing incidence. Multinodular goiter carries the same risk of malignancy as solitary nodules. Radiation doses greater than 200 cGy to the neck region is associated with a 13-fold increased risk of thyroid cancer. On literature review, no cases were reported of thyroid cancer in nodules picked up on thyroid ultrasound but missed on radioiodine scan.
A 35-year-old woman was referred for evaluation of asymptomatic multinodular goiter. She was on Levothyroxine 50 mcg daily for hypothyroidism. She had a history of head and neck irradiation 15 years ago for Hodgkin's lymphoma. Her past history was unremarkable except for treatment of breast carcinoma with no evidence of recurrence. Her mother had hypothyroidism but no family history of thyroid cancer. Physical examination was normal except for nodular goiter with no cervical lymphadenopathy. Thyroid ultrasound revealed 2 nodules on the right lobe, 3 nodules on the left lobe and a 1.2 cm nodule on the isthmus. All nodules were hypoechoic, solid, with grade 1 vascularity and no calcifications or irregular margins. Largest nodule measured 2.2 cm on the right side. Radioiodine scan was ordered to identify cold nodules for fine need aspiration. Scan showed increased uptake in the 2 nodules on the right side and all nodules on the left side. On comparing the radioiodine images with the ultrasound pictures, the isthmus nodule was not detected on the radioiodine scan. A biopsy of 0.9×0.5×1.2 cm isthmus nodule revealed suspicious cells for malignancy. Total thyroidectomy is scheduled with pathology reports pending.
This case illustrates the potential benefits of using thyroid ultrasound in conjunction with radioiodine scan in patients with multinodular goiter as part of evaluation and management of thyroid nodules. This is especially important in patients with a history of neck irradiation, which increases the likelihood of malignancy.
Using thyroid ultrasound in conjuction with radioiodine scan increases the chances of detecting cold nodules. This is vital in patients with a history of head and neck irradiation due to increased likelihood of malignancy.