
Abstract

H
Although we take it for granted in 2014 that hypothyroidism can be easily treated with several thyroid hormone preparations, thyroid hormone replacement therapy was in its very early stages only a century ago. It is noteworthy that the publication of the Guidelines for the Treatment of Hypothyroidism coincides with the 100th anniversary of the crystallization of thyroxine (T4) by Edward C. Kendall (1886–1972) on Christmas day 1914 at the Mayo Clinic (4). This seminal discovery laid the basis for the synthesis of T4 by Sir Charles Harington in 1927 (5). The physiological role of the thyroid and the clinical entity of hypothyroidism, at that time called myxedema, had only been recognized in the late 19th century. In 1874, the British physician William Gull briefly described a “cretinoid state supervening in adult life in women” (6). This clinical entity was subsequently confirmed by William Ord in 1878 and he called it “myxoedema,” a “cretinoid” affection occasionally observed in middle-aged women (7). Ord also observed that the condition was associated with an atrophy of the thyroid gland. While none of the authors was aware of the causal role of the thyroid in the pathophysiology of the myxedematous condition, they emphasized its resemblance with cretinism. In 1882, Jacques and Auguste Reverdin, two surgeons from Geneva, Switzerland, presented a series of 21 total thyroidectomies and described the devastating consequences on the patients. They coined the term “myxoedème opératoire” and accurately described the hypothyroid phenotype resulting from total surgical removal of the thyroid (8,9). A few months later, Theodor Kocher from Berne, Switzerland, reported results on 200 thyroidectomies performed by several surgeons in Switzerland and Germany, 101 performed by himself, at the Congress of the German Society for Surgery in Berlin in April 1883 (10). He described the clinical picture developing after total thyroidectomy as “cachexia strumipriva.” To investigate the observations by Gull and Ord further, as well as the findings of the Swiss surgeons, the Clinical Society of London established a committee, which concluded in 1888 that myxedema, total thyroidectomy, and cretinism all result from “the annihilation of the function of the thyroid body” (11) (Fig. 1). The clinical signs and symptoms were described in great detail in the committee's report, but treatment was barely mentioned.
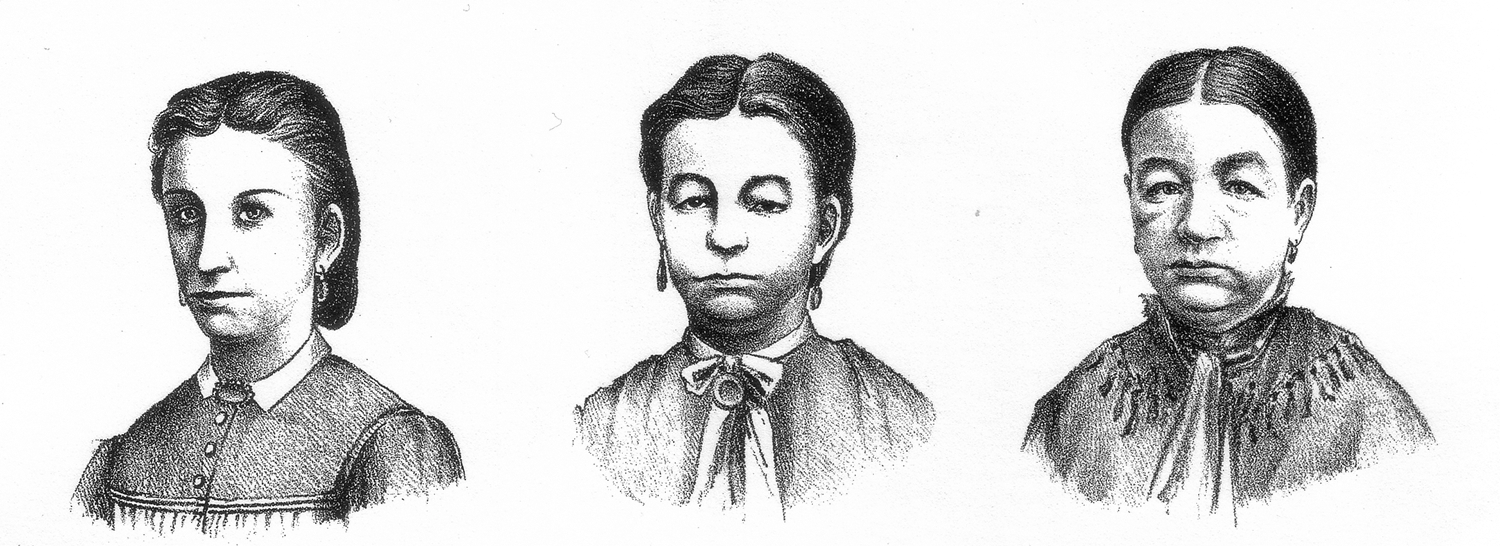
The first series of pictures of a woman with myxedema by William Ord. Left, at the age of 21 years, before onset of hypothyroidism; middle, at the age of 28 years; right, at the age of 32 years. From the report of a committee of the Clinical Society of London nominated December 14, 1883, to investigate the subject of myxoedema. Trans Clin Soc Lond. 21(Suppl):1–215, 1888 (11). The left and the middle panel were previously published in: Ord WM. On myxœdema, a term proposed to be applied to an essential condition in the “cretinoid” affection occasionally observed in middle-aged women. Med Chir Trans
The first treatment of hypothyroidism in humans was preceded by several transplantation experiments in animal models (12 –14). For example, Moritz Schiff, a German physiologist working in Berne, reported in 1884 that “thyroidectomy loses its danger, and an essential amount of its effect, if one previously introduces and fixes other thyroid glands from an animal of the same species in the abdominal cavity” (12). In a letter written in 1891, the eminent physiologist and neurosurgeon Victor Horsley informed George R. Murray about the progress in the quest to find a treatment for hypothyroidism (15). A few months later, Murray reported that the subcutaneous injection of a sheep extract into a hypothyroid human patient was indeed able to cure myxedema (16), an observation that was quickly confirmed by others (17). Thyroid extracts continued to be used as the primary treatment of hypothyroidism until the 1950s when T4, and in particular levothyroxine, gradually started to enter the clinical realm (18). Of note, levothyroxine is on the World Health Organization's List of Essential Medicines, a compendium of the most important medications for basic medical needs (19).
In the early 1950s, T3 was discovered by Jacques Gross and Rosalind Pitt-Rivers, as well as by Roche, Lissitsky, and Michel (reviewed in (20)). It was found to be more physiologically active, and it became apparent that T3 is responsible for most of the direct genomic effects. In healthy adult individuals, 80–90% of T3 is generated by deiodination of T4 through the type I and type II deiodinases, enzymes that are widely and differentially expressed in target cells (21). The identification of several thyroid hormone transporters that are expressed in a tissue-specific manner has added further complexity to our understanding of thyroid hormone action at the cellular level during the last few years (22). The intricacies of thyroid hormone metabolism, cellular uptake, and action suggest that these elements could, at least in some patients, have an impact on thyroid hormone replacement therapy (23).
The 2014 Guidelines for the Treatment of Hypothyroidism provide a comprehensive overview on the current evidence about treatment modalities for patients with hypothyroidism and a solid review of the literature that has accumulated to date (3). Importantly, the guidelines also highlight existing gaps in our knowledge, and they identify areas in need of future research, for example the need for long-term clinical trials testing the outcomes of combination therapies and continuing research on thyroid hormone analogs. The current standard of care consists in the administration of levothyroxine and is associated with excellent clinical outcomes in the majority of patients with biochemical and clinical euthyroidism. However, a subset of patients remains symptomatic despite the normalization of their thyroid hormone levels (23,24). In part, this may be unrelated to the thyroid condition, but in some individuals, these signs and symptoms could, for example, be the consequence of impaired conversion of T4, which is considered a prohormone, to T3 at the tissue level (25,26). These and other questions need additional investigation that will, hopefully, permit to improve and fine-tune the therapy of patients with hypothyroidism further.
Looking back at the history of thyroid hormone substitution reveals that we have indeed come a very long way. However, future insights may question some of our current concepts and result in a more individualized and refined therapeutic approach.