
Abstract
Background:
Currently, the measurement of urinary iodine concentration (UIC, μg/L) is the recommended parameter to assess iodine status, however, the dependency of UIC on urine volume may limit its use as an accurate parameter for monitoring iodine status in populations. Therefore, our objective was to compare two approaches for the assessment of urinary iodine excretion in spot urine samples: UIC (μg/L) and a creatinine-scaled estimate of 24-hour iodine excretion (est24h-UIEcrea [μg/d]) against actually measured 24-hour urinary iodine excretion rates (24h-UIE, μg/d).
Methods:
Urinary iodine and creatinine were measured both in 24-hour urine samples and parallel collected spot urine samples from 180 healthy participants of the DONALD Study, aged 6–18 years. 24h-UIE was used as quasi-reference for actual iodine status. Published 24-hour creatinine reference values served to calculate est24h-UIEcrea. Correlation analysis, cross-classifications, and Bland-Altman plots were used to evaluate agreement between the different assessment approaches.
Results:
Correlation coefficients of 24h-UIE with UIC (r=0.12, r=0.22; p=n.s.) were substantially weaker than with est24h-UIEcrea (r=0.41, r=0.47; p<0.001) in the 6–12 year old and 13–18 year old groups, respectively. Cross-classification into opposite quartiles by UIC was 7% (6–12 year old group) and 15% (13–18 year old group) versus 5% and 3% by est24h-UIEcrea, respectively. Bland-Altman plots indicated greater deviation from 24h-UIE for the UIC versus the est24h-UIEcrea approach.
Conclusion:
Our findings in children and adolescents clearly show a better comparability of real 24h-UIE with est24h-UIEcrea than with UIC. Whenever highest possible validity is required for iodine status assessment from spot urine sampling, the determination of est24h-UIEcrea appears to be the more accurate monitoring approach.
Introduction
D
In spite of the relative simplicity and feasibility of using the UIC approach, the method has a weakness because UIC (μg/L) can be affected by daily urine volume (4,6,7), and therefore has the risk of falsely underestimating or overestimating iodine deficiency prevalence. Meanwhile, it has been shown that not even a large sample size is always sufficient to level out interindividual and intraindividual variations in hydration status (6,8).
At the individual level, 24-hour urinary iodine excretion (24h-UIE, μg/d) is considered to be a quasi-reference standard (7,9), although it is clear that usually one 24-hour urine sample is not enough to assess individual iodine intake reliably (10). König et al. (11) reported that up to ten 24-hour urine samples are needed to provide a valid estimate of usual individual iodine intake (11). The major advantage of using 24h-UIE as an indicator is that it reduces the hydration status-dependent variations in iodine excretion. However, the disadvantage of collecting 24-hour urine samples is the elaborate procedure and therefore a risk of lower compliance, compromising data quality especially in field studies (7).
To overcome the dependency of urinary concentration measurements on hydration status, in practice, analytes have been frequently related to creatinine (CR) to minimize variation in urine volume, because CR is known to be excreted at a relatively constant rate in 24 hours (12). Accordingly, the iodine to creatinine ratio (I:CR ratio) has also been used apart from UIC (μg/L) to characterize iodine status (7). However, in children it turned out that this approach alone is inappropriate because the index, especially during the period of marked growth, shows a clear age-dependency that limits its applicability (13,14). Therefore, the additional involvement of age- and sex-stratified 24-hour CR reference values has been suggested as a more accurate approach to assess analyte excretions from analyte to creatinine ratios in spot samples. Remer et al. (15) showed the successful applicability of the 24-hour CR scaling method to estimate 24-hour excretion rates of urinary analytes such as calcium, deoxypyridinoline, and dehydroepiandrosterone sulfate quantified in spontaneous urine samples. Using predicted 24-hour CR values for the estimation of 24-hour iodine has already been applied in adults from industrialized countries (9,16). However, it is currently not certain whether the use of this methodological approach also provides a more accurate assessment of iodine status in children.
Thus, the goal of the present study was to evaluate and compare the applicability of two approaches to assess iodine status from spot urine samples in healthy children and adolescents: (1) UIC (μg/L) alone, the current World Health Organization (WHO) recommendation and (2) 24-hour iodine excretion estimation (est24h-UIEcrea, μg/d), using a CR scaling method that involves published 24-hour CR reference values for children and adolescents. Both approaches were validated against daily iodine excretion actually measured in parallel-collected 24-hour urine samples (24h-UIE, μg/d) of the same children and adolescents. By using urine osmolality as hydration index, we further tested our hypothesis that hydration has an independent relevant effect on iodine concentration measurements in spot urines.
Materials and Methods
Subjects and study design
Urine samples and anthropometric data of 6- to 18-year-old children and adolescents who participated in the Dortmund Nutritional and Anthropometric Longitudinally Designed (DONALD) Study between 1996 and 2002 were utilized for this cross-sectional study. The DONALD Study is an ongoing open cohort study that investigates relation between nutrition, growth, metabolism, and endocrine function in healthy subjects from infancy through early adulthood. Details on the study design and methods have been published elsewhere (17). In brief, the assessments include 3-day weighed dietary records, anthropometric measurements, collections of 24-hour urine samples, and interviews on lifestyle and medical assessments (including spot urine collection). The DONALD study is exclusively observational and noninvasive until the age of 18 years. All examinations are performed with written parental consent and children's assent. The study has been approved by the Ethics Committee of the Rheinische Friedrich-Wilhelms-University of Bonn, Germany.
The number of children included in this analysis was derived from a total of 1479 spot urine samples from the DONALD urine bank, available for the age range of interest and studied time period. Initially, all urine samples were selected if the following inclusion criteria were fulfilled: (1) availability of at least one spot urine sample in parallel with a 24-hour urine sample collection (within±15 days of difference between collections [n=593]); (2) no pathologic finding according to dipstick analysis (protein, leucocytes, glucose, ketones, urobilinogen, bilirubin, blood, and nitrite; Combur® Test, Roche, Mannheim, Germany (n=522); (3) complete 24-hour urine sample, using as criteria a body weight-related 24-hour creatinine excretion rate >0.1 mmol/kg per day (15), as well as reported full collection compliance (n=512); (4) no reported intake of iodine containing medications (levothyroxine, all povidone-iodine–containing disinfectants and formulations) and/or nutrition products (multivitamins, high-energy or protein supplements with added iodine, kelp, or other algae products) before or during urine collection (n=463). Exclusion periods due to ingestion of these iodine sources before urine collection were up to 1 week for supplements and 6 months for medications. None of our children had ingested or incorporated amiodarone or iodinated contrast agents. The available sample pairs were further reduced from 463 to a final number of 452, because 11 sample pairs were from participants with more than one set of urine samples per subject. From this subject pool, sample pairs of 120 (60 girls) 6–12 year olds and 60 (30 girls) 13–18 year olds were then randomly selected. Mean difference between spot and 24-hour collections was ±9 days.
Urine sampling and analysis
The 24-hour urine collection was generally carried out on the third day of the dietary recording. Children and their caregivers received personal information and written instructions on how to collect 24-hour urine samples. The time of the start (discard of the first micturition of the start day) and finish of the urine collection (the first micturition in the morning of the following day) were recorded, including the time of any lost micturition or intake of medications during the urine collection period. The urine samples were immediately stored in preservative-free, Extran-cleaned (Extran, MA03; Merck, Darmstadt, Germany) 1-L plastic containers at less than −12°C before the transfer by a dietitian to the Institute where they were stored at −20°C or less until analyzed. After thawing, combining urine contents of more than 1 container and thorough mixing, total urine volume was determined and a routine check was performed in a separate small aliquot using a commercial test strip (Combur). Dipping of the test strip into the original urine sample was strictly avoided because a considerable liberation of iodine from the strips occurs (18,19). Exclusion criterion for an incompletely collected urine sample was a body weight-related 24-hour CR excretion rate <0.1 mmol/kg per day (15). Spot urine samples were collected from participating children at the examination center on the day of the anthropometrical and medical assessments. Spot urine collection time has not been fixed in the protocol of the DONALD Study and therefore collections were distributed over the day between 8:00
Anthropometric measurements
Anthropometric measurements of the DONALD participants were performed at each annual visit by trained personnel following standard procedures. Weight and height were obtained at the time of the dietary recording. Body weight was measured using an electronic scale (Seca 753 E; Seca Weighing and Measuring System, Hamburg, Germany) to the nearest 0.1 kg. Height was measured in a standing position to the nearest 0.1 cm using a digital telescopic stadiometer (Harpenden, Crymych, UK). Body surface area (BSA) was calculated according to the formula by Du Bois and Du Bois (23) as follows: BSA (m2)=0.007184×height (cm)0.725×weight (kg)0.425.
Data handling and statistical analysis
SAS® statistical program (version 9.1.3, SAS Inc., Cary, NC) was used for data analysis. A p value <0.05 was considered statistically significant. Descriptive statistics of the study sample are presented as medians (25th and 75th percentiles). Unpaired Wilcoxon's tests were used to compare variables between age groups and sex.
The 24h-UIE was measured in 24-hour urine samples and was considered as the reference standard for determining iodine intake (i.e., iodine status). From the parallel collected spot urine samples, different parameters indicating iodine status were derived: (1) measured iodine concentration (UIC, μg/L), the current WHO recommendation; (2) iodine to creatinine ratio (I:CR, μg/mmol), formerly recommended; (3) estimated 24h-UIE (est24h-UIEcrea, μg/d), based on UIC and 24h-CR reference excretion values (15):
To grossly evaluate the proportion of children in the present population at risk of inadequate iodine intake, we compared 24h-UIE with the estimated average requirements (EAR). The proportion of children below the EAR cutoff values (24) was estimated after considering a mean nonurinary iodine loss of 15% (25).
The urinary iodine variables of interest (24h-UIE, UIC, I:CR ratio, est24h-UIEcrea) were skewed (Shapiro-Wilcoxon <0.05), thus log-transformed data were used for analysis of agreement between methods. Pearson's correlation coefficients and cross-classification were calculated for each indicator from the spot urine samples (UIC, I:CR ratio, and est24h-UIEcrea), in comparison with 24h-UIE (quasi-reference) across the different age groups (6–12 year old and 13–18 year old groups). By means of cross-classification, the percentage of children who were classified into either the same or the adjacent quartile of urinary iodine excretion by UIC or est24h-UIEcrea, respectively versus 24h-UIE as reference, or misclassified into the opposite quartile, were computed (26). We used Bland-Altman plots to illustrate the differences between both UIC and est24h-UIEcrea versus directly measured 24h-UIE. For the Bland-Altman comparison, which requires comparable units (here μg/d), each measured UIC (μg/L) was multiplied by age-characteristic average 24-hour urine volumes (6–12 year old group, 1000 mL/d; 13–18 year old group, 1500 mL/d) as suggested by Zimmermann and Andersson (4). This “constant”-volume-derived estimate, calculated to obtain an assumed 24-hour iodine excretion for the respective spot sample UIC is termed est24h-UIEassumedVOL. A quite constant, not systematically varying urine volume is generally assumed when using UIC for iodine status assessment.
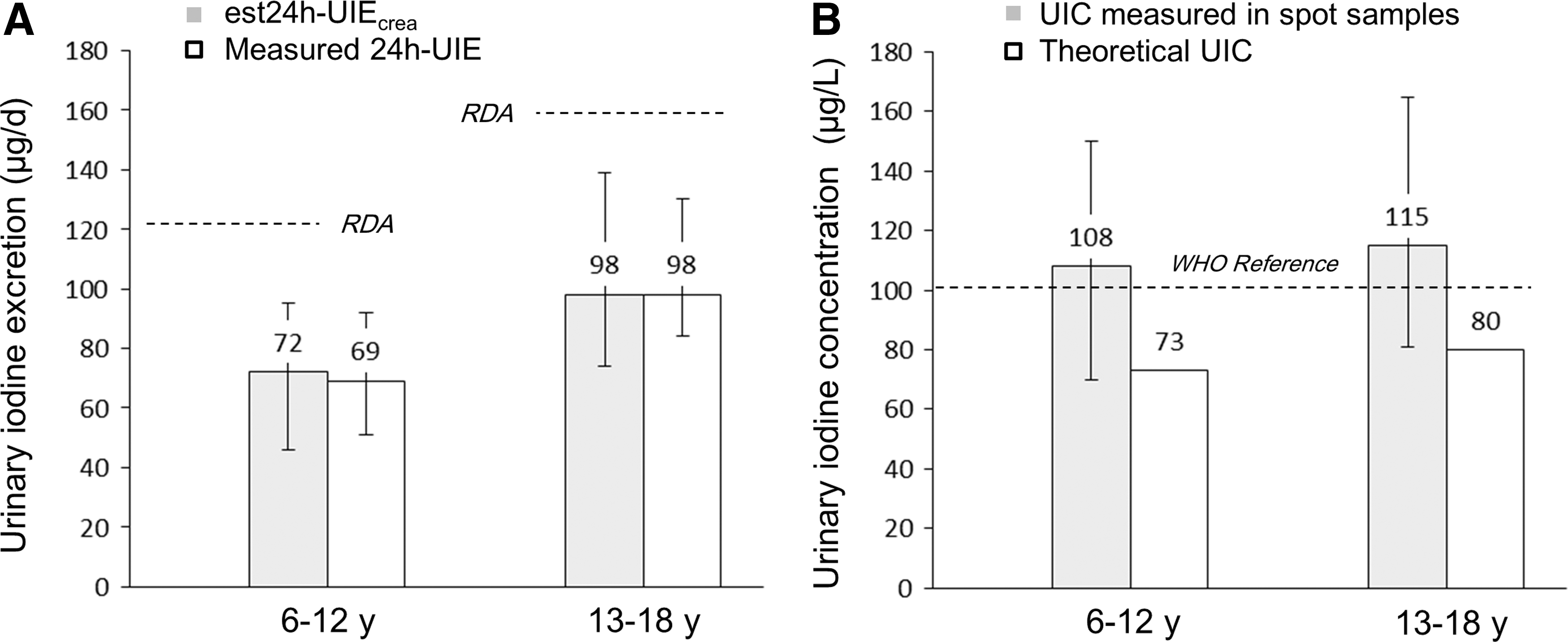
To evaluate the practical consequences of the application of different iodine assessment approaches (i.e., the conclusion that would be drawn from the different estimates), we tested for both estimated 24h-UIE (from the spot samples) and actually measured 24h-UIE whether mean daily renal iodine output decreased below, reached, or exceeded the respective age-group characteristic recommended dietary allowance (RDA) (24) after considering 15% nonrenal iodine losses. These findings were subsequently compared with the corresponding assessment results according to UIC measurements, which was related to the WHO reference level of 100 μg/L as criterion of sufficiency in two ways: first, comparison with the original measurement at the actual spot urine osmolality, and second, with the theoretical UIC at a desirable osmolality reflecting euhydration. Osmolality values of 585 mOsm/kg in the 6–12 year old group (27) and 619 mOsm/kg in the 13–18 year old group (28) were used as reference for desirable osmolality.
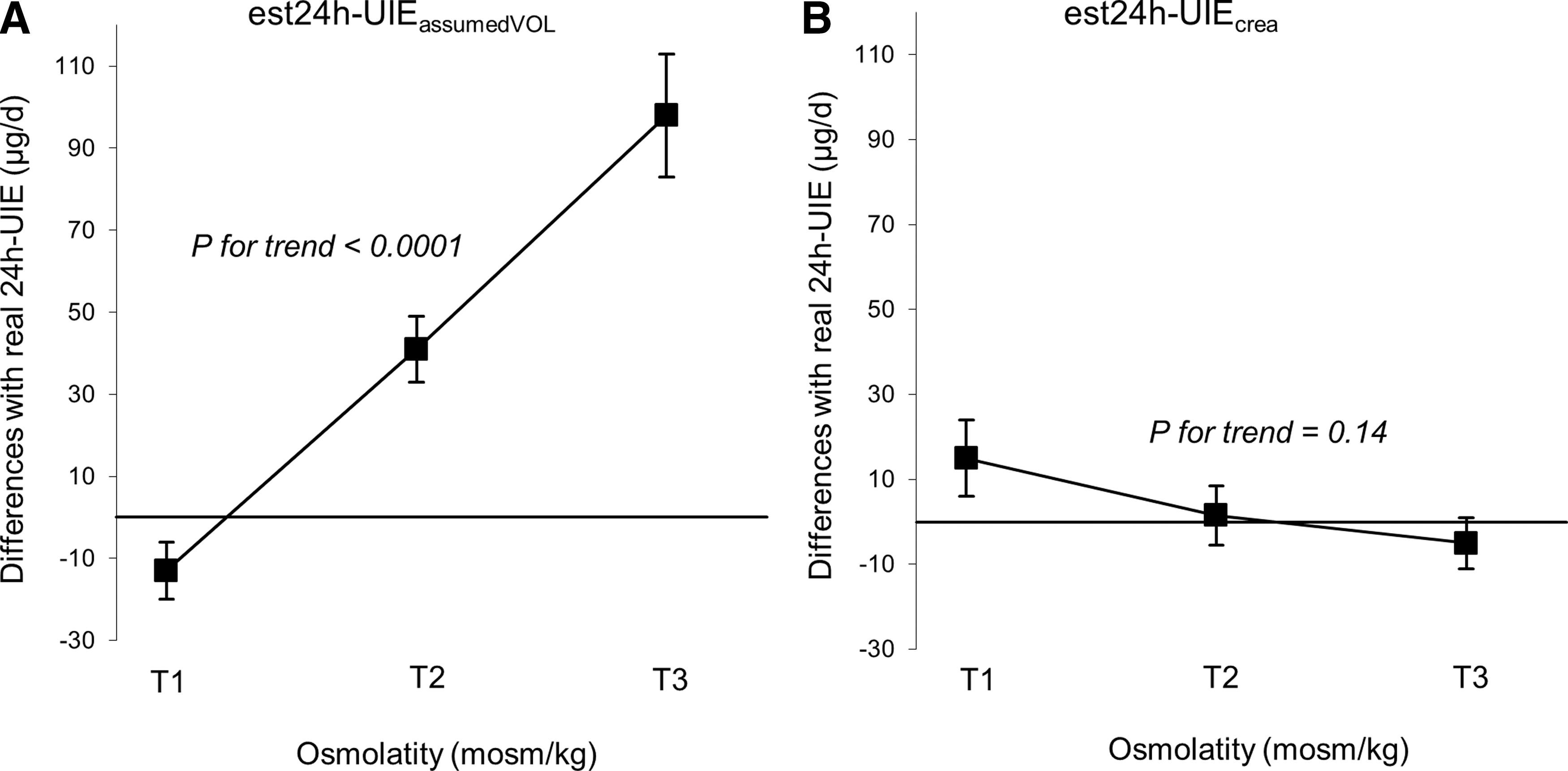
Finally, to test for the effect of hydration status on the distinct iodine assessment approaches derived from spot urine samples (UIC and est24h-UIEcrea), we evaluated their deviation from the directly measured 24h-UIE in relation to urine osmolality. For this, we grouped the distribution of urine osmolality (mOsm/kg) into sex- and age-group specific tertiles and calculated for each tertile the mean of the differences between the reference standard (24h-UIE) and either est24h-UIEassumedVOL (μg/d) or est24h-UIEcrea (μg/d).

Results
Table 1 presents anthropometric and urinary characteristics of the study sample stratified by sex and age group. Estimates of urinary iodine varied widely across the sex and age categories depending on the type of urine collection. Overall, the children's and adolescents' median (25th, 75th percentiles) 24h-UIE was 69.4 μg/d (51.0, 91.5) and 98.0 μg/d (83.4, 130.1), respectively. For 118 of the 180 examined DONALD participants, two additional 24-hour urine collections were available (with iodine measurements) within a 2-year time frame encompassing the actual parallel collection of the spot and the 24-hour urine samples. One of these additional 24-hour samples had been collected 1 year before and the other, 1 year after the combined spot and 24-hour sampling. The corresponding overall 2-year-median of UIE (consisting of 3 separate 24-hour collections per individual), was close to the median of the actually examined single 24h-UIE (see above) in both the 6–12 year old group (67.3 μg/d [52.4, 86.4], n=73) and the 13–18 year old group (103.0 μg/d [87.0, 125.0], n=45), indicating a rather comparable iodine intake over a longer time period. Correspondingly, the individuals' actual 24-hour UIEs and their individual 2-year means were highly correlated (6–12 year old group: r=0.79, p<0.0001; 13–18 year old group: r=0.75, p<0.0001).
All values are medians; 25th, 75th percentiles in parentheses.
Significant difference between boys and girls same age-group tested with unpaired Wilcoxon test.
Significant differences between same-sex different age-group tested with unpaired Wilcoxon test.
Defined by using the daily iodine estimated average requirement (EAR) for 4<10 years old, 65 μg /d; for 10<15 years old, 73 μg/d; for 15<19 years old, 95 μg/d (24) corrected for 15% of nonurinary losses.
Osmolality measured in spot urines, data available for the study n=127 samples.
BSA, body surface area; EAR, estimated average requirement; 24h-UIE, 24-hour urinary iodine excretion; UIC, urinary iodine concentration; I:CR, iodine to creatinine ratio.
A relatively higher proportion (∼30%) of children in the 6–12 year old group had inadequate iodine intake (derived from comparison of 24h-UIE with EAR values) compared with the older group (∼15%). UIC (μg/L) measured in spot urine samples was not significantly different in any of the evaluated groups. Twenty-four–hour urine osmolality (mOsm/d) significantly increased by age in both groups, and boys had a significantly higher solute load compared to girls. However, sex differences in osmolality (mOsm/kg) measured in spot urine samples was significant only in the 6–12 year old group.
Table 2 presents the values for agreement (Pearson's correlation coefficients and cross-classification) between 24h-UIE (quasi-reference standard) and iodine assessment approaches measured in spot urine samples (UIC, est24h-UIEcrea, I:CR ratio). In all age groups, est24h-UIEcrea was better correlated with 24h-UIE (r=0.41–0.47, p<0.05) than UIC alone (r=0.12–0.22 p=n.s.). Misclassification into the opposite quartile occurred in 7% and 15% (6–12 and 13–18 year old groups) when UIC approach was applied, and in 5% and 3% (6–12 and 13–18 year old groups) when the 24-hour CR scaling method (est24h-UIEcrea) was used.
Log-transformed variable.
Estimated with 24-hour creatinine scaling method (description in the Methods section).
I:CR ratio has been formerly used as approach so it has been included only for illustrative purposes.
UIC, urinary iodine concentration; est24h-UIEcrea, estimated 24-hour urinary iodine excretion; I:CR, iodine to creatinine ratio.
The Bland-Altman plot for the total study sample indicated that differences in 24h-UIE versus est24h-UIEassumedVOL were more scattered than versus est24h-UIEcrea. Also, the interval within which 95% of differences between measurements by the two methods are expected to lie, were notably broader for est24h-UIEassumedVOL than for est24h-UIEcrea. (Fig. 1A and 1B).

Bland–Altman plot of log-transformed data for the total study group including boys and girls.
Median (25th, 75th percentile) values of the est24h-UIEcrea and actual 24h-UIE were both compared with the age-corresponding RDAs showing comparable appraisal of iodine status with both approaches (Fig. 2A). In the case of UIC (as estimation parameter) a similar evaluation was only obtained when the desired hydration status was taken as a basis (Fig. 2B).
Median (25th, 75th percentiles) urinary iodine excretion analyzed in 180 urine samples by age group
Effect of osmolality on estimated iodine excretion for the two different approaches (est24h-UIEassumedVOL vs est24h-UIEcrea) is illustrated in Figure 3. The mean differences between est24h-UIEassumedVOL and actual measured 24h-UIE was significantly higher in children with a higher urine osmolality (p<0.0001). The mean deviation from real 24h-UIE increased by approximately 50 μg/d per tertile of osmolality. In comparison the mean differences between est24h-UIEcrea and 24h-UIE were minimal and not significantly different (p>0.14).
Dependency of UIC multiplied by an assumed age-characteristic average 24-hour urine volume (est24h-UIEassumedVOL) (description in the Methods section)
Discussion
Currently, the recommended and most widely used method to estimate iodine status in populations is the measurement of UIC, which in individuals is known to be highly influenced by both iodine intake and hydration status (4). The present investigation demonstrated that hydration status can not only affect individual UIC but also average UIC of certain age groups during growth. As shown here in healthy children and adolescents, a hydration status-dependent shift of median UIC values is possible and may no longer allow an appropriate assessment of their potentially true iodine status. Therefore, the application of UIC without considering hydration status bears the risk of overestimation or underestimation of the actual iodine status. With the 24-hour CR scaling method described here, we present a simple and reliable hydration status-independent approach to assess iodine status from spot urine samples in children and adolescents.
As recognized, the most reliable method of estimating iodine intake is the measurement of 24-hour iodine excretion (7). However, in epidemiologic surveys, analyses of 24-hour urine samples in general are rare because of the larger efforts and difficulties associated with this type of urine collection (1,4). Hence, a more convenient method to assess iodine status of populations using spontaneous urine samples has been suggested, simply by measuring iodine concentration (UIC, μg/L). The underlying assumption for this approach is that usually there exists a “sufficient” number of spot urine samples to level out interindividual and intraindividual variations in hydration status (1,4). However, whether n=30 (5) or up to n=500 (29) subjects or spot samples are necessary to possibly overcome the confounding effect of day-to-day diurnal variation of dietary iodine intake or water (beverage) ingestion (10) has not been uniformly reported.
Because the concentration of iodine in urine depends on urine volume, alternative methods to estimate the daily urinary iodine excretion by additional measurements of CR concentration have been proposed. The I:CR ratio (μg iodine/g creatinine) had been applied as an assessment method decades ago. However, CR measurements were later considered unnecessary (5), partly due to a putatively higher variation of I:CR compared to UIC measurements alone. Despite this, several authors proceeded to determine analytes in spot urine samples normalized to urinary CR. Mostly they used ratios of I:CR to estimate 24-hour excretion rates of the trace element iodine, for example by multiplying the ratio with sex- and age-specific CR reference values. This has, in fact, been shown to yield more reliable assessments of real 24-hour iodine excretion rates than simple UIC measurements in adults (10,16).
The obviously inappropriate evaluation of children's iodine nutrition by the I:CR approach was evidenced approximately two decades ago (13), because of the observed physiologic, particularly strong age-dependent increase in muscularity and hence CR production during growth. By establishing reference values for 24-hour CR excretion for healthy children, it could be shown that their use allowed reasonably estimated average 24-hour excretion rates of certain analytes (calcium, deoxypyridinoline, dehydroepiandrosterone sulfate) from spot urine samples (15). The results of the present study extend these findings also to the micronutrient iodine and support the application of this methodological approach when examining spot samples. In a relatively small sample of n=160 spot and parallel 24-hour urine collections, the 24-hour CR scaling method (est24h-UIEcrea) yielded satisfactorily comparable median excretion estimates with the measured actual 24h-UIE in the same individuals. Pearson correlations and cross-classifications confirmed the advantages of est24h-UIEcrea over simple concentration measurements (UIC).
By using the cutoff as proposed by the WHO (median of the population >100 μg/L) (5) without further considering hydration status, a clear underestimation or (as in our study) overestimation can occur for iodine status in populations. In the present study, UIC findings inappropriately suggested iodine sufficiency in a group of 6–12 year old healthy DONALD participants, who in approximately 30% of cases (according to the actual 24h-UIE) showed iodine intakes below EAR. However, caution has to be taken here regarding the percentage of subjects below the respective EAR due to the intraindividual day-to-day variability, being present also with 24-hour urine collections. As reported by Haldimann et al. (30), and also discussed by Zimmermann and Andersson (4), appropriate adjustment for intraindividual and interindividual variation of iodine excretion can result in a substantial attenuation of the proportion of individuals lying below the EAR.
In our sample of healthy 6–12 year old children, median UIC was >100 μg/L and the corresponding urinary osmolality ranged from 108 to 1257 mOsm/kg. A similar osmolality range has recently been observed in 9–11 year old children in the United States: 99–1259 mOsm/kg (31). Under the assumption that changes in hydration status and osmolality also affect UIC, we could show for children with such a relatively high osmolality that their median UIC at a more desirable osmolality will be markedly decreased toward values below 100 μg/L. In contrast to this, est24h-UIEcrea values were almost not influenced by hydration status and/or varying osmolality, and this is one of the main prerequisites for the use of spot urine samples to evaluate iodine nutrition. Accordingly, in children a relevant confounding of hydration status on mere UIC measurements also exists.
Theoretically, UIC and 24h-UIE can be used interchangeably, if the average daily urine volume produced by a certain population approximates 1 L, as it often (but not always) is the case in older schoolchildren (1,4). We also tested this approach of a constant average 24-hour urine volume (using est24h-UIEassumedVOL) and observed no satisfactory agreement between est24h-UIEassumedVOL and the 24h-UIE (see Bland-Altman plots). On the other hand, we did observe a higher level of agreement between the est24h-UIEcrea method and real 24h-UIE in our children (Bland-Altman plots; Fig. 1B). Thus, even in a relatively homogeneous population as that of the DONALD Study the approach of using UIC or “UIC interchangeable” (assumed urine volume 1 L) to appropriately characterize real 24-hour iodine status was not successful.
So far, few studies have investigated alternative approaches to estimate 24h-UIE from spot UIC values, and the existent literature only refers to studies conducted in adults (8,9,16,30). Moreover, the Institute of Medicine (24) has proposed one equation to simplify the calculation of daily iodine intake, using approximated values based on iodine bioavailability, observed urine volumes and weight; however, this approach represents only an approximation without considering the obviously common interindividual and intraindividual variations in urine volume that can confound the Institue of Medicine suggested method. We applied that formula and found an overestimation of iodine excess of ∼10 μg/d in 6–12 year old children (p=0.05), and ∼50 μg/d in the 13–18 year old group (p<0.001) compared to real 24h-UIE (data not shown).
To our knowledge, the present study is the first to compare values of iodine excreted in 24-hour urine samples against 24-hour iodine estimated from spot urine samples in a sample of healthy children and adolescents. A particular strength of the present study consists in having 24-hour urine samples parallel to spot urine samples from the same children, and measurement of the same urinary parameters (iodine, creatinine, and osmolality) in both samples for methods comparisons. Furthermore, the consideration of osmolality in the evaluated urinary parameters, allowed illustrating the effect of potential changes of hydration status on iodine excretion that until now were only observed by measuring urine volume (6,7).
In the present study, spot urine samples and 24-hour urine collections were allowed to have a maximum time difference of 15 days. The fact that the single 24-hour UIEs in our subjects (at least in all in whom we could check it) were closely associated with their 2-year average iodine excretion (comprising 3 separate 24-hour collections per individual) shows that the herein examined single 24-hour UIEs, for the most part, reflect the subjects' longer term iodine status. Thus, the 24-hour urine samples represent a reasonable quasi-reference for the comparison with random spot samples (i.e., urine samples not collected at well-defined time points), as is the normal practice in urinary iodine monitoring surveys.
Our finding of nearly the same median population estimates for spot-sample–derived 24-hour iodine and real 24-hour iodine excretion both in the 6–12 and 13–18 year old groups suggest a reasonable applicability and suitability of the CR scaling approach also under more realistic field conditions with spot urine collections, for example in monitoring studies.
The challenge, in general, for adopting the 24-hour CR scaling approach might be the accustomed practice and familiarity of using UIC as a simple iodine biomarker, for which the cutoff values for sufficiency are worldwide in use. We considered UIC and est24h-UIE in some detail to provide the reader with an idea of the relative accuracies of the different in approaches (Fig. 1). The present CR scaling approach is based on UIC values measured in spot urine samples, thus the application is quite simple and feasible. Its advantage, as demonstrated, is that it provides a hydration status-independent 24-hour iodine excretion level (comparable to 24-hour iodine intake data) that makes it suitable to be compared with the official iodine intake recommendations. However, for this, validated population thresholds for determining iodine sufficiency need to be developed. Currently such thresholds do not exist, apart from the concept to integrate the EAR values (32) into this threshold system. In this respect, important steps have been made by Zimmerman and Andersson (4) and Haldimann et al. (30) who have convincingly suggested the use of the EAR cut-point method for estimating the prevalence of iodine inadequacy.
Since mild to moderate iodine deficiency affects not just low- and middle-income countries but also countries in the industrialized world (1), the 24-hour CR scaling method suggests itself as an alternative reliable approach to estimate iodine status from spot samples, at least in children from industrialized countries with similar dietary and physical developmental characteristics, as found in the population for which required CR reference values have been published. To further enhance the feasibility of applying this more accurate method for a population's iodine assessment, in other children outside the above context too, the possible applicability of these already published CR reference values could also be explored for different populations (e.g., with substantially differing protein intakes) (15,33).
In conclusion, we found reasonable estimates of daily iodine excretion by applying the 24-hour CR scaling approach (est24h-UIEcrea) when simply analyzing spot urine samples in healthy children and adolescents. The comparison with the conventional approach of UIC (μg/L) showed clear advantages (e.g., almost entirely hydration status independent). The successful application of est24h-UIEcrea also in larger epidemiologic studies has just recently been demonstrated in adults (using different CR reference values) (8), and may thus constitute a fruitful and not too complicated way to assess iodine status more precisely in epidemiologic surveys in children and young adults.
Footnotes
Acknowledgments
We acknowledge the participation of all children and their families from the DONALD Study. The authors thank the staff of the Research Institute of Child Nutrition for collecting anthropometrical and dietary data, and for urine laboratory analyses. The DONALD Study is funded by the Ministry of Innovation, Science and Research of North Rhine, Westphalia, Germany.
Author Disclosure Statement
No competing financial interests exist.