
Abstract
Background:
The number of thyroid cancer (TC) survivors is increasing exponentially worldwide. However, little research details the unmet information, support needs, and survivorship concerns of TC patients.
Methods:
Two thousand TC survivors completed an online survey examining the importance of and recollection of receiving care addressing three areas at the time of diagnosis and treatment: medical/physical issues, practical matters, and emotional/psychological concerns. A summed score was generated of (1) the “important” responses for each category, and (2) if they remembered receiving that information/support. Regression analyses explored the relationship between each total score of importance and a patient's demographics, treatment, and recollection of receiving each domain of information/support.
Results:
Respondents were generally female (88.6%), part white (91.1%), and had eventual total thyroidectomy (95.8%) and radioiodine (80.6%). Mean age at diagnosis was 42.1 years and average time from diagnosis 5.43 years. Less than 50% of patients recalled receiving information regarding long-term and health effects after treatment, or any practical matter or emotional/psychological concern. Multivariate linear modeling with forward stepwise regression revealed that age, sex, and survivorship time were important predictors for recollecting having received information and support for medical/physical issues, practical needs, and emotional/psychological concerns after controlling for treatment and other demographic factors (all 0.001 or <0.001). Similar modeling demonstrated that female sex and feeling that they received care in a given category (medical/physical issues, practical needs, or emotional/psychological concerns) predicted the importance placed on those specific needs when controlled for other variables (all 0.001 or <0.001).
Conclusion:
TC patients place high importance on most types of information and concerns. However, the majority of information and support needs are unmet, which varies based on demographic and treatment factors as well as the importance placed on each specific topic of information. Qualitative research is needed to further focus and refine these unmet needs that should be followed by targeted interventions.
Introduction
T
The goal of this study is to detail the unmet support needs and survivorship concerns in a large cohort of TC patients. In doing so, clinicians may become better equipped to deliver information and support in such a way as to improve both physical and psychosocial outcomes for TC patients.
Methods
Participants
Two thousand TC patients >15 years of age at diagnosis completed online surveys via a link on the ThyCa (Thyroid Cancer Survivor Association) website. Participants had to be able to read and comprehend English to complete the survey.
Procedures
Participants were recruited from April 22–November 1, 2013 through listserv e-mails (that also include providers and family members) and a direct link on the ThyCa website that was easily visible to all ThyCa website visitors. Reminder emails to complete the survey were sent out on three separate occasions. The survey was conducted and data stored using Survey Monkey with patient anonymity. The data was locked and downloaded for analysis on November 1, 2013, once 2000 patients had completed the survey.
Measures
A demographic form assessed sex, ethnicity/race, and each of the following at the time of initial cancer diagnosis: age, employment/education status, insurance status, living situation (household composition), relationship status, and geographic region of residence. A treatment form detailed the setting (rural vs. urban; academic/health maintenance organization/cancer center vs. private) and type of initial cancer treatment (extent of surgery and radioiodine). Patients rated the importance of receiving various medical/physical, practical, and emotional/psychological domains of information during diagnosis and treatment, as well as their recollection of receiving such information (Fig. 1). Participants ranked the importance, from 1=extremely important through 5=not important, of receiving various types of information during diagnosis and treatment, grouped into three domains: medical and physical matters (14 items), practical issues (9 items), and emotional and psychological concerns (8 items). They were then asked to remember if they received information regarding these same types of information (yes/no). Lastly, participants were asked if they felt that overall they received care for their concerns in the three realms of information (yes/no). Patients were given the option to write additional comments at the end. The study questionnaire is detailed in a previous report (4). It was designed at a sixth-grade reading level.
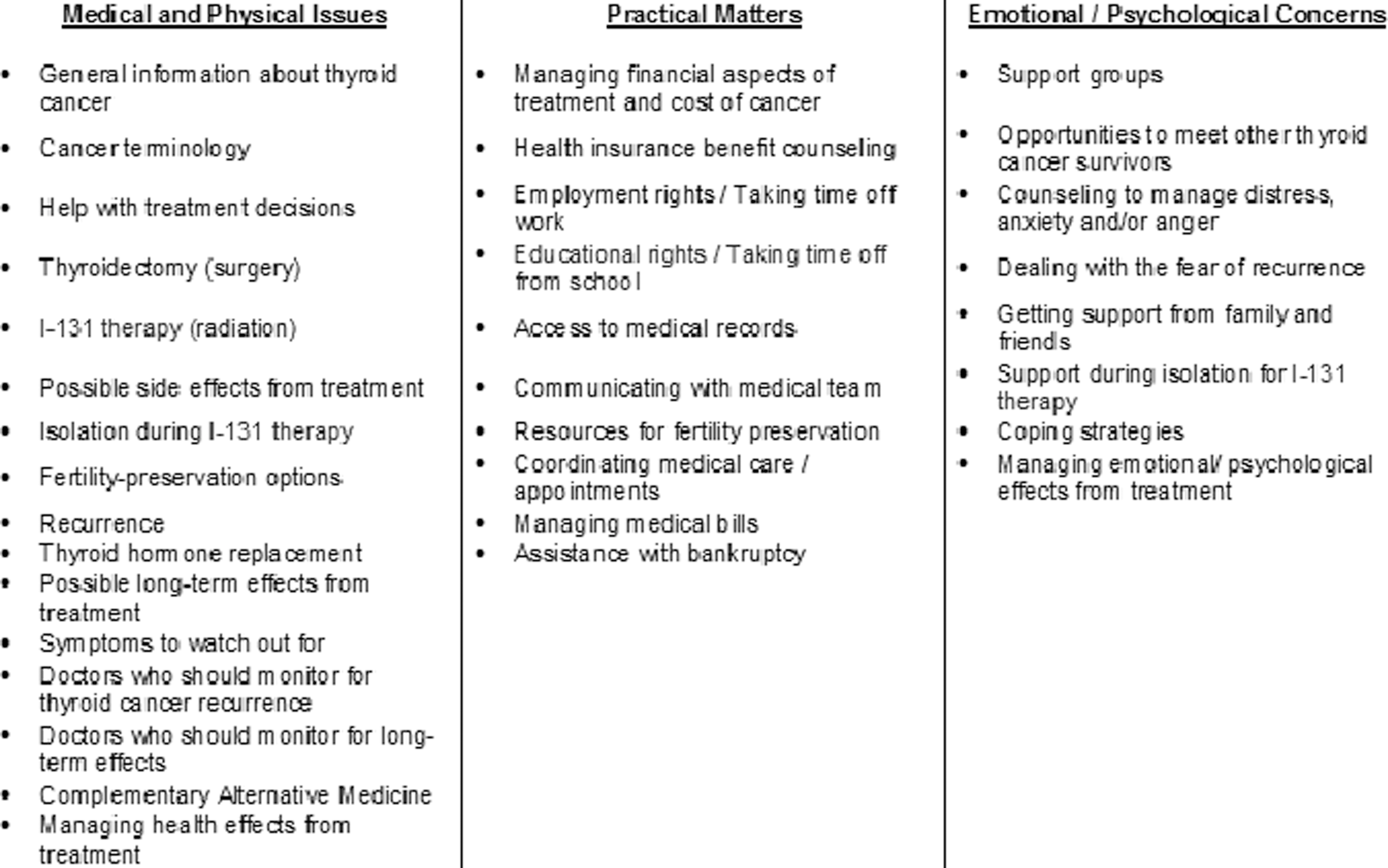
Specific questionnaire items in each category.
Statistical analysis
Data were examined to make sure there were no duplicate entries, so that each set of patient information was unique. For the ranking of information importance, responses were grouped into two categories to elucidate those categories that patient's felt were most important: “very or extremely important” (responses 1 and 2) and “not important, somewhat important, and important” (responses 3–5). A summed score was generated for each information/support domain of (1) the “very or extremely important” responses for each category and (2) if they remembered receiving that information/support. Descriptive statistics (frequencies, mean, and standard deviation) were used to describe the whole group. To explore relationships between the total scores of importance that patient's place on each of the three domains by demographic, treatment, and acknowledgement of receiving various realms of information, t-tests, Mann-Whitney U tests, and Kruskal-Wallis tests were used. Linear modeling with forward stepwise regression defined which demographic and clinical variable(s), and their relative importance, significantly affected each of the three information/support domains and patient recollection of receiving each type of information. Variables that were significant at the p<0.05 level were entered.
Data analyses were performed with the Statistical Package for the Social Sciences (SPSS) software (version 21.0; SPSS Inc., Chicago, IL). All tests were two-sided, missing data was handled with list-wise deletion, and a p value of <0.05 was considered to be statistically significant.
Results
Of 2000 respondents, most were female (88.6%); part-white (91.1%) (black 2.2%, Asian 2.6%, Hispanic 5.6%, Native American 1.8%); insured at diagnosis (95.2%); and treated in urban settings (88.7%) across the country (Table 1). The majority underwent eventual total thyroidectomy (95.8%) and radioiodine (80.6%) treatment with half (50.9%) being treated by a private clinician. Most patients (93.4%) were<60 years of age at diagnosis (average 42.1 years), and the mean time since initial cancer diagnosis was 5.43 years (standard deviation=7.16 years) with 63.5% were within 5 years of diagnosis. Socially, 18.4% were unemployed/not in school, 21.1% single, and 15.6% lived alone. Approximately 90% of patients completed each question.
For the entire cohort, the average scores for types of information and support that patients remembered receiving were 6.98 (out of a possible 16) medical and physical issues, 1.45 (out of a possible 10) practical matters, and 1.39 (out of a possible 8) for emotional and psychological concerns. Less than 50% of patients recalled receiving information regarding long-term and health effects after treatment, or any practical matter or emotional/psychological concerns. (Table 2). Table 3 shows differences in total scores by demographic and treatment variables. Patients over 60 years of age, males, and insured patients remembered receiving more information regarding medical and physical issues; younger males, and those treated at an academic or cancer center and having some form of neck dissection received more information concerning practical matters; younger patients, males, and those treated in an academic or cancer center recalled receiving information for their emotional and psychological concerns.
When queried as to the importance each participant placed on the various categories of information and support, medical and physical issues (mean 14.5 out of 16) were the most important, followed by emotional and psychological concerns (mean 6.04 out of 8), and practical matters (mean 5.86 out of 10). Table 4 shows the breakdown of which demographic groups found each type of needs “very or extremely important.” Female, non-white, younger patients rated more categories of information and support “very or extremely important” compared with male, white, older patients. Recollection of having received care in a given domain also significantly affected the importance rating placed on those specific needs.
Individual linear models revealed that age and sex were important predictors for recollection of receiving information and support for medical and physical issues, practical needs, and emotional/psychological concerns when controlling for treatment and other demographic factors (Table 5). Females and younger patients recalled receiving information less frequently than did males and older patients. Survivorship time was also important for receiving information on medical and physical issues as well as practical matters; patients diagnosed within the past year recalled receiving information more often than patients further out from treatment. Other linear models demonstrated that female sex and race/ethnicity influenced how important each category of information and support were rated after control for other variables (Table 6). Females rated information very or extremely important more often than males, Hispanics more frequently rated information on medical and physical issues are very or extremely important, blacks more frequently for practical matters, and any non-white for emotional and psychological concerns. Additionally, patients that felt they received information and care for practical matters and emotional/psychological concerns were more likely to rate that information in that specific category of information as very or extremely important.
Controlling for type of surgery, ethnicity, insurance, region of treatment.
Controlling for type of surgery, ethnicity, race.
Controlling for type of surgery and survivorship time.
LND, lymph node dissection.
Discussion
Unmet supportive care needs for cancer patients has been defined as “those needs which lack the level of service or support an individual perceives is necessary to achieve optimal well-being” (7). This is the largest study to date to examine unmet needs in TC patients and survivors. Most patients expressed a strong desire for receiving information and support regarding medical and physical matters, practical issues, and emotional and psychological concerns at the time of TC diagnosis. However, most of these information and support needs were unmet. Less than 50% of patients recalled receiving information regarding long-term and health effects after treatment, or any information on practical matters or support for emotiona/psychological concerns. Females and younger patients (<40 years of age) reported receiving the least information. Additionally, race and sex influenced which information and support needs were rated as most important by TC survivors.
Studies in other cancer survivor populations have reported differences in unmet needs by sex, race/ethnicity, and health as well as between hospitals and based upon the clinician–patient relationship (8 –11). They are not as dismal as the results of the few previously completed studies involving TC patients. A study of 306 TC survivors published last year indicated that patients were not at all or only a little satisfied with the information they received over their courses of treatment (3). Moreover, 31% of respondents claimed that they found the information that was provided to be only slightly or not at all helpful, and 34% specified that they would have liked to receive more information, suggesting that at least a third of patients experienced an unmet need. Unfortunately, this study did not explore differences in the demographic variables of their participants. Similarly, another recent study that looked at cancer-related worry in TC survivors in Canada showed that younger age, partnered marital status, having children, and ≤≤5 years since TC diagnosis increased worry as well (6).
A smaller, earlier survey examined quality of life, needs, and preferences for information and support in 62 TC patients (12). Although many patients reported good quality of life and felt they received adequate information throughout the course of treatment, most respondents delineated a desire for ongoing information resources, with particular regard to lifestyle habits that might affect recurrence, and symptoms of recurrence, which corresponds with some of the practical and medical questions in the present study that were largely unmet and that patient's expressed were important. Again, this study did not examine demographic variation in information and support concerns.
There are two main limitations to the current study. First, patients and survivors had to know about the study and opt to participate, creating the potential for selection and response bias. Patients had to either be registered on the ThyCa listserv or check the ThyCa website during the two months of enrollment. Although one might hypothesize that these patients had worse cancer treatment experiences or came only from large academic or cancer centers, in fact almost half were treated by a private clinician, more than 10% were from rural areas, and in the survey comments (not discussed in the paper), many had positive things to say about their clinicians. However, all patients had to have knowledge about the support group, which would either come from their physicians and/or from being internet savvy. Second, some participants (about 1/3), were >5 years out from their thyroid cancer treatment and thus their recollection of met needs and concerns may be somewhat different than their concerns at the time of diagnosis and initial treatment, leaving the possibility open for recall bias. Nevertheless, this study was able to capture more than 2000 patients from a wide range of demographic backgrounds and thyroid cancer treatments and thus should be fairly representative of the larger TC patient and survivor population.
Future research should aim to conduct rigorous qualitative studies with both newly diagnosed and long-term thyroid cancer survivors, similar to what has been done in other cancer patients (13,14). These would further focus and refine the gaps identified in the current study as well as construct a TC-specific questionnaire for unmet needs similar to what has been done for other cancers or age groups (15,16). Afterwards, interventions to address these gaps, with a particular emphasis on ways to tailor information to specific demographic groups, need to be designed and implemented followed by qualitatively and quantitatively assessing their impact. Based on the results of the current study, females and younger patients appear to desire more information and support and have the highest unmet needs. For the present, clinicians treating TC patients and survivors could consider implementing some of the newer global cancer initiatives such as treatment summary and survivorship care plans. Other options may include designing information pamphlets or other readily available resources for patients and offering referral to social work or other relevant specialists.
Conclusion
TC patients place high importance on most types of information and concerns. However, the majority of information and support needs are unmet, which varies based on demographic and treatment factors as well as the importance placed on each specific topic of information. Qualitative research is needed to further focus and refine these unmet needs that should be followed by targeted interventions.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Jackie Cassillas MD, Associate Professor of Pediatrics UCLA, for her help in designing the survivorship survey.
Author Disclosure Statement
No competing financial interests exist.