
Abstract
Background:
The first-choice treatment of thyrotropin (TSH)-secreting pituitary adenomas is surgical adenomectomy, with 40–60% of patients cured after surgery. The presence of somatostatin receptors on the adenomatous cells suggests that first-generation somatostatin analogs (octreotide, lanreotide) could be used as an adjuvant treatment to surgery for TSH-secreting pituitary adenomas. The aim of this study is to describe the efficacy and safety of primary medical treatment with first-generation somatostatin analogs in patients with a TSH-secreting pituitary adenoma.
Methods:
Retrospective study on 7 patients (5 women, 2 men) aged 57±14 years with pure TSH (n=4) or mixed TSH/GH (n=3) secreting pituitary adenomas primarily treated with first generation somatostatin analogs. Magnetic resonance imaging revealed a microadenoma in 3 patients and a macroadenoma in 4 patients. The follow-up period was 8.5±7.3 years.
Results:
At initial diagnosis, the patients presented with thyrotoxicosis with elevated free thyroxine (26.5±6.5 pg/mL) and free triiodothyronine (7.3±0.9 pg/mL) levels and a mean TSH of 4.3±1.4 mU/L. During somatostatin analog treatment, free thyroid hormones and TSH levels normalized after 4.4±3.9 and 7.0±8.4 months, respectively. At the time of the last visit, 6 patients were biochemically controlled. Adenoma volume decreased in 6 patients and a decrease in adenoma volume persisted in 2 patients several years after initiation of somatostatin analog treatment. Safety of treatment was good and no patients discontinued somatostatin analogs due to side effects.
Conclusion:
This study confirms the efficacy of primary medical treatment with first-generation somatostatin analogs in terms of hormonal control and tumor volume reduction in patients with TSH-secreting pituitary adenomas, and its good safety profile. First-generation somatostatin analogs may serve as a medical alternative to surgical treatment, especially in patients where surgery is contraindicated or in subjects presenting with invasive macroadenomas that render complete surgical resection difficult.
Introduction
T
The standard treatment of TSH-secreting pituitary adenomas is surgical adenomectomy, with 40–60% of patients cured after surgery (1,3,4). The presence of somatostatin receptors on the adenomatous cells (5 –7) suggests that first-generation somatostatin analogs (octreotide, lanreotide) could be used as an adjuvant treatment to surgery for TSH-secreting pituitary adenomas. Few studies have investigated the efficacy of primary medical treatment with these somatostatin analogs in patients with a TSH-secreting pituitary adenoma (8 –11).
The objective of this study is to describe the efficacy and safety of primary medical treatment with first-generation somatostatin analogs in patients with a TSH-secreting pituitary adenoma.
Patients and Methods
Patients
This is a retrospective study of patients with a pure TSH-secreting adenoma or a mixed TSH/growth hormone (GH) adenoma medically treated with first-generation somatostatin analogs alone or combined with a dopamine agonist.
The diagnosis of TSH-secreting pituitary adenoma was based on the presence of a detectable, normal, or elevated TSH level associated with an increase in the free fractions of thyroid hormones in patients with or without clinical signs of thyrotoxicosis and/or a tumor syndrome characterized by headache while the visual field was normal. Magnetic resonance imaging (MRI) evidence of a pituitary adenoma, the absence of a TSH response to the thyrotropin releasing hormone test, and an increase in the α-subunit and in sex hormone binding globulin levels formally confirmed the diagnosis of a TSH-secreting pituitary adenoma.
The patients were informed about the aims of the study and gave their written consent by signing the consent form.
Methods
The clinical data were collected from information contained in the patients' records. TSH, free triiodothyronine (FT3), free thyroxine (FT4), GH, and insulin-like growth factor 1 (IGF-1) tests were performed with kits routinely used in the biochemistry laboratory. Pituitary MRI was performed after intravenous injection of gadolinium. Depending on size, the pituitary adenomas were divided into microadenomas (maximum diameter less than 10 mm) or macroadenomas (maximum diameter greater than or equal to 10 mm). The volume of the adenomas was calculated in mm3 (transverse diameter×anterior–posterior diameter×height×0.52). The results of the quantitative variables are given as mean±standard deviation. A p-value <0.05 is considered significant.
Results
Population characteristics at diagnosis
Our population consists of 7 patients (5 women and 2 men) aged 35 to 79 years (57±14 years) (Table 1). Cosecretion of GH was reported in 3 patients. MRI revealed a microadenoma in 3 patients and a macroadenoma in 4 patients. The 3 patients with TSH/GH adenoma had a macroadenoma.
F, female; FT3, free triiodothyronine; FT4, free thyroxine; GH, growth hormone; M, male; NA, not available; ND, no data; TSH, thyrotropin.
Medical treatment
Patients were treated with subcutaneous octreotide or with once-monthly intramuscular injection of octreotide long-acting release (octreotide LAR, Novartis Lab, France) or with subcutaneous Lanreotide Autogel (Ipsen Lab, France). Dopamine agonist (cabergoline) treatment was introduced in patient 1. The follow-up period ranged from 1.8 to 20.8 years (8.5±7.3 years), and no patient was treated with surgery or radiotherapy.
Hormonal efficacy
Table 2 shows the TSH, FT4, and FT3 values before treatment and at the last assessment for each patient. In 6 patients, free thyroid hormones and TSH levels normalized after 4.4±3.9 and 7.0±8.4 months, respectively. Only patient 4 had elevated FT4 and FT3 levels following treatment with octreotide LAR 30 mg every 28 days.
p<0.02.
p<0.03.
SD, standard deviation.
Figure 1 shows the mean TSH, FT4, and FT3 values at diagnosis, after 3 months of treatment, and at the last assessment. After 3 months, TSH decreased by 30%, FT4 by 49% and FT3 by 48%. At the last visit, the decrease was 57% for TSH (p<0.02), 44% for FT4 (p<0.02) and 56% for FT3 (p<0.03).
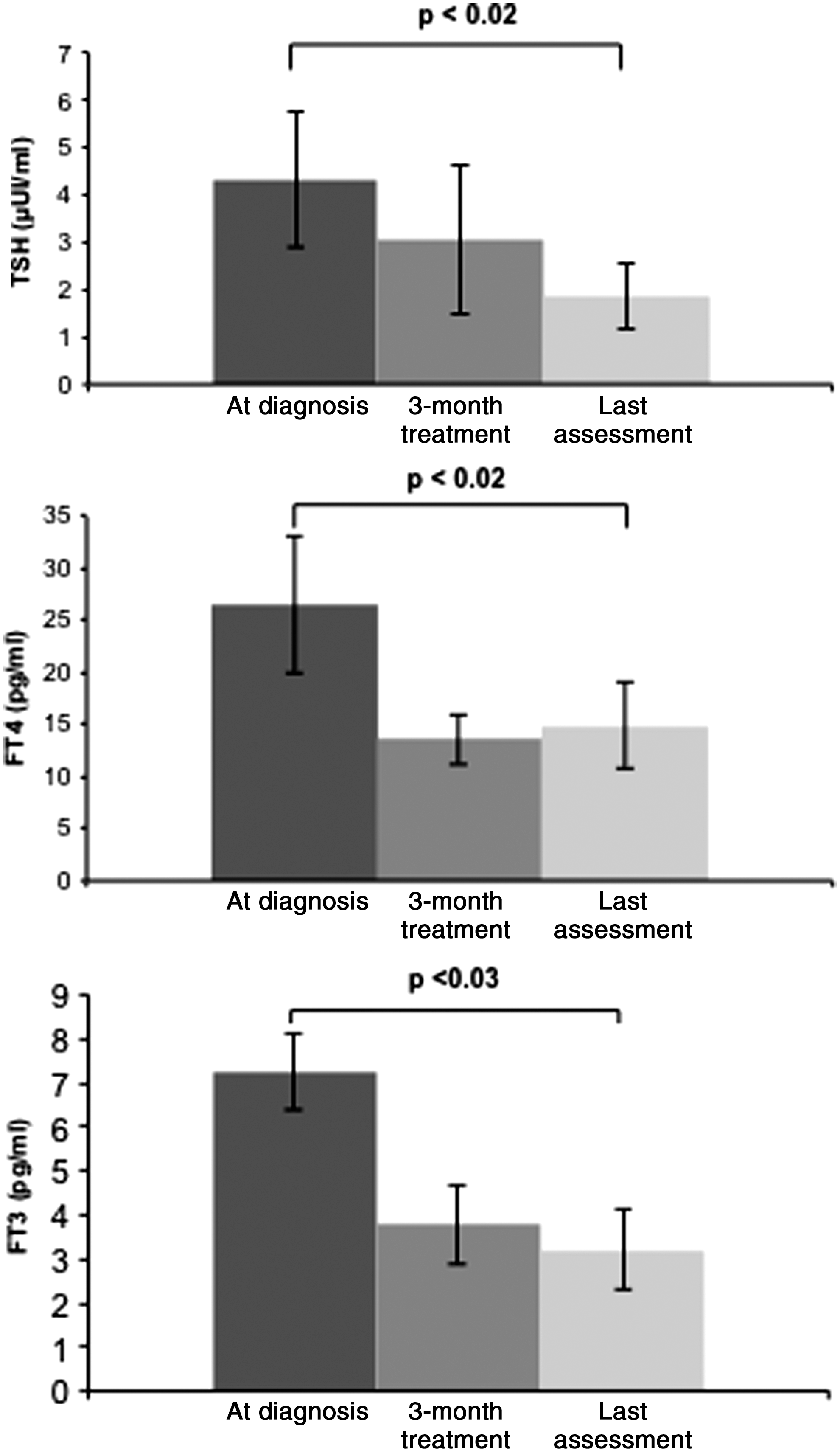
Thyrotropin (TSH), free thyroxine (FT4), and free triiodothyronine (FT3) values before, at 3 months of medical treatment, and at the last assessment in patients with a TSH-secreting pituitary adenoma treated with somatostatin analogs.
Of the three patients with mixed TSH/GH adenomas, control of GH/IGF-1 hyper-secretion was achieved only in patient 7 (GH <1 ng/mL, IGF-1 normal for age and sex), while partial control was obtained in the other two patients.
Tumor control
A decrease in adenoma volume was documented in response to treatment with the somatostatin analogs (at diagnosis 2414±4207 mm3, at the last assessment 1079±1688 mm3) (Table 3, Fig. 2). Adenoma volume increased (+18%) only in patient 4, for whom no hormonal control was achieved.
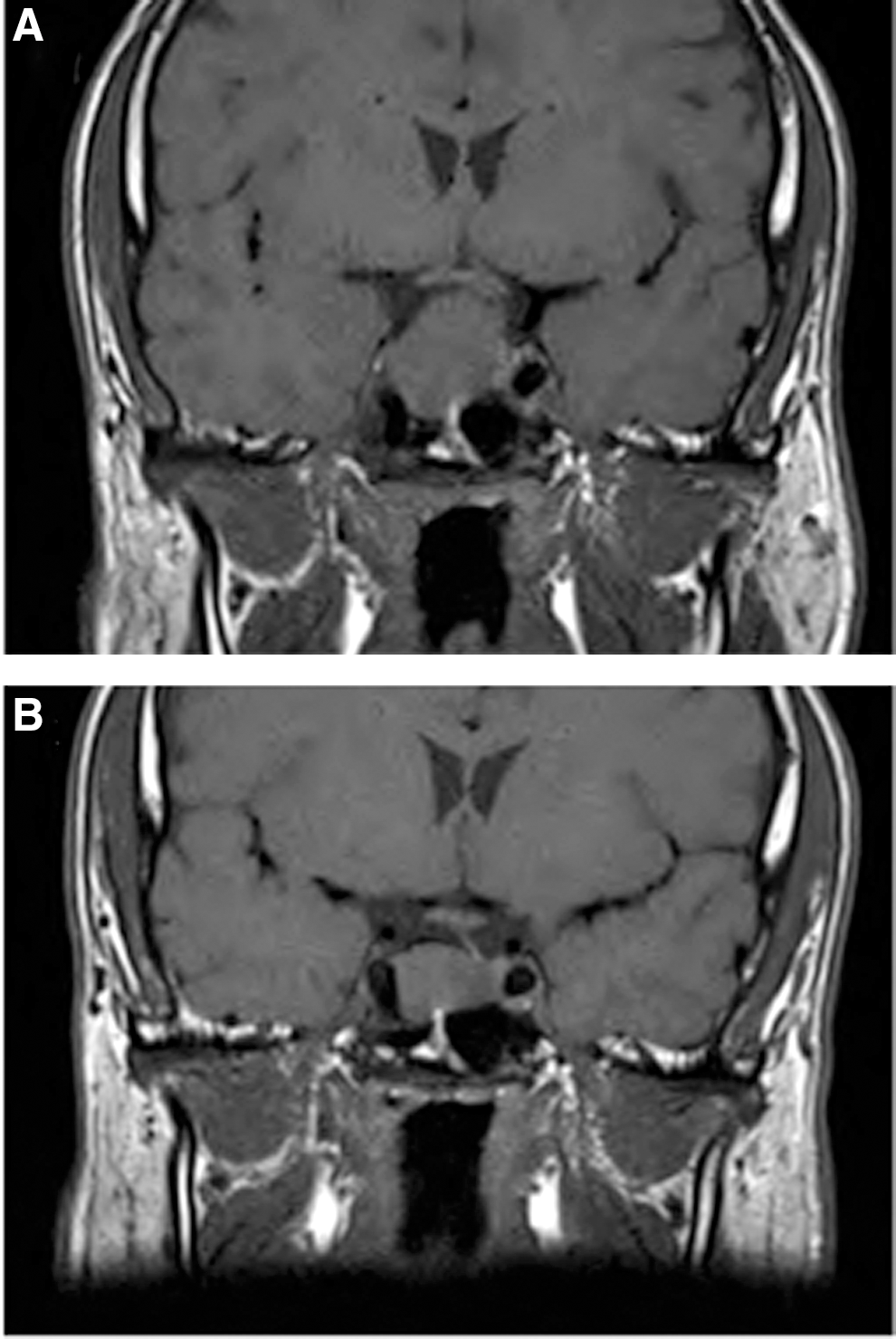
Magnetic resonance imaging of patient 1 before treatment
ND, no data.
Safety
Safety of treatment with somatostatin analogs was good and none of the patients discontinued treatment due to side effects. Patient 7 presented with abdominal pain on initiation of treatment with lanreotide Autogel. Ten days after each injection of octreotide LAR, patient 4 presented with diarrhea lasting 3 days. Treatment with ursodeoxycholic acid was introduced in patient 6 who developed gallbladder sludge 6 months after starting treatment with octreotide LAR, which disappeared on subsequent ultrasound scans. The patient also received pancreatic extract treatment to alleviate the symptoms of diarrhea occurring after injection of octreotide. At initial diagnosis, patient 7 had type 2 diabetes mellitus treated with diet and exercise (glycated hemoglobin [HbA1c ]6.5%). Metformin treatment was introduced after 2 years of treatment with Lanreotide Autogel. The HbA1c was 6.1% at the last visit.
Discussion
This study confirms the hormonal and antitumor efficacy of primary medical treatment with first-generation somatostatin analogs in patients with a pure TSH-secreting pituitary adenoma or a mixed TSH/GH adenoma. Of the 7 patients included in the study, 6 were hormonally controlled at the time of the last visit. Morphologically, a decrease in adenoma volume was observed in 6 out of 7 patients, among them all the patients who presented with a macroadenoma.
Thyrotropin-secreting pituitary adenomas are rare (1,4,12). The standard treatment is surgical adenomectomy, but only 40% to 60% of patients are cured after surgery (1,3,4). Medical treatment with somatostatin analogs or pituitary radiotherapy may then be offered as adjuvant therapy after surgery. The somatostatin analogs reduce TSH secretion in 90% of patients, and in the majority of patients, TSH and thyroid hormone levels are normalized. Few patients underwent exclusively medical treatment. In the study by Van Varsseveld et al. (8), 3 out of 18 patients were treated with somatostatin analogs alone. Of these, 2 patients normalized their thyroid function in the long term, with a decrease in tumor volume on imaging. One of them was considered cured after 4 years of treatment, with a pituitary MRI showing complete regression of the adenoma (9). In the study by Valdes-Socin et al. (10), 7 out of 43 patients were treated exclusively with somatostatin analogs and control of the disease was achieved for all patients. Önnestam et al. (2) reported remission in 2 of 5 patients after long-term treatment with somatostatin analogs; the other 3 patients had been treated for less than 1 year and were not controlled. A recent study assessed the efficacy of surgery and radiation therapy in a large series of 70 patients with a TSH-secreting pituitary adenoma, 70% of whom with macroadenomas (13). Of these patients, only one was treated exclusively with a somatostatin analog and achieved disease control.
In our study, a decrease in FT4 and FT3 of 49% and 48% respectively, with a 30% decrease in TSH, was observed after 3 months of treatment. In 8 patients treated with octreotide for 2 months, Mannavola et al. (14) showed a significant reduction of 42% in FT4, of 50.5% in FT3, and a nonsignificant decrease in TSH (3.8±2.8 μU/mL on day 0 and 2.7±2.8 μU/mL on day 56). The authors explained this significant decrease in thyroid hormones concentrations compared with that of TSH by an alteration in the TSH structure with secretion of TSH molecules with reduced bioactivity. It should be noted that a greater decrease in TSH (57%) occurred in our patients after treatment with a mean duration of 8.5±2.7 years, resulting in a significant decrease in FT4 and FT3 levels compared with baseline. In the study by Mannavola et al. (14), a decrease in FT4 and in FT3 of 83% and 87% respectively occurred in one of the 8 patients and led to hypothyroidism, as in our patient 3 in whom treatment with levothyroxine was instituted. These hormonal data presented here confirm the efficacy of primary treatment with somatostatin analogs of TSH-secreting pituitary adenomas.
Furthermore, we observed tachyphylaxis only in patient 2, which necessitated a dose increase after 3.7 years. For patient 1, dopamine agonist treatment was then added following partial control of TSH and GH/IGF-1 hypersecretion. The efficacy of a combination treatment in pure TSH-secreting adenomas is controversial in the literature (9,11,15). It may be beneficial and effective in mixed TSH/prolactin-secreting adenomas (16,17). On the other hand, somatostatin analogs cause a reduction in the volume of TSH-secreting pituitary adenomas (1). A reduction in the volume of TSH-secreting pituitary adenomas occurred in 6 patients, and a decrease in adenoma volume on MRI persisted in patients 2 and 3 several years after initiation of treatment with somatostatin analogs.
Tolerability of treatment was good in all patients. The treatment was not discontinued in any of the patients due to adverse reactions. While surgical treatment of TSH-secreting pituitary adenomas may be accompanied by complications (anterior and posterior pituitary insufficiency) (18), treatment tolerability with somatostatin analogs is good, as demonstrated by the long-term treatments in acromegaly patients (19,20). The most common side effects are abdominal pain, nausea, diarrhea, and discomfort at the injection site (21). They are usually transient. In our population, three patients (4, 6, and 7) had gastrointestinal adverse reactions. No increased incidence of gallstones was found by liver ultrasound screening, which is consistent with the literature (22). Gallbladder sludge occurring 6 months after octreotide therapy in patient 6 regressed under treatment with ursodeoxycholic acid. Only one patient had type 2 diabetes mellitus at initial diagnosis of the TSH-secreting adenoma and it remained satisfactorily controlled during treatment with Lanreotide Autogel.
Conclusion
This study confirms the efficacy of hormonal and tumor volume control using primary medical treatment with first-generation somatostatin analogs of TSH-secreting pituitary adenomas, and its good safety profile.
While trans-sphenoidal or endoscopic surgery is the standard treatment for TSH-secreting pituitary adenomas, first-generation somatostatin analogs may serve as a medical alternative to surgical treatment, especially in cases where surgery is contraindicated or when the macro-adenoma is invasive, thereby making complete surgical resection difficult. The fact that these treatments are well tolerated defines them a valuable alternative.
Footnotes
Acknowledgment
The authors thank Novartis laboratory (Rueil Malmaison, France) for the help in the preparation of the manuscript.
Author Disclosure Statement
The authors state that no competing financial interests exist. Philippe Caron is consultant and speaker for Ipsen Laboratory and Novartis Laboratory.