
Abstract
Background:
The objective of this study was to describe national trends in robotic thyroid surgery from 2009 through 2013.
Methods:
The University HealthSystem Consortium (UHC) database was searched for patients undergoing robotic thyroidectomy (RT) from 2009 through 2013. Another U.S. institution's RT data, not included in the UHC database, were also evaluated. Patient demographics, institutional volume, comorbid conditions, complications, and cost information were analyzed.
Results:
Sixty-one institutions performed 484 RT during the study period. From 2009 through 2011, U.S. annual RT volume increased from 39 cases to 140. Annual volume dropped to 69 cases in 2012 and 93 cases in 2013. Higher-volume centers reported lower complication rates (p<0.02). Hematoma formation (3.7%) was the most common complication, and there was one death. More than 10% of patients were obese. Brachial plexus injury and axillary skin flap perforations were reported in <1% of cases. Mean cost for a total RT was $13,287 ($5,125–42,444).
Conclusions:
From 2009 through early 2011, there was a steady increase in RT volume, especially among high-volume institutions. In mid-to-late 2011, there was a noticeable drop in RT volume, which significantly altered the projected trajectory of the procedure in this country. Despite higher complication rates, lower-volume centers perform the majority of RT and are also responsible for recent increases in RT utilization patterns in the United States.
Introduction
C
To enhance cosmesis and improve patient satisfaction, endoscopic approaches using extra-cervical incisions were developed but met with limited enthusiasm by surgeons because the small workspace in the neck made the procedures technically difficult and introduced new complications (5 –7). In 2007, surgeons in South Korea pioneered robotic thyroidectomy (RT) with the da Vinci Surgical System to improve the ergonomics of extra-cervical approaches and have since described its use for a wide range of thyroid pathology (8).
In 2009, Kuppersmith and Holsinger introduced RT to North America and initially garnered interest across the United States in re-creating the Korean experience (9). However, in October 2011, Intuitive Surgical, Inc., informed its U.S. clients that they would no longer “provide or facilitate any promotion, training, case observations, proctoring or on-site procedural support for use of the da Vinci System in conjunction with thyroidectomy procedures” (10 –12). The announcement was issued after the company had received multiple letters reporting complications (not isolated to the thyroidectomy application) with the device, in addition to concerns over whether the manufacturer had properly obtained Food and Drug Administration (FDA) approval for RT.
While the announcement likely diminished enthusiasm for RT in the United States, some American institutions have continued providing RT for patients wishing to avoid a neck scar, and several investigators have reported good results (13 –17). Examination of a large database will allow generation of data regarding the recent history of robotic thyroid surgery and will provide a context for future evaluation of relative volume, complications, and costs. This information may be useful for patients, providers, and policy makers regarding use of healthcare resources for surgical treatment of thyroid disease.
Materials and Methods
This study was reviewed and exempted by the UAMS Institutional Review Board. The University HealthSystem Consortium (UHC) consists of 112 academic medical centers and more than 250 affiliated hospitals. Data are compiled from discharge summaries into the Clinical Database/Resource Manager (CDB/RM). The CDB/RM provides an expanded set of comparative demographic, cost, and procedural data as well as analytic tools to support the clinical operations of member institutions. The authors had access to the entire database behind the web portal by special arrangement and collaboration. Outpatient data are a relatively new addition to the originally established UHC inpatient discharge database. Data have been phased in over the last several years and are not considered exhaustive across all member institutions.
Data were accessed in the fall of 2014 and reflect quarterly data collected from 2009 (1st quarter) through 2013 (4th quarter). CDB/RM search strategy was based on the diagnoses of benign and malignant thyroid disease and patients undergoing RT across all UHC member facilities. Comorbidities were differentiated between complications via present-on-admission (POA) code indicators. Specific comorbidities were assigned using Comorbidity Software (v3.7, 2012). Complications or hospital-acquired conditions (HACs) were defined according to the International Classification of Disease, 9th Revision, Clinical Modifications (ICD-9-CM) codes (Table 1). Since encounters are treated as discrete events, unique identifiers were used to link encounters of possible significance for 30 days following the surgery encounters.
The Database/Resource Manager (CDB/RM) data were searched on the basis of ICD-9-CM discharge codes for hospital-acquired conditions (HACs) and any other complications occurring within 30 days of the surgery encounter. Comorbidities were differentiated from complications using present-on-admission (POA) code indicators.
Only UHC institutions performing at least one RT during the study period were included in the analysis. UHC hospital RT volumes were modeled as categorical variables. The total volumes were divided into tertiles: “low volume”=performed one RT during the study period; “moderate volume”=performed between two and four RT during the study period; “high volume”=performed five or more RT during the study period. The indications for intensive care unit (ICU) admission were not directly reported by either database and are not intended to be an indicator of condition severity.
For both outpatients and inpatients, the CDB/RM calculates a risk-adjusted, expected cost based on patient demographics, comorbidities, and Medicare Severity Diagnosis Related Group (MS-DRG) Model. Total charges, defined at the code level, were converted to cost estimates by applying CMS rates of cost to charge. Total cost estimates were aggregated at the patient level and represent the cost to provide care for a particular patient. An adjustment for the regional variation in the cost of labor (area wage index) was also applied to the expense portion associated with labor. Purchase and maintenance for the robotic platform were considered indirect costs and not factored into the total cost analysis.
Another non-UHC academic medical center (Tulane University) provided supplemental data, not included in the UHC database, that were also evaluated. Complications and comorbidities were collected from patient records. For consistency, the supplemental data were reviewed and reported to resemble the CDB/RM output. The databases were similar but not the same. First, specific comorbidity types were not reported for the non-UHC series (patients were merely designated as having one or more comorbidities versus none). Second, total costs were not evaluated. While specific complication types and rates were evaluated, no comparisons between UHC institutions and Tulane were performed because of meaningful differences in the data sets and in order to avoid isolating one institution.
Means, medians, standard deviations, and ranges were used to summarize continuous variables, while proportions, counts, and percentages were used to summarize categorical variables. Group comparisons of continuous variables were made using Welch's two-sided sample t-tests, while Pearson's chi-square tests or Fisher's exact tests were used to analyze categorical responses. A simple linear regression model was used to estimate the average trend in the number of RT cases performed each quarter. The analyses were performed using SAS v9.2 (SAS Institute, Inc., Cary, NC) and R v2.9.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
During the study period, 61 institutions performing 484 RT were identified. The mean±standard deviation (SD) age of the cohort was 45.6±14.2 years (range 13–85 years). Sixty-seven percent of patients were white and 19.4% black. In total, 84.7% of patients had RT for benign thyroid disease and 19.3% for thyroid cancer. Sixty percent of cases were hemithyroidectomies and 17.4% total thyroidectomies. Seven patients (2.2%) in the UHC database (N=314) had simultaneous neck dissections.
From 2009 through 2010, OT volume increased by 10.3% from 16,500 cases to 18,200. RT accounted for 0.24% and 0.70% of all thyroid surgery volume in 2009 and 2010, respectively. National RT volume grew an additional 8.5% between 2010 and 2011 (Fig. 1). In mid-to-late 2011, a significant drop in RT volume was observed across UHC institutions, and national volume fell by more than 50% in 2012. This significantly altered from the projected trend based on the first 24 months of data (Fig. 2). In 2013, RT volume increased by 47.6% from 69 cases to 93. Throughout this period, RT volume never accounted for more than a percent of total thyroid surgical volume.
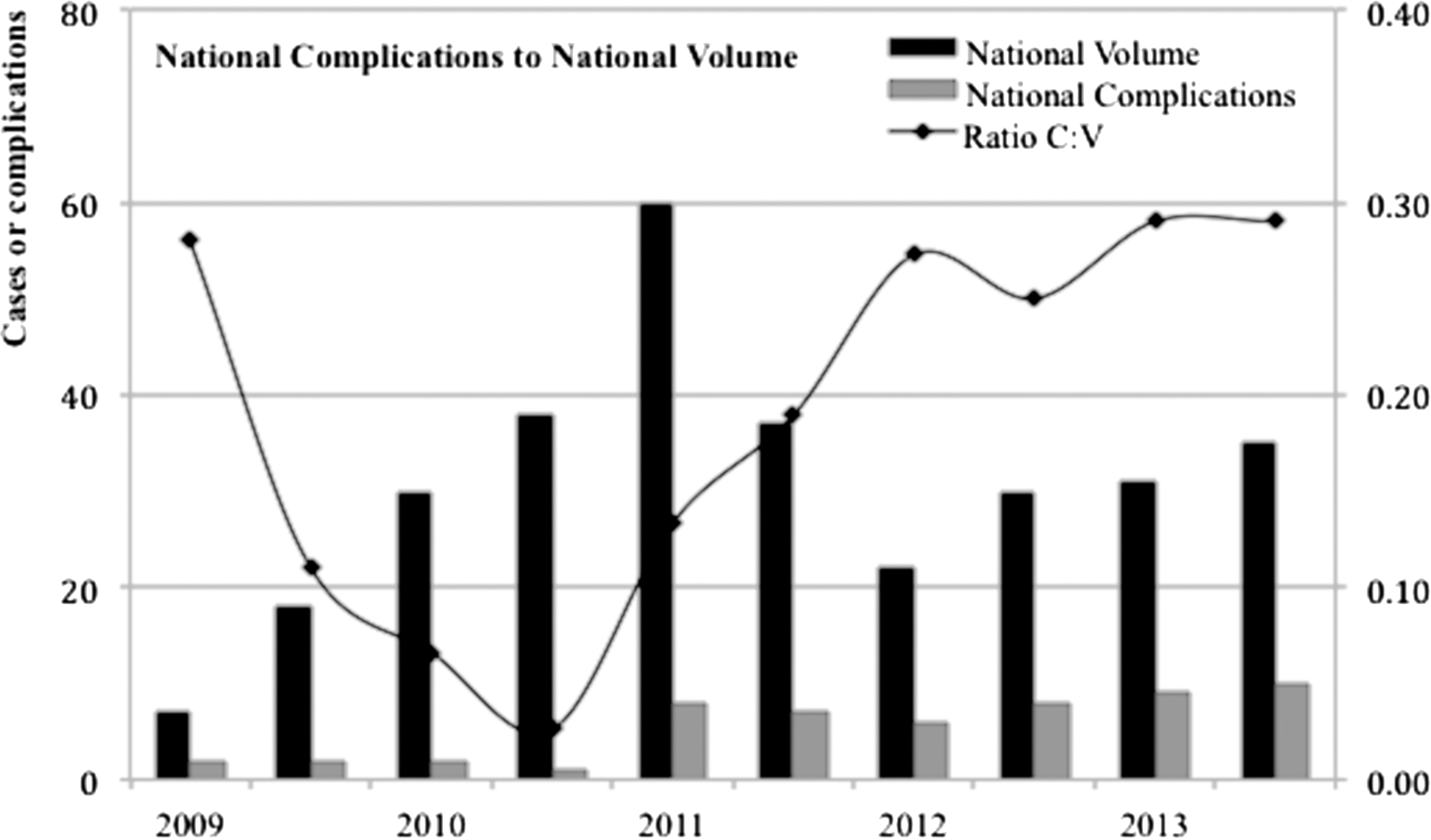
National robotic thyroidectomy volume and complications. After the introduction of robotic thyroidectomy in the United States in 2009, case volume steadily increased for about 18 months and peaked in 2011. In mid-to-late 2011, a noticeable drop in volume was observed across University HealthSystem Consortium (UHC) institutions, and higher relative rates of complications were observed. C:V, complications to volume ratio. UHC only.

Projected and observed robotic thyroidectomy utilization patterns. The dots represent the number of robotic thyroidectomy cases performed each month from June 2009 to December 2013. The solid vertical line marks the end of 2nd quarter 2011. The solid line represents the curve fitted to the data between June 2009 and September 2011. The dashed line represents the trend if the predicted trend continued (simple linear regression model based on the first 24 months of data). The gray region represents the 95% prediction interval.
The U.S. institution performing the highest RT volume performed 170 cases during the study period (33.4 cases per year). No UHC institutions, even those considered “high volume,” averaged 10 or more cases a year. Despite fluctuations in RT volume across UHC institutions, there were no statistical differences in complication rates when compared between the first 10 quarters of the study (2009–2011) and the second 10 quarters (2011–2013; p=0.77).
The UHC institutions performing five or more cases during the study period demonstrated significantly lower complication rates compared with their lower-volume counterparts (Figures 1 and 3). UHC institutions performing fewer than five cases during the study period had complication rates ranging from 41.7% (weighted 47.1%) to 51.9% (weighted 51.2%), respectively. In contrast, institutions performing five or more cases had a significantly lower complication rate of 16.7% (weighted 13.0%; p=0.02).
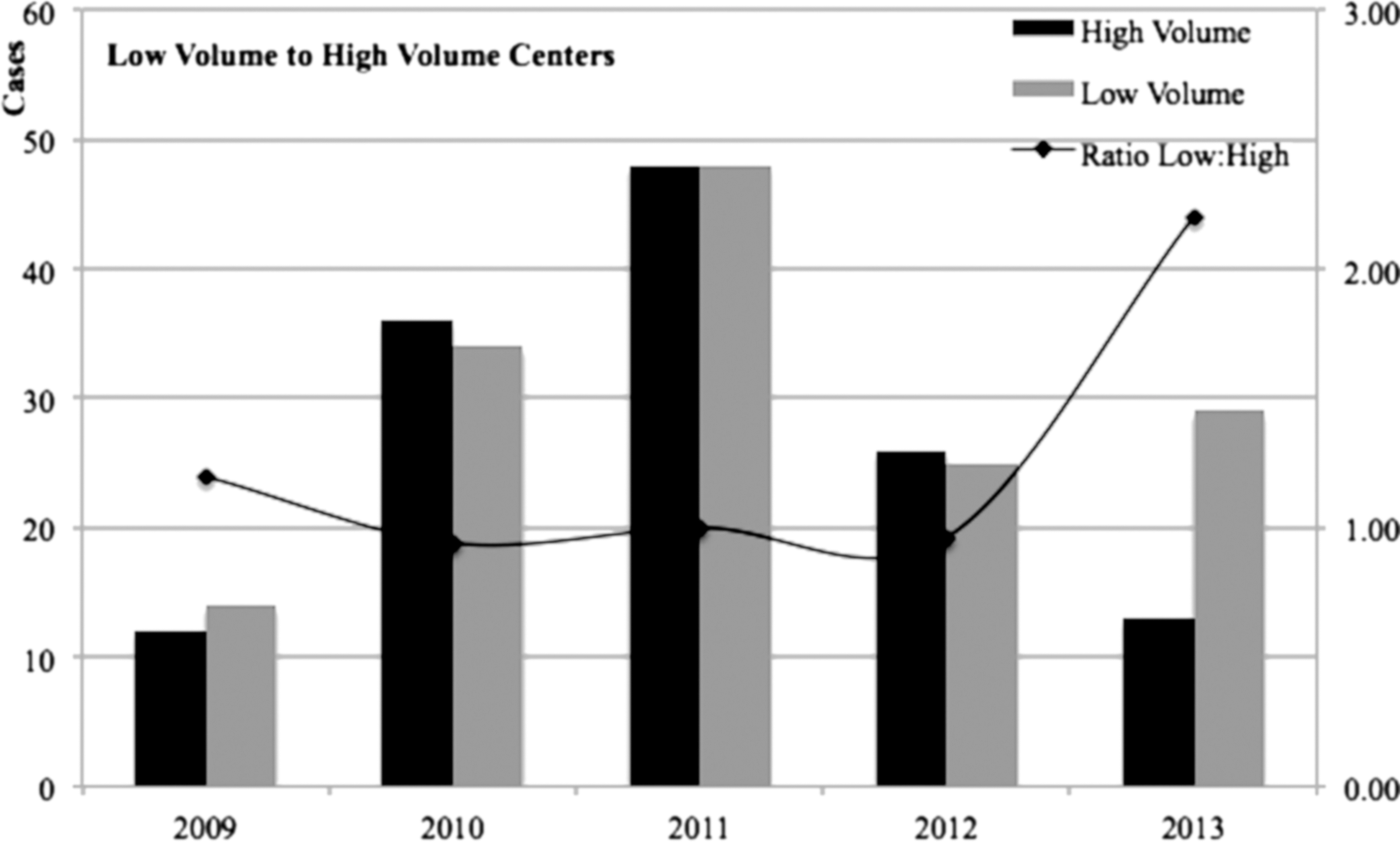
Robotic thyroidectomy trends according to institution volume. Higher-volume centers are not responsible for recent growth in national RT volume. Despite higher complication rates, low-volume RT centers combined perform the majority of robotic thyroid surgery in the United States, and the trend appears to be increasing. UHC data only.
Outpatient RT accounted for 43.3% of all RT. When evaluating only hemithyroidectomy (N=290) and total thyroidectomy patients (N=83), a higher percentage of inpatients (31.5%) had total thyroidectomies compared to outpatients (11.6%; p<0.001). The median length of hospital stay was 1±3.1 days (range 1–31 days) for inpatients, and 57.6% (121/210) of outpatients stayed overnight. Fewer than 10% of UHC patients returned to the hospital within 30 days of discharge, and only one patient was readmitted to hospital. In 2012, outpatient RT cases (N=36) outnumbered inpatient cases (N=33) for the first time (Table 2). When controlled for procedure type, there were no differences among UHC hospitals between inpatient and outpatient mean total costs (p=0.29–0.85). On average, a hemi-RT cost $11,905±$5924 (range $4,178–32,714), and a total RT $13,287±$8820 ($5125–42,444). Cost over time is presented in Figure 4.
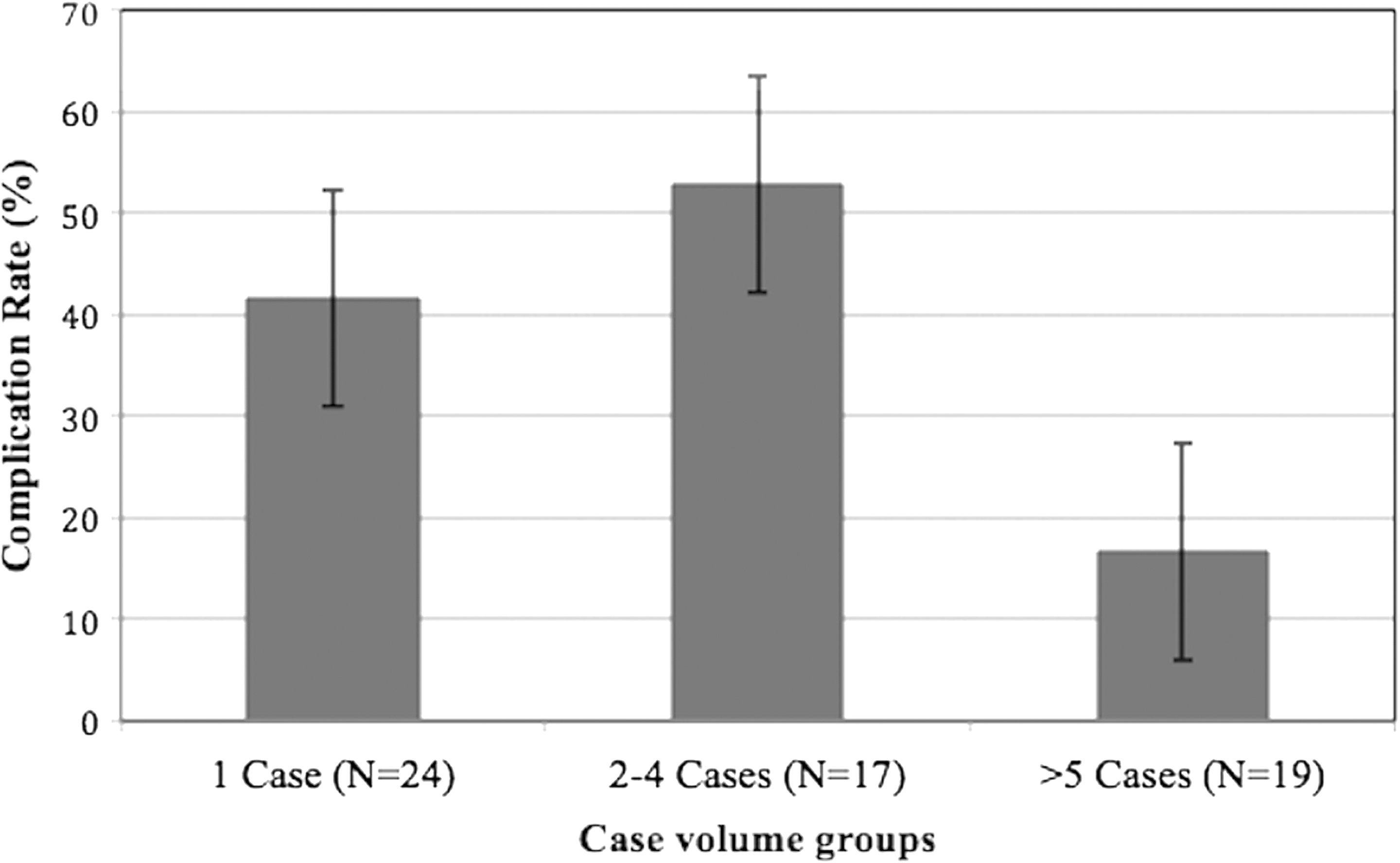
Robotic thyroidectomy trends according to institution volume. Low to moderate RT volume UHC-institutions had complication rates ranging from 41.7% (weighted 47.1%) to 51.9% (weighted 51.2%), respectively. In contrast, the high-volume institutions had a significantly lower complication rate of 16.7% (weighted 13.0%; p=0.02). UHC data only.
Two-sample t-test was used for age and costs, whereas Pearson chi-square was used for sex. N=484 cases; 61 U.S. institutions.
At least one comorbidity was present in 45.0% (218/484) of patients (Table 3). The four most prevalent comorbidities among UHC patients (N=314) were hypertension (32.8%), hypothyroidism (11.9%), obesity (10.8%), and metastatic cancer (10.4%). At least one complication was reported in 23.1% (111/484) of all cases (Table 4). The most common complications were hematoma formation (3.7%), hypocalcemia (3.1%), and recurrent laryngeal nerve damage (2.5%). Brachial plexus injuries were observed in four cases (0.8%), and accidental laceration/perforation was reported in one case (0.2%). Finally, one death was reported in the series (0.02%). The patient was a 68-year-old white male with a nontoxic multinodular goiter who subsequently developed cardiac arrest during his hospital admission. The patient had multiple comorbid conditions including hypertension and alcohol abuse. The patient expired on postoperative day 6 in the ICU.
N=314 cases; 60 institutions; University HealthSystem Consortium (UHC) only.
N=484 cases; 61 institutions.
Discussion
Between 2007 and 2011, surgeons in South Korea performed more than 6000 RT cases with less pain after surgery, faster recovery times, shorter hospital stays, improved patient satisfaction, and comparable operative outcomes versus traditional techniques (8,15,18). Koreans have a higher incidence of subcentimeter nodules (60% vs. 20% in the United States), smaller body size (percentage of patients with a body mass index >30 is 10 times more in the United States than it is in Korea), and smaller thyroidectomy resections (average volume resected in the United States is double that in Korea) (18 –22). Due to such differences, the Korean data have been heavily criticized in the United States for not being applicable when predicting outcomes in American populations (20 –22).
In July 2009, Intuitive Surgical, Inc., began promoting its robotic system in the United States, under the general laparoscopic surgery FDA clearance, for its use in thyroidectomy procedures (10,11). Shortly thereafter, North American institutions began reporting their initial experiences with RT (9,23 –25). U.S. surgeons performing RT in high volumes soon demonstrated that, with some slight modifications in patient arm positioning and minimizing the amount of robotic arm collisions during surgery, RT could technically be implemented in their patient populations without significantly increasing operative time or complications (9,23,25 –27).
Brachial plexus injury and axillary skin flap perforations are complications unique to robotic thyroid surgery and not observed after open thyroidectomy. Brachial plexus injury results from overstretching of the lesion-side arm during surgery. The injury presents with pain or movement difficulties in the shoulder or upper arm but generally resolves spontaneously within a few months. Some have cautioned that obese patients may require greater traction during surgery and for potentially longer durations, which may result in higher rates of complications. In the present data, while more than 10% of RT patients were obese, brachial plexus injury (0.13%) was comparable with Korean reports (0.1–0.3%) (5,8,18). Similarly, axillary skin flap perforations were within an equivalent range (0.9–0.1%) (5,8,18).
Across the globe, the most important factor impacting RT growth appears to be cost (higher than conventional techniques) relative to the amount the payer is willing to reimburse (15,21,28,29). In South Korea, where the procedure has been heavily marketed, there is a graduated reimbursement system for thyroidectomy depending on the technique performed (20). Compared with OT, endoscopic thyroidectomy and RT receive double and quadruple reimbursement, respectively (20). In Japan, where much of the remote-access surgical technology developed, there is no difference in compensation across the thyroidectomy techniques. Perhaps for this reason, RT volume in Japan has plummeted in the last several years despite initial enthusiasm for the procedure (2,20,30). There are similar cultural concerns regarding cervical incisions in both Korea and Japan. Like Japan, there is currently no difference in reimbursement for RT and OT in the United States, despite the increased cost associated with RT (13). Thus, in the context of escalating healthcare costs, there remains a financial disincentive for widespread implementation of RT in the United States.
In 2013, approximately 422,000 procedures of all types were performed with the da Vinci Surgical System in the United States, compared with approximately 376,000 and 292,000 in 2012 and 2011, respectively (31). The growth in robotic surgery in the United States from 2011 to 2013 was driven by increases in gynecologic and general surgery procedures (31). From the present data, despite early U.S. popularity of the procedure from 2009 through 2011, RT has not contributed to overall growth of robotic surgery in the United States. Since its introduction to the United States, RT has never accounted for more than 1% of total thyroid surgery volume. Based on the present data, there are no trends that suggest that this will change anytime in the near future.
While many centers have abandoned the technique, RT continues to be performed at select U.S. institutions. It is possible that patients desiring a “scar-less” thyroidectomy are now traveling to a handful of high-volume institutions that have established their skillful reputation and proficiency with RT. Considering RT requires approximately 45–50 cases to become proficient and higher-volume centers have significantly lower rate of complications (16,32,33), consolidation of volume into higher-volume centers could be beneficial for patients. In the present series, the highest-volume institution performed more than 30 RT cases per year throughout the five-year period. However, recent trends suggest that higher-volume centers are not responsible for the recent growth in national RT volume (Fig. 5).
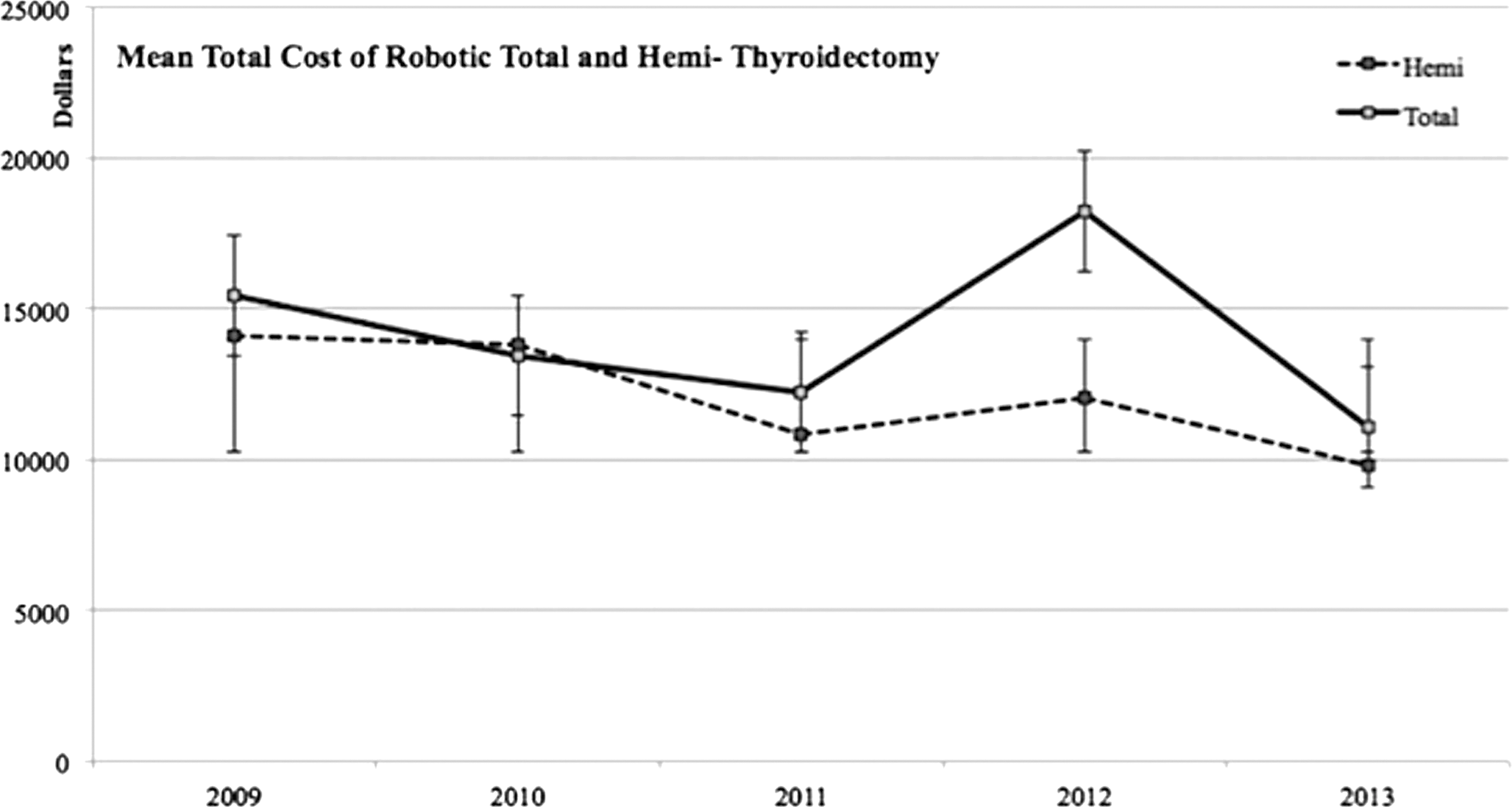
Average total cost of robotic thyroid surgery over time. Total cost was defined as the cost necessary to produce care at the patient level. Purchase and maintenance for the robotic platform were considered indirect costs and not factored into the total cost analysis. When controlled for procedure type, there were no differences among UHC hospitals between inpatient and outpatient mean total costs (p=0.29–0.85). UHC data only.
There are major limitations to consider with the present study. Common complications for thyroid surgery are likely under-reported. Thyroid surgery complications are often diagnosed in the outpatient clinic (unilateral vocal fold paralysis, hematoma, wound infection, or hypocalcemia) that might not transmit to central electronic medical records. Not all member institutions enter clinical data into the UHC database, even if the outpatient clinic encounter occurs in a hospital-based clinic.
Another shortcoming of this study is that the same clinical problem is often coded differently and/or inaccurately. Further, procedure and diagnostic codes could be entered retrospectively and not necessarily at the time of the event. Poor physician documentation may compromise data accuracy. Attempts to overcome inherent shortcomings of the database design with respect to the thyroidectomy population will continue through additional analysis and ongoing research.
Conclusion
The 2011 announcement that the surgical robot manufacturer no longer supported RT in the United States appears to have had an impact on the nascent growth of the technique in the United States. Despite higher complication rates, lower-volume centers collectively perform the majority of volume in the United States and are also responsible for the recent increases in RT utilization patterns. Decentralization of RT away from high-volume centers may be associated with observed increases in RT complication rates.
Footnotes
Acknowledgment
Presented at the 84th Annual Meeting of the American Thyroid Association, Coronado, California, October 29–November 2, 2014.
Author Disclosure Statement
No competing financial interests exist.