
Abstract
Background:
Trends in the epidemiological profiles of differentiated thyroid cancer (DTC) have shifted the disease spectrum. This study aimed to evaluate the recurrence rates and identify factors related to persistent disease in a contemporary cohort of patients with DTC.
Methods:
A cohort of DTC patients submitted to total thyroidectomy followed in a referral center were included in the study. “Disease free” was defined as no clinical, imaging, or biochemical evidence of tumors. “Recurrence” was defined as evidence of disease in a patient who had been previously classified as disease free.
Results:
A total of 786 patients were included. The mean age at diagnosis was 45.8±15.1 years, 81.6% were female, and papillary thyroid cancer accounted for 86.6% of cases. The median tumor size was 2.0 cm, 28.5% had lymph node involvement, and 6.1% had distant metastases. Disease status after the initial therapy was available for 548 patients: 357 (65.1%) were disease free, and 191 (34.9%) had persistent disease (90 biochemical and 101 structural disease). In multivariate model analyses, the variables male sex, lateral lymph nodal involvement, distant metastasis, and 2009 ATA high-risk classification were independent prognostic factors for persist disease. After a four-year follow-up (two to eight years), 97.2% of the patients who had been classified as disease free remained in disease remission status. Of the 10 (2.8%) patients with recurrent disease, eight presented biochemical and two cervical structural disease.
Conclusions:
The majority of the DTC patients who were considered to be disease free after the initial treatment remained with this status at long-term follow-up. These data suggest that less intensive follow-up may apply for these patients.
Introduction
D
Several different staging systems have been proposed for DTC patients based on clinicopathological findings that are available soon after surgical therapy, which have been developed to predict the risk of death but not of recurrence (11). The TNM staging system of the American Joint Committee on Cancer (TNM/AJCC) and the Metastasis, Age, Completeness of Resection, Invasion, and Size (MACIS) are the most commonly used systems. Both of them have limitations, since they do not consider the response to treatment and do not predict persistent disease and recurrence accurately. In recent years, some authors have suggested that risk stratification can be further improved if the initial risk estimate systems are actively modified over time based on the response to therapy and the course of the disease. These novel risk stratification systems seem to identify those patients with a greater likelihood of progressing toward long-term remission after initial therapy (12 –15).
The current thyroid cancer management guidelines advise that patients with DTC should be followed at least annually for an undetermined period of time (16,17). Because of improvements in the medical armamentarium with highly sensitive thyroglobulin measurements and high-resolution ultrasonography, the long-term follow-up is primarily based on the likelihood of late recurrences (18). This strategy, which lacks evidence of benefit in terms of survival or well-being, adds the burden of unnecessary examinations and medical appointments to patients and health systems.
Here, the objective of the present study was to estimate overall recurrence rates and identify factors related to persistent disease in a contemporary cohort of patients with DTC attending a referral center hospital in southern Brazil.
Material and Methods
Patients and study design
A cohort of DTC patients who attended the Thyroid Outpatient Clinic of the Endocrine Division of Hospital de Clínicas de Porto Alegre (HCPA), a tertiary care, university-teaching hospital in southern Brazil from 2000 to 2014, was evaluated. The inclusion criterion was the histological diagnosis of DTC, and there were no exclusion criteria. The study was approved by the Institution Ethical Committee of the HCPA.
Treatment protocol and follow-up
The DTC treatment protocol consisted of performing a total thyroidectomy, administering radioactive iodine (RAI) for remnant ablation or adjuvant therapy, as indicated, and using levothyroxine suppression. Decisions regarding cervical lymph node dissection were made based on the discretion of the surgeon team at the center in which the patients underwent the first surgery. The follow-up duration was defined as the time between the thyroidectomy and the last medical visit to the clinic.
The ablation protocol used RAI activities prescribed at the attending physician's discretion. A low-iodine diet was prescribed for two weeks before the RAI administration until two days afterward. The RAI was administered under conditions of endogenous hypothyroidism (thyrotropin [TSH] >30 mIU/L) after withdrawing levothyroxine for at least three to four weeks. A post-therapy whole body scan (WBS) was performed seven to ten days after the RAI administration.
In the first evaluation, the following data were recorded for each patient: patient demographics, tumor characteristics (e.g., the date of diagnosis, histological features, extension, and lymph node involvement) and treatment (e.g., surgery, RAI, and other interventions). Each patient was classified using the 7th edition of TNM/AJCC staging system (I, II, III, or IV) (11). N0 status was defined considering the clinical examination of the neck, preoperative and postoperative neck ultrasound (US) imaging, macroscopic examination during surgery, and pathological examination in patients with lymph node resection. The baseline tumor stage and the risk for persistent/recurrent disease were also defined based on the proposed classification using the 2009 American Thyroid Association (ATA) guidelines (17).
The follow-up protocol called for an initial assessment at three to six months after the initial treatment, which included physical examination of the neck and measurements of the serum thyroglobulin levels under TSH suppression (Tg-T4), as well as and antithyroglobulin antibodies (TgAb). In a second evaluation, 6–12 months after the initial treatment, serum Tg (sTg) was measured under conditions of a stimulated TSH with endogenous hypothyroidism (TSH >30 mIU/L). Neck US was also performed in this first year of follow-up. At this point, the patients were classified according to their response to initial therapy (see below in outcomes section), and those patients classified as disease free were scheduled for annual visits, during which a physical examination of the neck and measurements of Tg-T4 and TgAb were performed. Patients with persistent disease were scheduled for the same examination twice a year. Additional imaging studies (e.g., dx-WBS, computed tomography [CT]) were performed, as needed, whenever the clinical or laboratory findings raised the suspicion of persistent or recurrent disease.
Outcomes
In the first year of follow-up, the response to initial therapy was assessed based on the serum Tg levels, neck US, post RAI WBS (whenever available), and appropriate additional imaging.
“Disease free” was defined as having no clinical or imaging evidence of tumor (i.e., no uptake outside the thyroid bed on the post-treatment WBS and no imaging evidence of tumor on neck US), undetectable (<1 ng/mL) serum Tg-T4 levels, and sTg levels <2 ng/mL.
Persistent disease was subdivided into biochemical or structural disease. Biochemical disease was defined as Tg-T4 values ≥1 ng/mL or sTg levels ≥2 ng/mL, without structural evidence of disease. Structural disease of the cervical lymph node was defined by evidence on imaging studies or biopsy-proven disease (cytology or histology), with or without abnormal Tg values. Patients who were diagnosed with persistent disease were evaluated for additional treatment (e.g., surgery, radioiodine, and external-beam radiation), depending on the involved site(s).
Recurrence was defined as new biochemical or structural evidence of the disease detected in a patient who had been previously determined to be disease free.
Laboratory analysis
Serum Tg measurements were conducted using immunoradiometric assays (from 2000 to 2002 radioimmunoassay, 2002 to 2010 electrochemoluminescence, and 2010 until the present chemiluminescence) that indicated functional sensitivities of at least 1 ng/mL. TgAb were measured using the passive agglutination method from 2000 to 2010 and by chemiluminescence from 2010 until the present. After implementation of every new technique, the necessary procedures of standardization and validation were performed. TSH levels were measured by electrochemiluminescent immunoassay (ADVIA Centaur XP; Siemens, Tarrytown, NY). These tests were all conducted in the central laboratory of the HCPA.
Statistical analysis
The clinical and laboratory data, which are reported as the mean±standard deviation (SD) values, or as the median with percentiles 25 and 75 (continuous variables), or as absolute numbers and percentages (categorical variables), were compared using an unpaired Student's t-test, Mann–Whitney U-test, or chi-square test, as appropriate.
Generalized linear models with a log link and Poisson errors were used to estimate relative risks and confidence intervals for persistent disease. Using univariate regression analysis, clinical variables, such as sex, age at the time of diagnosis, histological subtype, multicentricity, tumor size, lymph nodal and distant metastases, 2009 ATA risk, and TNM AJCC stage, were evaluated as potential prognostic factors of DTC. The factors that presented p<0.10 in the univariate analysis were included in the multivariate models.
All tests were two-tailed, and all analyses were performed using the SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). A two-tailed p<0.05 was considered to be statistically significant.
Results
Clinical characteristics
The clinical and oncological characteristics of the 786 patients are described in Table 1. The mean patient age at the time of diagnosis was 45.8±15.1 years, and there were 641 (81.6%) women. PTC was diagnosed in 681 (86.6%) patients. The median tumor size measured 2.0 cm; 224 (28.5%) patients had lymph node metastases, and 48 (6.1%) patients had distant metastases. The TNM/AJCC classification was as follows: 484 (61.6%) patients were stage I; 92 (11.7%) patients were stage II; 93 (11.8%) patients were stage III; and 96 (12.2%) patients were stage IV. The TNM/AJCC stage was unknown for 21 patients. According to the 2009 ATA classification, the risk level was low in 388 (49.4%) patients, intermediate in 327 (41.6%) patients, and high in 71 (9.0%) patients. Seventy-two (9.2%) patients were positive for TgAb.
The tumor size was unavailable in these patient subgroups (all patients were older than 45 years of age).
TNM/AJCC, TNM staging system of the American Joint Committee on Cancer; ATA, American Thyroid Association; TgAb, antithyroglobulin antibody.
All patients underwent surgery with curative intent (total thyroidectomy and neck dissection, as necessary). RAI for remnant ablation or adjuvant therapy was administered in 658 (83.7%) patients (mean dose 109.4±38.0 mCi; range 30–250 mCi). A post-therapy WBS was performed in 566 patients; 28 (4.9%) patients showed no uptake, 506 (89.4%) presented only cervical uptake, and 32 (5.7%) distant metastases.
Response to initial therapy
Data concerning the disease status after the initial therapy (response to therapy) were available for 548 patients: 357 (65.1%) patients were considered to be disease free, and 191 (34.9%) patients had persistent disease. Of those patients diagnosed with persistent disease, 90 patients had biochemical disease, and 101 patients had structural disease (62 patients with cervical metastasis and 39 patients with distant metastasis). The clinical and oncological characteristics of the 238 patients who were not included in this analysis were similar compared to the whole sample population (p>0.05).
To investigate the factors associated with the disease status after the initial treatment, the patients were grouped into disease free or persistent disease categories. Univariate analysis indicated that male sex, multicentric tumors, larger tumor size, lymph node and distant metastases, and intermediate and high 2009 ATA risk classifications were all associated with persistent disease (Table 2). An additional analysis using a multivariate model that included all variables with p<0.10 in the univariate analysis and disease status as the dependent variable showed that male sex, lateral lymph nodal involvement, distant metastasis, and 2009 ATA high-risk classification were independent prognostic factors for persistent disease (Table 3).
Recurrence rate
All 548 patients were re-evaluated after a median four-year follow-up (interquartile range 2–8 years). Of the 357 patients who were considered to be disease free in the first evaluation, 347 (97.2%) continued to be disease free. Remarkably, only 10 (2.8%) patients presented recurrences (eight patients with biochemical disease and two patients with cervical structural disease; Table 4). All structural recurrences were limited to the cervical lymph nodes.
RAI, radioactive iodine; sTg, stimulated thyroglobulin; Tg-T4, thyroglobulin under suppressive LT4 therapy.
All patients with persistent disease (biochemical or structural) were evaluated for additional therapy (i.e., surgical interventions or RAI) at the discretion of the attending physician. Among the 90 patients with biochemical disease after the initial therapy, 14 (15.6%) were considered to be disease free at follow-up. Interestingly, eight (57%) of them did not receive any additional treatment, and the Tg levels fell spontaneously. The remaining six patients received an additional RAI administration. Seventy (77.8%) patients remained with biochemical disease, and only six (6.6%) patients evolved to having cervical structural disease at the four-year follow-up. Among the patients (n=101) diagnosed with structural disease, only 11 (10.9%) became disease free after additional treatment (two patients underwent only surgical reintervention, and nine patients underwent surgery+RAI therapy); 15 (14.9%) patients exhibited biochemical disease, and 75 (75.2%) patients continued with structural disease (Fig. 1). Additional analyses, including only those patients (n=292) with at least five years of follow-up, showed similar results.
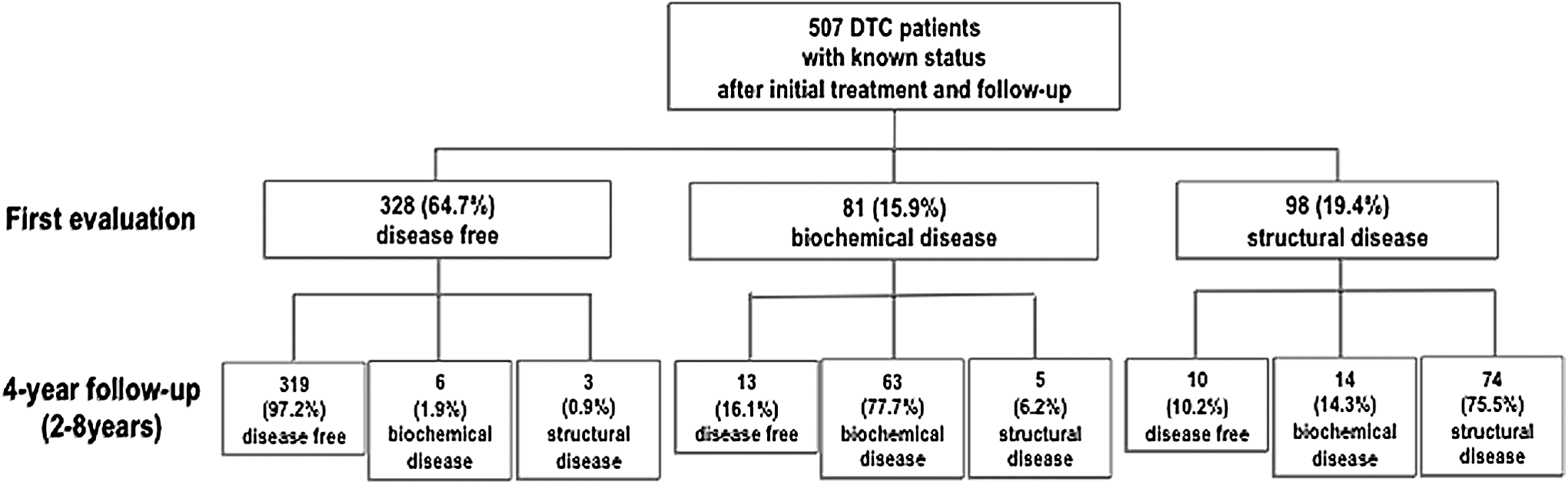
Follow-up outcomes, according to the patients' responses to therapy. DTC, differentiated thyroid carcinoma.
The group of patients with recurrence has heterogeneous clinical and pathological characteristics (Table 4). The median tumor size measured 3.9 cm (range 0.5–6.5 cm); five (50%) patients had lymph node metastases, and none of them had distant metastases. The TNM/AJCC classification was as follows: seven (70%) patients were stage I, one (10%) was stage II, and three (30%) were stage IV. According to the 2009 ATA classification, the risk level was low in three (30%) patients, intermediate in five (50%), high in two (20%). All patients underwent total thyroidectomy and received RAI. The median time for recurrence was six years (range 2–12 years). Comparing this group of patients with the patients who remained free of disease on the follow-up examination, no predictor of recurrence could be identified.
Discussion
Recently, it has been suggested that DTC might be overdiagnosed because the incidence is increasing, but the mortality rate is stable (6,19). Changes in the epidemiological profile and advances in the follow-up management of these patients could also lead to a similar result, the “over follow-up effect,” with unnecessary surveillance, diagnostic tests (thyroglobulin measurements, imaging studies, and fine-needle aspiration biopsies) and medical appointments because the majority of the patients can be defined as disease free at the first evaluation after initial therapy, remaining disease free in the long-term follow-up.
The primary purpose of surveillance after initial therapy in patients with malignant neoplasia is the early identification of those patients with recurrent disease who might potentially have more favorable outcomes with additional interventions. The recurrence timing and patterns, particularly in the case of metastatic disease, vary according to the type and stage of cancer at the time of diagnosis. There are several malignancies with follow-up guidelines (20,21), and in the majority of cases, even in those more aggressive cancers, life-long testing to evaluate for recurrent or metastatic disease is not recommended in otherwise asymptomatic cancer survivors. In the case of DTC, the optimal follow-up strategy has not been determined, and the majority of the patients, even those asymptomatic and considered free of disease, are followed for an undetermined time period with biochemical and radiological examinations.
The discrepancy highlighted above is greater when we consider the current low recurrence rate in patients with DTC. The present study demonstrates that the recurrence rate in patients who had been classified as disease free after the initial therapy was only 2.8% after a median follow-up of four years. Notably, the recurrence rate for cervical structural disease was even lower at 0.6% (2/357 patients). These results align with the findings of other contemporary studies that showed that the actual recurrence rate for DTC is approximately 1–4% (10,12,15,22 –26). All these studies defined recurrence as newly detected biochemical or structural disease following any period of no evidence of disease. Consequently, only a patient who had achieved a disease free status could be classified as having disease recurrence. Of note, when analyzing the group of 81 patients diagnosed with persistent biochemical disease, it was observed that 10% (eight patients) became disease free without any additional treatment, whereas only 6.6% (five patients) evolved to cervical structural disease, a finding that raises questions about the clinical significance of a detectable thyroglobulin without structural disease in the follow-up of DTC.
This study has some limitations. Although a median four-year period is a reasonable follow-up for assessing clinical outcomes, some professionals may be concerned that a longer follow-up is required to assess the risk of late recurrences and death. However, as already demonstrated by other groups, disease recurrence occurs mostly in the first two to five years of follow-up (10,26). Another possible limitation is that the majority of the patients received RAI, and the disease course may be different in low-risk patients who do not receive RAI, as currently advocated. Nevertheless, one should note that all patients with disease recurrence received RAI as adjunctive therapy. On the other hand, the fact that all patients included in the present study were followed at a single institution ensures a similar therapeutic approach and follow-up strategy, thereby enhancing the validity of the data. Furthermore, the nonexclusion of patients with positive TgAb and those at high risk for recurrence enhances the external validity of the findings.
In conclusion, the majority of patients who were defined as disease free after the initial treatment remained disease free after a long follow-up and might not require active, life-long surveillance. The data, derived from a cohort of DTC patients from a South American referral center, add to the evidence to review the current protocol of follow-up for patients with no structural or biochemical signs of persistent disease after the initial evaluation. In the authors' view, a conservative approach consisting of determining only Tg-T4 annually for the first three years of follow-up and, based on the methodology used for Tg measurements, sTg testing, might be considered. For those patients who remain disease free, Tg-T4 determination can be considered biannually up to 10 years with no further follow-up after this period. This approach would provide a more effective follow-up strategy for DTC patients, with more efforts and resources directed at those patients at high risk for recurrence and progressive disease.
Footnotes
Acknowledgments
This work has been made possible due to grants from CNPq, CAPES, FIPE, and PRONEX/FAPERGS. We wish to thank the surgeons of our Hospital, Dr. Alceu Migliavacca, Dr. José Ricardo Guimarães, and Dr. Diego Mossmann, for surgical management of our patients.
Author Disclosure Statement
R.S.S., J.M.D., D.A., A.B.Z., and A.L.M. have nothing to declare.