
Abstract
Introduction:
Chronic kidney disease (CKD) impairs thyroid hormone (TH) metabolism and is associated with low serum triiodothyronine (T3) concentrations in patients with a low glomerular filtration rate (GFR). Whether this results from decreased T3 formation from thyroxine (T4) by impaired 5′-deiodinase (DIO) activity and/or enhanced degradation of T3 and increased reverse triiodothyronine (rT3) formation from T4 by elevated 5-DIO activity remains unclear. Both activating 5′- and the inactivating 5-deiodination of TH are catalyzed by three selenium (Se)-dependent DIO isoenzymes. Selenoprotein P (SePP) is the major constituent of serum selenium, and functions as Se transport protein from liver to kidney and several other organs. This study tested the hypothesis that serum SePP and TH status are associated with the degree of renal impairment in patients with CKD.
Patients and Methods:
A total of 180 CKD patients (stages 1–5) and 70 chronic hemodialysis (CHD) patients undergoing hemodialysis three times per week for at least two years were prospectively investigated for clinical data, parameters of renal function, serum TH profile (thyrotropin, T4, free thyroxine [fT4], T3, free triiodothyronine (fT3), rT3, thyroxine-binding globulin [TBG]), C-reactive protein (CRP), and serum SePP.
Results:
In CKD patients, renal function was negatively associated with SePP concentration (standardized β = −0.17, p = 0.029); that is, SePP concentrations increased in more advanced CKD stages. In contrast, significantly lower SePP concentrations were found in patients on hemodialysis compared with CKD patients (M ± SD = 2.7 ± 0.8 mg/L vs. 3.3 ± .9 mg/L; p < 0.001). Notably, in CKD patients, the SePP concentration was negatively associated with T4 (standardized β = −0.16, p = 0.039) and fT4 (standardized β = −0.16, p = 0.039) concentrations, but no association was found with T3, fT3, rT3, T3/T4, rT3/T3, rT3/T4, or TBG concentrations. The SePP concentration was also negatively associated with CRP levels (standardized β = −0.17, p = 0.029). In the CHD group, no association was detected between SePP and the investigated TH parameters.
Summary and Conclusion:
Impaired renal function is positively correlated with serum concentrations of SePP. In patients undergoing CHD treatment, SePP concentrations were significantly reduced, but the TH profile remained unaffected. These findings indicate an important contribution of kidney function on serum SePP homeostasis, and consequently on Se status.
Introduction
C
Low serum Se concentrations have been described in chronic hemodialysis (CHD) patients (6 –9). The clinical impact of hyposelenemia in young hemodialysis patients was shown in a recent study where low serum Se concentrations were associated with a high mortality rate (10).
Moreover, patients with impaired renal function show specific features of nonthyroidal illness (NTI), such as low T3 and T4 concentrations in the presence of normal thyrotropin (TSH) values (11,12). However, rT3 concentrations are also low in CHD, in contrast to other forms of NTI with normal renal function, suggesting differences in TH degradation pathways (13).
Data on SePP status in CKD and its potential contribution to altered TH metabolism in renal tubular epithelium are missing. Therefore, this study prospectively evaluated both SePP and TH status in a large cohort of patients with various degrees of CKD and in CHD patients. It was hypothesized that alterations in SePP concentrations with renal failure may be associated with concomitant changes in T3/T4 and rT3/T3 profiles.
Patients and Methods
A total of 180 patients (45 females) who presented to the authors' nephrology outpatient department for further workup of presumed kidney disease were prospectively evaluated. In addition, 70 patients on CHD treatment (three times per week for four to six hours; mean time on hemodialysis 3.4 years) were studied. Exclusion criteria were medication known to influence TH function (amiodarone, high-dose cortisone, and/or high-dose furosemide therapy, anti-epileptics, heparin, lithium) and TPO-antibody positivity (14).
Serum creatinine, C-reactive protein (CRP; normal range <0.5 mg/dL), and serum albumin (normal range 3.5–5.5 mg/dL) were determined by standard methods, and the GFR was estimated using the abbreviated Modification of Diet in Renal Disease (MDRD) according to the MDRD formula (15). CKD stages were defined as follows: CKD stages 1 and 2 (n = 2): eGFR >60 mL/min; stage 3a (n = 23): eGFR 45–59 mL/min; stage 3b (n = 43): eGFR 30–44 mL/min; stages 4 and 5 (n = 82): eGFR < 30 mL/min.
Automated chemiluminescence immunoassay systems were used for the determination of TSH, T4, free thyroxine (fT4), T3, and free triiodothyronine (fT3; ADVIA Centaur, Bayer Vital, Fernwald, Germany): TSH (0.3–4.0 mIU/L, T4 (58–140 nmol/L, fT4 (11.5–22.5 pmol/L), T3 (0.9–2.8 nmol/L), fT3 (3.5–6.5 pmol/L), and thyroxine-binding globulin (TBG; 10–35 mg/L). rT3 (reference 0.14–0.54 nmol/L) was measured by a radioimmunoassay (Fa. Adaltis, Freiburg, Germany).
SePP concentrations were determined using an immunoluminometric sandwich assay as described (16). Except for the SePP ILMA, which was performed at the Institute of Experimental Endocrinology, Charité, Berlin, all laboratory investigations were performed in the Division of Laboratory Research at the University Hospital Essen. All analyses were performed in a blinded way with respect to patient characteristics.
To compare CKD and CHD patients, independent samples t-tests and univariate analysis of covariance (ANCOVA; controlling for age) were used. TH concentrations in CKD patients with different disease stages were compared with univariate analysis of variance (ANOVA), followed by Bonferroni tests controlling for multiple testing. To analyze associations between SePP concentrations, THs, and renal function within CKD patients, linear regression models were conducted, additionally controlling for age and CRP where appropriate. Additionally, partial correlation analyses were completed to control for age and CRP. Results are given as mean ± standard deviation (SD) unless stated otherwise. The alpha level for significance was set at 0.05.
The study was approved by the local ethical committee. All patients gave informed consent.
Results
Patient characteristics
The biochemical features of the CKD and CHD patients are summarized in Table 1. Reported differences between CKD and CHD patients remained significant after controlling for age.
Differences between CKD and CHD patients remained significant after correcting for age.
25th–75th percentile of healthy individuals (13).
CKD, chronic kidney disease; CHD, chronic hemodialysis; CRP, C-reactive protein; SePP, selenoprotein P; TSH, thyrotropin; n.s., not significant; T4, thyroxine; fT4, free thyroxine; T3, triiodothyronine; fT3, free triiodothyronine; rT3, reverse triiodothyronine; TBG, thyroxine-binding globulin.
Serum SePP and TH status
In patients with CKD, SePP concentrations increased with impaired renal function (GFR; standardized β = −0.17, p = 0.029; Fig. 1), and this association remained significant after controlling for age and CRP concentrations (standardized β = −0.19, p = 0.031). In contrast, SePP concentrations were significantly lower in the CHD compared with the CKD group (p < 0.001; Fig. 2).

Renal function (glomerular filtration rate [GFR]) and selenoprotein P (SePP) status in chronic kidney disease (CKD) patients.
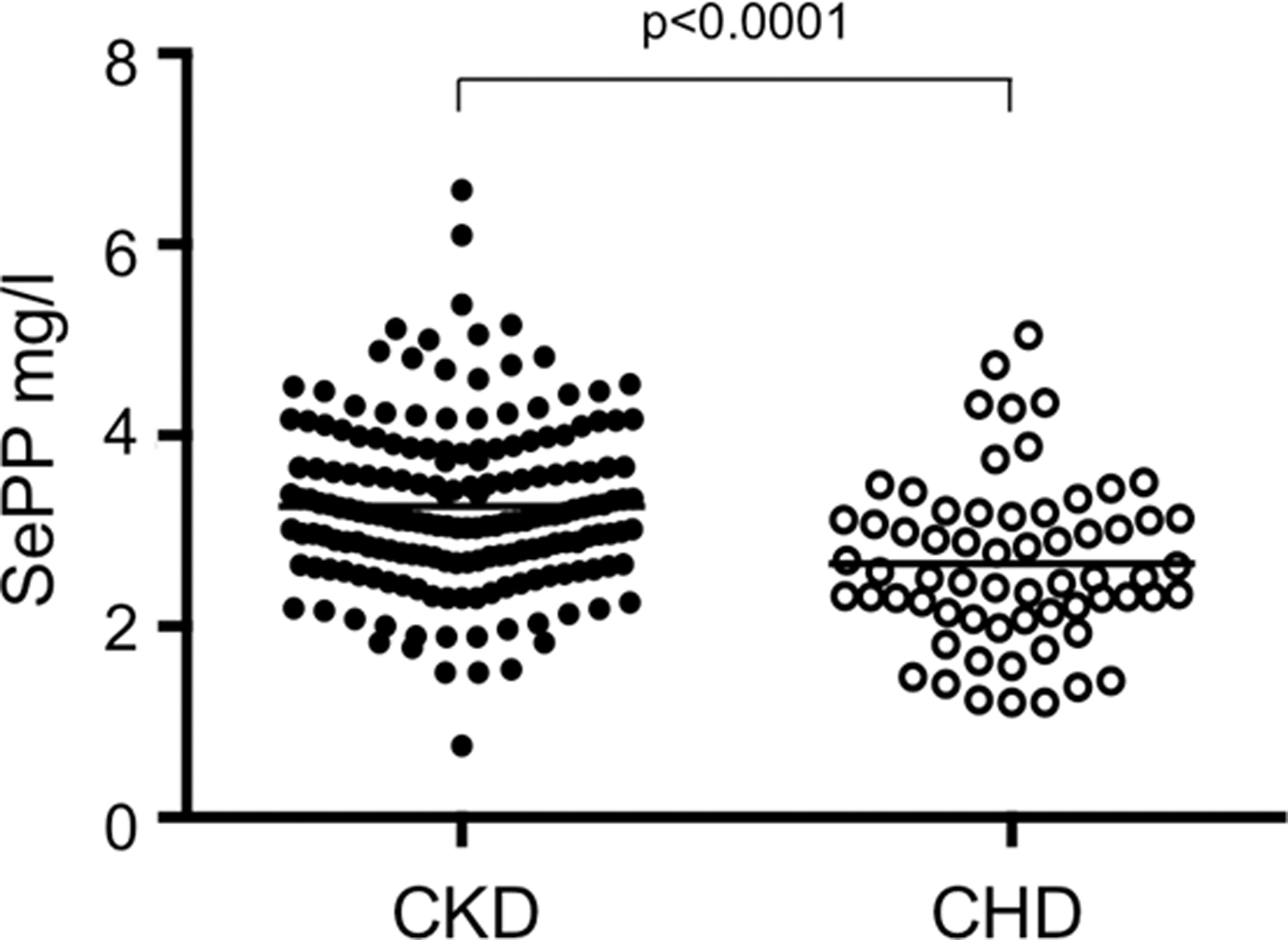
SePP concentrations (median) in CKD and chronic hemodialysis (CHD) patients.
As expected, T4, fT4, T3, and fT3 were negatively associated with renal function, while rT3 and TSH were not (Table 2). Furthermore CHD patients had significantly lower TH concentrations (T4, fT4, T3, fT3) compared with CKD patients. TSH and TBG concentrations were similar in the two patient groups (Table 1).
All associations between GFR, SePP, and thyroid parameters remained significant after controlling for CRP (with exception of the association between SePP and T4, see text for details). β = standardized β, p = p-value.
TH, thyroid hormone; GFR, glomerular filtration rate.
In patients with CKD, lower SePP concentrations were significantly associated with higher T4 (standardized β = −0.16, p = 0.039; Fig. 3A). However, after statistically controlling for CRP, this association remains only as a statistical trend (standardized β = 0.14, p = 0.079). Further, lower SePP concentrations showed an association with higher fT4 (standardized β = −0.16, p = 0.039; Fig. 3B), which remained significant after controlling for CRP (fT4: standardized β = −0.17, p = 0.034). No significant association was observed between SePP and TSH, T3, fT3, rT3, T3/T4, rT3/T3, rT3/T4, or TBG concentrations (Table 2). SePP concentrations were negatively associated with CRP levels (standardized β = −0.17, p = 0.029). In the group of CHD patients, SePP was not significantly associated with any of the investigated classical TH parameters. Among all patients, T3 showed a significant decrease from stage 1 to 5 (F = 16.86, p < 0.001 for post-hoc test; Fig. 4). rT3/T3 and rT3/T4 ratios were calculated and showed a significant increase from stage 1 to 3b and 4 (rT3/T3: F = 4.10; p = 0.003; rT3/T4: F = 4.85, p = 0.001) and remained unaffected in CHD patients due to stable rT3 concentrations accompanying slightly decreasing T3 and T4 concentrations (Fig. 5).
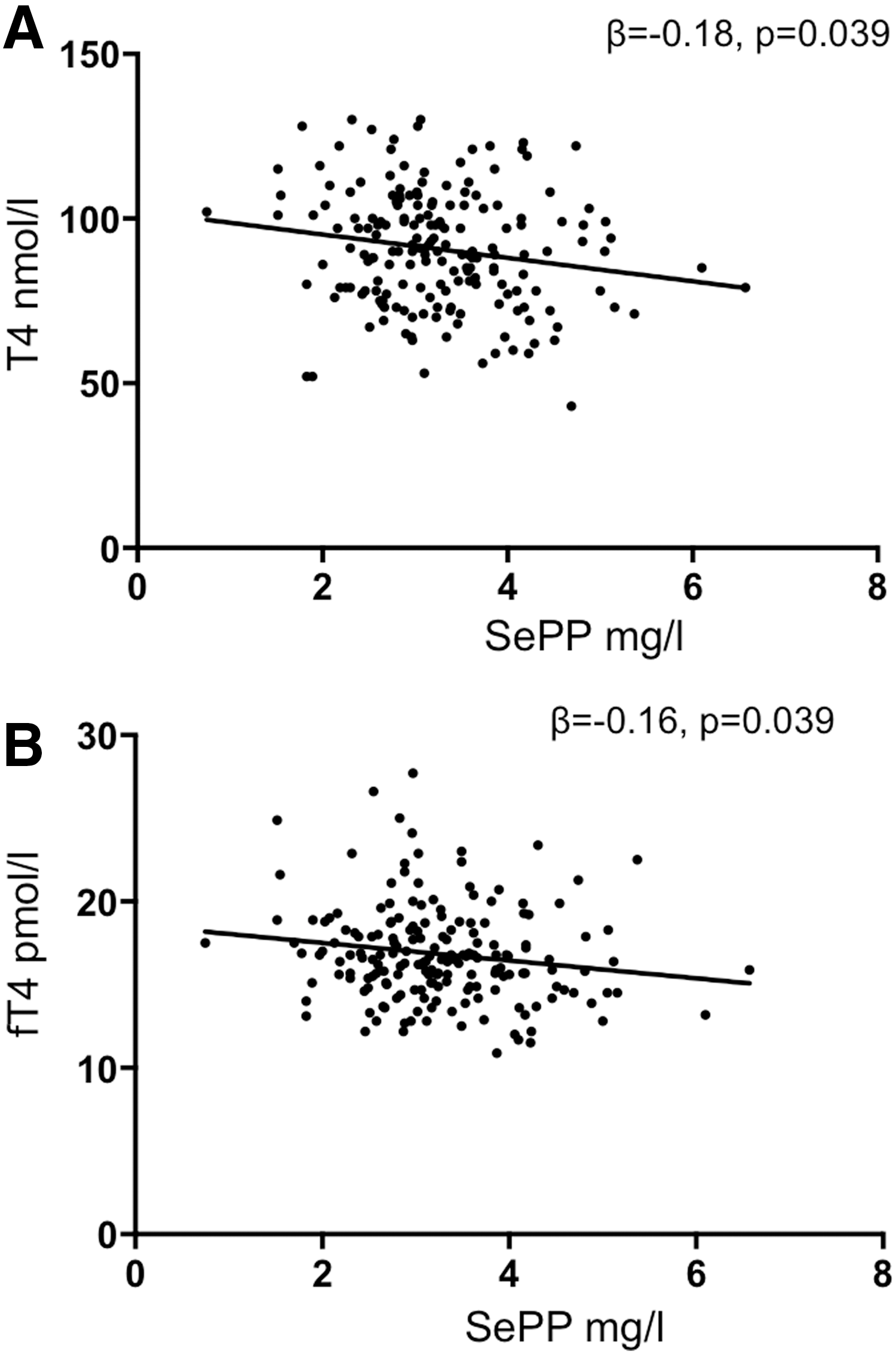
Thyroxine (T4) and free thyroxine concentrations and SePP status in CKD patients.

Reverse triiodothyronine (rT3) and T3 concentrations in distinct CKD stages and in CHD patients.
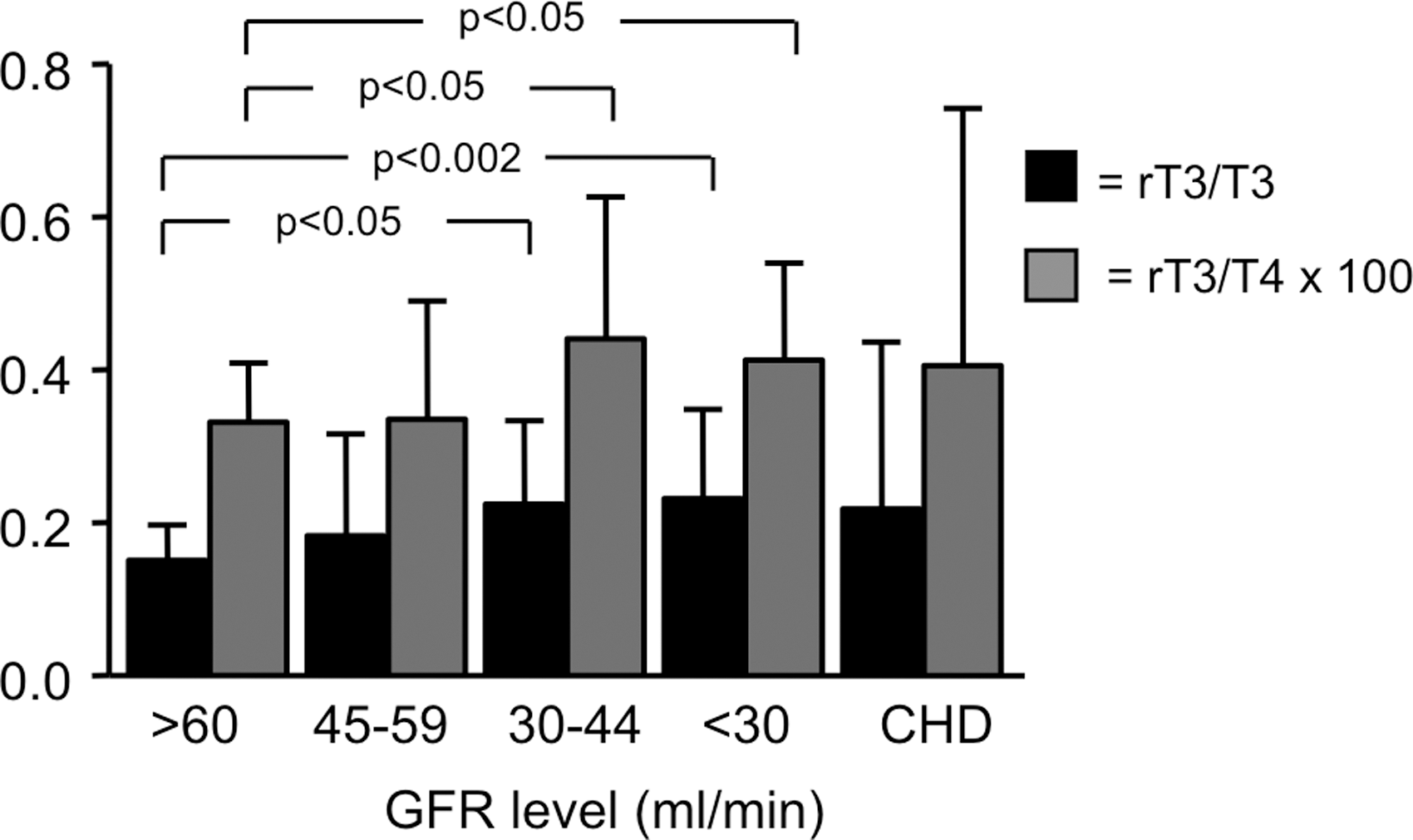
rT3/T3 and rT3/T4 ratios in patients with distinct CKD stages and in CHD patients.
Discussion
Renal and liver function markedly impact peripheral deiodination of TH, which is dependent on an adequate Se status, as reflected by the serum concentration of its biomarker SePP. Thus, this study tested whether impaired renal function in CHD and CKD reveals any relationships between SePP and TH concentrations similar to the status of NTI.
A negative correlation was observed between SePP and fT4 or T4 concentrations in patients with CKD. Similar results were reported by Hoeg et al. (17). In a large cohort of postmenopausal women with normal kidney function, they found a negative correlation between SePP and fT4 and fT3 (17). In the present study, all other investigated TH parameters (TSH, T3, fT3, and rT3) were not associated with SePP levels in CKD patients, indicating that this relation is maintained even in CKD, at least in its milder manifestation.
A constellation of decreasing T4 serum concentrations in the presence of increasing Se concentrations is supported by several studies. Thus, T4 and fT4 decreased after Se supplementation, which may in part be explained by increased TH turnover that is not always reflected by elevated DIO-mediated T3-production and/or a less active thyroid gland under conditions of adequate selenium levels (18 –20). However, in the majority of studies reporting on either baseline associations or alterations of TH status subsequent to nutritional interventions with various Se compounds, no significant interactions or only a mild sex-specific decrease of T4 and/or an increase of T3 were reported (21 –27). These observations suggest that there is no immediate clinical benefit from supplementation with selenium compounds with respect to improved function of the TH axis in the absence of any signs of autoimmune thyroid disease, severe selenium deficiency, or any other disease resulting in inadequate selenium status.
SePP values were in the same range as reported before in other studies (3,17). In CKD patients, there was a negative association of SePP with renal function in patients not requiring hemodialysis. This could be due to impaired Se and/or SePP clearance with declining renal function, as SePP has been shown to be specifically bound by megalin in the healthy kidney of rodent models, likely preventing its loss or degradation (4,5). A significant negative correlation of SePP and CRP has also been reported, presumably due to altered hepatic SePP biosynthesis, as previously seen in cell culture studies and mouse models of acute phase response (28 –30). However, in the present patients, the association of SePP with renal function was still present when corrected for CRP, highlighting the complexity of the interaction.
The situation with the patients on CHD is different. Here, SePP concentrations were significantly lower in the dialysis group. Low serum Se concentrations in dialysis patients were previously reported in several studies (6,8,31,32); this observation might be explained by a lower Se (via lower protein) intake and/or impaired intestinal absorption in sick dialysis patients and less likely by a loss of Se through the dialysis membrane (33). However, at present, it cannot be excluded that the dialysis membrane has specifically removed some of the circulating SePP, as this possibility has been suggested in patients undergoing low-density lipoprotein apheresis (34). Whether an altered concentration of GPx3, a selenoprotein produced and secreted by renal tubules, contributes to the differences observed between CKD and CHD patients remains open. GPx3 accounts for < 20% of the serum or plasma selenium concentration in healthy individuals, and its synthesis and secretion might be decreased in CHD patients (35).
More recently, in a study from Japan, low Se concentrations were associated with a high mortality rate, especially due to infectious disease–related deaths in young hemodialysis patients (10). Moreover, low T3 concentrations as well as elevated TSH concentrations were also associated with a high mortality rate (2,36). In contrast to Liu et al., who found a positive correlation of serum Se and T3 and fT3 in their CHD patients, a correlation was not observed between SePP and TH parameters in the present dialysis group (32).
This study confirms previous results on a negative association of TH status, that is, decreasing T4, fT4, T3, and fT3 concentrations with declining renal function (37,38). Thus, all TH parameters except for TSH and TBG were lower in CHD patients.
A continuous increase in rT3 with declining renal function was not found, but rather a peak of rT3 concentrations (but still within the reference range) in patients with stage 3 CKD, and then a further decrease of rT3 with more advanced CKD stages approaching rT3 concentrations similar to those found in CHD patients. Moreover, rT3/T3 and rT3/T4 ratios showed a gradual increase up to CKD stages 3 and 4 as in other forms of NTI, but no further increase in patients on CHD. Again, these alterations were not accompanied by changes in the SePP status. In a previous study, a significant decrease of rT3 concentrations in patients with CKD stages 4–5 compared with CHD patients was also reported (38). Such a constellation has been explained by a normal production rate concomitant with an increased clearance rate of rT3 (39). Here, one can speculate that in addition to altered deiodination, additional mechanisms such as decarboxylation, acetylation, and/or oxidative deamination or T4 degradation might occur (40).
This study cannot provide mechanistic information on the possible interactions between kidney and liver function, hepatic production and renal delivery of SePP, common or independent factors such as proinflammatory cytokines, uremia toxins, hypoxia, or oxidative stress. These factors might independently or simultaneously interfere with hepatic SePP production and/or renal, hepatic or peripheral TH metabolism, as suggested by the associations between serum concentrations of SePP and TH in CHD and CKD observed in this study.
In conclusion, to the authors' knowledge, this is the first study evaluating SePP status and TH metabolism in a large group of patients in various CKD stages. SePP concentrations were found within the reference range in the presence of decreasing T4 and fT4 concentrations. TH degradation to rT3 seems to be unaffected by SePP status in patients with CKD. Significantly lower SePP values were observed in patients undergoing CHD, but this is not associated with serum TH parameters.
Footnotes
Author Disclosure Statement
No competing financial interests exist.