
Abstract
Background:
Small papillary thyroid carcinomas have contributed to the worldwide increased incidence of differentiated thyroid cancer observed over the past decades. However, the mortality rate has not changed over the same period of time, raising questions about the possibility that thyroid cancer patients, especially those with small tumors, are overdiagnosed and overtreated. Molecular prognostic marker able to discriminate aggressive thyroid cancers from those with an indolent course would be of great relevance to tailor the therapeutic approach and reduce overtreatment. Mutations in the TERT promoter were recently reported to correlate strongly with aggressiveness in advanced forms of thyroid cancer, holding promise for a possible clinical application. The occurrence and potential clinical relevance of TERT mutations in papillary thyroid microcarcinomas (mPTCs) is currently unknown. This study aimed to analyze the occurrence of two TERT promoter mutations (-124C>T and -146C>T) and their potential association with unfavorable clinical features in a large cohort of mPTCs.
Methods:
A total of 431 mPTCs cases were collected from six Italian institutions, and TERT promoter mutational status was assessed by a next-generation sequencing approach.
Results:
TERT promoter mutations were found in 4.7% of the analyzed mPTCs, showing that even microcarcinomas carry mutations in this gene. Correlation analysis showed that TERT promoter mutations are not associated with aggressive features or clinical outcome in the cohort analyzed.
Conclusions:
TERT mutations are present but uncommon in mPTCs. Apparently, in mPTCs, the occurrence of TERT mutations is not correlated with unfavorable clinical features.
Introduction
T
Recently, a high frequency of mutations in the promoter of the Telomerase Reverse Transcriptase (TERT) gene has been detected in a variety of solid tumors (9 –12). In particular, the majority of alterations were mapped in two hot spots at positions -124 bp (chr5:1,295,228 G>A, hereafter termed -124C>T) and -146 bp (chr5:1,295,250 G>A, hereafter termed -146C>T) upstream of the transcription starting site (12). These alterations were found to increase promoter activity and TERT expression, most likely introducing new consensus sites for transcription factors belonging to the ETS family (9,13,14). In thyroid cancer, mutations in the TERT promoter have been strongly associated with aggressiveness and metastatic behavior of the tumors (15 –19). In well-differentiated thyroid cancer, TERT promoter mutations were reported to occur in <10% of the lesions, while the incidence of these mutations increase in thyroid cancers of follicular origin with distant metastases (>30%) (15,20) and in poorly differentiated lesions (up to 50%) (17 –19). These observations suggest that TERT promoter mutations could be a marker to discriminate a subset of aggressive tumors from the majority of those that are relatively indolent. As of yet, the occurrence and clinical relevance of TERT promoter mutations in mPTCs is unknown.
The aim of this work, therefore, was to assess the occurrence and the frequency of TERT promoter mutations in a large cohort of mPTCs and to establish whether the presence of these mutations may hold promise as a useful prognostic biomarker in this subtype of thyroid cancer.
Material and Methods
Patients
For this study, 431 cases of well-differentiated PTC measuring≤1 cm (mPTC) were retrieved from the archives of six different Italian centers (Table 1). Tumor slides were classified according to the criteria of the World Health Organization Classification of Tumors (21) and staged according to AJCC Cancer Staging Manual, 7th edition (22). The histological variant was evaluated for each mPTC case. Tissues from 12 lymph node metastases (LNMs) developed from mPTC were also retrieved and analyzed.
RE, Arcispedale S. Maria Nuova, Reggio Emilia, Italy; BO, Bellaria-Maggiore Hospitals, Bologna, Italy; SGR, “Casa Sollievo della Sofferenza” Hospital—IRCCS in San Giovanni Rotondo, Italy; RM, University Hospital, Università “Sapienza,” Rome, Italy; CZ, City Hospital of Catanzaro, University of Catanzaro, Italy; MT, Tinchi-Pisticci Hospital of Matera, Italy.
mPTC, papillary thyroid microcarcinomas.
The 431 mPTCs were from 405 patients, since multiple mPTC lesions were retrieved for 20 patients (2–4 lesions/patient). Follow-up was available for 306 of the 405 patients, and ranged from 6 to 170 months (mean 58±27 months). Clinical and pathological features of all the cases are summarized in Supplementary Table S1 (Supplementary Data are available online at
Sequencing
Next-generation sequencing analysis of the TERT promoter hot spot harboring the mutations -124C>T and -146C>T was performed on formalin-fixed and paraffin-embedded (FFPE)-extracted DNA using the 454 GS-Junior Next Generation sequencer (Roche Diagnostics, Mannheim, Germany), according to established protocols (
BRAF V600E mutation analysis was performed with the same DNA extracted for the TERT promoter analysis, by direct sequencing as previously described (23), or by allele-specific locked nucleic acid polymerase chain reaction, as previously described (24).
Statistical analysis and bioinformatics analysis
Statistical analyses were performed with R package (R Foundation for Statistical Computing, Vienna, Austria;
Results
TERT promoter mutations in mPTCs
The mutational status of a hot spot region within the TERT promoter was successfully analyzed in 404 primary mPTCs. Table 1 summarizes the results of this mutation analysis. The TERT promoter mutations -124C>T and -146C>T were found in 19 out of 404 mPTCs, corresponding to 4.7% of the overall cohort. The -124C>T was the most frequent mutation, occurring in 11 of the 19 TERT mutated samples, while the -146C>T was found in eight mPTCs (Table 1). The average mutated allele percentage in the 19 TERT mutated tumors was 7.2±5.7% (range 2–17%), suggesting that only a subgroup of tumor cells harbored the mutations.
Tweleve lymph node metastases (LNMs) were also analyzed for the presence of the TERT promoter mutations. Two LNMs derived from patients with TERT mutations in the primary mPTC, seven derived from six individuals with absent TERT mutations (two LNMs were from the same wild type mPTC), and three LNMs originated from subjects whose primary tumors were not available for molecular analysis. Overall, 4 of the 12 LNMs (25%) harbored TERT promoter mutations. Of these, two developed from the same mutated primary mPTCs, one was acquired de novo in the metastatic lesion, while in one case the primary mPTC was not available for genotyping (Fig. 1). The average percentage of mutated TERT alleles in the LNMs was 18.8±19.1%, (range 4–46.5%) with an increased percentage of the mutated allele in the metastatic site compared to the primary lesion (Fig. 1).
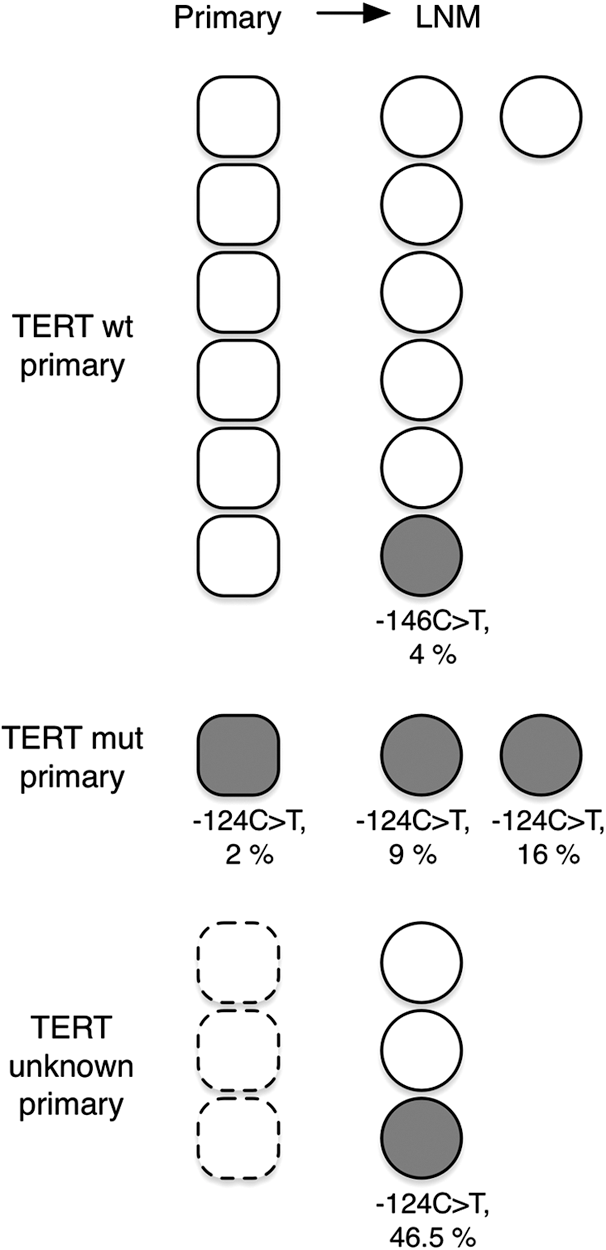
TERT promoter mutation status in matched primary papillary thyroid microcarcinomas (mPTC; squares) and lymph node metastases (LNMs; circles). Gray shape are TERT mutated (type of mutation is indicated, with corresponding mutated allele percentage), white shapes are wild type.
Besides the -124C>T and -146C>T mutations, three additional mutations were detected in the primary mPTCs and LNMs, with frequencies comparable to the canonical -124C>T and -146C>T (Table 2).
Mutations -126C>T and -138C>T are reported in COSMIC database with ID: COSM1717363 and COSM1717364, respectively. Their somatic status has not been confirmed. The variation -161C>T is not reported in the databases.
LNM, lymph node metastasis.
TERT promoter mutations and clinical features of mPTCs
Interestingly, it was found that even mPTCs without aggressive behavior carried mutations in the TERT promoter. Next, the possible association of the TERT promoter mutations -124C>T and -146C>T with clinicopathological features of the included mPTCs (Table 3) was examined. The presence of a TERT promoter mutation was not associated with any of the parameters taken into consideration, likely due to the low frequency of the mutations in the overall cohort. It is known that the majority of persistent/recurrent structural disease (about 77%) in mPTCs occurs within five years after the initial treatment of the patient (25). The average follow-up length in our cohort was of 59 months, without significant differences between the patients with and without TERT mutations (63.6±22.3 vs. 57.5±27.3, n.s.). Within this follow-up period, no significant association between the presence of these mutations and a negative outcome was detected (Table 3). However, since mPTCs are slowly growing tumors, potential effects of TERT promoter mutations on the progression of these lesions over a longer period of follow-up cannot be excluded.
Data are reported as mean±SD or frequencies. In some cases, the clinicopathological features and the outcome status were not available for every TERT-genotyped mPTC.
All the cases were clinically evaluated and the lymph nodes were negative at ultrasound examination.
For 20 patients, multiple mPTC lesions were TERT-genotyped (2–4 lesions/patient). For the analysis of association of TERT promoter status with patient features and outcome status, only one genotype status was utilized for each patient. In 17 patients, the genotype was concordant (wt) in multiple lesions, in one case the genotype was discordant between three lesions of a single patient (one -124C>T-mutated, two wt) and the patient was considered as TERT-mutated the analysis.
Recently, a positive correlation between TERT promoter mutations and the BRAF V600E mutation was reported in advanced PTCs, suggesting a functional cooperation (18,20). The BRAF V600E mutation was successfully analyzed in 428 of the 431 mPTC samples, and it was detected in 261 mPTCs, corresponding to 61% of the overall cohort. No statistical correlation was observed between the presence of TERT promoter mutations and the occurrence of the BRAF V600E mutation (Table 3, p=0.63) in mPTCs. As previously reported (26,27), the BRAF V600E mutation alone was also associated with tumor size, tall-cell histological variant, and higher stage in this study. However, the presence of this mutation did not correlate with the clinical outcomes (Supplementary Table S2). When considered together, the co-occurrence of a TERT promoter and the BRAF V600E mutation was significantly associated with higher pT and pN, due to the statistical effect of the BRAF V600E mutation. Intriguingly, the presence of both mutations was inversely associated with multifocality (Table 4). Finally, the co-existence of TERT promoter mutations and BRAF V600E mutation did not affect the clinical outcome in the follow-up analysis (Table 4).
Comparisons were performed as described in Table 1, between the no mutation group and each of the other three groups (only TERT mutation; only BRAF mutation; TERT+BRAF mutation).
p-Values refer to the comparison of the no mutation group with the group in the column at the left of the p-value.
Significant values are shown in bold.
BRAF V600E was not evaluable in two TERT-genotyped mPTC.
All the cases were clinically evaluated and the lymph nodes were negative at ultrasound examination.
Discussion
Small thyroid cancers are usually indolent lesions with a low rate of growth and low metastatic potential. Nonetheless, a significant percentage of mPTCs (up to 25%) behave aggressively, developing local recurrences, LNMs, and, rarely, distant metastases (7,28). The identification of prognostic markers able to discriminate aggressive mPTCs from those with an indolent course would be of great relevance to tailor the therapeutic approach, avoiding overtreatment, and long-term surveillance. This study analyzed the occurrence of TERT promoter mutations in a large cohort of mPTCs. It was demonstrated that a subset of mPTCs (4.7% of the cohort) harbored mutations in the TERT promoter. This frequency is lower than that reported in the literature for PTCs>1 cm (7–9%) and significantly lower than that reported for highly aggressive thyroid carcinomas (up to 51%), suggesting that the incidence of these mutations increases as the tumor progresses toward more advanced stages. To the authors' knowledge, this is one of the first reports in which the presence of TERT promoter mutations in thyroid cancer has been assessed using a quantitative approach. While the percentage of TERT mutated allele was found to be quite low in primary mPTCs, it increases significantly in the LNMs (up to 46.5%). This observation suggests a clonal expansion of cells harboring TERT promoter mutations during tumor progression. The overall low prevalence of TERT mutations in small PTCs compared with larger tumors, together with the low percentage of mutated alleles observed in primary mPTCs and its increase in LNMs, suggest that TERT promoter mutations are late events in thyroid tumorigenesis and that they confer a functional advance toward aggressiveness and progression.
The present study focused on the two most commonly analyzed TERT promoter mutations, namely -124C>T and -146C>T, for which a functional effect on TERT expression has been experimentally confirmed (9,13,14). However, within the analyzed hot spot region, three additional mutations were detected with frequencies and allele percentages comparable with these previously reported mutations. If a pathogenic role of these mutations is confirmed, the association between TERT mutational status and the clinical features of mPTCs should be reconsidered by integrating these new mutations.
In conclusion, this study analyzed for the first time TERT promoter mutations in a large series of mPTCs. It was observed that TERT promoter mutations do not predict unfavorable features in mPTCs either alone or in combination with the BRAF V600E mutation, at least within the period of follow-up considered in this work. This may be partially due to the low frequency of TERT mutations in this category of thyroid cancer. It is also needs to be considered that even though quite a large number of mPTCs were analyzed, none of them developed distant metastases or an ominous outcome. The authors have recently shown that TERT promoter mutations are strongly associated with the presence of distant metastasis but not with the presence of LNMs in well-differentiated PTCs (15). Thus, the present data seem to support the concept that TERT promoter mutations are strongly linked with advanced metastatic spreading, which is an extremely rare feature in small thyroid carcinomas.
Footnotes
Acknowledgments
This work was supported by a grant from the Italian Ministry of Health (GR-2011-02350937) and MIUR (20093XZC57_003). GG is supported by a Fondazione Umberto Veronesi Fellowship.
Author Disclosure Statement
The authors declare that no conflict of interest exists over this research.