
Abstract

American Thyroid Association guidelines recommend against routine use of postoperative radioactive iodine (RAI) for low-risk thyroid cancers such as papillary thyroid carcinomas (PTC) ≤1 cm (1). Inappropriate use of RAI places patients at unnecessary risk of permanent treatment-related toxicity and secondary cancers.
We have previously shown that county-level access to healthcare affects the likelihood that a small thyroid cancer will be diagnosed (2). We hypothesized that these same factors would be associated with the likelihood of receiving inappropriate RAI treatment for low-risk PTC.
Using the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) database, we performed an ecologic analysis across 337 U.S. counties, encompassing 13,401 patients undergoing thyroidectomy from 1983 to 2009 for low-risk (≤1 cm intrathyroidal N0 M0) PTC. We modeled county-level access to healthcare with eight socioeconomic factors known to be indicative of access to care, in population-weighted least squares regression: mean family income and percentage of residents uninsured, unemployed, in poverty, white-collar employed, non-English speaking, only high-school educated, and college educated (2,3).
All socioeconomic indices of lower healthcare access correlated with a higher likelihood of RAI treatment, with healthcare access explaining a significant proportion of county-level variation (r=0.41, r 2=0.17, p<0.001; Fig. 1). There was wide variation in RAI treatment for low-risk PTC across counties (range 0–100%). In 42 counties with ≥50 cases, the range was 9.6–56.1%. In counties in the highest decile of access to care, RAI was used in 30% of patients; in counties in the lowest decile, 42% (p=0.04). Between 1983 and 2009, the proportion of U.S. patients receiving RAI for low-risk PTCs increased from 8% to 31% (p<0.001).
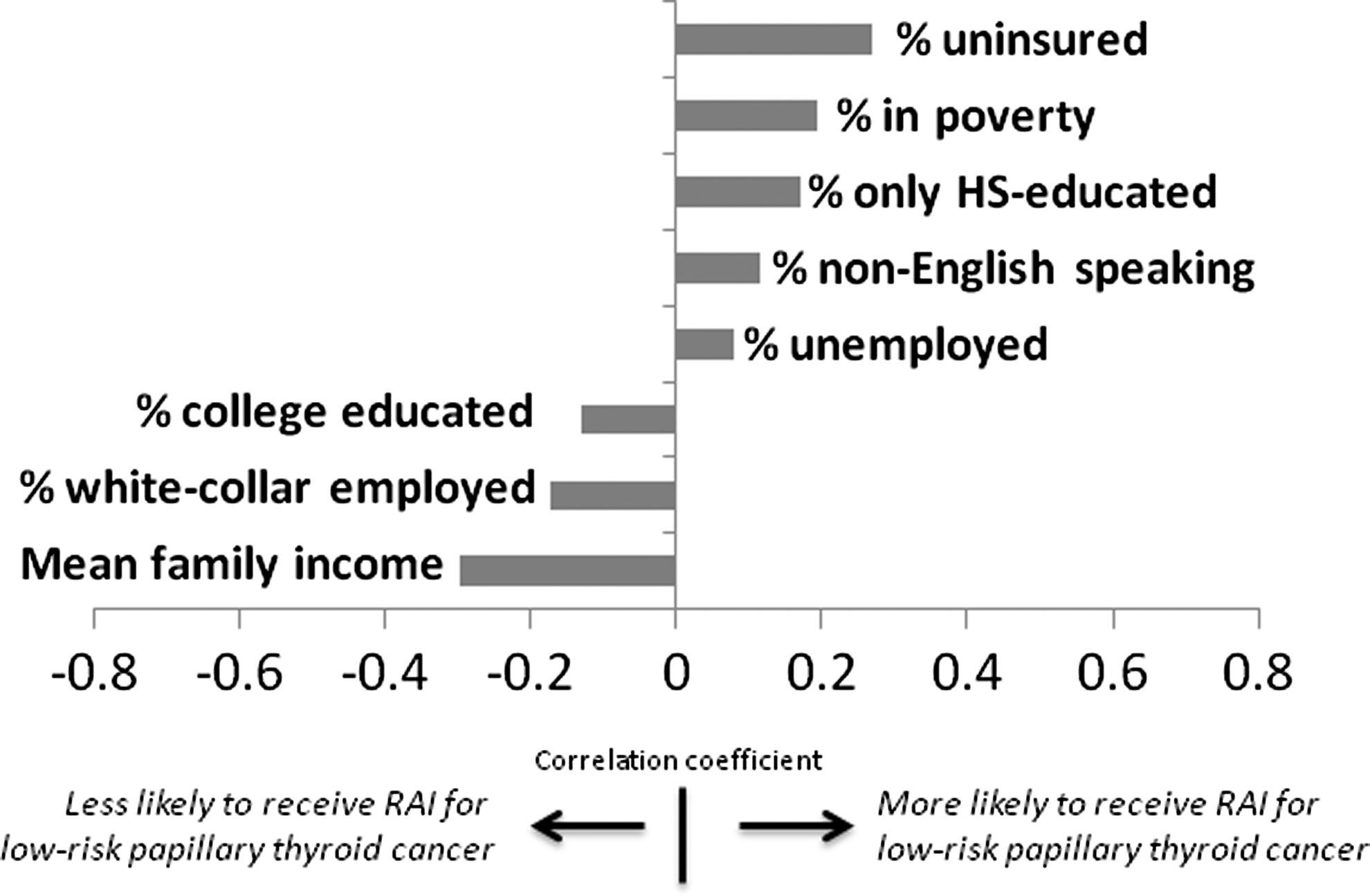
Correlation of county-level socioeconomic markers of access to healthcare with the use of RAI for very low-risk papillary thyroid carcinoma. HS, high school; RAI, radioactive iodine.
These data demonstrate a significant association between poorer access to healthcare and inappropriate use of adjuvant RAI for low-risk PTC. We caution that ecologic analyses such as this cannot prove causation but are a useful tool for showing problems with quality of care. Variation in clinical practice, such as observed here, generally suggests that quality of care may be suboptimal, as it implies that some patients are undertreated, or overtreated, or both. Such variation may represent clinical uncertainty in the field, but can also represent physician or patient preferences.
Haymart et al. reported that the likelihood of a young patient receiving RAI for a stage I PTC ranged from 0% to 90% across 397 U.S. hospitals. The majority of the variation in RAI use could not be explained by patient, tumor, or hospital factors, and was attributable only to “unexplained hospital characteristics” (4). In subsequent work, Haymart et al. have shown that RAI use is associated with the specialty of the primary decision maker (nuclear medicine physicians were more likely than endocrinologists, and surgeons less likely, to administer RAI), and with practice setting (nonacademic physicians were more likely than academic physicians to administer RAI) (5,6).
Here, we found that inappropriate treatment with RAI was most common in areas of the United States with less access to healthcare. There are a number of potential explanations for these findings. These may reflect differences in the intensity of care physicians are accustomed to delivering in populations with less access to care and poorer overall health. However, we did restrict analysis to cancers in which RAI is not recommended. Alternatively, these findings may reflect differences in access to experienced specialists, market forces, or other unmeasured factors. These data provide an opportunity to reinforce guidelines recommending against aggressive therapy of low risk PTCs, which remains common.
Footnotes
Acknowledgment
Delivered as an oral presentation at the 2013 annual meeting of the American Thyroid Association.