
Abstract
Background:
It is of critical clinical importance to select accurately for surgery thyroid nodules at risk for malignancy and avoid surgery on those that are benign. Using alterations in subcellular localization for seven putative biomarker proteins (identified by proteomics), this study aimed to define a specific combination of proteins in surgical tissues that could distinguish benign from malignant nodules to assist in future surgical selection by fine-needle aspiration biopsy (FNAB).
Methods:
Immunohistochemical subcellular localization (IHC) analyses of seven proteins were retrospectively performed on surgical tissues (115 benign nodules and 114 papillary-based thyroid carcinomas [TC]), and a risk model biomarker panel was developed and validated. The biomarker panel efficacy was verified in 50 FNAB formalin-fixed and paraffin-embedded cell blocks, and 26 cytosmears were prepared from fresh surgically resected thyroid nodules.
Results:
Selection modeling using these proteins resulted in nuclear phosphoglycerate kinase 1 (PGK1) loss and nuclear Galectin-3 overexpression as the best combination for distinguishing TC from benign nodules (area under the curve [AUC] 0.96 and 0.95 in test and validation sets, respectively). A computed malignancy score also accurately identified TC in benign and indeterminate nodules (test and validation sets: AUC 0.94, 0.90; specificity 98%, 99%). Its efficacy was confirmed in surgical FNAB cell blocks and cytosmears.
Conclusion:
Using surgical tissues, it was observed that a combination of PGK1 and Galectin-3 had high efficiency for distinguishing benign from malignant thyroid nodules and could improve surgical selection for TC among indeterminate nodules. Further validation in prospective preoperative FNAB will be required to confirm such a clinical application.
Introduction
T
Clinically detectable thyroid nodules occur in up to 10% of the population. Ultrasound-guided fine-needle aspiration biopsy (FNAB) is currently the most specific diagnostic technique available for the initial assessment of thyroid nodules (4). With a thyroid FNAB diagnosis of malignancy or suspicious for malignancy, clinicians will often recommend thyroidectomy (5). However, 15–30% of thyroid FNAB cytologic findings are indeterminate, and on surgical resection the surgical histopathologic diagnosis will be benign in approximately 75–85% of cases. If an indeterminate FNAB result could be better classified as benign or malignant, then surgery for definitive diagnosis might be avoided in a proportion of cases (6). Accurate distinction between benign and malignant thyroid nodules therefore has critical therapeutic implications. One of the most challenging areas of thyroid pathology includes follicular patterned nodules where the differential diagnosis ranges from benign entities such as adenomatous hyperplastic nodule and follicular adenoma to malignant tumors, most commonly the follicular variant of papillary carcinoma and less commonly, follicular carcinoma (7).
To address this issue, protein biomarker analyses by immunohistochemical subcellular localization (IHC) have been explored as an adjunct to FNAB cytology to facilitate the presurgical diagnosis of TC. Currently, two molecular tests based on patient tumor genotyping have become available as presurgical diagnostic aids (8 –24). The gene mutational panel test is based on genetic alterations associated with TC identified in PI3K-AKT and MAPK pathways that include rat sarcoma viral oncogene (RAS) point mutations (25), virus-induced rapidly accelerated fibrosarcoma murine sarcoma viral oncogene homolog B (BRAF V600E ) mutations (26), rearranged during transfection proto-oncogene/papillary thyroid carcinoma (RET-PTC) (27), and paired box gene 8/peroxisome proliferator-activated receptor gamma (PAX8/PPAR/) rearrangements (28,29). Recently, these mutations have been tested in FNAB to define a clinical algorithm for guiding the appropriate extent of initial thyroidectomy (23). The second test is a gene expression classifier (GEC), which is based on the expression profile of 142 gene mRNA transcripts (16), and has been independently assessed (18). Although these new genomic diagnostic tests have been proposed to improve the management of indeterminate nodules, several important issues remain to be resolved, including their cost and accuracy, before being recommended for widespread clinical use.
In comparison to these genomic tests, protein-based IHC analysis could offer an alternative approach that would be more efficacious for routine clinical use. Differential protein expression based on a panel of biomarkers, using IHC with FNAB, offers an excellent opportunity to develop an alternative strategy for presurgical evaluation of indeterminate thyroid nodules. Such a proteomic approach could provide a panel of biomarkers that would allow physicians to develop a personalized treatment plan for each patient. Hence, this diagnostic test could save not only patients from the burden of unnecessary surgery but also avoid excessive healthcare costs.
Recently, the authors' group analyzed the secretomes of three TC cell lines using proteomics and reported preliminary data based on a small patient cohort (6 benign tissues and 12 TC patients) to demonstrate that some of these identified proteins could be detected in patients' sera and tissues (30). Furthermore, differential subcellular expression of a subset of proteins was observed in benign and malignant thyroid nodules (30). In the current study, a panel of seven proteins (phosphoglycerate kinase 1 [PGK1], pyruvate kinase isozyme M2 [PKM2], Cyclin D1, Galectin-3, phosphatase and tensin homolog [PTEN], S100A6, and Profilin-1] was selected to determine their potential to distinguish TC from benign (non-neoplastic and neoplastic thyroid nodules) as well as indeterminate thyroid nodules (atypia, suspicious, and follicular lesion of undetermined significance [FLUS]). To this end, IHC patterns were determined using archived formalin-fixed paraffin-embedded (FFPE) tissue blocks of thyroid tissues, as well as FFPE cell blocks and cytosmears prepared from FNABs taken from the fresh surgical samples after removal of the thyroid nodules. From these studies, the study aimed to identify retrospectively the best combination of biomarkers that would accurately distinguish benign from malignant nodules and be applied in the future to presurgical management using FNAB.
Materials and Methods
Patient specimens
The study was approved by the Mount Sinai Hospital (MSH) Research Ethics Board (REB), Toronto, Canada. Informed consent for the scientific use of anonymous patient data and tumor tissues had been obtained from all patients as per REB guidelines. All data were analyzed anonymously. Archived FFPE tissue blocks from the MSH tumor bank were retrieved and reviewed by two blinded pathologists (C.M. and J.A.). The clinicopathologic parameters were obtained from surgical pathology reports and the clinical database (J.A. and R.S.) and are summarized in Table 1. Diagnoses at the time of surgery were used to stratify patients. A total of 115 nonmalignant thyroid tissues (53 benign non-neoplastic thyroid nodules and 62 follicular adenomas) and 114 TC tissues were analyzed for protein expression. The frequency of follicular carcinomas seen in the authors' hospital is low. Hence, these could not be included in this analysis. However, the study included 33 follicular and 9 oncocytic (Hürthle cell) variants of PTC. These cases often pose a challenge in FNAB diagnosis, and IHC markers are needed to improve their diagnosis. Anaplastic carcinomas are rarely indeterminate on aspiration. Nevertheless, these constitute the aggressive cancers, and it is important to know the status of our biomarkers in these cases. Hence, these were included in this study.
PTC, papillary thyroid carcinoma.
Fifty FNABs were collected from surgically resected fresh thyroid tissues using a 22-gauge needle in formalin, and used for preparation of FFPE cell blocks for IHC analysis. FNAB FFPE cell blocks were used to cut 4 μm sections. One section was stained with hematoxylin and eosin, and serial sections were used for IHC. Twenty-six cytosmears were made from the FNAB taken from fresh tissues of thyroidectomy specimens and included the clinical index nodules as well as tissue distant from the nodule. Cells were fixed using Cytology Fixative spray (Leica Biosystems). One slide was stained with hematoxylin and eosin while the others were used for IHC. The presurgical FNAB cytology and surgical pathology obtained in this study cohort was compared to the IHC results for the FNAB FFPE and cytosmears obtained at surgery.
Immunohistochemical analysis in thyroid tissues
FFPE tissues, including the cell blocks sections (4 μ thickness) were deparaffinized in xylene and hydrated with graded alcohol series as described previously (30,31). Surgical cytosmears were incubated in Tris-buffered saline with 0.025% Triton for 5 min. For antigen retrieval for proteins PGK1, PKM2, Cyclin D1, Galectin-3, S100A6, and PTEN, slides were immersed in Tris-EDTA buffer (10 mM Tris base, 1 mM EDTA, 0.05% Tween 20, pH 9.0) and pretreated in a 900 W microwave oven for 20 min (tissues) or 6 min (FNAB samples). Antigen retrieval for Profilin-1 was similarly performed using sodium citrate buffer (10 mM, 0.05% Tween 20, pH 6.0) in place of Tris-EDTA buffer. No antigen retrieval treatment was performed for cytosmears. All further incubations were conducted at room temperature.
The VECTASTAIN rapid protocol was followed for immunostaining. Nonspecific binding was blocked by incubating the slides with 10% horse serum for antimouse secondary antibodies and goat serum for antirabbit secondary antibodies for 20 min. The endogenous biotin in thyroid tissues was blocked using an Endogenous Avidin/Biotin blocking kit (ab64212) as described by the manufacturer. Thereafter, the sections were incubated with the following antihuman antibodies (Abcam) for 1 h: rabbit monoclonal Cyclin D1 (1:100; ab134175), mouse monoclonal S100A6 (1:600; ab55680), mouse monoclonal Profilin-1 (1:1500; ab118984), and mouse monoclonal PTEN (1:200; ab79156). The other antibodies were from Santa Cruz Biotechnology, Inc.: mouse monoclonal PGK1 (1:750 dilution; sc-130335), rabbit polyclonal PKM2 (1:100; sc-135048), and mouse monoclonal Galectin-3 (1:200; sc-32790). Tissues were then treated with 3% H2O2 in Tris-buffered saline for 5 min to block the endogenous peroxidase activity, and were subsequently incubated with biotinylated antimouse or antirabbit secondary antibody for 20 min. The sections were finally incubated with VECTASTAIN Elite ABC Reagent (Vector labs) for 30 min, and diaminobenzidine was used as the chromogen. Negative control tissues were incubated with biotinylated horse antimouse (or goat antirabbit) secondary antibody following the same protocol. The slides were counterstained with hematoxylin and viewed using a light microscope.
Evaluation of immunohistochemistry
The immunostaining scores were based on percentage positivity and staining intensity. Sections were scored as positive if epithelial cells showed immunoreactivity in the cytoplasm and/or nucleus when observed by two evaluators. Percentage positive scores were assigned according to the following scale: 0 (<10%), 1 (10–30%), 2 (31–50%), 3 (51–70%), and 4 (>70%). Staining intensity was scored semi-quantitatively as follows: 0 (none), 1 (mild), 2 (moderate), and 3 (intense). A total score for each cytoplasmic and nuclear staining was then obtained (ranging from 0 to 7) by adding the percentage positivity scores and intensity scores for each section. Three fields for each tissue were scored, and the average of the fields was calculated. The IHC scoring was blinded from the histopathology report and was performed by two evaluators independently and used for subsequent analyses. The interobserver variation between two evaluators was determined.
Statistical analyses
All statistical analyses were carried out using R v3.10. Multiple Imputations by Chained Equations (MICE) was used to impute missing data and generate 30 complete data sets to limit loss of power to <1% (32). Imputations were done using the predictive mean matching method, and were carried out using the MICE R package (33). Univariate and multivariable logistic regression analyses were used to assess the individual and cumulative predictive value of biomarkers for cancer versus benign (non-neoplastic nodules and follicular adenoma), as well as for benign non-neoplastic nodules versus benign follicular adenoma. Similar analyses were done using the receiver operator characteristics (ROC) curve to assess the discriminatory value of biomarkers summarized by the area under the curve (AUC). ROC curve analyses were performed using the pROC package in R (34). A two-step approach was used for model selection under multiple imputed data (35). Backward selection was used to derive the final model. The cumulative predictive value of biomarkers that correlated positively and negatively with cancer was assessed in a similar manner for exploring their biological relevance. The clinical validity of biomarkers was assessed using sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and AUC of the ROC curves between cancer versus benign (non-neoplastic nodules and follicular adenoma). The optimal cutoff value was chosen as the threshold that maximized the AUC. All analyses were internally validating using random split sample. The predictive value of biomarkers was assessed in both the test set and a validation set. Final models and optimal cutoff values were derived from the test set and verified in the validation set.
Results
Immunohistochemical analysis findings
Immunohistochemical analysis of seven proteins was carried out to determine the differences in their total cellular expressions and in subcellular localization (cytoplasmic and nuclear levels) in benign thyroid nodules (non-neoplastic nodules and follicular adenoma) and TC. Biomarker expression levels (average scores defined as the sum of % positivity score and intensity score evaluated by two scorers independently) in benign nodules and cancer tissues are summarized in Table 2. The concordance correlation coefficient (ccc) was used to measure the agreement between the two scorers on the average cytoplasmic score and average nuclear score. The ccc for PGK1 average cytoplasmic score was 0.998 [CI 0.996–0.999], and for average nuclear score was 0.975 [CI 0.958–0.985], indicating high interobserver reliability of the two scores. The ccc for all the other six proteins were also >0.95, suggesting high interobserver reliability of the two scores.
Expression levels are the sum of the score for percentage immunopositive cells and intensity of immunostaining and are summarized as mean±standard deviation (mean±SD).
PTEN, phosphatase and tensin homolog.
Representative photomicrographs of tissue sections showing the immunostaining expression patterns of all seven proteins (PGK1, PKM2, Cyclin D1, Galectin-3, PTEN, S100A6, and Profilin-1) in benign thyroid nodules and TC are shown in Figure 1. All seven proteins were detected in thyroid tissues, though there was differential subcellular localization in benign (non-neoplastic nodules and follicular adenoma; Fig. 1A and B, respectively) and TC (Fig. 1C and Table 2). Reduced PGK1 nuclear expression was observed in TC compared with benign nodules and adenomas (Fig. 1(i) and Table 2). Both nuclear and cytoplasmic staining was observed for PKM2 with a significant decrease in nuclear expression in TC (Fig. 1(ii) and Table 2). An increase in nuclear expression of Cyclin D1 was observed in cancer compared with benign nodules and adenomas (Fig. 1(iii) and Table 2). Both nuclear and cytoplasmic expression of Galectin-3 was increased in TC compared with nonmalignant tissues (Fig. 1(iv) and Table 2). Nuclear PTEN expression was significantly downregulated in malignant compared with benign tissues including adenomas (Fig. 1(v) and Table 2); expression of cytoplasmic and nuclear S100A6 was decreased (Fig. 1(vi)). A decrease in nuclear expression of Profilin-1 was also observed in TCs compared with benign tissues (Fig. 1(vii) and Table 2).
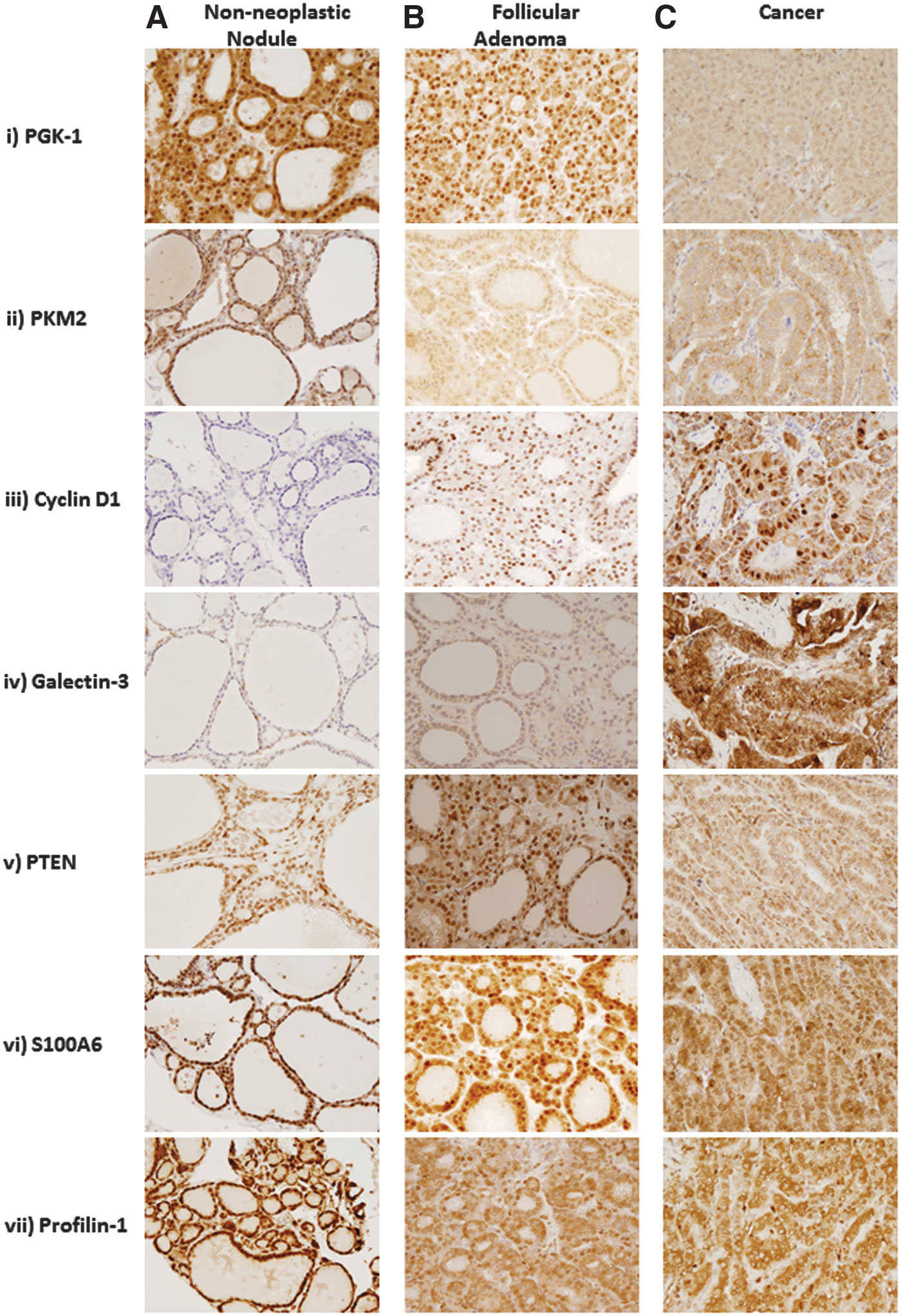
Immunostaining of proteins in benign thyroid nodules (non-neoplastic tissues, follicular adenomas) and thyroid cancers. Representative photomicrographs given in panels
Biomarker predictive values derived from surgical FFPE for benign versus malignant thyroid nodules
The predictive value of the biomarkers to distinguish TC from benign thyroid nodules (non-neoplastic nodules and follicular adenoma) was determined. The cases were divided into a test set (27 benign, 31 adenoma, 57 cancer) and a validation set (26 benign, 31 adenoma, 57 cancer) using random split sample. With the exception of cytoplasmic Profilin-1 and cytoplasmic S100A6, all the biomarkers had subcellular compartmental nuclear expressions associated with TC (Table 3). Nuclear PGK1 emerged as the strongest predictor of cancer in comparison with nonmalignant tissues (test set: OR=0.05 [CI 0.01–0.17], p<0.0001, AUC=0.93; validation set: OR=0.05 [CI 0.01–0.21], p<0.0001, AUC=0.96; Table 3) underscoring its potential clinical applicability. It was hypothesized that a model developed from a panel of these biomarkers could be more predictive of cancer compared to nuclear PGK1 alone. To test this hypothesis, model selection under multiple imputed data was used (35) to achieve an optimal final test set model of reduced nuclear PGK1 and overexpressed nuclear Galectin-3 (Table 3).
Surgical FFPE malignancy score based discrimination of benign versus malignant thyroid nodules
Based on the high predictive and discriminatory values, nuclear PGK1 and nuclear Galectin-3 risk scores were used to differentiate TC from benign thyroid nodules. A risk score model was developed in the test set, and an optimal cutoff value that maximizes the AUC was chosen. The risk score model based on regression estimates as weights is given as malignancy score=19.92+(2.128×Nuclear Galectin-3 score) – (3.322×Nuclear PGK1 score). The optimal cutoff was 0.86 (IHC score of 5.67 and AUC of 0.94; Table 4). Notably, 98% (specificity) of nonmalignant tissues were correctly identified in the test set with a sensitivity of 90%. The clinical applicability of this cutoff value was verified in the validation set, as it achieved an AUC of 0.90, with a sensitivity of 80%, and a specificity of 99% (Table 4).
Optimal cutoff: nuclear PGK1=5.6; nuclear Galectin-3=1.
Benign (non-neoplastic nodules and follicular adenoma) vs. cancer: malignancy score=19.92+(2.128×nuclear Galectin-3 score) – (3.322×nuclear PGK1 score).
Biomarker predictive values for distinguishing benign from malignant nodules in surgical FNAB-FFPE cell blocks
To test the efficacy of PGK1 and Galectin-3 for identifying TC from benign thyroid nodules (non-neoplastic nodules and follicular adenoma), FNAB FFPE cell blocks were prepared from 50 fresh surgically resected thyroid nodules, and IHC was performed for these proteins and correlated the FNAB findings with the surgical pathology diagnosis. Representative photomicrographs depicting immunostaining for PGK1 and Galectin-3 in FNAB FFPE cell blocks are shown in Figure 2A. Based on the PGK1 nuclear IHC score positivity cutoff value of <5.6 for TC, a diagnosis was made and compared to the surgical diagnosis for each case to assess concordance between surgical pathology diagnosis and biomarker-based diagnosis.

(
The PGK1 IHC-based diagnosis matched surgical diagnosis in 34/50 (68%) of FNAB cases (Table 5 and Supplementary Table S1; Supplementary Data are available online at
Patients included in FFPE FNA: age, range 25–78 years, median 53 years; male=12, female=88 cases.
Patients included in cytosmears: age, range 25–77 years, median 48 years; male=6, female=20 cases.
SD, surgical diagnosis.
Efficacy of biomarkers for identifying TC using surgical cytosmears
The efficacy of PGK1 and Galectin-3 for detecting TC using cytosmears obtained at surgery was evaluated in 26 cases. Representative photomicrographs depicting immunostaining for PGK1 and Galectin-3 in cytosmears are shown in Figure 2B. Based on the PGK1 Nuclear IHC score positivity cutoff value of <4 for TC and ≥4 for benign cases, IHC-based diagnosis was made and compared to the surgical diagnosis for each case to assess the degree of correspondence between the surgical pathology diagnosis and biomarker based diagnosis. The PGK1 IHC-based diagnosis matched the surgical diagnosis in 25/26 (96%) of cytosmears (Table 5 and Supplementary Table S2).
Discussion
Based upon the authors' earlier proteomic studies and functional relevance of seven proteins (PGK1, PKM2, Cyclin D1, Galectin-3, PTEN, S100A6, and Profilin-1) in human cancers, particularly in TC (30,36), the current study evaluated the expression of the panel of these proteins in human thyroid tissues, and examined their potential to serve as a diagnostic tool for distinguishing TC from benign thyroid nodules (non-neoplastic nodules and follicular adenomas). The significant association of decrease in nuclear and/or cytoplasmic expression of PGK1, PKM2, PTEN, and Profilin-1 and increase in nuclear and/or cytoplasmic expression of Cyclin D1 and Galectin-3 in TC warranted a study on their potential utility in future presurgical FNAB as a part of a diagnostic strategy to improve the detection of TC among preoperative indeterminate thyroid nodules. To the authors' knowledge, this is the first report to detect the expression of Profilin-1 in thyroid tissues as a cancer biomarker. Ding et al. reported Profilin-1 to be downregulated in breast cancers with propensity to metastasize (37). PGK1, PKM2, S100A6, and Galectin-3 have previously been identified in the authors' studies using secretome analyses of TC cell lines in TC (30,36). Two other proteins, cyclin D1 and PTEN, were investigated in the selected panel of candidates based on their important biological role in head and neck cancers and/or TC (38).
PGK1 is a metabolic protein that has been shown to have different roles in cancer progression, and affects DNA replication and repair in the nucleus (39). Thus, PGK1 has dual roles that are essential for tumorigenesis: regulating cancer cell metabolism and gene transcription. PGK1 is expressed in several cancers such as breast, ovarian, pancreatic, and gastric cancer (39 –41). Cyclin D1 is a member of the family of cyclins that function as regulators of cyclin-dependent kinases for controlling cell proliferation. Overexpression of cyclin D1 has been observed in thyroid (38,42 –45), breast (46), and head and neck squamous carcinoma (47). Galectin-3 is a member of a family of carbohydrate binding proteins and is known to have roles in apoptosis, cell adhesion, innate immunity, and T-cell regulation. In support of the findings are the reports from other groups that demonstrated expression of Galectin-3 in TC (48 –50). Galectin-3 positivity in FNAB samples from PTC was associated with aggressive pathological features such as extrathyroidal extension and lymph node metastasis (51). More than 60 protein expression studies evaluating more than 6000 thyroid specimens have been reported and reviewed that investigate the utilization of Galectin-3 as a TC marker (52). The great variance in IHC methodologies used in these studies, specificity of different Galectin-3 antibodies, and inherent high biotin expression in thyrocytes that requires an avidin-biotin treatment blockade or use of biotin free detection systems may account for inconsistencies in its reported diagnostic utility. Further, Galectin-3 genomic expression studies have shown inconsistent results and thus are not recommended. Hence, the translation of Galectin-3 as a TC biomarker into clinical use has not been successful. In the present study, adequate steps were taken to ensure blockage of endogenous biotin in thyrocytes and ensuring specific detection of Galectin-3. Therefore, its potential was explored in combination with other proteins as a panel of biomarkers. PTEN is a tumor suppressor that is mutated in several cancers (37,53 –56). It negatively regulates signaling of the PI3K pathway. The current findings, using PGK1 and Galectin-3, suggest that these proteins together in a panel, rather than individually, have the potential to serve as effective biomarkers for distinguishing benign thyroid nodules from TC in a clinical setting. The malignancy score based on regression estimates as weights resulted in an AUC of 0.94 with high specificity (98%), PPV (97%), sensitivity (90%), and NPV (91%) in the test set, and a similar performance in the validation set (AUC of 0.90, with high specificity [99%], PPV [99%], sensitivity [80%], and NPV [84%]).
Importantly, all the surgical FNAB FFPE cell blocks could be accurately classified using a combination of nuclear PGK1 and nuclear Galectin-3. Nine of 50 cases were nondiagnostic in presurgical FNAB cytology; the protein biomarker analysis classified three cases as adenomatous nodules and six cases as papillary TC, including one microcarcinoma, and these findings were supported by the surgical pathology. Further, 19 indeterminate cases in presurgical FNAB cytology (13 AUS/FLUS, 2 FN/SFN, and 4 suspicious for malignancy) were also accurately classified based on the molecular diagnosis concordant with their surgical pathology. Importantly, IHC biomarker analyses identified two follicular carcinomas that had been classified as FN/SFN and suspicious for malignancy based on presurgical FNAB cytology. Notably, 96% of cytosmears could be accurately classified using nuclear PGK1 alone, obviating the use of Galectin-3 in these cases. These preliminary data from direct FNAB from the surgical thyroidectomy specimens has overcome the potential sampling errors.
One of the limitations of the study is the use of fresh surgically removed thyroid nodules for FNAB preparation of FFPE cell blocks and cytosmears rather than the use of preoperative FNAB. The current report provides a proof of principle using these surgical FNAB preparations for biomarker analysis. However, it is recognized that its ultimate clinical applicability will require confirmation by preoperative FNAB sampling in a large cohort of patients with benign, malignant, and indeterminate tumors and subsequent surgical pathology correlations that can be achieved through a prospective, blinded multicenter study with a panel of expert surgeons, pathologists, and researchers. Nevertheless, the results from direct sampling of surgical material suggest it could improve preoperative surgical selection particularly in patients with FNAB cytology showing features of atypia, suspicious for malignancy, or indeterminate findings.
In comparison to this approach of using a panel of proteomic biomarkers to discriminate benign from indeterminate thyroid nodules, there are two other alternative FNAB genomic strategies that have been proposed (12,14,23). Nikiforov et al. used a gene mutation panel test in FNAB samples derived from 513 thyroid nodules that has high specificity (96–99%) and PPV (87–95%) but low sensitivity (57–63%) and NPV (72–94%) for indeterminate nodules (10). The addition of this mutation panel to FNAB cytology can be used to stratify indeterminate nodules with positive markers with high probability of malignancy for total thyroidectomy. The limitation of this algorithm is that FNABs negative for mutations testing did not reliably exclude malignancy (23,57). However, the recent centralized testing of the gene panel in a prospective multicenter and blinded investigation validated its value in combination with local cytopathological evaluation of preoperative thyroid nodule FNAB for accurate clinical risk assessment with a specificity of 89% (72–95%), a PPV of 86% (72–95%), a sensitivity of 48% (29–68%), and a NPV of 64% (47–79%) for indeterminate nodules or non-diagnostic cytologic diagnoses (58). In the second approach, a method has been developed based upon a GEC using RNA expression analysis that has been validated in multiple studies (15 –21,24). Taken together, the rate of GEC benign results appears to be about 50%. These tests have been included in the 2013–14 revisions of the National Comprehensive Cancer Network guidelines on TC, and their utility is recognized (59). By comparison, the IHC protein biomarker strategy used in the present study is based on subcellular changes in protein expression and has the potential to offer a sensitive and cost-effective diagnostic test as an adjunct to FNAB cytopathology. A large-scale validation of the proteomic markers in an independent patient cohort will be required to confirm its ultimate clinical application.
In conclusion, IHC analyses of the selected panel of seven proteins on archived surgical tissues showed differential subcellular localization between benign and malignant thyroid tissues. In-depth data analyses suggest that a combination of nuclear PGK1 loss and overexpression of nuclear Galectin-3 could not only distinguish benign from malignant thyroid nodules, but also characterize a subset of nodules considered being indeterminate with high sensitivity and specificity. These findings underscore the potential utility of analyzing the expression of these proteins in presurgical FNAB as a diagnostic strategy to improve surgical selection among nodules with indeterminate FNAB cytology. This is of paramount importance for not only avoiding unnecessary surgery on benign nodules with its associated morbidity, but also for reducing healthcare costs through selection for surgery those nodules at risk for malignancy.
Footnotes
Acknowledgments
The financial support of this work from Da Vinci Gala Fundraiser, Alex and Simona Shnaider Chair in Thyroid Cancer (P.G.W.), Canadian Institutes of Health Research (CIHR) for CIHR Chair in Advanced Cancer Diagnostics (R.R.), and the Mount Sinai Hospital Department of Medicine Research Fund is gratefully acknowledged.
Author Disclosure Statement
P.G.W. and R.R. are shareholders in Proteocyte Diagnostics, Inc. All the other authors declare that they have no competing interests.