
Abstract
Background:
Thyroid cancer (TC) incidence is rising in many countries, but the corresponding mortality is constant or declining. Incidence increases appear largely restricted to small papillary TC in young/middle-age individuals. We compared age-specific incidence rates across countries and time periods in order to estimate the fraction of TC possibly attributable to increased surveillance of the thyroid gland (diagnostic changes) following the introduction of neck ultrasonography in the 1980s.
Methods:
We focused on high-resource countries, including four Nordic countries, England and Scotland, France, Italy, the United States, Australia, Japan, and the Republic of Korea. Before the 1970s, TC incidence in Nordic countries increased proportionally to the second power of age, consistent with the multistage model of carcinogenesis. Using this historical observation for reference, we attributed the progressive departure from linearity of the age curves in each country to an increased detection of asymptomatic disease in young/middle-age individuals. The proportion of cases attributable to diagnostic changes was estimated from the difference between observed rates and those expected using the Nordic countries as reference.
Results:
Diagnostic changes may account for ≥60% of TC cases diagnosed in 2003–2007 in women aged under 80 years in France, Italy, the United States, Australia, and the Republic of Korea, and approximately 50% in other assessed countries, except Japan (30%). The proportions attributable to diagnostic changes were higher in countries with largest incidence increases and were consistent across sexes, although increases were smaller and delayed in men.
Conclusions:
A large proportion of TC cases diagnosed in high-resource countries in the last two decades are likely to be due to diagnostic changes. This proportion has progressively increased over time, and it is likely to grow further in the future. Since there is evidence of harm but no proof of benefit from the intense scrutiny of the thyroid, the dangers of overdiagnosis and overtreatment of TC should be urgently addressed.
Introduction
T
The contribution of established TC risk factors, including environmental or medical radiation (10), a deficit or excess of iodine intake (11), and excess body mass (including being overweight or tall) (12), or suspected nutrition-related determinants, such as dietary aspects (13), nitrates and nitrites, and certain microelements in the diet or in drinking water (14), to the observed incidence trends is unclear. Upward trends have, however, clearly coincided with major increases in the use and sensitivity of diagnostic techniques for the assessment of the thyroid gland (5,8). Until the late 1970s, most TCs were found in patients presenting with nodules causing compression symptoms or visible neck masses and only relatively big nodules were assessed by palpation and biopsy. The advent of neck ultrasonography and ultrasound-guided fine-needle biopsy in the late 1980s enabled the detection and histologic examination of nodules as small as a few millimeters. Additional increases in TC diagnoses have resulted from the spread of portable ultrasound machines and, after 2000, new imaging technologies (i.e., computed tomography [CT] and magnetic resonance imaging) used for a variety of medical indications related or unrelated to thyroid symptoms (5).
In many countries, the shape of the age-specific incidence curves of TC have changed over time because increases particularly concerned young/middle-aged individuals (3,4). In the present study, we have investigated how much of this increase may be attributed to diagnostic changes and increased surveillance of the thyroid gland. Our analyses are based on a comparison of the shape of age-specific incidence rates of TC in different countries over time.
Materials and Methods
Data sources
New cases and rates of TC by age, sex, and calendar year of diagnosis were obtained from population-based cancer registries from the series Cancer Incidence in Five Continents (CI5) Volumes I to X (
Regional registries: France (Bas-Rhin, Calvados, Doubs, Isère, Haut-Rhin, Herault, Somme, Tarn); Italy (Lombardy-Varese, Modena, Parma, Ragusa, Romagna, Torino); Japan (Osaka, Miyagi Prefectures); Republic of Korea (Seoul); United States SEER 9 registries (SEER: states of Connecticut, Hawaii, Iowa, New Mexico, and Utah and metropolitan areas of San Francisco-Oakland, California; Detroit, Michigan; Seattle-Puget Sound, Washington; and Atlanta, Georgia).
Average annual number of cases obtained for the most recent 5-year period.
Average annual number of person-years (expressed in million person-years at risk) obtained for the most recent 5-year period.
For Republic of Korea, it refers to period 1993–1997.
ASRs, age-standardized (world population) incidence rates.
Statistical methods
Age-standardized incidence rates (ASRs) per 100,000 person-years were calculated using the world standard population. Standardized rate ratios were computed from comparison of ASRs in 2003–2007 versus 1988–1992, with the exception of the Republic of Korea for which rate ratios referred to periods 2003–2007 compared with 1993–1997. The confidence intervals of rate ratios were not computed because small meaningless differences between groups can lead to significant p values in studies of large sample size. ASRs versus 5-year periods were plotted on a semi-log scale. Age-specific incidence rates were plotted on a log–log scale or a semi-log scale, as indicated, by 5-year age groups (from 15–19 to 75–79 years). Cubic splines (15) were used to smooth the incidence curves.
Age-period-cohort (APC) models have been applied to TC incidence trends in an attempt to distinguish period effects, which can be influenced by diagnostic changes, from cohort effects, which often reflect a changing prevalence and distribution of TC risk factors across different birth cohorts (3). Although we were able to exclude major cohort effects through visual inspection of the cohort-specific rates by age group in our study population (Supplementary Fig. S4; Supplementary Data are available online at
Age-specific rates of TC incidence for periods prior to diagnostic changes
For the majority of epithelial carcinomas, the incidence rate has been shown to increase exponentially with age (17). The multistage model of carcinogenesis demonstrated the wide applicability of the formula rate ∝ (age) k where the exponent k is to be estimated for individual carcinomas. The relationship between the logarithm of incidence rate and the logarithm of age is linear—log(rate) = c + k × log(age), where c is a constant value (17). This would result in a straight line when plotting incidence rates against age on a log–log scale. However such a relationship could be distorted by changes in carcinogenetic exposures, such as tobacco smoking and lung cancer (17), or in diagnostic practices, such as cervical cancer screening (18 –20).
We took advantage of the availability of high-quality cancer data from four Nordic countries relative to periods preceding the time at which ultrasonography started being widely used to inspect the thyroid gland (late 1980s). Age-specific incidence rates of TC for the 1958–1967 period from population-based cancer registries in the four Nordic countries were analyzed and their compatibility with the shape predicted by the multistage model of carcinogenicity examined. The exponent k was estimated as the slope of the linear regression between the logarithm of incidence rate and the logarithm of age. The pooled exponent of the four Nordic countries was estimated for each sex and referred to as the historical shape of age-specific profile for TC incidence.
As a sensitivity analysis, we also evaluated the historical shape of age-specific profile for TC prior to the introduction of ultrasonography in two other long-duration cancer registries, i.e., Manitoba, Canada (1958–1967) and Israel (1963–1967).
Expected TC rates in a scenario without diagnostic changes
The expected incidence rates of TC during the 2003–2007 period for all study countries were obtained by hypothesizing that the age curve of the disease would have retained the historical shape observed prior to the 1970s in the Nordic countries. A key observation was that, within all studied countries, the TC incidence rates at ages 75–79 years were of approximately equal magnitude for each country across periods and birth cohorts, in contrast to the large rate increases seen in younger age groups. This reasonably allowed the possibility to add a constraint that set the expected incidence rates to be equal to those observed within this age group. The expected rates for all other age groups were therefore extrapolated according to the multistage model, assuming linearity on a log–log scale, with the same slope as that estimated for the Nordic countries and restricted to pass by the mid-point of the age group 75–79. The progressive departure from linearity (multistage model) of the observed rates was hypothesized to be attributable to the increased detection of small TC. The proportion of cases attributable to diagnostic changes was estimated, based on the difference between the observed and expected rates. Corresponding 95% confidence intervals (CI) were obtained using standard bootstrap methods (21).
Results
Table 1 shows TC incidence data by sex for ages 15–79 for the eight selected populations, ASRs, and the corresponding rate ratios for the periods 2003–2007 compared to 1988–1992 (1993–1997 for the Republic of Korea). Trends in the ASRs over time are plotted in Figure 1. TC rates across countries differed much more in 2003–2007 than in 1988–1992 (1993–1997 for the Republic of Korea). Rate ratios >2.0 were found in France, Italy, and the Republic of Korea (in both sexes) and in Australia and the United States (women only). The greater than fourfold increase in incidence rates in the Republic of Korea in just 15 calendar years is noteworthy, with ASRs in 2003–2007 being by far the highest worldwide and markedly different by sex (59.9 and 11.3 per 100,000 women and men, respectively). The 2003–2007 female-to-male ratio ranged from 2.8 in the Nordic countries, and England and Scotland, to 5.3 in the Republic of Korea (data not shown).
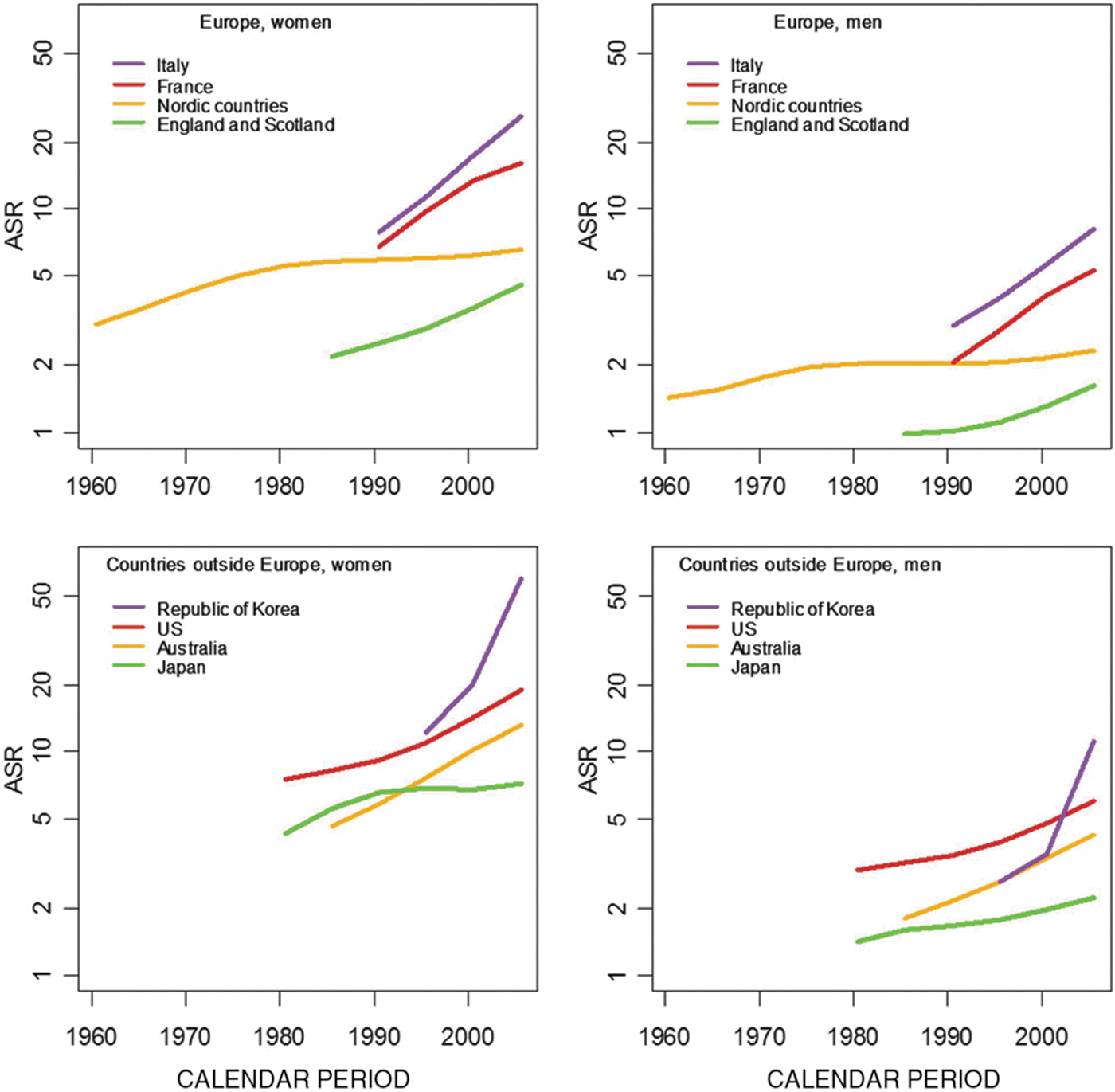
Age-standardized incidence rates (ASRs) per 100,000 of thyroid cancer by sex and country, age 15–79 years.
Figure 2 shows sex- and age-specific TC incidence rates in the historical period 1958–1967 for the four Nordic countries. The logarithm of the age-specific TC incidence rate is plotted against the logarithm of the mid-point of the age group and the straight dotted line represents the slope of the linear regression between these two variables. The slope of the regression line was significant in all countries. Values of the linear regression slope ranged from 1.6 (Norway) to 2.3 (Denmark) in women, and from 2.2 (Sweden and Norway) to 2.6 (Denmark and Finland) in men. No significant heterogeneity in slope values was detected across Nordic countries (p-values for heterogeneity = 0.06 in women and 0.96 in men) thus allowing us to compute a combined slope whose value has been estimated to be 2.0 in women and 2.4 in men (Supplementary Fig. S1). Sensitivity analyses of TC incidence by age before the introduction of ultrasonography in Manitoba, Canada and in Israel showed compatible findings with those observed in the Nordic countries; that is, there was no major departure from linearity with a linear regression slope equal to 1.5 and 1.3, respectively (data not shown). Figure 3A and B shows a comparison of age-specific TC rates observed in 2003–2007 and the corresponding rates expected if age curves had retained the historical shape. For all countries except Japan (in men), the observed age curve of TC incidence in 2003–2007 was elevated relative to the expected age curve and resembled an inverted U-shaped curve instead of a straight line.

Age-specific incidence rates per 100,000 (rates) of thyroid cancer in four Nordic countries in a log–log scale, 1958–1967. The logarithm of incidence rate is plotted against the logarithm of the mid-point of the age group. The straight dotted line represents the slope of the linear regression between the two variables.
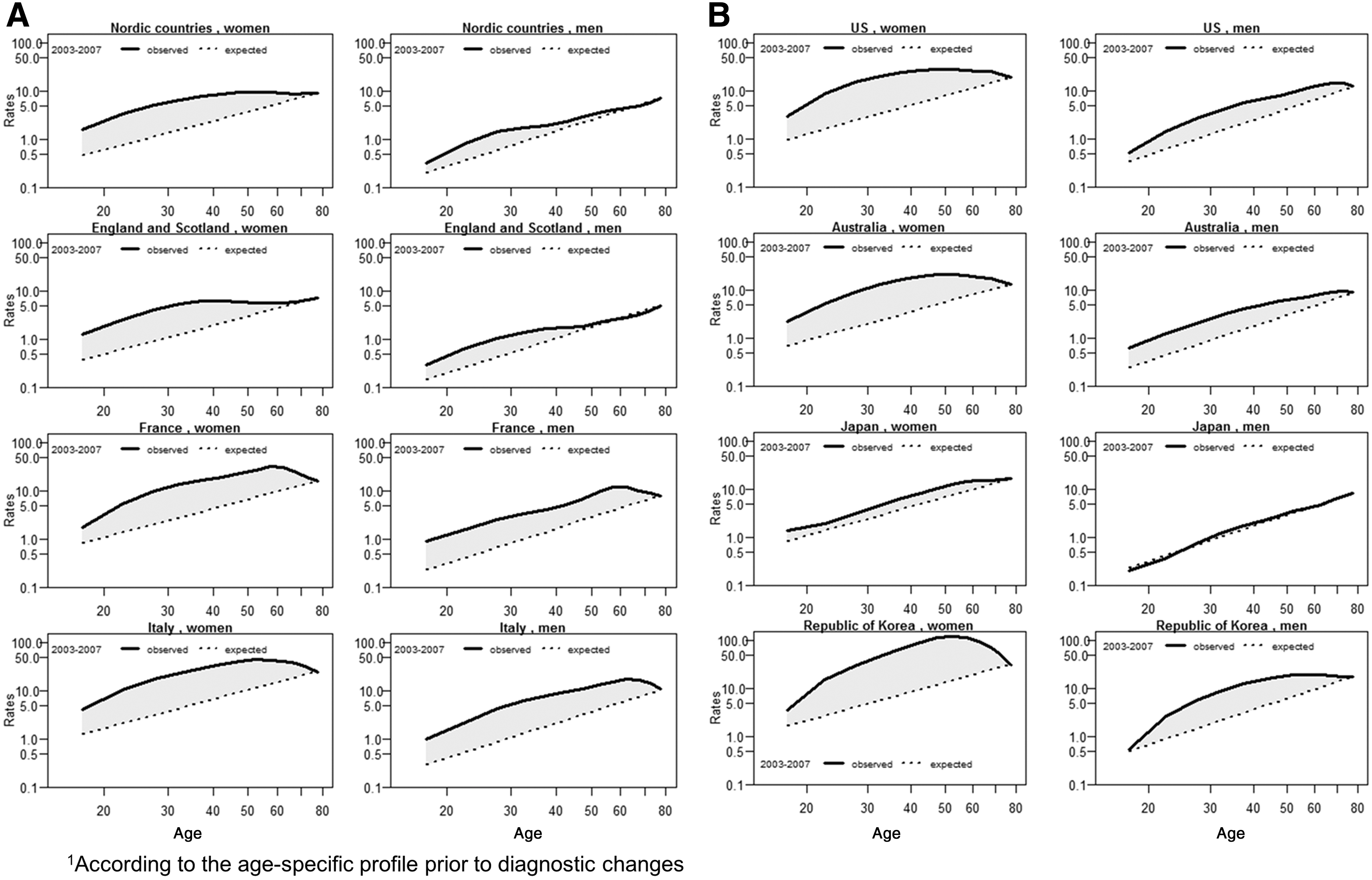
Observed (solid lines) and expected (dashed lines1) age-specific rates per 100,000 of thyroid cancer in 2003–2007 in selected European
Supplementary Figures S2A, S2B, and S3 show the gradual modification of TC age curves from 1988–1992 to 2003–2007 for women and men in different countries; that is, there was a gradual departure from linearity in countries in which incidence increases were observed.
Supplementary Figure S4 shows cohort-specific TC incidence rates by age groups in women. For each age group, TC risk increased across birth cohorts, although to a different extent across countries. However, there was no evidence of abrupt changes in rates in consecutive generations, thus allowing us to exclude important cohort effects.
Estimates of the proportion of TC incident cases attributable to diagnostic changes based on differences between observed and expected rates, overall and by sex and age, are presented in Table 2. The largest difference between observed and expected ASRs was found in both women and men in the Republic of Korea, with 49.8 and 6.5 extra cases of TC per 100,000, respectively. Large discrepancies between observed and expected ASRs were found also in women in France (10.9 extra cases per 100,000), Italy (18.6), and the United States (13.6) (Table 2).
O, observed; E, expected; CI, confidence interval.
Discussion
Our study provides for the first time a quantitative estimation of the impact of diagnostic changes in the steep increase in TC incidence observed in many countries (1,3,5,6,22). Our estimates are based on the assumption that the age curve of TC incidence prior to the introduction of ultrasonography represents the historical age-related behavior of symptomatic TC. The progressive changes of age-specific curves are hypothesized to be due to the intense search for thyroid nodules that very seldom lead to death in young and middle-age individuals. According to our estimates, diagnostic changes accounted for 60% or more of all TC cases diagnosed in 2003–2007 in women below the age of 80 years in France, Italy, the United States, Australia, and the Republic of Korea, and 30% or more in other very high-income countries. In France and Italy, men experienced proportionally similar increases as found for women, although the number of cases was approximately a third. Lower proportional increases in men than women were found in other countries.
Data for Nordic countries suggest that, prior to the advent of ultrasonography, TC incidence rates in both sexes increased approximately proportionally to the second power of age consistently with the behavior of most epithelial carcinomas according to the multistage model of carcinogenicity (17). Hormone-dependent carcinomas in women, such as breast (23) and cervix (24), are exceptions because incidence rates in unscreened populations grow exponentially until middle age and exhibit an inflexion thereafter. Although TC has a clear predilection for women, available studies suggest that hormone-related events in a woman's life (e.g., pregnancies) are not important risk factors per se (25,26) but may rather be circumstances that pose special demands on thyroid function and hence predispose women to iodine deficiency, thyroid cell proliferation, and the appearance of goiter and thyroid nodules (27). In addition, pregnancies, contraception, and perimenopausal symptoms expose women to medical surveillance more frequently and earlier than men (3,22). In fact, the progressive secular curving of the age-specific incidence rates started earlier and was more pronounced in women than in men. The presence of small asymptomatic papillary TC was found in >10% of both sexes in autopsy series (28,29). It is therefore not surprising that intense surveillance of the thyroid gland can uncover the large reservoir of indolent thyroid tumors, mostly, but not exclusively < 10 mm in diameter (7). The upward incidence trends and changes in the age-specific curves in the last two decades were accompanied by very low and stable TC mortality rates (1,5,6).
New or increased exposure to TC risk factors in younger generations can also lead to changes in incidence age curves. For the thyroid gland, a very radio-sensitive site in children and adolescents (30), medical exposure to ionizing radiation is a possible explanatory factor for the trends, given that it has been the fastest growing source of human radiation exposure in the last decades—for example, from 11% of total exposure in 1980 to 36% in 2006 in the United States (31). However, the only prospective study on the topic did not show a consistent association of TC with history of x-ray procedures (10). The modest association with dental x-rays performed before 1970 was not stronger for exposure in children than in adults. This led to the consideration that the association may have been induced by screening bias; that is, a positive correlation existed between dental care and medical surveillance in general (10). CT scans entail much heavier radiation than x-rays and exposure in children and adolescents has been shown to be associated with increased TC risk (risk ratio [RR] = 1.40 [95% CI, 1.23–1.59]) (32). However, CT scan use was limited prior to 2000 and should not have affected the adult populations explored in our present study. Increases in overweight and obesity have accompanied the rise in TC incidence, but the associations of weight and height with TC risk are weak and not restricted to the papillary type (12,33). Iodine deficiency has been shown to be associated with TC mortality in past (11) and recent ecological studies (34). According to the World Health Organization (35), the populations of a majority of countries in Europe, including France and Italy, still experience mild iodine deficiency. Iodine deficiency is not associated with papillary TC, and it may have affected incidence trends via increases in the prevalence of signs and symptoms of thyroid abnormalities that trigger further clinical investigation (27). The contribution of other suspected risk factors such as ingestion of nitrates and nitrites and the presence of certain micro-elements in the diet or drinking water (14) is even more uncertain. Despite our choice of not using APC models to assess the interaction between period and cohort effects, we were able to rule out the presence of important cohort effects (Supplementary Fig. S4). Other authors (3,22,36) who have applied APC models to TC trends have concluded that cohort effects played a considerably smaller role, if any, compared to period effects.
It seems, in any case, difficult to conceive any modern lifestyle or environmental risk factor that might vary across very high-income countries to the extent that the variability of current TC incidence trends would be affected. Conversely, how health systems are organized and funded, the number and attitude of physicians, and the penetration of new diagnostic and screening practices are known to differ substantially even across the richest countries and have been shown to correlate with the probability of detecting benign and malignant thyroid diseases (8,37 –45).
For instance, in the United States, nearly 16% of CT and magnetic resonance images show incidental thyroid nodules, of which around three quarters are <1.5 cm (5), and more patients receive a TC diagnosis after an evaluation of an incidentally found thyroid nodule than after the evaluation of a symptomatic or palpable nodule. Another study in the United States found a correlation between increased TC incidence and the use of thyroid ultrasound and fine-needle aspiration (40). Several studies in the United States and Canada, though not all (41), found that markers of higher access to the health care system, such as socioeconomic status, were associated with an increased incidence of TC, mainly the papillary histologic type (37,42 –44). An ecological correlation across the United States was reported between TC incidence and the density of endocrinologists and surgeons and also the use of cervical ultrasonography (45).
The Republic of Korea represents a unique example of sudden large-scale introduction of opportunistic screening of the thyroid with ultrasonography in 1999 (8) when neck ultrasonography started being offered at a relatively low cost (between $30 and $50) back-to-back with organized screening programs for five other cancers (8).
Our study has limitations and consequently the proportion of cases of TC attributable to diagnostic changes should be interpreted with caution. First, we relied on Nordic countries to establish the historical age curve of TC incidence prior to diagnostic changes. However, TC incidence for the same period in Manitoba, Canada and Israel showed age profiles similar to those shown for Nordic countries. In addition, even in countries for which shorter cancer registration data were available, the gradual distortion of the age-specific curves over periods allowed us to deduce a similar pattern. Secondly, we computed the number of TC incident cases attributable to diagnostic changes by fixing the observed-to-expected ratio in the group 75–79 to unity. The choice of this age group is debatable but was considered a rational choice given that TC incidence rates were similar for this age group, across calendar time and birth cohorts, thus forming an age group largely unaffected by diagnostic changes. In the United States and Australia, however, the trajectory of the age-specific rates for different periods converged only at a later age, approximately 80–84. For these two countries we therefore performed a sensitivity analysis by extending the age range up to age 84. Expected rates were constrained to be equal to the observed rates at ages 80–84, instead of 75–79 years, but the change did not substantially alter our findings.
In conclusion, this study provides the first estimate of the large proportion of TC attributable to diagnostic changes in different periods and countries. While no benefits in terms of prevention of cancer deaths have been demonstrated, the human and financial costs of this enhanced surveillance are huge (46). Total thyroidectomy can induce hypoparathyroidism and vocal cord paralysis (8), and supraphysiological thyroid replacement therapy is associated with cardiovascular side effects and bone fractures (47).
Solutions to reduce overdiagnosis and overtreatment of low-risk TC would include 1) avoidance of TC screening activities; 2) reclassification of low-risk TC using terms other than cancer, as has been successfully accomplished for cervical intra-epithelial neoplasia grades 1–3 (48); 3) development and application of less aggressive guidelines for the management of thyroid nodules and TC (5,6,47); and 4) establishment of randomized clinical trials and observational cohorts in which the outcome of watchful waiting approaches can be evaluated.
Footnotes
Acknowledgments
This study was supported by the International Agency for Research on Cancer (IARC) and the Italian Association for Cancer Research (AIRC) (grant no. 11859).
Author Disclosure Statement
The authors have no competing interests to declare.