
Abstract
Background:
Carcinoma showing thymus-like differentiation (CASTLE) is an extremely rare malignant neoplasm of the thyroid that originates from ectopic thymic tissue. No sufficient evidence exists regarding the efficacy of chemotherapy for cases with distant metastases or advanced disease because of the rarity of the disease itself.
Patient:
We report a case of CASTLE with lung metastasis that showed good responses to first-line (cisplatin, doxorubicin, vincristine, and cyclophosphamide) and second-line (carboplatin and paclitaxel) chemotherapies.
Summary:
This is the first case of CASTLE reported to show a good response to two serial chemotherapies.
Conclusion:
This case suggests that CASTLE is a chemosensitive tumor and that chemotherapy should be attempted in patients with advanced or metastatic CASTLE.
Introduction
C
Patient
A 46-year-old man with no significant past medical history presented with a 6-month history of a right thyroid nodule. Physical examination revealed a right thyroid nodule with tenderness, but there was no lymphadenopathy. The laboratory findings, including thyroid function, thyroglobulin, carcinoembryonic antigen, and calcitonin, were within the respective normal limits. Ultrasonography revealed a 32 mm round-shaped tumor located in the lower part of the right lobe of the thyroid. The tumor was solid and showed a heterogeneous hypoechoic pattern. Positron emission tomography/computed tomography (PET/CT) showed a thyroid nodule with increased uptake of [18F]fluorodeoxyglucose at a maximum standardized uptake value of 9.0. Metastasis was not detected in the lymph nodes, lungs, or other organs. Fine-needle aspiration cytology for the thyroid nodule was performed, and the smear showed tumor cells forming a cohesive cluster. Tumor cells also showed nuclear atypia with very high nuclear/cytoplasmic ratios. The aspirate was interpreted as a malignant thyroid neoplasm, without further definitive classification. The patient underwent total thyroidectomy with right modified radical neck dissection. Microscopically, the tumor was composed of atypical cell nests separated by dense fibrous septa with many lymphocytes and plasma cell infiltration (Fig. 1A). There were no histological findings suggestive of typical thyroid tumor, including papillary carcinoma, follicular carcinoma, and medullary carcinoma. Immunohistochemically, the tumor cells were positively immunoreactive for CD5 (Fig. 1B), but negative for thyroglobulin, thyroid transcription factor-1, and calcitonin (data not shown). Thus, a diagnosis of CASTLE with central and right lateral neck lymph node metastases was made. Postoperative radiation to the neck (54 Gy/30 fractions) was performed as adjuvant therapy.
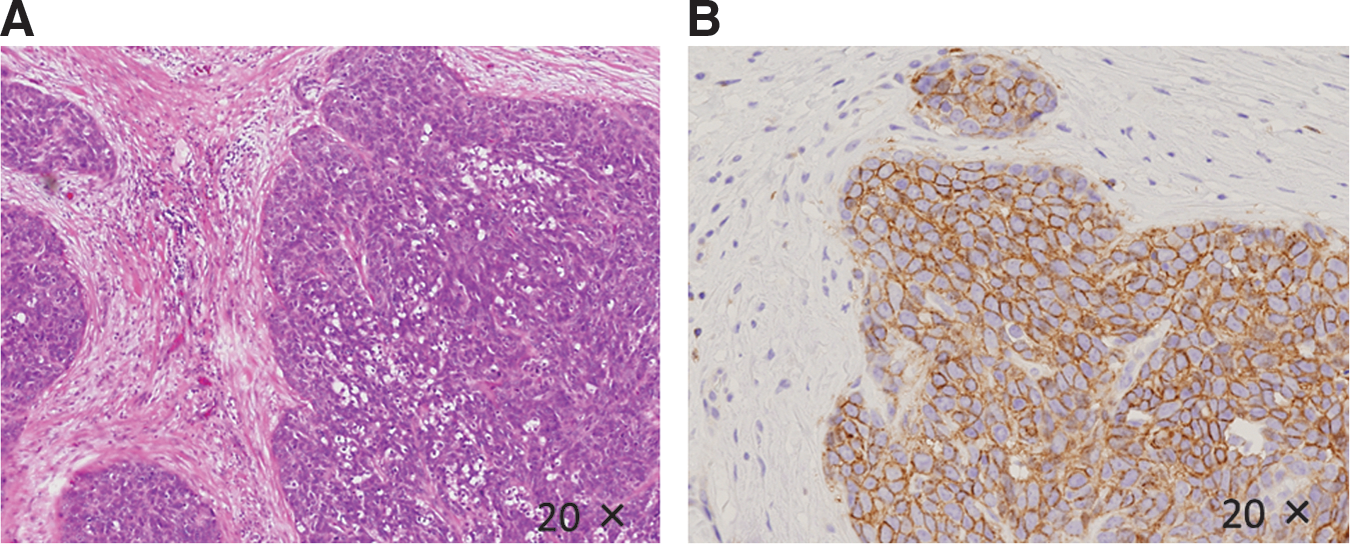
Microscopic findings. The tumor was composed of atypical cell nests separated by dense fibrous septa with many lymphocytes and plasma cell infiltration. The tumor cells were positively immunoreactive for CD5.
Thirteen months after resection, multiple nodules in both lungs were noted on whole body CT for postoperative follow-up, but there was no evidence of tumor recurrence in his neck or other organs (Fig. 2A). Physical examination and systemic review, including PET/CT, did not show any other abnormalities except pulmonary nodules. Therefore, a diagnosis of lung metastasis of CASTLE was made. The patient was initially treated with cisplatin (day 1; 50 mg/m2), doxorubicin (day 1; 40 mg/m2), vincristine (day 3; 0.6 mg/m2), and cyclophosphamide (day 4; 700 mg/m2) (ADOC) every 4 weeks. After four cycles of ADOC therapy, partial response was achieved (Fig. 2B). The most common adverse events, leukopenia/neutropenia and nonhematological toxicities, were mild. Twenty-three months after resection, the patient was without symptoms.
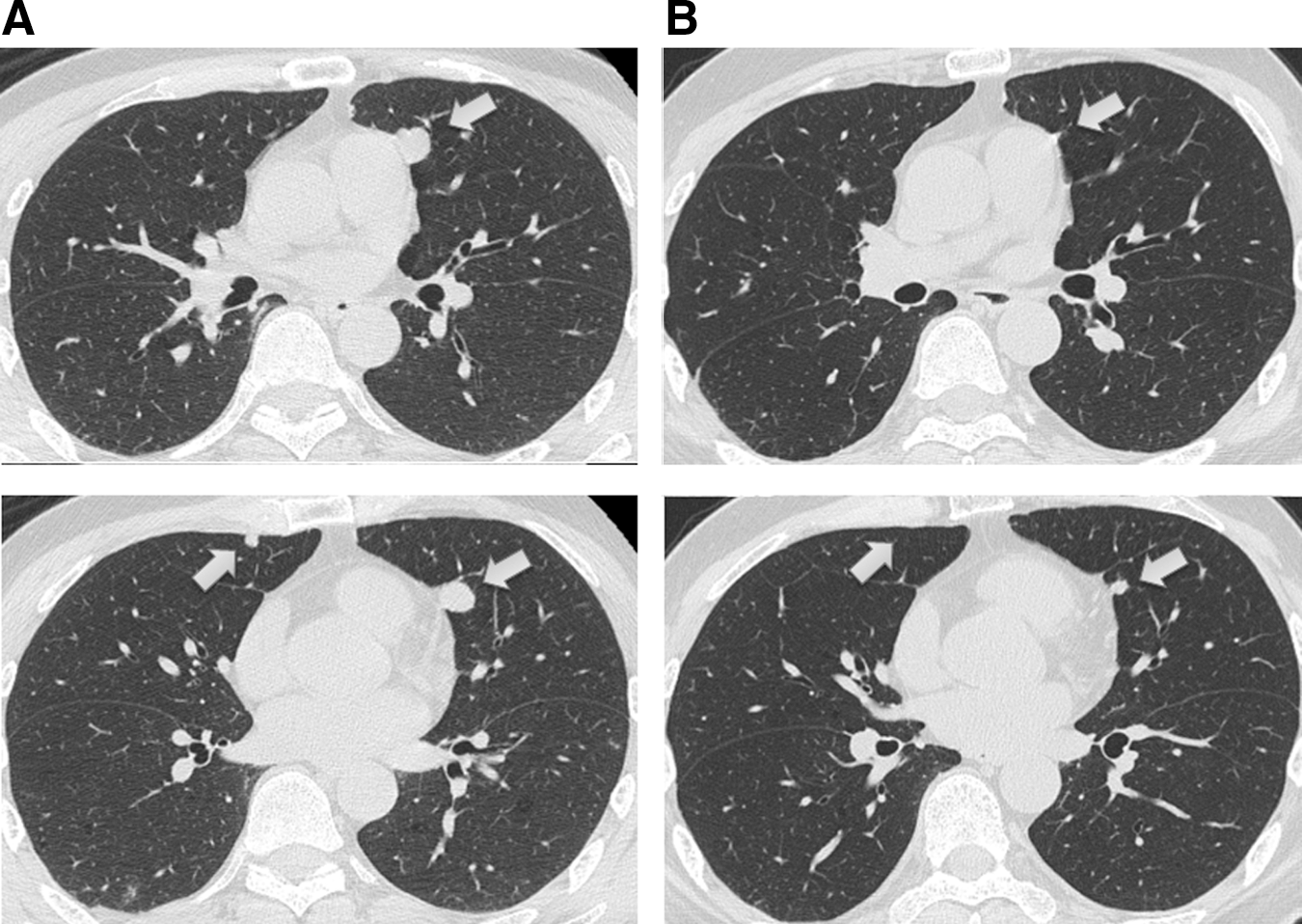
Computed tomography findings before
Nine months later, the disease relapsed on the same side in the lung and a new lesion was observed in the left interlobular space (Fig. 3A). Therefore, he was treated with combination chemotherapy consisting of carboplatin (CBDCA; AUC6) plus paclitaxel (180 mg/m2) every 3 weeks. Six cycles of CBDCA plus paclitaxel chemotherapy were performed and a partial response was achieved (Fig. 3B). Granulocyte colony stimulating factor was used as treatment for neutropenia in ADOC chemotherapy, but febrile neutropenia was not observed in either chemotherapy. Both chemotherapies were well tolerated, and there were no specific nonhematological toxicities over grade 3 as evaluated by the Community Toxicity Criteria of the National Cancer Institute (NCI-CTC) version 4.0.
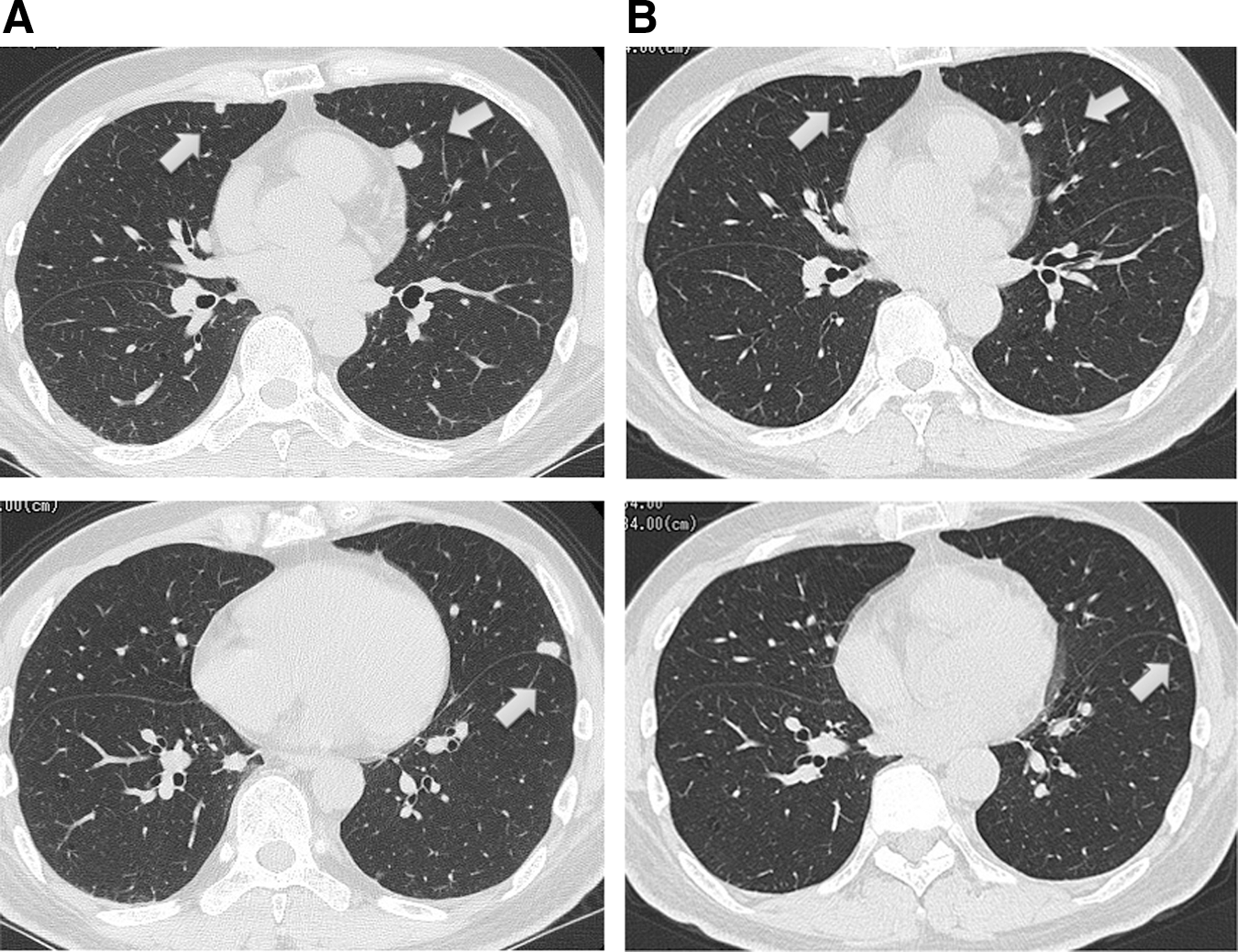
Computed tomography findings before
Discussion
CASTLE is an extremely rare malignant thyroid neoplasm, which occurs in middle-aged individuals at a mean age of 50 years. CASTLE accounts for 0.1%–0.15% of all thyroid cancers (6,9,10). Patients who undergo curative surgery have favorable outcomes. Thus, complete resection of the tumor, including resection of the infiltrated organs, is imperative (1,3,10). In addition, CASTLE has been reported to be radiosensitive and postoperative radiotherapy is considered for patients with positive nodal status (1,3,10).
Chemotherapy is commonly used in patients with unresectable and/or metastatic CASTLE (3 –8). However, because of the rarity of CASTLE, the data on the efficacy of adjuvant or palliative chemotherapy are anecdotal (3). Treatment regimens of first-line chemotherapy for metastatic or advanced disease reported previously are summarized in Table 1. Because tumor cells in CASTLE are thought to originate from ectopic thymic tissue, novel regimens for thymic malignancy have been attempted. Since agents used by concurrent chemoradiotherapy were included and no similar regimens were observed in these reports, the role of chemotherapy or a reliable treatment regimen has yet to be clarified. With regard to chemotherapy for advanced thymic carcinoma, we previously described the clinical responsiveness of advanced thymic carcinoma to ADOC as the first-line chemotherapy and reported overall response and disease control rates of 55.2% and 89.7%, respectively (13). Two prospective studies using CBDCA and paclitaxel as first-line chemotherapy for advanced thymic carcinoma were performed and showed response rates of 21.7% (14) and 36% (15), respectively. In addition, several case reports indicated that relapsed thymic carcinoma after ADOC chemotherapy responded well to salvage chemotherapy with CBDCA plus paclitaxel (16,17). These studies suggested that thymic carcinoma is a relatively chemosensitive tumor. There have been no previous studies regarding the biological association or homology between CASTLE and thymic carcinoma. Furthermore, as described above, little information is available regarding the efficacy of chemotherapy in patients with CASTLE. However, we would like to emphasize that the present experience regarding responses to two serial chemotherapies indicates that advanced and/or metastatic CASTLE should be treated with chemotherapy, specifically using a chemotherapeutic regimen designed for thymic carcinoma.
Died after the second cycle of chemotherapy.
Died from acute respiratory insufficiency the day after the first treatment.
Two cycles of chemotherapy, followed by radiotherapy, followed by three further cycles of chemotherapy using the same regimen.
CASTLE, carcinoma showing thymus-like differentiation; ACNU, nimustine hydrochloride.
In summary, we present a case of CASTLE with lung metastasis that showed a good response to two serial chemotherapies with platinum-containing regimens. To our knowledge, this is the first case of CASTLE reported to show a response to serial chemotherapies. Further clinical experience and studies are required to determine the usefulness of chemotherapy for metastatic CASTLE.
Footnotes
Author Disclosure Statement
No competing financial interests exist.