
Abstract

Total thyroidectomy, radioiodine therapy, and thyrotropin (TSH) suppression are the mainstay treatment of well-differentiated thyroid cancer (DTC). Treatment of metastatic DTC can include surgery when feasible, 131I therapy, and external beam radiotherapy. However, a few cases of metastatic carcinomas progress despite 131I treatment, and therapy with tyrosine-kinase inhibitors (TKI) has become an option. Sorafenib and lenvatinib have recently been approved by the Federal Drug Administration (FDA) for treatment of progressive radioiodine-refractory metastatic thyroid cancer.
Thyrotoxicosis is rarely associated with thyroid cancer, and most of these patients have concurrent Graves' disease. A few cases of triiodothyronine (T3) thyrotoxicosis in metastatic DTC have been described, and increased conversion of thyroxine (T4) to T3 associated with an increased activity of deiodinase type 1 (D1) and deiodinase type 2 (D2) has been demonstrated (1).
Two patients with metastatic follicular thyroid carcinoma (FTC) with T3 thyrotoxicosis are described in whom treatment with lenvatinib resulted in an unexpected control of T3 overproduction.
Patients
Patient 1
A 63-year-old female presented with progressive metastatic radioiodine-refractory FTC. For 10 years, she was on TSH suppression, receiving 125 μg/day of levothyroxine. In July 2009, she complained of palpitations. Thyroid function tests showed increased total T3 (TT3), low free T4 (fT4), and low TSH. To exclude T3 production by the tumor, levothyroxine was withdrawn for two weeks; TT3 and fT4 became undetectable, and TSH increased (Fig. 1A). The dose of levothyroxine was adjusted to 50 μg/day. As the disease progressed, she was initiated on sorafenib (November 2009) and remained stable for 23 months. During this period, the levothyroxine was adjusted to 100 μg/day. After sorafenib discontinuation, T3 thyrotoxicosis recurred, and the levothyroxine dose needed to be reduced to 50 μg/day.
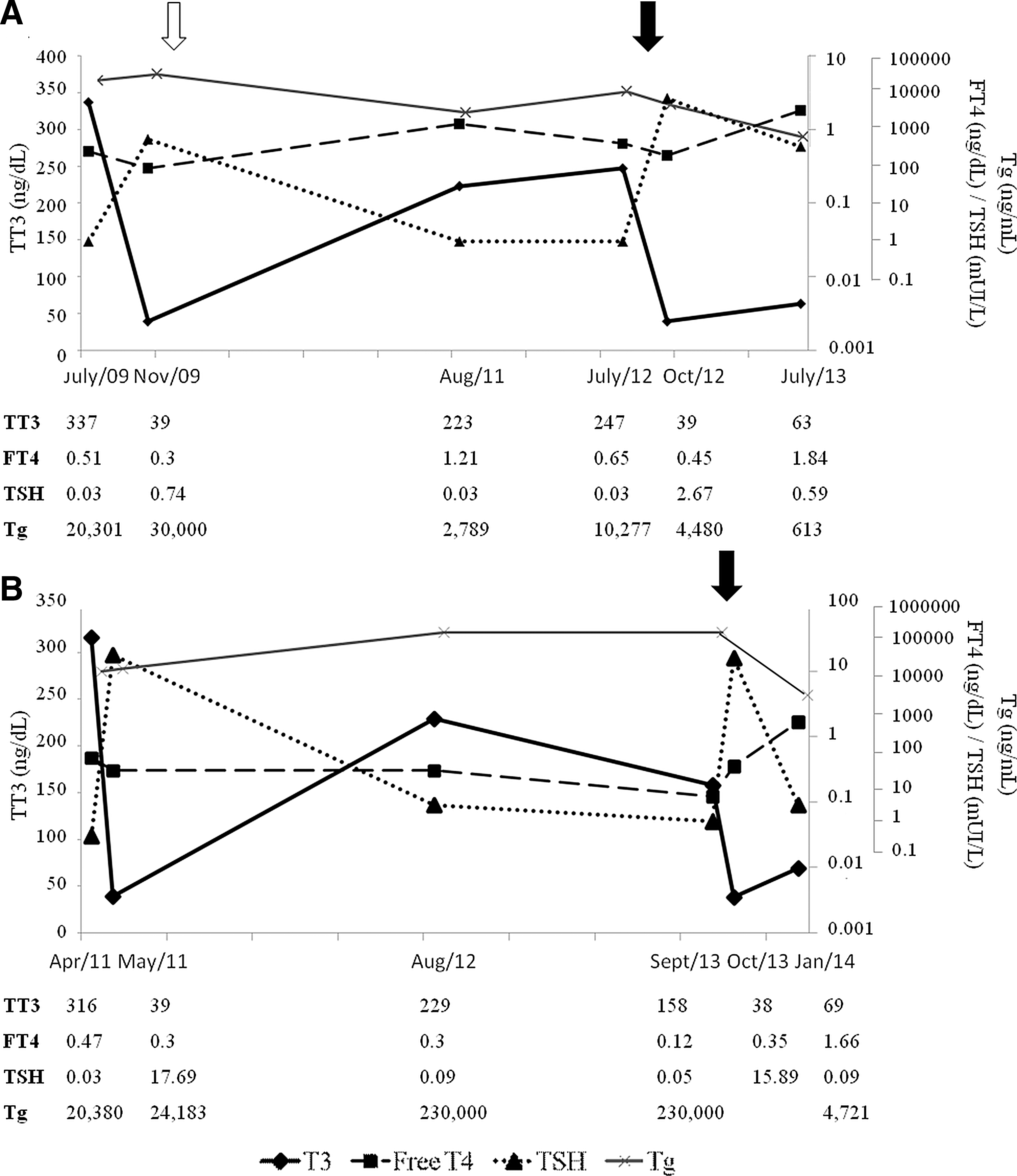
Thyroid hormone levels prior and after starting lenvatinib in (
In September 2012, she was included in a phase III clinical trial with lenvatinib (2). Within one month of treatment, the T3 abruptly fell, and the levothyroxine requirements increased to 200 μg/day in order to achieve TSH suppression (Fig. 1A). The patient had partial response to lenvatinib during 26 months of therapy.
Patient 2
A 74-year-old female also presented with progressive metastatic, radioiodine-refractory FTC. For three years, she received levothyroxine 125 μg/day for TSH suppression. In April 2011, she complained of palpitations, tremors, irritability, and weight loss. Thyroid function tests showed increased T3, low fT4, and low TSH levels. After levothyroxine withdrawal for four weeks, T3 and fT4 became undetectable, and TSH increased (Fig. 1B). The levothyroxine dose was reduced to 50 μg/day.
She was then included in a clinical trial with lenvatinib. Within one week of therapy (October 2013), she presented with acute symptomatic hypothyroidism (Fig. 1B). The levothyroxine was progressively increased to 175 μg/day. She remains on lenvatinib for 15 months with partial response.
Discussion
After thyroidectomy, thyrotoxicosis is usually iatrogenic and due to excessive doses of levothyroxine. Here, cases of T3 toxicosis related to metastatic FTC are described. At the onset of symptoms, the patients presented with elevated T3, low fT4, and suppressed TSH levels. The hypothesis of T3 tumor production was excluded, as both T3 and fT4 decreased after LT4 withdrawal, suggesting an increased conversion of T4 to T3 as a mechanism for the T3 toxicosis. In DTC, levothyroxine is usually employed to suppress TSH to suppressed or undetectable levels. Thyroxine is deiodinated at the 5′ position to generate T3, the active form of thyroid hormone, by the deiodinases D1 and D2 (3). Low D1 and D2 levels have been described in papillary thyroid carcinomas, a finding that contrasts with increased activities in metastases of FTC associated with T3 thyrotoxicosis (1).
Recently, TKIs have been employed in radioiodine-refractory metastatic thyroid cancer. Thyroid dysfunction is observed in euthyroid patients receiving TKI for other malignancies. Potential mechanisms involved include destructive thyroiditis, impaired iodine uptake, inhibition of thyroperoxidase activity, induction of type 3 deiodinase (D3) activity, and capillary regression within the thyroid (4). In this report, T3 thyrotoxicosis developed while patients were on standard levothyroxine doses. Upon initiation of therapy with lenvatinib, both patients developed hypothyroidism after a short period of time—one month and one week, respectively. Although tumor regression cannot be discarded as responsible mechanism for the observed hormonal changes, the rapid onset of hypothyroidism, even before documented tumor reduction, and an increased levothyroxine requirement that exceeded during the period with T3 toxicosis suggests the possibility of an inhibition of D1 and D2 by lenvatinib. Altered activity of deiodinases has already been observed with another multikinase inhibitor (4). In ex vivo experiments, sunitinib induced D3 and decreased D1 activity; both changes reverted after drug discontinuation (4). The decrease in deiodinase activity does not seem to be limited to lenvatinib, as a similar but discrete effect was observed while patient 1 was on sorafenib.
In conclusion, two patients with radioiodine-refractory metastatic FTC and T3 toxicosis are described in whom lenvatinib resulted in a significant reduction of thyroid hormone levels requiring a significant increase in levothyroxine supplementation. The mechanism of lenvatinib-induced hypothyroidism is unclear. However, it is hypothesized that it involves a decrease in D1 and/or D2 activity. Careful monitoring of thyroid hormone levels is indicated in patients receiving lenvantinib for the therapy of thyroid cancer in order to assure adequate TSH suppression.
Footnotes
Author Disclosure Statement
D.L.S.D., G.C., and A.O.H. received research support from Eisai. A.O.F. is a consultant for Eisai. R.Y.A.C., C.P., and S.M. have nothing to declare.