
Abstract
Background:
Sunitinib is a tyrosine kinase inhibitor (TKI) inducing thyroid dysfunction, but the precise mechanism(s) involved remains to be explained, including the role of thyroid autoimmunity. The objective of this study was to evaluate thyroid function, parameters of autoimmunity, and thyroid ultrasound findings in patients with metastatic cancer and normal thyroid function/autoimmunity before the initiation of sunitinib therapy. This was a prospective, observational cohort study.
Methods:
Twenty-seven patients with metastatic carcinomas at comparable tumor stages were evaluated over 12–18 months after initiating therapy with sunitinib given at a daily oral dose of 50 mg for four weeks (ON), followed by one to two weeks off therapy (OFF). Serum thyrotropin (TSH), free thyroxine (fT4), free triiodothyronine (fT3), and antithyroglobulin (TgAb), and antithyroid peroxidase (TPOAb) autoantibodies were measured in all cases. Thyroid morphology and volume were evaluated by echo-color Doppler ultrasound.
Results:
A total of 16/27 patients (60%) became hypothyroid (TSH range 7–114 mIU/L) within 30–120 days of therapy. The thyroid volume decreased in 24/27 (89%) patients (from M = 14.6 mL, SD = 6.4 mL to M = 3.8 mL, SD = 2.6 mL after 12 months; p < 0.001), together with the appearance of mild to severe hypoechogenicity. TPOAb (40–3000 IU/mL) became detectable in 7/27 (25%) patients, and TPOAb-positive patients displayed a higher degree of hypothyroidism and volume reduction. The progression-free survival (PFS) was significantly longer in patients developing TPOAb (10.8 months) than in the other group of patients (5.8 months).
Conclusions:
These data confirm the thyroid inhibitory effect of sunitinib, in keeping with the key role of kinases in controlling thyroid function and growth. However, the novel appearance of TPOAb in a subgroup of patients with more severe hypothyroidism and longer survival indicates that sunitinib may also trigger/exacerbate thyroid autoimmunity contributing to thyroid failure. The development of TPOAb was associated with a longer PFS.
Introduction
S
In particular, the role of thyroid autoimmunity in the pathogenesis of TKI is controversial. While thyroid autoimmunity was found to be absent in some prospective series (2,10) of sunitinib-treated patients, the presence of lymphocytic thyroiditis has been documented even at the histological level in an isolated case report of sunitinib-induced hypothyroidism (11).
The aim of the present investigation was therefore to evaluate thyroid function and thyroid autoimmunity longitudinally before and during sunitinib administration in a homogenous series of patients with metastatic carcinomas, with normal thyroid function and negative thyroid antibodies before starting sunitinib therapy.
Patients and Methods
Patients
A total of 27 consecutive patients (24 male) aged 44–77 years old (M = 59.9 years, SD = 7.6 years) with metastatic carcinomas (26 with mRCC and 1 with gastrointestinal stromal tumor [GIST]) currently treated at the Medical Oncology Unit of Cagliari University and Businco Hospitals were enrolled in the study. All patients were at an advanced tumor stage with the following distribution of distant metastases: 20/27 (74%) lung, 4/27 (14%) bone, and 3/27 (11%) liver, adrenal, and pancreas metastases. Thyroid evaluation was performed at the outpatient clinic of the Endocrinology Unit of Cagliari University Hospital.
All patients were euthyroid with no serological and/or ultrasound evidence of associated thyroid autoimmunity and a negative familial history of thyroid disease. All patients were initially treated with sunitinib (Sutent®) for 2–18 months (M = 8.3 months, SD = 3.9 months). Sunitinib was given at a daily oral dose of 50 mg for four weeks (ON), followed by one to two weeks (OFF) on the basis of the clinical condition. Sunitinib was withdrawn in three patients after three to five months due to progression of the disease and replaced by axitinib (Inlyta®) given at a daily oral dose of 10 mg.
Tumor measurements were evaluated by the treating oncologist according to the Response Evaluation Criteria in Solid Tumors (RECIST) (12). Computed tomography scans were performed every 16 weeks during treatment with sunitinib, and every 12 weeks during treatment with axitinib.
All patients signed an informed consent, and the study was approved by the Institutional Ethics Committee.
Biochemical and instrumental investigations
Blood samples were collected before and at the end of the “ON” and “OFF” periods during the sunitinib administration.
Thyrotropin (TSH; reference range 0.3–3.0 mIU/L), free triiodothyronine (fT3; 1.8–4.2 pg/mL), free thyroxine (fT4; 0.9–1.9 ng/dL), and antithyroglobulin (TgAb; 0–20 IU/mL) and antithyroid peroxidase (TPOAb; 0–35 IU/mL) autoantibodies were measured by an ultrasensitive chemiluminescent assay (Immulite 2000; Siemens). All patients underwent a careful clinical examination, followed by thyroid ultrasound using echo color Doppler technique, always performed by the same operator (F.P.) and with the same instrument (Sonoline G60S; Siemens Medical Solutions). In all cases, the estimated thyroid volume (ETV) was evaluated using the formula of the ellipsoid of rotation (depth × width × length × 0.52) (13). The parenchymal echogenicity and the presence of thyroid nodules were always assessed.
Statistical analysis
Parametric (Student's t-test) and nonparametric (Mann–Whitney U-test) tests were used to compare different groups. The hazard ratio (HR) and confidence interval (CI) were estimated by stratified Cox proportional hazards regression. Statistical significance was considered at p < 0.05. All calculations were performed using GraphPad Prism®.
Results
Patient characteristics
Sex, age, and basal and follow-up data on thyroid function and volume and status at the end of the study of all patients are reported in Table 1. Before sunitinib administration, all patients had normal TSH levels, and TgAb and TPOAb were within the reference range (<20 IU/mL and <35 IU/mL, respectively). With the exception of the single patient with GIST who was treated for five months with imatinib until three months before inclusion in the present study, none of the patients received any antineoplastic drug before the treatment with sunitinib. The median duration of treatment with sunitinib was 64 weeks (range 8–78 weeks).
In patients developing hypothyroidism, the first value represents the highest TSH concentration observed before the beginning of LT4 therapy, and the second value is the last measurement available. In the other patients, the value represents the last TSH measurement available.
The first value represent the basal volume, the second value the last measure available.
Shifted to axitinib.
TPOAb, antithyroid peroxidase autoantibody; TSH, thyrotropin; ETV, estimated thyroid volume; I, improved; N, no change; W, worsened; D, died; LT4, levothyroxine.
Thyroid function during sunitinib administration
As shown in Table 1, 16/27 patients (60%) developed variable degrees of hypothyroidism (TSH 7–114 mIU/L) after 30–120 days of treatment. Two patients displayed a transient period with suppressed TSH, presumably due to mild thyrotoxicosis secondary to a destructive thyroiditis (TSH <0.01 mIU/L), and one of them later developed thyroid failure (TSH 9.5 mIU/L). Hypothyroid symptoms were mostly mild, with the exception of the patient with a serum TSH of 114 mIU/L. During the first three months of sunitinib therapy, an increased serum TSH concentration was observed in all patients developing hypothyroidism only during the “ON” period, but subsequently TSH remained abnormally elevated even during the “OFF” period. Serum fT4 displayed a trend to decreasing levels without reaching statistical significance (data not shown). Levothyroxine (LT4) therapy (25–75 μg) was started in all patients showing a persistent serum TSH elevation of ≥7 mIU/L at the end of the “OFF” period and was followed by a stable normalization of the serum TSH on therapy. The mean serum TSH concentration observed at the last evaluation before starting LT4 (M = 14.5 mIU/L, SD = 24.6 mIU/L; range 7–114 mIU/L) was significantly higher than basal levels (M = 1.2 mIU/L, SD = 0.6 mIU/L, p < 0.001 by paired Student's t-test). This difference remained significant even after excluding the highest TSH concentration of 114 mIU/L (M = 17.2 mIU/L, SD = 9.7 mIU/mL; range 7–30 mIU/L; p < 0.01).
Antithyroid antibodies and thyroid function during sunitinib administration
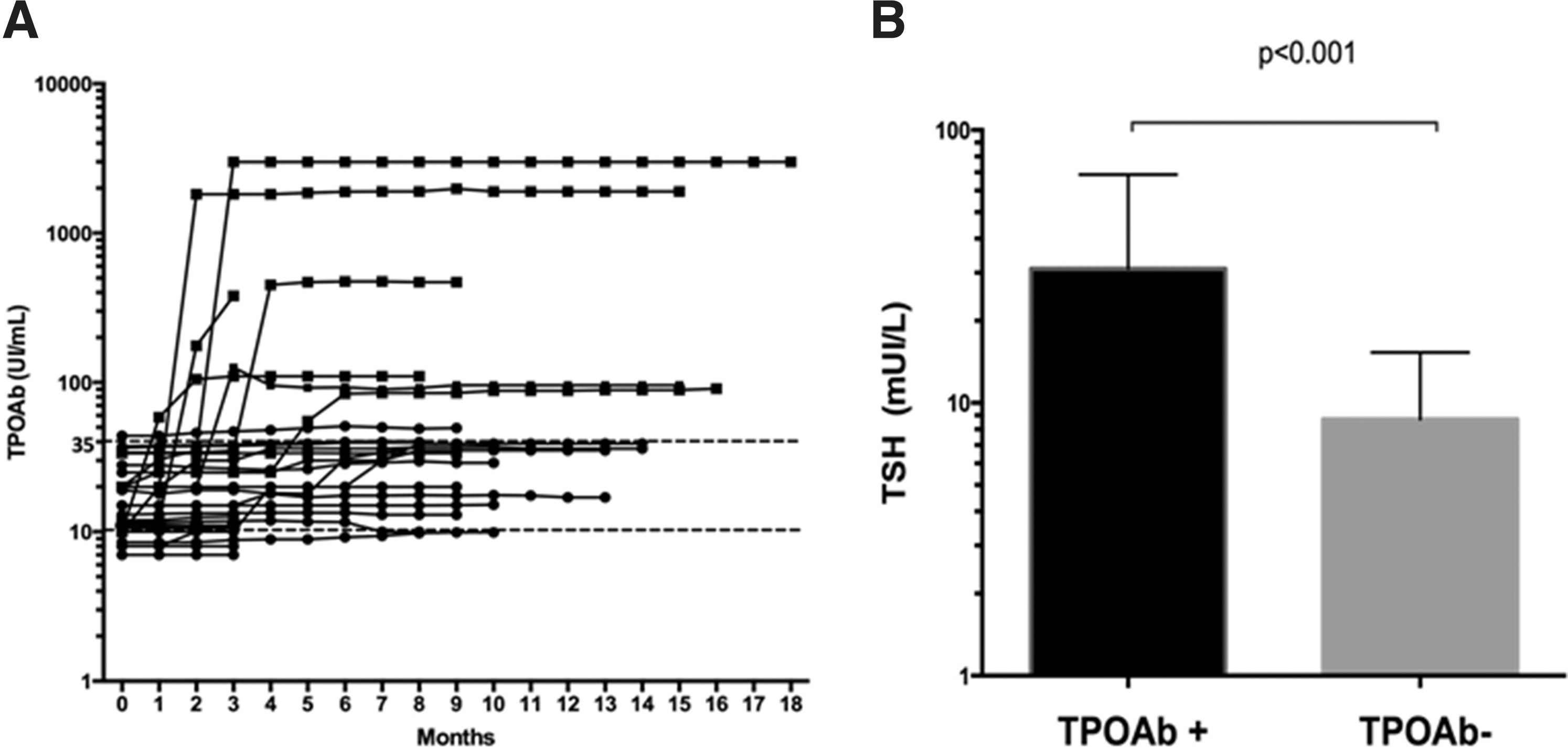
Although both TgAb and TPOAb were within the reference range (<20 IU/mL and <35 IU/mL, respectively) at baseline before starting therapy with sunitinib, seven (26%) patients developed mildly to significantly elevated titers of TPOAb (40–3000 IU/mL), and they remained elevated after initiating LT4 replacement therapy (Fig. 1A).
(
In contrast with TPOAb, TgAb did not increase above the reference range during all cycles of treatment (data not shown).
As shown in Figure 1B, the mean of the maximal serum TSH elevation observed during sunitinib treatment before LT4 therapy was significantly higher (M = 40.1 mIU/L, SD = 18.8 mIU/L) in the seven patients developing TPOAb than in the 20 patients who remained TPOAb negative (M = 8.7 mIU/L, SD = 1.8 mIU/L; p < 0.001 by unpaired Student's t-test). This difference remained significant (M = 17.2 mIU/L, SD = 9.7 mIU/L; p < 0.01 by unpaired Student's t-test) after excluding the highest value (114 IU/mL) observed in patient 8.
Antithyroid antibodies and tumor response
As shown in Figure 2, the median duration of treatment in the seven patients developing high TPOAb was longer (15 months; range 3–18 months) than that observed in the 20 patients in whom TPOAb did not increase (9 months; range 2–14 months). The progression-free survival (PFS) of TPOAb-positive patients (10.8 months) was significantly higher than that of TPOAb-negative patients (5.8 months [CI 0.45–0.76], HR for PFS of 0.59; p < 0.001 by Cox regression analyses).

Kaplan–Meier estimate of survival probability in seven patients who developed TPOAb (■) and in 20 patients who remained TPOAb negative (●) during sunitinib therapy.
Echo-color Doppler ultrasonography evaluation
At baseline, all patients showed a normal ETV with normal echogenicity, although three of them (patients 1, 7, and 15 in Table 1) displayed one or more thyroid nodules ranging from 16 to 22 mm in maximal diameter. The nodule observed in patient 1 was not suspicious, and its benign nature was confirmed by fine-needle aspiration cytology (FNAC). In contrast, the nodules observed in patients 7 and 15 displayed some suspicious features, but the patients refused FNAC.
The individual variations of the ETV in all series are reported in Figure 3. The reduction of ETV was clearly higher in TPOAb-positive compared with TPOAb-negative patients. Although this phenomenon could be partially due to the longer duration of sunitinib administration in TPOAb-positive patients, the mean ETV observed after four months of therapy was already significantly lower (M = 2.1 mL, SD = 1.3 mL) than the mean ETV observed in TPOAb-negative patients (M = 6.8 mL, SD = 3.4 mL; p < 0.001 by unpaired Student's t-test). The decrease in the ETV was much more evident in TPOAb-positive patients both in the “ON” and in the “OFF” phase of sunitinib therapy (data not shown).
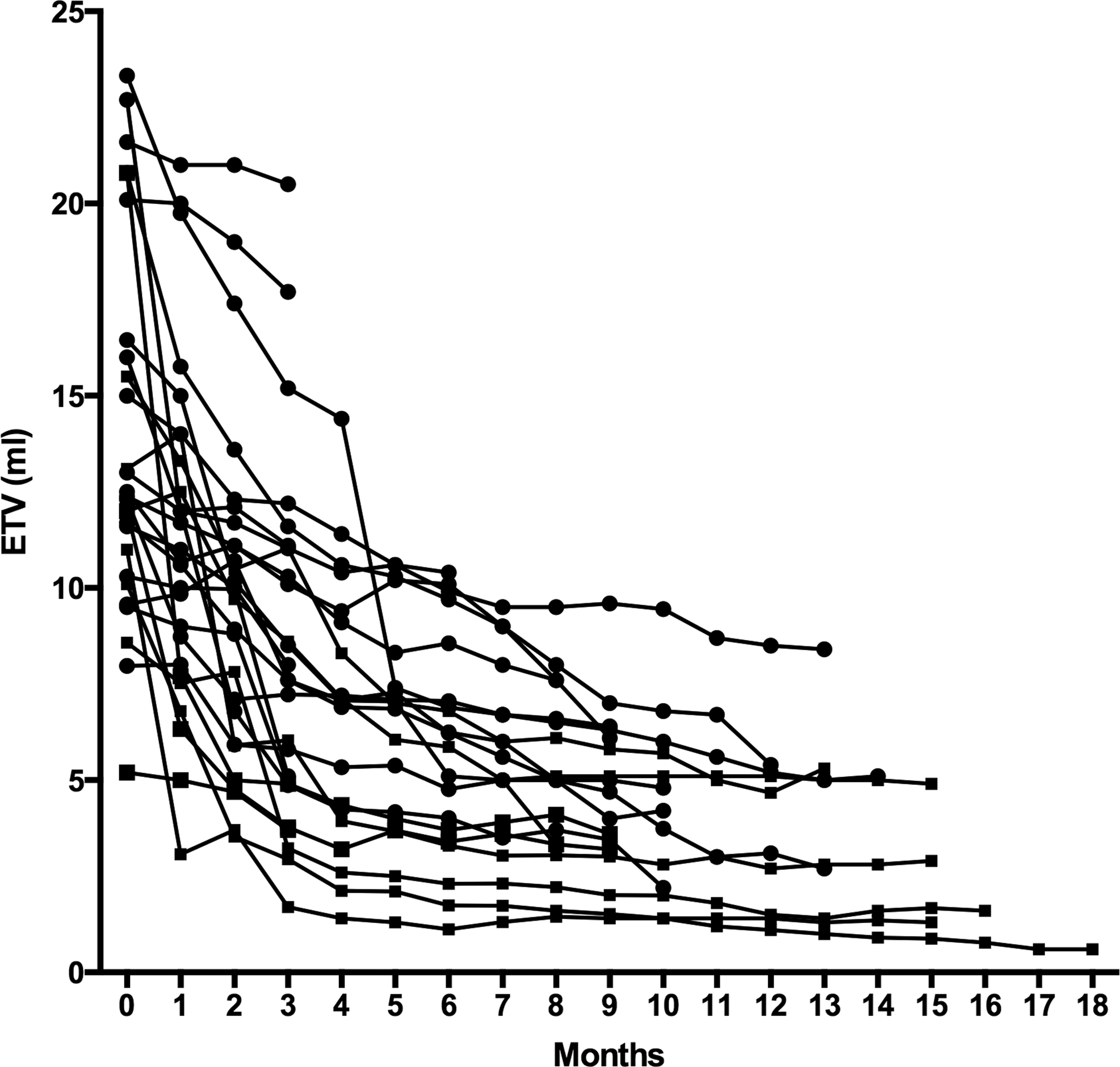
Individual values of estimated thyroid volume (ETV) in 27 patients with metastatic cancer before (basal) and during 1–18 months of sunitinib treatment. Filled circles (●) indicate TPOAb-negative patients, and squares (■) indicate TPOAb-positive patients.
Besides a reduction in the ETV, sunitinib treatment was associated with a change in parenchymal ultrasound features and vascularization (Fig. 4A and B). As shown in Figure 4A and B, a marked hypoechogenicity was observed compared with basal findings, and this decrease in the echogenicity was more evident in TPOAb-positive patients (Fig. 4B). As far as vascularization is concerned, there was a trend to a reduced parenchymal perfusion, which did not reach the level of statistical significance.
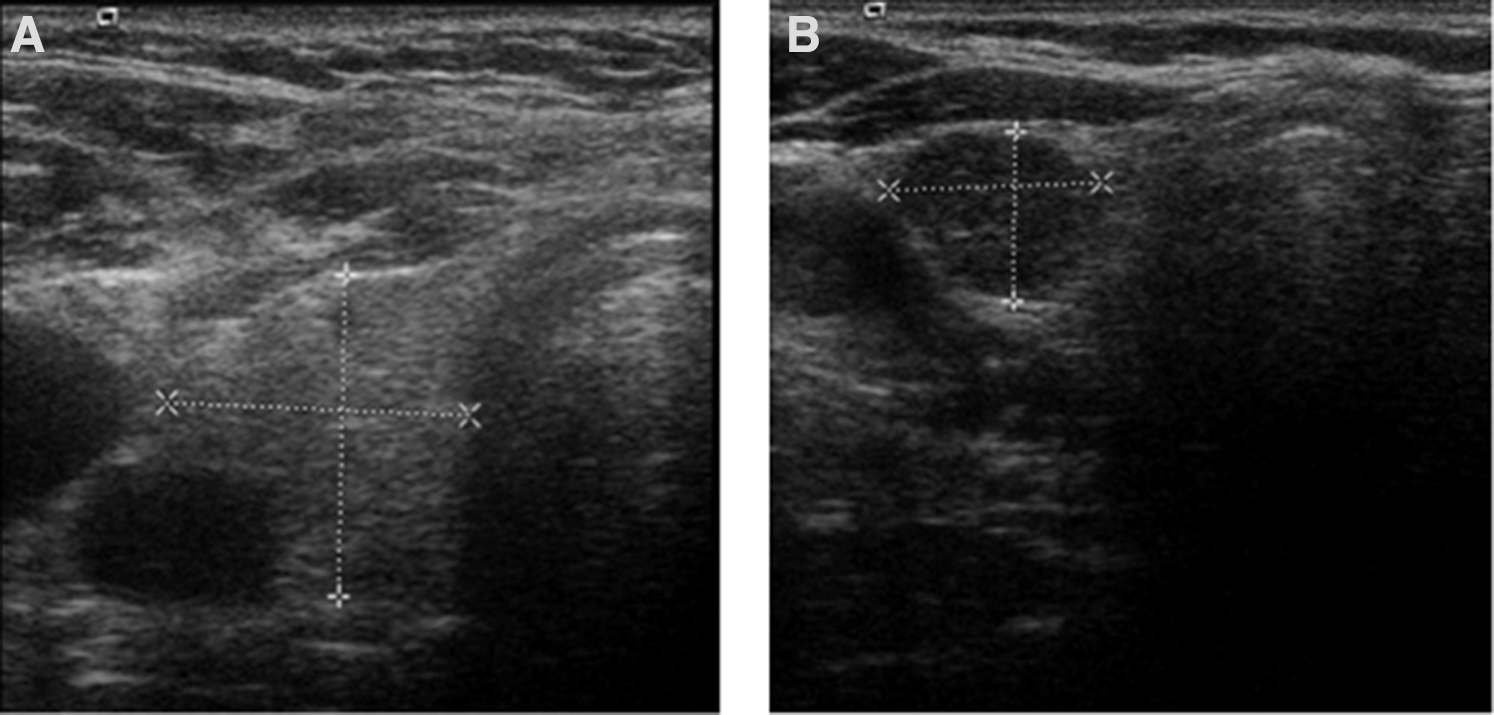
Selected thyroid ultrasound images from sunitinib-treated patients with metastatic cancer. (
Interestingly, in three patients presenting with thyroid nodules, sunitinib treatment was associated with a marked size reduction of the nodular lesions.
Discussion
This study prospectively analyzed thyroid function, thyroid autoantibodies, and thyroid ultrasound findings in patients with metastatic cancer during sunitinib treatment. The high prevalence of mild to severe hypothyroidism (60%) was consistent with previous reports (14,15). This study provides several additional insights on sunitinib-associated thyroid dysfunction, which have not been systematically reported before.
Although VEGF inhibition is considered the main mechanism common to all TKIs that cause hypothyroidism (16), it is still unclear whether other effects might be responsible for sunitinib-induced thyroid dysfunction. Although most of these effects remain hypothetical, it is worth noting that sunitinib-induced thyroid dysfunction has been attributed to inhibition of iodine uptake (10), reduced synthesis of thyroid hormone (17), influence on deiodinase activity (18), impairment of MCT8-mediated iodothyronine transport (19), destructive thyroiditis (3), impaired blood flow (20,21) and damage by autoimmune processes (11). Few studies have been carried out so far focusing on a potential role of sunitinib in modulating thyroid autoimmunity and function. Wolter et al. (8) found positive TPOAb and TgAb in 2/49 patients prospectively evaluated for thyroid dysfunction on sunitinib therapy, but thyroid antibody tests were performed only at baseline. A higher prevalence of TgAb (but not TPOAb) was found by Rini et al. (22) in 13/44 (30%) patients prospectively evaluated for thyroid dysfunction while on sunitinib therapy. Of those, eight patients were TgAb positive at baseline, and five patients developed detectable TgAb after sunitinib therapy, but no correlation was found between the presence of TgAb and either the incidence or the severity of thyroid dysfunction. In a single study (10), where antithyroid antibodies were assessed in 24 patients both at baseline and during six sunitinib cycles, TgAb and TPOAb remained undetectable in all but one patient, who had mild hypothyroidism and positive TPOAb before starting sunitinib therapy. Thus, recent reviews on the effect of TKI on thyroid function concluded that, in contrast with IL-2 and interferon-alpha (IFN-α), thyroid autoimmunity cannot be included as an etiological factor in TKI-induced hypothyroidism (10,16), although histological evidence of sunitinib-associated lymphocytic thyroiditis was obtained in a single case of an euthyroid patient with negative serum antithyroid antibodies (11).
In contrast with the above findings, the data obtained in the present study provide strong evidence that thyroid autoimmunity may contribute to sunitinib-induced thyroid dysfunction in at least 25% of patients. This conclusion arises from the following considerations: (i) the novel appearance of persistent serum TPOAb in patients without any clinical, serological, or ultrasound features suggestive of thyroid autoimmunity, including familial history prior to therapy; (ii) a higher degree of hypothyroidism; and (iii) a more pronounced decrease in thyroid volume in TPOAb-positive when compared with TPOAb-negative patients.
The reasons for the apparent discrepancy between the previous reports and the present study on a possible autoimmune contribution in the etiology of sunitinib-induced thyroid dysfunction are not immediately clear. However, it should be noted that thyroid autoimmunity was systematically assessed only in one study (10), which had a shorter duration (six sunitinib cycles) when compared with the present investigation, which was extended up to 18 cycles. Other still unknown factors such as differences in the genetic background of the populations studied may also be involved in this context, for example the known increased susceptibility of the Sardinian population to developing autoimmune diseases (23 –25).
The appearance of sunitinib-induced thyroid autoimmunity was apparently related to a better outcome. However, since patients developing TPOAb also developed more severe hypothyroidism, the improved survival of TPOAb-positive patients could simply be related to thyroid failure, as already suggested in previous reports (26 –28). Thus, whether and to what extent thyroid autoimmunity might be the expression of a widespread activation of the immune system contributing to the control of tumor growth remains a matter of future investigation.
Another difference of the present study is the availability of longitudinal thyroid ultrasound evaluation. While this confirmed previous studies showing a reduction of thyroid volume and nodules (29,30), it also allowed the time course of this effect to be characterized better, showing that a significant reduction of thyroid volume was already observed in the early phase of treatment, when it was partially dependent from the ON or OFF phase of sunitinib administration, and that it reached its maximal effect after four to six months of therapy. The reduction of thyroid volume was associated to a reduction of thyroid echogenicity, which was more evident in TPOAb-positive patients, providing further support for the involvement of thyroid autoimmunity in sunitinib-induced thyroid damage.
The longitudinal ultrasound follow-up also allowed evaluation of thyroid vascularization during sunitinib therapy. Although a trend toward reduction in vascularity was found, the difference did not reach statistical significance. This finding contrasts with the marked anti-angiogenetic effect of TKI, which is considered one of the most important factors involved in sunitinib-induced hypothyroidism. This paradox could be possibly explained by considering the stimulating effect of increased TSH on thyroid vascularization, which may compensate the drug-induced effect (31). This study also allowed a precise characterization of the effect of Sunitinib on the volume reduction of thyroid nodules. Although the lack of cytological data on two of three patients with nodules is a limitation because they refused FNAC, the complete disappearance of all nodules within four to nine months of sunitinib therapy represents a remarkable finding, which deserves further investigation.
In conclusion, the data of the present study confirm and extend our knowledge on the thyroid-inhibitory effects of sunitinib. Besides the functional inhibition expected on the basis of the key role of kinases in thyroid function and growth, the novel appearance of antithyroid antibodies in one third of patients with more severe hypothyroidism and a higher degree of thyroid volume reduction indicates that sunitinib is able to trigger/exacerbate thyroid autoimmunity, which, in turn, may contribute to thyroid damage and could play a role as a potential biomarker of response.
Footnotes
Acknowledgment
This work was partially supported by funds of the University of Cagliari (Contributo di Ateneo alla Ricerca) to S.M.
Author Disclosure Statement
The authors have nothing to disclose.