
Abstract
Background:
Renal function is related to thyroid hormonal status, and glomerular filtration rate (GFR) seems to be impaired in patients with hypothyroidism. The aim of this work was to evaluate quantitatively the effect of hypothyroidism on GFR using a 51Cr-EDTA radioisotope assay.
Methods:
Twenty-eight patients without known renal disease or dysfunction who had been referred for radioiodine therapy (RIT) after total thyroidectomy were enrolled in this study and divided into two groups. Group A underwent thyroid hormone withdrawal (THW) resulting in hypothyroidism, while group B underwent recombinant human thyrotropin (rhTSH) stimulation and hence remained euthyroid. GFR was assessed by 51Cr-EDTA before and after THW or rhTSH.
Results:
No clinical differences were observed between the two groups. The mean ± SD GFRs were 94 ± 19 mL/min/1.73 m2 before THW and 76 ± 16 mL/min/1.73 m2 after THW for group A (p = 0.009), and 91 ± 18 mL/min/1.73 m2 before rhTSH and 93 ± 15 mL/min/1.73 m2 after rhTSH for group B (p = 0.613). The percent decrease in GFR during hypothyroidism is approximately 18–22%.
Conclusion:
GFR decreases in patients with normal kidney function during THW for RIT, and rhTSH preserves GFR in these patients. This GFR impairment following thyroidectomy is related to hypothyroidism due to a significant reduction in thyroid hormone levels and is not due to a rise in the TSH level.
Introduction
I
Radioiodine therapy (RIT) has been used in patients with thyroid carcinoma since 1946 as an adjuvant therapy after total thyroidectomy (11,12). To stimulate radioiodine uptake, a thyrotropin (TSH) elevation can be obtained through thyroid hormone withdrawal (THW) resulting in hypothyroidism or the injection of recombinant human thyrotropin (rhTSH), which leaves the patient in a euthyroid state (13 –15). Therefore, patients who are candidates for RIT can be used as a model to evaluate the effect of hypothyroidism on GFR and to improve the method of quantification of GFR.
The aim of this work was to use 51Cr-EDTA to compare GFR in patients referred for RIT with hypothyroidism induced by TWH to euthyroid patients treated with rhTSH in preparation of RIT.
Materials and Methods
Study design
Twenty-eight differentiated thyroid carcinoma (DTC) patients were prospectively enrolled in this study from November 2011 to January 2014, and all of them had been referred for RIT after total or near total thyroidectomy. All patients were already receiving substitutive thyroid hormone therapy and had never previously undergone RIT. The inclusion criterion for RIT ablation was a resected thyroid tumor >1 cm in diameter with or without extrathyroidal extension and with or without positive central neck lymph nodes. The exclusion criteria were pregnancy, lactation, younger than 18 years of age, the presence of any known renal disease, and known distant metastasis. Patients who were already in a hypothyroid state prior to the beginning of TSH stimulation were not enrolled, as the study aimed to estimate and quantify the effects of TSH elevation associated with (THW) or without (rhTSH) hypothyroidism. This exclusion criterion was included to avoid interference of pre-existing hypothyroidism on the final results, as prior hypothyroidism could result in a lower GFR.
An a priori sample size calculation was performed based on a 15% variation of GFR in THW and a 0% variation of GFR in rhTSH, with sigma values of 15% for both groups and with a type I error of 5% and a statistical power >90%. Interim analyses were conducted during patient recruitment, and if the type I error was <1% and the statistical power was >95%, recruitment was terminated.
Patients were divided randomly in two distinctive groups of 14 patients using the simple randomization method (16). Group A (GA) included patients stimulated by THW, while group B (GB) included patients stimulated by rhTSH. All patients were euthyroid before stimulation, and after stimulation, the GA patients were hypothyroid and the GB patients were still euthyroid. All patients underwent measurement of 51Cr-EDTA GFR, as well as measurements of the serum levels of free thyroxine, TSH, thyroglobulin (Tg), Tg antibodies (anti-Tg), urea, creatinine, and albumin before and after TSH stimulation, with an expected interval of four weeks between these two measurement time points. Neither the patients nor the physicians were blinded to the randomization. Serum levels of creatinine, urea, and albumin were entered into the modified MDRD (17) formula to calculate GFR, and the results were compared with those of the 51Cr-EDTA assay. The modified MDRD equation was used to calculate GFR at two days after RIT and at 7–10 days after RIT, when the patients returned to undergo a whole body image scan (WBS). 51Cr-EDTA was not performed at these later time points due to the possibility of radioactive interference as a consequence of the high level of radioiodine in the patient's circulation.
Sex, age, height, weight, systolic and diastolic blood pressure (SBP and DBP), heart rate (HR), tumor size, lymph node involvement, and comorbidities, such as arterial hypertension and diabetes, were also assessed. Informed consent was obtained from each patient, and the institution's ethical committee approved the study.
Radioiodine treatment procedures
Before RIT, all patients were submitted to low-iodine dietary restrictions for 15 days, and were instructed to avoid external iodine contamination for at least four weeks. No patients underwent iodine contrast-enhanced computed tomography scans within three months prior to RIT.
Patients in GA underwent a four-week THW for TSH stimulation, and their TSH serum levels were measured during the week before RIT. A minimum TSH serum level of 30 μIU/mL was considered necessary prior to RIT, and if the level was below this cutoff value, THW was extended by one week. As variances in the THW period between patients could occur due to hospital bed availability, the THW periods were recorded in days and are reported in the Results section.
Patients in GB received 0.9 mg intramuscular injections of rhTSH (Thyrogen, Genzyme) on two consecutive days before RIT, and radioiodine was orally administered on the third day after the first injection. For patients in GB, the TSH serum level was measured on the day of iodine dose administration (third day).
All 28 patients received 5550 MBq (150 mCi) 131I-labeled sodium iodine (131I-NaI) in a single capsule (IPEN) for RIT ablation based on the institutional protocol (18). All RITs were performed in special shielded rooms that were appropriate for the administration of nonsealed radioactive sources, and all patients were discharged once an external radiation exposure rate equal to that of a 1110 MBq (30 mCi) 131I source was achieved in compliance with the local radiation regulatory authority. To exclude pregnant patients from the study, beta human chorionic gonadotropin level was measured in all fertile female patients prior to RIT.
GFR measurement procedures
After a fasting period of at least three hours, the patients were given approximately 300 mL of water one hour prior to the procedure, and their heights and weights were measured. For each procedure, two syringes containing 3.7 MBq (0.1 mCi) 51Cr-EDTA (IPEN) in a volume of at least 1 mL were obtained and weighed on an analytical balance (Quimis Q500L210C). The content of the first syringe was injected into a volumetric balloon containing 1000 mL of distilled water for the standard control, and the content of the second syringe was injected in the patient followed by a 10 mL saline flush. After injection, both syringes were again weighed on the analytical balance, and the difference between each syringe was considered the 51Cr-EDTA injected mass. This weighing method was used because the analytical balance provides better precision than a dose calibrator (19). The injection site was monitored for radioactive counts with a pancake surface (IEN SPQ-7026) monitoring Geiger–Müller probe (IEN MIR-7026) to guarantee that no extravasation of the radiopharmaceutical occurred during the injection. Blood samples were collected in heparinized tubes at two and four hours after the injection in the contralateral arm of the 51Cr-EDTA administration. The blood samples were centrifuged (Quimis Q222T) at 1000 g for 10 min, and 2 mL aliquots containing only plasma were pipetted. The radiation in the samples was subsequently counted for five minutes in a radiation well countercentered at the chromium-51 photopeak of 320 keV. Background radiation was also counted for five minutes before counting the radiation in the samples and was subtracted from the count for each sample. Countings were used to plot curves using the slope-intercept method with the single compartment model and were corrected by Brochner–Mortensen's method and body surface area (20). This method was previously confirmed as having similar validity to that of the inulin clearance test (10).
Statistical analysis
A descriptive statistical analysis was performed for the clinical parameters. For Tg and anti-Tg, median values were obtained instead of mean values because certain patients presented with values that were quite different from the majority of patients in their study group. A comparative statistical analysis was performed using the Student's t-test for variables with normal distributions based on the Kolmogorov–Smirnov test and using the Wilcoxon signed-rank test for variables that were not proven to be normally distributed. Also, the Wilcoxon signed-rank test was applied for categorical and discrete variables. Differences were considered statistically significant with a p-value of <0.05 as the type I error, with a statistical power >80% (power >0.8). Paired tests were used when comparing the results of variables measured in the same patient at different times, while nonpaired tests were used when comparing variables between GA and GB. For the statistical analysis, Action v2.8 based on R platform as a plug-in for Microsoft Excel 2010 was used.
Results
The clinical parameters before the initiation of TSH stimulation for GA and GB are shown in Table 1, and no differences were observed between the groups for any variable. Additionally, no differences between GA and GB were observed for pathological tumor stage or lymph node stage. The mean results before TSH stimulation for free thyroxine, TSH, thyroglobulin, and antithyroglobulin antibody levels are also shown in Table 1, and there were no significant differences between the two groups.
No significant differences were observed between the two groups.
TSH, thyrotropin; GA, group A; GB, group B; HR, heart rate; SDP, systolic blood pressure; DBP, diastolic blood pressure.
Values are expressed as absolute numbers or as M ± SD.
The mean duration of levothyroxine withdrawal in GA was 35 ± 5 days (range 28–45 days). In GA, the free thyroxine and TSH levels after stimulation were 0.24 ± 0.19 ng/dL and 68 ± 38 μIU/mL, respectively, and in GB, they were 1.76 ± 0.26 ng/dL and 117 ± 34 μIU/mL, respectively. The differences between the two groups for both of these variables were significant (p < 0.001) as expected.
The GFR results obtained by 51Cr-EDTA and by the modified MDRD equation are presented and compared in Table 2. In GA, the GFR was significantly different from before-to-after THW by both the 51Cr-EDTA (p < 0.001) and modified MDRD (p < 0.001) methods. In GB, the GFR was not significantly different from before-to-after rhTSH by both the 51Cr-EDTA (p = 0.64) and modified MDRD (p = 0.69) methods.
A significant difference was observed in GA but not in GB.
GFR, glomerular filtration rate; THW, thyroid hormone withdrawal; rhTSH, recombinant human thyrotropin.
Values are expressed as M ± SD.
GRF measured by 51Cr-EDTA was not significantly different between GA and GB before stimulation (p = 0.61) but was significantly different after THW and rhTSH (p = 0.009). GFR measurements before and after TSH stimulation for GA and GB are presented in Figure 1.
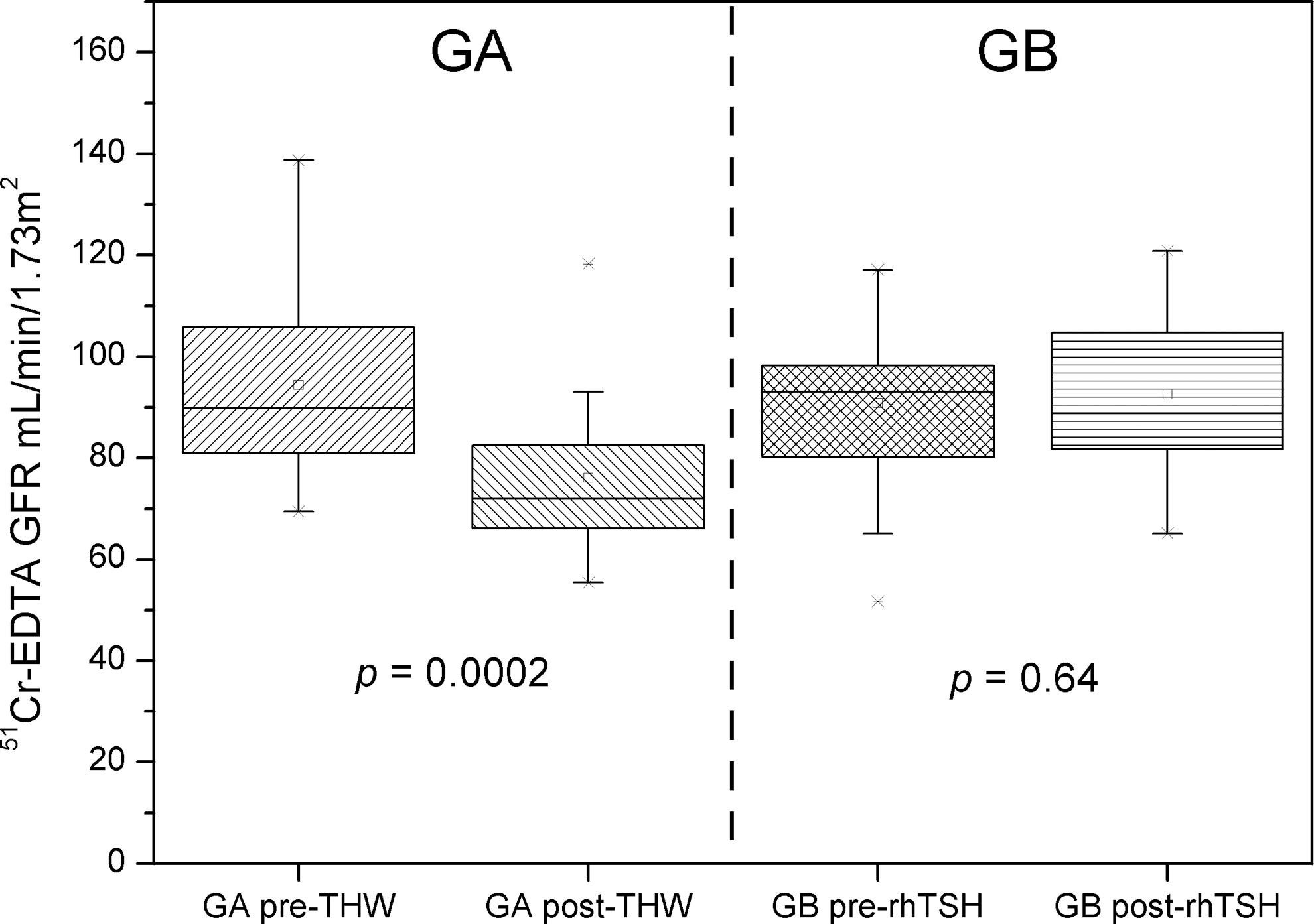
Comparison between glomerular filtration rate (GFR) before and after thyroid hormone withdrawal (THW) in group A (GA), and between GFR before and after rhTSH in group B (GB). The data indicate that a significant difference is observed in GA, while no difference is seen in GB.
The percentage difference between GA and GB in GFR after TSH stimulation obtained by subtracting the former from the later was 22.5% for the 51Cr-EDTA measurements and 30% for the MDRD measurements. The correlation between GFR measured by 51Cr-EDTA and modified MDRD is presented in Figure 2, and variances between GFR percentages are presented in Figure 3. Modified MDRD results before and after TSH stimulation, two days after RIT, and at the WBS moment for GA and GB are shown in Figure 4.

Correlation between GFR measured by 51Cr-EDTA assay and the modified MDRD equation. The Pearson correlation coefficient was 0.79, indicating a moderate positive correlation.

Correlation between the percentage variance of GFR measured by the 51Cr-EDTA assay and the modified MDRD equation. The Pearson correlation coefficient was 0.51, indicating a moderate positive correlation.
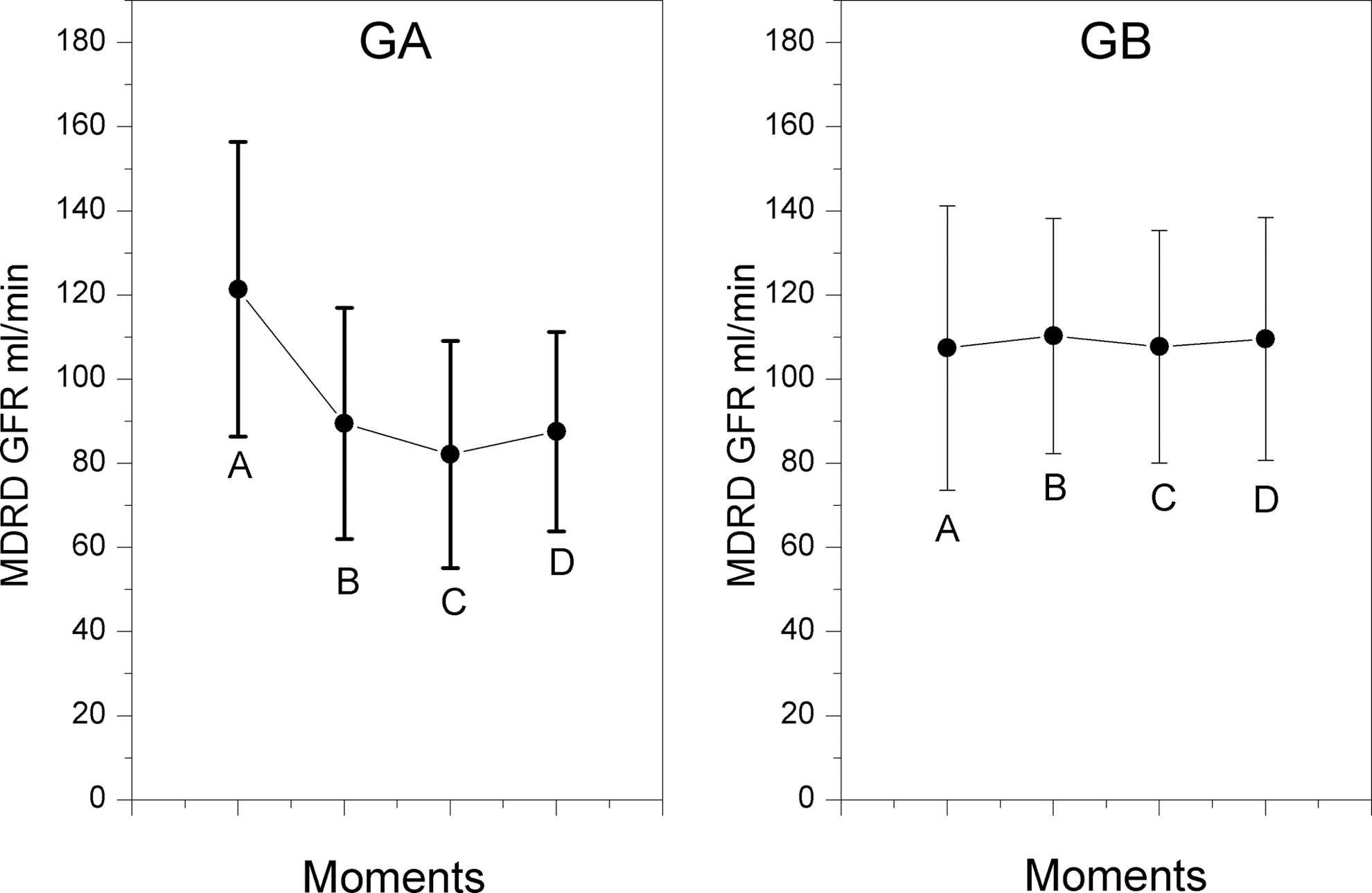
Results of GFR measured by the modified MDRD equation in GA (
Discussion
Both groups were clinically similar, without any significant differences between them, except for the method used to stimulate radioiodine uptake, and were also similar to those of previously published clinical studies (21). The TSH stimulation methods used in this study were similar to those described in previous studies and are considered to be equally effective for RIT (13,14). The purpose of ablative RIT in these patients was to reduce disease recurrence and disease-related mortality for intermediate risk DTC patients (18,22). No differences between their initial GFR statuses were observed prior to TSH stimulation, and GFR values were within the reference range, possibly indicating adequate thyroid hormone replacement. No patient was diagnosed with GFR impairment before TSH stimulation.
Montenegro et al. demonstrated that serum creatinine levels decrease in patients with primary hypothyroidism after thyroid hormone replacement, resulting in an increase in creatinine clearance (23). Other authors have also demonstrated differences in GFR in different clinical hypothyroid settings (8,24 –26). Hypothyroid patients could show improved renal function with adequate management, even when hypothyroidism is associated with chronic kidney disease, as shown by Hataya et al. (27). Also, the levels of thyroid hormones in chronic kidney disease patients could possibly be independent predictors of mortality, even in euthyroid patients, as stated by Carrero et al. (28). Saini et al. addressed the need for regular monitoring of thyroid hormone status (29), but the quantitative impact of thyroid hormone on GFR measured by reliable methods and the physiological causes of this impairment have not been thoroughly evaluated.
To the authors' knowledge, only two studies have assessed GRF in hypothyroidism using 51Cr-EDTA. The first study was published by Villabona et al. in 1999 and evaluated 17 patients with primary hypothyroidism that experienced a recovery of GFR from 99.6 ± 32.2 mL/min before hormonal treatment to 125.7 ± 41.2 mL/min after hormonal treatment (9). Interestingly, the authors also evaluated effective renal plasma flow (ERPF) and observed an increase from 542.8 ± 215.8 mL/min/1.73 m2 prior to treatment to 717.0 ± 140.6 mL/min/1.73 m2 after hormone substitution (9). Therefore, the GFR impairment may be secondary to ERPF. Some authors have reported that endothelial dysfunction induced by hypothyroidism can persist even after prolonged thyroid hormone replacement (30) and that this endothelial dysfunction can be related to changes in blood flow in different organs, including the brain (31). Serum thyroid hormones are also related to blood pressure variability (32), and it is possible that cardiovascular alterations result in a redistribution of splanchnic flow leading to an ERPF decrease that could possibly underlie GFR impairment.
The second study by Karanikas et al. studied patients who were about to undergo thyroidectomy and subsequent RIT (8). The authors used 51Cr-EDTA to measure GFR and measured tubular function with 99mTc-MAG3 in 27 patients in THW for RIT and repeated the measurement after eight weeks of thyroid hormone therapy. An improvement in GFR from 61 ± 18 mL/min to 75 ± 23 mL/min (8) was observed, but renal tubular function determined by 99mTc-MAG3 was not significantly different between patients in a hypothyroid and a euthyroid state. However, due to the absence of a control group, the results of that study have limited reliability because alterations in maximal urine osmolarity, free water clearance, free water reabsorption, and ion tubular reabsorption can occur in hypothyroidism, as demonstrated in animal models (33). Additionally, recent studies have demonstrated that kidneys express thyroid-related genes such as the TSH receptor gene (TSHR) (34). Therefore, the possibility that renal effects on GFR are mediated by direct action of TSH on renal TSHRs to elicit a nonthyroid hormone-mediated response cannot be ruled out (8).
This study included patients with no prior renal disease who had never previously experienced a hypothyroid state. THW resulted in a GFR decrease of approximately 18%, which is similar to that observed by Karanikas et al. (8). rhTSH in GB resulted in a slight increase in GFR of approximately 4%, but that increase was not statistically significant. Another recent study suggests that rhTSH can improve renal function (35). However, because renal function was assessed using a creatinine-based MDRD equation, the results of that study may be inaccurate, and the improvement in renal function may have been overestimated. The present study used a direct GFR measurement method and demonstrated a slight increase in GFR after rhTSH. Therefore, TSH stimulation may have a small stimulatory effect in euthyroid patients. This study also demonstrates an increase in free thyroxine levels in GB after rhTSH compared with the level before stimulation, which could have accounted for the slight increase in GFR. Although this is an interesting finding, further investigations are required to clarify the mechanisms related to the increase in GFR following rhTSH administration.
A moderate positive correlation was also found between GFR measured by 51Cr-EDTA and the modified MDRD, as well as a moderate positive correlation between the percentage variances of these two methods, indicating that both of these methods can be used to evaluate GFR in hypothyroidism. The percentage variation for GFR measured by the modified MDRD was higher than that for GFR measured by 51Cr-EDTA, and this finding may be related to an overestimation of GFR by creatinine-based equations.
In conclusion, based on the present results, it is suggested that the GFR impairment is related to low levels of thyroid hormone in hypothyroid humans and is not due to TSH stimulation. It can also be concluded that during RIT, THW impairs glomerular filtration while rhTSH stimulation does not. The underlying cause of GFR impairment in patients with hypothyroidism is still unclear, and further investigation is needed.
Footnotes
Acknowledgments
This work was funded by the government of São Paulo through FAPESP research grant number 11/51133-5 and was registered on
Author Disclosure Statement
George Barberio Coura-Filho has been an advisor and speaker for Bayer Healthcare