
Abstract
Background:
Both endogenous and exogenous thyrotoxicosis has been associated with atrial fibrillation and low bone mineral density. Therefore, this study investigated the risk factors associated with prevalent and incident thyrotoxicosis and the initiation of thyroid hormone therapy in a healthy, aging cohort.
Methods:
A total of 1450 ambulatory community volunteer participants in the Baltimore Longitudinal Study of Aging examined at the NIA Clinical Research Unit in Baltimore, MD, have undergone longitudinal monitoring of serum thyrotropin (TSH) and thyroid hormone (free thyroxine and free triiodothryonine) levels as well as medication use every one to four years, depending on age, between 2003 and 2014.
Results:
The prevalence of low TSH was 9.6% for participants on thyroid hormone and 0.8% for nontreated individuals (p < 0.001). New cases occurred at a rate of 17.7/1000 person-years of exposure to thyroid hormone therapy [CI 9–32/1000] and 1.5/1000 person-years in the unexposed population [CI 0.7–2.9/1000]. Women were more likely to be treated and more often overtreated than men were. The adjusted hazard ratio (HR) for thyrotoxicosis between treated and untreated women was 27.5 ([CI 7.2–105.4]; p < 0.001) and 3.8 for men ([CI 1.2–6.3]; p < 0.01). White race/ethnicity and older age were risk factors for thyroid hormone therapy but not overtreatment. Body mass index was not associated with starting therapy (HR = 1.0). Thyroid hormone initiation was highest among women older than 80 years of age (3/100 person-years). For one-third of treated participants with follow-up data, overtreatment persisted at least two years.
Conclusions:
Iatrogenic thyrotoxicosis accounts for approximately half of both prevalent and incident low TSH events in this community-based cohort, with the highest rates among older women, who are vulnerable to atrial fibrillation and osteoporosis. Physicians should be particularly cautious in treating subclinical hypothyroidism in elderly women in light of recent studies demonstrating no increased risk of cardiovascular morbidity or death for individuals with elevated TSH levels <10 mIU/L.
Introduction
T
An emerging consensus in the literature suggests that mild subclinical hypothyroidism (elevated TSH levels <7–10 mIU/L with normal thyroid hormone levels) is not associated with a statistically significant increased risk of mortality or morbidity (7 –18). Consistent with this perspective, results of randomized trials of levothyroxine treatment have generally failed to show a benefit for symptoms, and have had mixed results regarding favorable impact on serum lipids, cardiac function, and survival, with positive effects observed for those with more severe hypothyroidism (reviewed in Cooper and Biondi (6)).
Subclinical thyrotoxicosis, a low TSH with normal thyroid hormone level, can occur from endogenous causes such as Graves' disease or toxic goiter, and from iatrogenic overtreatment with thyroid hormone. Endogenous subclinical thyrotoxicosis has been associated with atrial fibrillation in multiple studies, with the risk proportional to the degree of TSH suppression (19 –24). This increased risk of atrial fibrillation appears to be similar when thyrotoxicosis stems from overtreatment with thyroid hormone supplementation (22). A recent pooled evaluation of 10 cohort studies covering 52,674 participants also found greater total and coronary heart disease mortality associated with subclinical hyperthyroidism (25). Finally, subclinical hyperthyroidism has also been associated with reduced bone mineral density and increased risk of fracture in women, although the data remain controversial (26).
The large size of the population at risk for harm from iatrogenic thyrotoxicosis was first suggested 10–20 years ago. Cross-sectional studies in the United States found that 14–22% of treated subjects have low TSH, consistent with excessive therapy, although some proportion of this might be intentional in thyroid cancer patients who were not excluded in the early studies (27 –30). More recently in the United Kingdom, 16% of those on thyroid hormone, excluding cancer, were found to have had at least one low TSH by five years of therapy, about a third of these suppressed <0.1 mIU/L (3). Understanding overtreatment is especially relevant to geriatric populations, as representative population data from NHANES demonstrated that subclinical hypothyroidism increases with increasing age (29) and prescribing trends for initiating therapy at lower TSH thresholds have occurred particularly in older persons (3,31).
In summary, the risks of atrial fibrillation and decreased bone density are both of particular concern in the geriatric population who appear to be at increased risk from thyroid hormone overtreatment. Data were therefore used from the Baltimore Longitudinal Study of Aging (BLSA) to examine the rates and risk factors for endogenous and iatrogenic thyrotoxicosis in community-dwelling older adults and to assess the characteristics of those receiving new thyroid hormone prescriptions.
Methods
Study population
The eligible population included the subset of participants with thyroid function tests in the BLSA, a long-term study of aging begun in 1958 that recruits healthy volunteers living independently in the community (32). Participants can enroll at any age over the age of 20 years provided they are free of cognitive impairment, functional limitations, and major chronic conditions. Once enrolled, participants are followed for life on a variable schedule depending on age. Visits typically take place over a three-day stay at the National Institute on Aging Clinical Research Unit in Baltimore, Maryland, starting in the afternoon on day 1. Thyroid function tests have been collected in the morning on day 2 of the visit, after an observed overnight fast and before morning medication administration, since 2003. In the event of an acute illness or injury, participant visits are postponed and rescheduled. Detailed medication data and medical history are collected at every visit. The vast majority of those on thyroid hormone were using levothyroxine alone, with two participants on desiccated thyroid preparations and one on cytomel as well as levothyroxine. Because of the heterogeneous nature of the supplementation, the general term “thyroid hormone” is used throughout. Information was also collected on of the use of steroids, lithium, estrogenic compounds, anti-estrogenic therapies, and amiodarorone. No one was excluded based on medication use. Demographic and anthropometric data are also available for relevant potential covariates including race/ethnicity, sex, age, smoking history and status, and BMI. At least 1 and up to 11 measures of thyroid function including TSH and/or free thyroxine (fT4) were available through July 2014 for 1450 participants. Seven participants who had or developed thyroid cancer were excluded from the analysis, as sometimes TSH suppression is a deliberate therapeutic strategy in these cases. The study population was therefore 1443, of whom seven are missing an initial TSH, 16 missing initial fT4, and none missing both. Total triiodothyronine was only available for 6% of observations and free T3 (fT3) for 78% of observations. Thyroid antibodies are not available.
Thyroid function definitions
A TSH-dependent definition of thyrotoxicosis was used that includes both cases with endogenous hyperthyroidism and those with excess exogenous thyroid hormone therapy. Over 11 years, several different assays for TSH have been used with slightly different reference ranges. In 2003–2004, TSH, fT4, and fT3 assays were run at Esoterix (TSH reference range 0.5–4.7 mIU/L). Since 2005, the Vista Chemiluminesence Immunoassay (Siemens, Tarrytown, NY) for each analyte has been run on the day of sample collection by the clinical laboratory at Harbor Hospital, Baltimore (TSH reference range 0.35–5.5 mIU/L 2005–2011; 0.4 4.0 mIU/L since 2011).
The assay-specific lower limit of normal was used to define a low TSH for each measure as being below the lower limit of normal in that assay. Prevalent cases of thyrotoxicosis were defined as a low TSH at the first available measure, while incident cases were euthyroid at their first available measure, but had a low TSH during follow-up. Subjects treated with antithyroid therapies, including methimazole, propylthiouracil, or radioactive iodine, were also considered to have thyrotoxicosis from the first report of the medication, even if observed TSH levels were normal.
Overt thyrotoxicosis, with frankly elevated fT4 and low TSH, was observed in only two participants, and therefore the analysis was not stratified by subclinical versus overt disease. Euthyroid sick syndrome is not likely to be an alternative explanation for low TSH in this study because the design requires good health for onsite visits. Furthermore, fT3 levels, which were available for 78% of the visits and 75% of the low TSH measures, were never low in conjunction with a low TSH (data not shown). Central hypothyroidism was also not observed in this cohort, as no low TSH was found in conjunction with a low fT4 (available for 100% of low TSH measures).
Statistical analysis
Pairwise analysis followed by step-wise multivariate Cox proportional hazard and survival analysis was used for prevalent and incident cases, respectively, to examine the relationships between the outcome of a low TSH and possible risk factors or confounding variables, including sex, race/ethnicity, age, the use of thyroid hormone supplementation, body mass index (BMI), and smoking status. For the prospective analysis, the survival analysis was based on time on thyroid hormone therapy for all participants, including those who initiated therapy during the study. A similar approach with step-wise multivariate logistic regression and survival analysis was performed to examine the associations between race/ethnicity, sex, age, smoking and BMI, on the one hand, and being on or beginning treatment with thyroid hormone supplementation.
Results
The study population (Table 1) includes approximately equal numbers of men (725, 50.2%) and women (718, 49.8%). Overall, 25.1% of the cohort identified their race/ethnicity as black and 69.0% identified as white, with 5.9% identifying other races/ethnicities. The average age at the first measured TSH across the whole cohort was 64.6 years [CI 63.8–65.3], with women and nonwhites generally younger. As of July 1, 2014, the average length of follow-up was 4.5 years. Of 1443 participants, 1207 (83.6%) were considered participants in the active cohort, having had their most recent visit within six months of their expected visit date. Further, 122 were deceased, 5 had withdrawn, 30 failed to complete the most recent visit, and 86 were lost to follow-up.
Initial BMI missing for 38.8% of women and 45.4% of men.
Smoking status missing for 5% of women and 7.6% of men.
p < 0.01.
BMI, body mass index.
Use of several medications that can affect TSH levels were found at very low rates, including oral glucocorticoid preparations (n = 10 at the time of the visit, n = 7 within six months of the visit), lithium (n = 1), oral contraceptives or hormone replacement therapy (n = 110), and tamoxifen or aromatase inhibitors (n = 13). Amiodarone, which can cause thyrotoxicosis, was used by 17 participants, one of whom developed hyperthyroidism over the course of the follow-up. Although this rate of thyrotoxicosis is greater than the endogenous rates in nonamiodarone exposed participants, the rate estimate is not precise given the small number of amiodarone users. None of these medications was found to have an association with starting thyroid hormone therapy or having a low TSH in pairwise analysis either for the whole cohort or among those not treated with thyroid hormone. Sensitivity analysis did not demonstrate any significant changes in the hazard ratio estimates for any model when participants were excluded for each medication individually or as a group. Therefore, the final analysis includes all participants.
Prevalent cases of thyrotoxicosis
At the time of their first measurement, 20 participants had a TSH below the lower limit of normal in the assay used, and two were on antithyroid drugs, for an overall prevalence of thyrotoxicosis in 22/1443 or 1.5%. Stratifying by thyroid hormone therapy status, 12/125 treated participants (9.6%) and 10/1318 untreated participants (0.8%) had any degree of thyrotoxicosis (p < 0.001). Thus, 12/22 or 54.5% of low TSH occurred on thyroid hormone. All prevalent cases of thyrotoxicosis were mild, with a mean TSH of 0.24 mIU/L (SD = 0.15 mIU/L) and mean fT4 of 1.33 ng/dL (SD = 0.29 ng/dL). Only 1/12 on thyroid hormone and 2/10 untreated participants had a TSH <0.1 mIU/L (n.s., p = 0.13), all with a normal fT4.
Among those not on thyroid hormone, the average TSH was lower in black compared with white participants (2.1 mIU/L [SE = 0.06] vs. 2.6 mIU/L [SE = 0.07]; p < 0.001). However, the prevalence of TSH below the lower limit of normal did not differ significantly by race/ethnicity (0.88% of blacks vs. 0.73% of whites; p = 0.8). TSH averages increased as expected by age: 2.1 mIU/L (SE = 0.07) younger than 50 years of age, 2.4 mIU/L (SE = 0.04) for those aged 51–79 years, and 2.9 mIU/L (SE = 0.1) for those older than 80 years of age.
New cases of thyrotoxicosis
Follow-up data were available for 1029 initially euthyroid participants, 87 of whom were on thyroid hormone at baseline. Fifty-eight nonthyroid cancer patients initiated thyroid hormone therapy during follow-up, one of whom received combination therapy with L-triiodothyronine and levothyroxine. New cases of thyrotoxicosis were observed in 5/58 and 5/87 newly treated and continually treated participants, respectively. Thus, in total, 10/145 (6.8%) treated participants compared with 8/884 (0.9%) untreated participants developed a low TSH during observation, with 55% (10/18) occurring as a results of thyroid hormone use. Again, the vast majority of cases were subclinical, with a mean TSH of 0.18 mIU/L (SD = 0.1 mIU/L) and a mean fT4 of 1.46 ng/dL (SD 0.4 ng/dL). Two endogenous cases had TSH suppression <0.1 mIU/L, both with concurrent fT4 elevation.
Rates of thyrotoxicosis were found to be 17.7/1000 person-years of exposure to thyroid hormone [CI 9.5–32.8] compared with 1.5/1000 person-years in untreated participants [CI 0.7–2.9]. Stratifying by exposure to thyroid hormone, rates between men and women were similar in unexposed subjects (1.7 men vs. 1.1 women per 1000 person-years); but women much more frequently developed thyrotoxicosis while on thyroid hormone treatment (4.8 men vs. 25.2 women per 1000 person-years; Fig. 1).

Cumulative incidence plot of thyrotoxicosis stratified by sex and the use of thyroid hormone therapy demonstrates the interactive increased risk for women on thyroid hormone therapy. Among those not on therapy men (solid gray) and women (solid black) have similar rates of thyrotoxicosis. While the rate is increased threefold (HR = 3.8) among men on thyroid hormone (dashed gray), women on thyroid hormone (dashed black) develop overtreatment at 10 times the rate of men (HR = 27.7).
Cox proportional hazard analysis of risk factors for thyrotoxicosis was therefore performed with an interaction term for sex and use of thyroid hormone supplementation. Other potential predictors analyzed and adjusted for included age, race/ethnicity, calendar year of the TSH assessment, BMI, and smoking status. Only thyroid hormone use and female sex increased the risk of developing thyrotoxicosis, with significant interactions (Table 2). Although too small a group to analyze separately, it is interesting to note that among the three participants with T3 supplementation as part of their therapy, all had at least one low TSH, two at their first visit and the third during follow-up.
HR, hazard ratio; CI, confidence interval.
Because of the strength of thyroid hormone therapy as a predictor, the subset never on thyroid hormone was also analyzed separately in order to identify risk factors for endogenous thyrotoxicosis, which occurred in 8/884 participants. None of the variables tested demonstrated a significant association with endogenous thyrotoxicosis, including race/ethnicity, BMI, smoking status, age, and total length of follow-up.
Natural history of overtreatment
There were 18 cases of mild (TSH below the lower limit of normal) and four cases of severe (TSH <0.1 mIU/L) subclinical thyrotoxicosis in thyroid hormone–treated subjects without cancer. Among 18 participants with follow-up beyond the first observed low TSH, three mild and three severe cases had persistent thyrotoxicosis over years of observation. For example, in one case, a total of four observed low TSH measurements occurred over six years between the ages of 79 and 85 years.
Thyroid hormone prescriptions
One hundred and twenty-five nonthyroid cancer participants were on thyroid hormone at the first measurement of TSH. This included 45/680 (6.2%) of men and 80/638 (11.1%) of women (p < 0.01). Stratified by age, there were significant differences by sex at younger ages, with 9.2% of women younger than 60 years of age but only 1.4% of men in that age range on thyroid hormone at the first TSH measure (p < 0.01). However, these differences were smaller and nonsignificant among the older participants, such that older than 70 years of age, 13.9% of women and 9.7% of men were on thyroid hormone (n.s., p = 0.1).
Fifty-eight subjects without thyroid cancer initiated therapy during follow-up. While the specific TSH values for which thyroid hormone was initiated were not necessarily observed by the study, it is interesting that only 29/58 ever had an observed maximum TSH above the upper limit of normal, with seven participants having a maximum TSH >10 mIU/L and an additional 10 participants with maximum observed TSH values between 7 and 10 mIU/L.
We examined whether there was a relationship between the peak TSH before supplementation and the risk of thyrotoxicosis on thyroid hormone in the 58 participants started on LT4. Among the five participants who subsequently developed a low TSH, none had a maximum observed TSH >7 mIU/L, and four out of five had a maximum TSH <5 mIU/L. Thus, 5/41 with peak TSH elevations <7 mIU/L who were started on thyroid hormone developed thyrotoxicosis, while none of the 17 with peak observed TSH >7 mIU/L did so, although this difference was not statistically significant (p = 0.1).
Participant characteristics that predicted thyroid hormone initiation include older age, female sex, and white race/ethnicity (Table 3). BMI was not associated with increased risk of starting therapy for the overall cohort. However, the average starting BMI of those in their 50s who were subsequently treated with thyroid hormone was 31.3 (n = 6) compared with 27.2 (n = 158) among those who did not start therapy, with marginal significance due to the small numbers (p = 0.05). Smoking status was not associated with thyroid hormone initiation.
n.s., not significant.
The rate of thyroid hormone supplementation initiation increased with age and among women compared with men (Fig. 2). Maximum rates of therapy initiation were 3.6/100 person-years for women in their 80s (433 years at risk) compared with 1.0/100 for similarly aged men (701 years at risk). For participants in their 60s, rates were estimated at 0.8/100 years for both men and women (765 and 1100 years at risk, respectively).
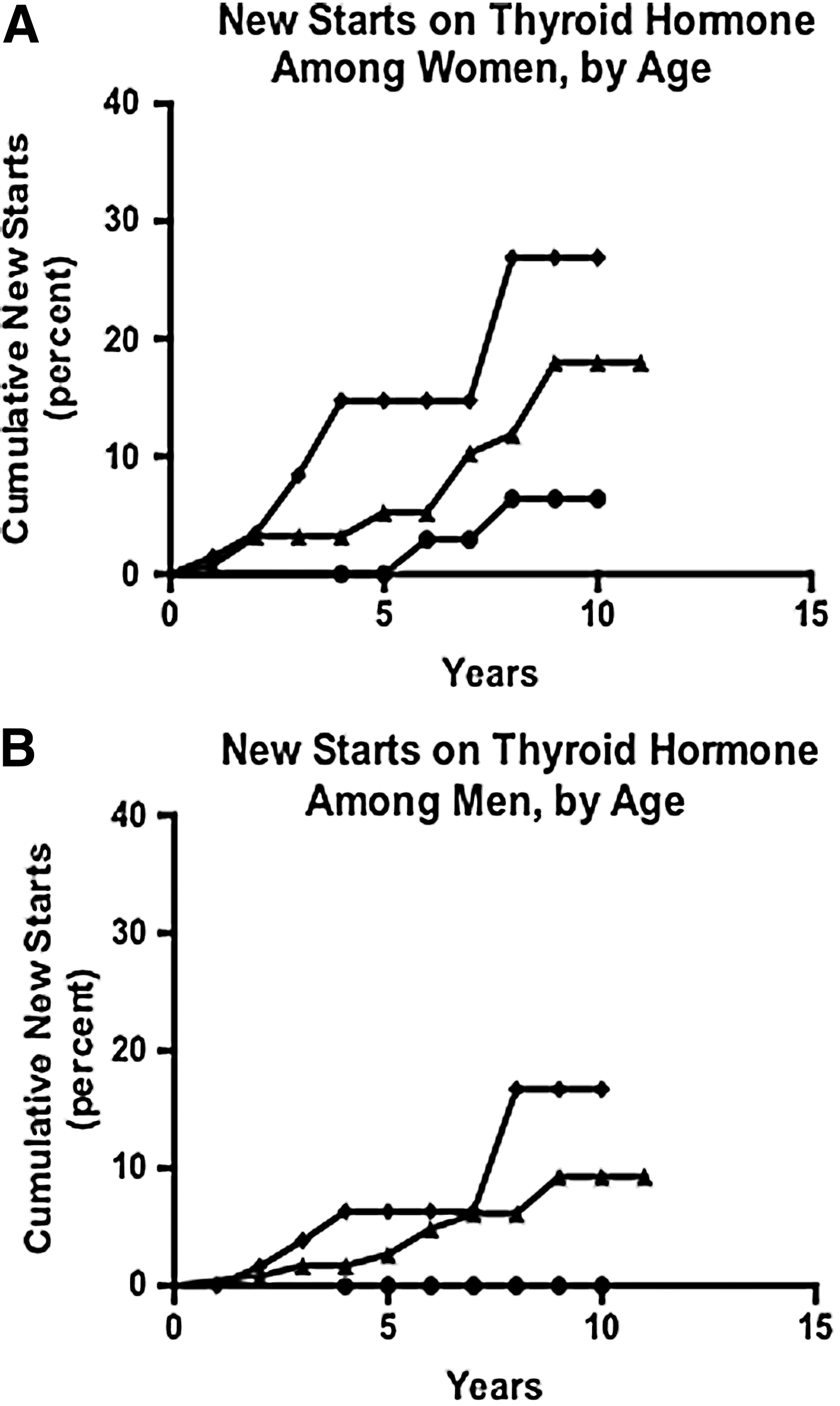
Cumulative incidence of new starts on thyroid hormone therapy among men
Discussion
Thyroid hormone therapy is a medical intervention like any other, with risks and benefits that should be thoughtfully considered (33). Virtually the sole risk attributable to therapy is overtreatment resulting in thyrotoxicosis with consequent increased risk for atrial fibrillation and decreased bone density. With overtreatment defined as a TSH below the lower limit of the reference range, the overall rate in the BLSA study population is estimated at 17.7/1000 participant years of exposure to thyroid hormone therapy, with higher rates for women. This rate is an order of magnitude greater than the endogenous rate of thyrotoxicosis. With current rates of thyroid hormone supplementation in the population, exogenous hormone accounts for half of all cases. A recent estimate of 13.6 million people on levothyroxine in the United States (34) would translate into more than 240,000 new cases of low TSH from overtreatment every year. The risks are probably even higher for those on combination therapy with T3, as thyrotoxicosis was observed in all three subjects on these preparations.
To compare the present results with the older literature, prevalence based on the first observation in which TSH was measured is reported. We found that 9.6% of those on thyroid hormone were overtreated at the start of observation, slightly lower than, but still consistent with, most older cross-sectional studies that report overtreatment in 12–20% of subjects (27 –30). Although not directly reported, the data can be extracted from these studies to estimate that half of low TSH values occur in treated subjects, in line with the present observations.
This is the first study to estimate rates of thyrotoxicosis in the United States using prospective data. A recent study in the United Kingdom reported a similar cumulative rate of overtreatment—16% over five years (3). There are several interesting differences from the present results, which may be due to differences in patient and physician behavior between the two countries. For example, Taylor et al. (2014) report increased odds for thyrotoxicosis in women to be 1.4–1.5 compared with men, where the present study found that women were five times more likely to develop thyrotoxicosis on treatment compared to men. In the British study, younger patients and those with more severe thyroid disease were at highest risk of overtreatment, while the present study did not find a relationship with age, and among the 17 participants started on therapy for peak observed TSH >7 mIU/L, none became subsequently overtreated. However, the average age of the British cohort was younger (59 vs. 66 years), pretreatment TSH assessment was more precise, and the sample was larger, all of which preclude cultural differences as the sole explanatory factor.
If overtreatment were due to clinical lags in the downward adjustment of dose required to match decreased LT4 clearance and increased half-life as people age (35 –37), rates would have been expected to increase with increased age, which they did not. The fact that low TSH persisted over years in about a third of treated participants despite provision and discussion of all clinical laboratory results to study participants at the time of their visit, raises the possibility that risks of overtreatment are unappreciated or that deliberate generous treatment may be thought to improve symptoms. This possibility is also suggested by a recent finding that overtreatment was more likely if prescriptions were started for fatigue or depression (3). It would also be important for future research to understand the extent to which patient preferences may be driving physician practices.
The present rate estimates may be affected by bias that arises from the frequency of sampling, which could lead to failure to identify cases. Annual data were not available for all participants, only for those aged 80 years and older in the cohort. Thus, participants in the younger age groups may have had low TSH events that were addressed by their primary care doctor between study visits. This is more likely to affect iatrogenic events than endogenous events, since initiation of antithyroid therapies is reported at subsequent study visits and thus captured. Thus, the present estimates represent a lower limit on the absolute number of people affected and the rates of overtreatment among thyroid hormone users. Age was not found to be a risk factor for overtreatment, but the sampling bias means that it is possible that younger people are even more frequently overtreated than is thought to be the case. Endogenous events are also underestimated for systematic reasons, since thyroiditis as a cause of transient thyrotoxicosis rarely lasts more than a few months. Underestimating endogenous disease rates more than iatrogenic cases would lead to overestimating the proportion of thyrotoxicosis due to iatrogenic causes. Given the order of magnitude difference in the rates of these diseases, however, any such correction is likely to have a small impact on the estimate.
Another potential bias arises from the practice of the BLSA to report abnormal values found during study visits back to study participants and, with permission, primary care providers. Thus, the primary care physicians may be given TSH data from the BLSA that would not have been available from participants' routine clinical care. This may lead to an increase in the rates of thyroid hormone treatment being initiated among study participants compared with the general population. Being in the study as a risk factor for thyroid hormone therapy was analyzed according to the total years of follow-up, which was longer in bivariate analysis among those who were started on thyroid hormone than in those not started on thyroid hormone (7.1 vs. 4.3 years), although not significant in the fully adjusted Cox models (p = 0.88). Provision of clinical laboratory findings could also serve to reduce the likelihood and/or duration of overtreatment by alerting primary care providers of abnormally low TSH levels about which they would not have otherwise known. Thus, the levels of overtreatment observed in this study may underestimate those in the community at large.
The present results demonstrate that the rates of thyroid hormone therapy initiation increase with age and were highest for women over older than 80 years of age, at up to 3% per year, and whites were more than twice as likely to initiate therapy as black participants. A study from the Cardiovascular Health Study reported a similar finding with an overall rate of new thyroid hormone starts at 1% per year, with higher rates for women, whites, and older subjects (38). That group found an association with higher BMI, which in the current cohort was only present for the youngest subjects.
In conclusion, this study confirms prospectively that overtreatment is a significant risk for those on thyroid hormone therapy, with rates of thyrotoxicosis an order of magnitude higher than background endogenous rates. Therefore, the decision to start therapy and the approach to ongoing monitoring and dose adjustments should consider the potential for this harm. This is especially true when treating geriatric populations who, despite being no more likely to develop iatrogenic thyrotoxicosis, are more vulnerable to its adverse effects.
Footnotes
Acknowledgments
We thank Dr. David Cooper for his close reading of the manuscript. Financial support came from the Passano Foundation, the Walton Family Foundation, NIH grant K23DK095954 to J.S.M., and the NIH Intramural Research Program, National Institute on Aging. Data for these analyses were obtained from the Baltimore Longitudinal Study of Aging, a study performed by the NIA.
Author Disclosure Statement
No competing financial interests exist.