
Abstract
Background:
Studies have suggested that microRNAs (miR) may be useful prognostic markers and are associated with aggressive clinicopathologic features in papillary thyroid cancer (PTC). This systematic review examined associations between miRs and aggressive clinicopathologic features in PTC.
Methods:
A literature search was performed within the PubMed, Embase, Cochrane, Web of Science, and Scopus databases for papers published prior to November 24, 2014. The search was performed by combining the concepts “thyroid tumor” with “microRNA” and by using “and” as the Boolean operator. Upon retrieval of candidate studies, full-text publications were reviewed in their entirety and selected if they examined the prognostic significance between miR expression and established aggressive clinicopathologic features of PTC.
Results:
Fifteen studies from 13 unique groups that included 807 patients were reviewed. Most of the studies were retrospective, and none included patients who had undergone routine central lymph node dissection. Expression levels of miRs-21, −34b, −130b, −135b, −146b, −151, −181b, −199b-5p, −221, −222, −451, −623, −1271, −2861, and let-7e showed significant association with at least one aggressive feature, such as large tumor size, extrathyroidal extension, multifocality, lymphovascular invasion, lymph node metastases, distant metastasis, advanced American Joint Cancer Committee stage, and presence of the BRAFV600E mutation. Herein we summarize the literature with regard to these associations.
Conclusion:
Further studies are needed to investigate whether miRs are independent predictors of aggressive clinicopathologic features before it can be recommended that miR expression levels should be incorporated into the management algorithm for patients with PTC. A well-designed prospective study is needed to assess these potential associations.
Introduction
P
Aggressive clinicopathologic features of PTC such as tumor size >2 cm, multifocality, extrathyroidal extension (ETE), lymphovascular invasion (LVI), lymph node metastasis (LNM), distant metastases, and histological variants such as tall-cell or columnar types determine treatment options and play key roles in patient outcome. However, often these clinicopathologic features are unknown preoperatively and are thus unavailable to guide precise surgical management, including the determination of whether a patient should undergo a prophylactic central lymph node dissection (CLND) (4 –7).
The recent expansion of knowledge and efforts to genetically characterize PTCs by The Cancer Genome Atlas Research Network (TCGA) Thyroid Working Group and others have revealed that microRNAs (miR) may play an important role in PTC prognosis (8 –19). miR are small nonprotein-coding RNA molecules that are 21–25 nucleotides in length. They regulate gene expression at the post-transcriptional level by binding to imperfectly complementary sequences within target miRs (often in the 3′-untranslated regions), thereby leading to degradation or translational suppression (20). Previous studies have reported that specific miRs are associated with aggressive clinicopathologic features of PTC, such as those listed above in addition to BRAF mutation. However, other studies have failed to report any significant association (9 –18,21 –25).
Despite the inconclusive studies in the literature, the incorporation of specific miR expression panels into the surgical management algorithm of PTC in order to improve perioperative decision making has been suggested (9 –18,21 –25). To the authors' knowledge, however, there is no published systematic review examining the clinicopathologic significance of miRs in PTCs. Therefore, a systematic review of the literature was conducted to examine the associations between expression levels of certain miRs and aggressive clinicopathologic features in PTC.
Materials and Methods
All aspects of the Cochrane Handbook for Interventional Systematic Reviews (26) were followed. The study was written in accordance with the guidelines proposed by the preferred reporting items for systematic review and meta-analyses (PRISMA) statement (27). Papers published prior to November 24, 2014, were searched on PUBMED, EMBASE, Cochrane, Web of Science, and Scopus databases by combining the terms “thyroid tumor” with “microRNA” by using “AND” as the Boolean operator (see Supplementary Data; Supplementary Data are available online at
Three reviewers (P.A.H., C.H.W., and H.T.K.), working independently and in three teams of two, used web-based standardized forms and screened all abstracts and titles for miR expression in PTC. Upon retrieval of candidate studies, full-text publications were reviewed in their entirety and selected if they examined the prognostic significance between miR expression and any clinicopathologic features of PTC. Specific clinical features included patient sex, age, tumor size, histological subtype of PTC, multifocality, capsular invasion, LVI, ETE, LNM, distant metastasis, stage of disease (American Joint Cancer Committee; AJCC), and BRAFV600E mutation status.
Exclusion criteria included the following: review articles, single case reports, letters to the editor, abstracts presented in conferences, studies using miRs for differentiation between benign and malignant thyroid lesions, studies examining miR target genes, and studies of in vitro models. In instances where the same study cohort was used in multiple articles reporting different miRs, only the study based upon the largest patient population was included in the total patient count (11,12,17,18). The reviewers also independently assessed citations of relevant articles to identify additional studies for inclusion. At each stage of the selection process, discrepancies in article selection between two reviewers were discussed by the study team members and resolved. Reviewers also extracted methodological and outcome data from all eligible studies.
Results
Figure 1 describes the flow of candidate and eligible articles. After removing duplicates, a total of 830 abstracts were identified, of which 174 by title and abstract alone were deemed relevant. Of the 174 full-text articles evaluated against the predetermined inclusion criteria described above, 48 articles met the initial eligibility criteria. Of these, 33 articles were excluded because they were in vitro studies or studies using miRs for diagnosis only. The remaining 15 studies were systematically reviewed and abstracted.
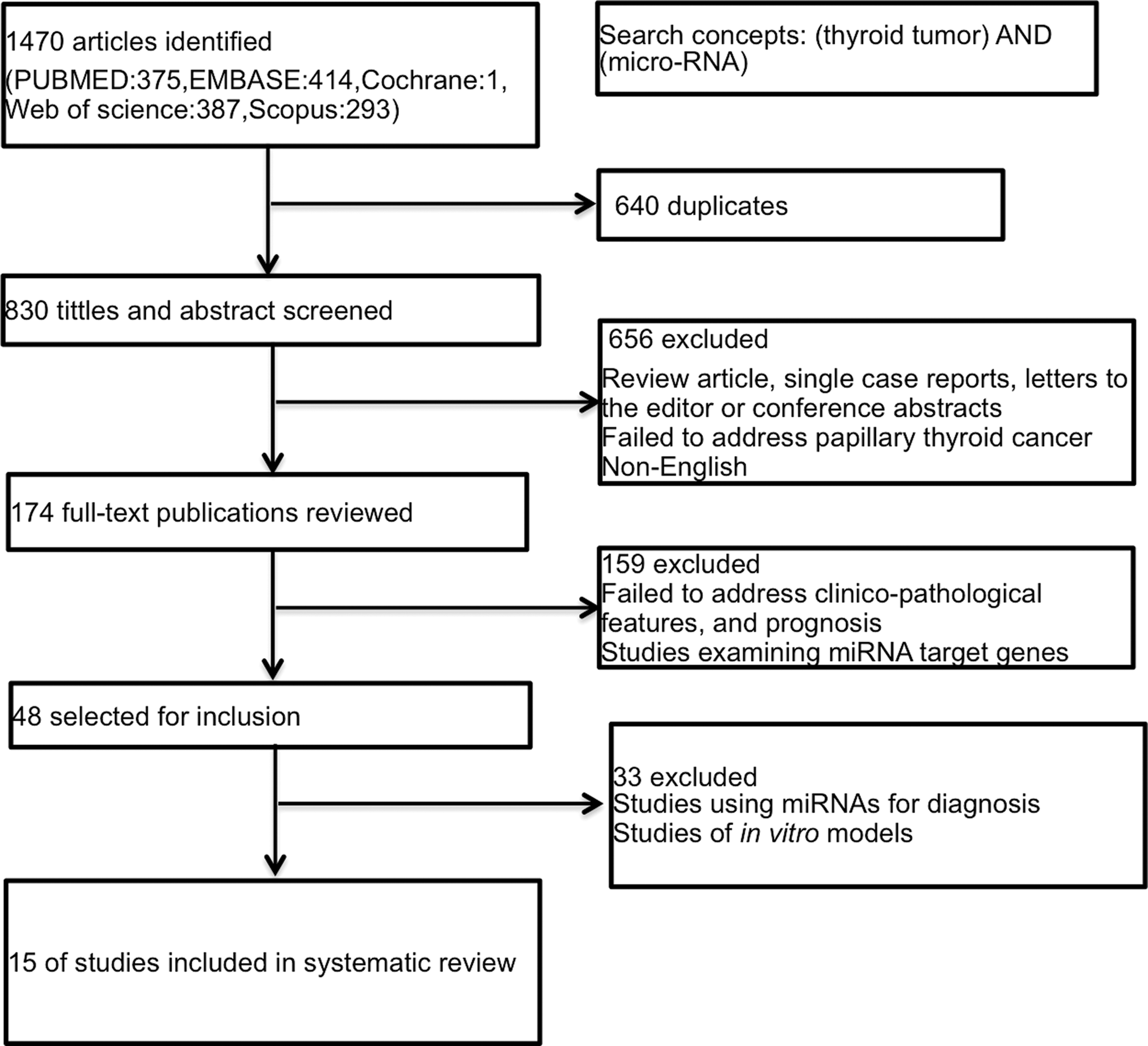
Preferred reporting items for systematic review and meta-analyses (PRISMA) flowchart: algorithm for identification of eligible studies with inclusion and exclusion criteria.
Design of the studies
Table 1 summarizes the results of the 15 studies comprising 807 patients (9 –15,17,18,21 –25,28). The earliest study was published in April 2009 (23), and the latest in August 2014 (14). The largest study evaluating miR expression from tissue samples included 100 patients (18); only one study evaluated circulating serum miR and included 106 patients (25). The smallest study evaluating miR expression in tissue samples included 30 patients (15). Two studies were prospective (17,25). None of the studies included patients who had undergone prophylactic lymph node dissection.
miR nomenclature: The prefix “miR” is followed by a dash and a number, the latter often indicating order of naming (e.g., miR-21 was named prior to miR-34); a capitalized “miR-” refers to the mature form of the miRNA; miRs with nearly identical sequences except for one or two nucleotides are annotated with an additional lower case letter (e.g., miR-146a and miR-146b are closely related); when two mature miRs originate from opposite arms of the same pre-miR, they are denoted with a −3p or −5p suffix (e.g., miR-146-3p and miR-146-5p).
Studies 3 and 14 and 8 and 9 studied different miRs.
The total n includes the larger number of cases from the two sets of presumably overlapping patients.
All miRs were upregulated, except miRs-34b and −130b, which were downregulated. Study #3 performed multivariable logistic regression analysis; study #10 measured circulating serum miRs.
, statistically significant; −, no association; [blank space], surrogate outcome was not tested.
miR, microRNA; PTC, papillary thyroid carcinoma; LVI, lymphovascular invasion; ETE, extrathyroidal extension; LNM, lymph node metastases; AJCC, American Joint Cancer Committee.
For initial biomarker screening, eight studies performed miR microarray (10 –12,14,15,21,22,28), and one performed Solexa RNA sequencing (25) followed by quantitative polymerase chain reaction (q-PCR) to validate the results. Conversely, six studies identified candidate miRs from the literature and performed q-PCR (13,17,18,23,24) or Northern blots (9) to characterize miR expression. Four studies evaluated miR expression in formalin-fixed paraffin-embedded (FFPE) tissue (13,15,21,23), whereas seven used fresh frozen tissue (11,12,14,17,18,24,28), three used a combination of FFPE and frozen (9,10,22), and only one examined serum (25).
The 15 studies utilized a variety of statistical methods to analyze their outcomes (Supplementary Table S1). A number of studies (9 –12,15,17,21,24,25) compared the mean of miR expression using Student's t-test, a parametric test for testing differences in mean between groups. In studies where the assumptions for using parametric tests were not met (9 –13,15,17,18,22 –25), Kruskal–Wallis, Mann–Whitney U, or Wilcoxon rank sum tests were used to compare continuous values of miR. Eight studies (10,13 –15,21,22,25,28) also utilized parametric and nonparametric tests to compare other continuous variables. The correlation between different miRs was tested in three studies (21,24,25) by using Pearson's correlation coefficient. Differences between groups for categorical variables were analyzed utilizing Pearson's chi-square test in multiple studies (9,12,13,15,17,22,23). Specifically, this was often used for comparing BRAF mutation status between groups. Only one study performed both univariate and multivariable logistic regression to identify independent clinicopathologic features and molecular markers for prognosis (17). Disease-free survival was analyzed in two studies, which utilized Kaplan–Meyer graphs, log–rank test, and Cox proportional hazards models (17,22). None of the studies examined addressed the positive predictive value (PPV) or negative predictive value (NPV) of miRs in their analyses (9 –15,17,18,21 –25,28).
The risk of bias in the included studies was assessed using a modified Newcastle–Ottawa Scale (NOS) for observational studies (29). The NOS includes a set of questions, or scale, consisting of eight multiple-choice questions that address subject selection and comparability (of cases and controls in case-control studies, of cohorts in cohort studies) and the assessment of the outcome (in case-control studies) or exposure (in cohort studies). High-quality responses earn a star, totaling up to nine stars (the comparability question earns up to two stars) (29,30). In this review, a score was presented summarizing the number of stars earned by each study in each domain (Supplementary Table 2). Overall, the studies were consistently of high quality. However, including patients with routine CLND would have improved comparability. For the assessment of selection criteria, one study received two stars (21), while 14 of the 15 studies had four stars (9 –15,17,18,22 –25,28). For the assessment of comparability of the groups, three studies were given two stars (17,22,25), while 12 studies received one star (9 –15,18,21,23,24,28). All 15 of the included studies scored four stars in the exposure criteria (9 –15,17,18,21 –25,28).
miR and aggressive features in PTC
Sex and age
Ten studies, including 644 cases, analyzed the association between miR expression levels and sex (9,12 –14,17,18,23 –25,28), of which two studies reported a significant association (12,18). Expression levels of miRs-146b, −221, and −222 were significantly higher in male patients. The same 10 studies analyzed the association between miR expression levels and age (9,12 –14,17,18,23 –25,28). Only one study (12) reported age-associated expression changes, with significantly higher expression of miR-222 in patients ≥45 years of age.
Tumor size, histological subtypes, and multifocality
Ten studies, including 632 cases, analyzed the association between miR expression and tumor size (9,12 –14,17,18,21,23 –25), of which five studies reported a significant association (12,13,21,23,25). There was a positive correlation between larger tumor size and expression levels of miRs-135b, −146b, −151-5p, −181b, −221, and −222 (12,13,21,23,25). Three studies (21 –23), including 157 cases, analyzed the association between miR expression and histological subtypes of PTC. Higher expression levels of miRs-221, −222, and −623 were associated with classical variant of PTC (CVPTC), whereas higher expression levels of miRs-125a-3p, −153, and −1271 were associated with follicular variant of PTC (FVPTC) (21,22). Furthermore, miRs-146b, −221, and −222 exhibited the highest fold change in tall-cell variant of PTC, followed by CVPTC and FVPTC (23), whereas miRs −375 and −551b were found to be highly upregulated in FVPTC (22). Nine studies, including 649 cases, analyzed the association between miR expression and multifocality (9,12,14,18,21,23 –25,28), of which only two reported a significant association (21,25). Higher expression levels of miR-146b and let-7e were associated with multifocal PTC (21,25).
Capsular invasion, LVI, and ETE
Only one study (21), including 57 cases, analyzed the association between miR expression and capsular invasion, of which miRs-146b, −221, and −222 were significant (21). Two studies (13,21), including 109 cases, analyzed the association between miR expression and LVI. Only one (21) reported expression levels of miRs-146b, −221, and −222 to be associated with LVI. Seven studies, including 326 cases, analyzed the association between miR expression and ETE (9,12,14,17,18,23,24), of which five reported a significant association (9,12,14,18,24). Higher expression levels of miRs-135b, −146b, −199b-5p, −221, and −222 were associated with ETE (9,12,14,18,24). Furthermore, higher expression levels of miR-146b were associated with extensive extrathyroidal invasion in a subgroup analysis of 25 cases with ETE (12).
LNM and distant metastasis
Eleven studies, including 701 cases, analyzed the association between miR expression and LNM (9,11 –14,17,21,23 –25,28), of which eight reported a significant association (9,11 –14,17,21,25,28). Expression levels of miRs-21, −146b, −151-5p, −199b-5p, −221, −222, −451, and −2861 were significantly higher in patients with LNM (9,11 –14,17,21,25,28). Furthermore, expression levels of miRs-451 and −2861 were significantly higher in patients with lateral LNM (11). Three studies, including 209 cases, analyzed the association between miR expression and distant metastasis (17,21,24). Expression levels of miRs-146b and −221 were significantly higher in cases with distant metastasis (21).
Tumor staging (AJCC)
Nine studies, including 572 cases, analyzed the association between miR expression and tumor staging (9,10,12,13,17,18,21,24,25), of which seven reported a significant association (9,10,12,13,17,21,25). Higher expression levels of miRs-135b, −146b, −221, and −222 were significantly associated with high-risk groups, defined as patients with AJCC stage III or IV (9,10,12,13,17,21,25).
BRAFV600E mutation
Nine studies, including 496 cases, analyzed the association between miR expression and BRAFV600E mutation status (9,10,13,15,17,18,23,25,28), of which six reported a significant association (9,10,13,15,17,28). Expression levels of miRs-21, −146b, −203, −181b, −221, and −222 were significantly higher in tumors with BRAF mutation compared with those with wild-type BRAF gene alleles (9,10,13,15,17,28).
Discussion
This systematic review outlines several miRs that were shown to be associated with aggressive features of PTC. The five main publication databases were searched to assure identification of all relevant publications. To the best of the authors' knowledge, this represents the first systematic review of miR association with aggressive features of PTC. Overall, most studies identified upregulated expression of miRs-146b, −221, and −222 in association with several aggressive features in PTC. These associations do not necessarily presuppose a causative role for these miRs in progression, but it is possible that miR and miR target dysregulation could represent key molecular events in PTC development and its progression. One could hypothesize, based upon these findings, that increased expression levels of miRs-146b, −221, and −222 provide cells with a selective growth advantage, leading them to develop aggressive features sequentially such as larger tumor size, ETE, LNM, and advanced AJCC stage. As shown in Table 2, these latter aggressive features were the most consistently reported to be associated with miR upregulation. Older age and male sex are risk factors associated with poorer thyroid cancer prognosis, but predicting them using miRs is not meaningful, and they are only listed in the tables as reference to the primary literature.
Number of asterisks (*) in columns representative of number of studies with a significant association.
All miRs were upregulated except miRs-34b and −130b, which were downregulated.
These results are consistent with observations that miR-146b is associated with a risk of recurrence and promotes cell migration and invasion with expression of cancer-promoting genes and regulators of apoptosis (8,17). Furthermore, previous studies have identified that miR-221 and miR-222 are activated by high-motility group box 1 protein (HMGB1) in PTCs, and both promote proliferation by inhibiting the translation of cell cycle regulator p27kip1 (31).
Target genes regulated by miRs-146b, −221, and −222 in PTC remain under study, and little has been reported regarding the molecular mechanism by which miRs influence aggressive features in PTC. MiR-146b is encoded by a gene on chromosome 10q24. Some of the predicted miR-146b-5p targets include adherens junction and mesenchymal-epithelial transition (MET) gene sets, which suggests a functional role in promoting epithelial-mesenchymal transition (EMT). EMT is an important step in metastasis, and as documented in this review (Table 2), several studies suggest that miR-146b-5p may be associated with central LNM. The MiR-221 and miR-222 genes are clustered on chromosome X, which might explain their similar expression pattern and presumed sphere of influence (Table 2). Some of the predicted miR-221 and −222 targets include gene sets that enhance genomic instability and subsequent cell proliferation. The mechanism by which they do so includes reducing p27Kip1 protein expression and promoting EMT that in turn leads to increased growth rate and cancer-cell invasiveness (31,32).
While the biological implications of miRs-146b, −221, and −222 remain under study, recently the TCGA Thyroid Working Group has proposed putative target genes for miR-146b, −221, and −222, which include: IRAK1, KIT, TRAF6, and PDCD4 for miR-146b; and p27Kip1 for miRs-221 and −222 (8), findings that are relevant to the present analysis.
Notably, it is apparent in this systematic review that miRs-146b-5p, −221, and −222 may play a role in BRAF-mutated PTCs. However, there is also evidence that altered expression of miR may occur independent of the BRAFV600E mutation, and other (epi)genetic mechanisms might instead be responsible for their dysregulation (25). BRAFV600E is known to be the most common mutation (up to 80%) found in PTC. However, its role as an independent predictor marker associated with aggressive features, specifically with LNM, is still controversial (33).
While the overwhelming majority of studies measured miR expression in tumor tissue, one study measured circulating miR expression in serum. This study demonstrated the potential of serum let-7e, miR-151-5p, and miR-222 as markers for prognosis in PTC by showing that circulating levels of these miRs are detectable both before and after tumor excision. However, the mechanism underlying the release of miR from tissues into the bloodstream is unknown, and it remains unclear whether circulating miR levels can accurately reflect miR expression in specific tissues (34,35).
Importantly, in the course of conducting this review, a number of limitations were identified in the included studies that may explain the differences in reported results. First, results may be biased because, with the exception of two studies (17,25), all were retrospective. Second, small numbers of patients were analyzed in each study; the largest study included 106 patients (25), raising questions about achieving adequate statistical power. Third, the cutoff levels of miR expression in tumor tissues used to predict prognosis were not uniform. Fourth, with one exception, none of the studies included multivariable analysis (17). Lastly, and most importantly, none of the studies included patients who had undergone routine prophylactic central neck dissection. Performing lymph node dissection only for patients already suspected to have metastases preoperatively can result in a biased study outcome, since the lymph node status is only known for this particular subset of patients.
Because discrepancies exist in the existing literature regarding the association of several miRs with aggressive clinicopathologic features of PTC, the prognostic value of miRs remains to be established in well-designed future studies. An ideal prospective study needs to be adequately powered to detect clinically meaningful differences in the association between miR levels and each of the aggressive features described above, including central LNM. Such a study would require prophylactic CLND in all patients and would need to be powered to detect relationships between miR levels and outcomes across all PTC subtypes. It is recognized that it may be difficult to enroll sufficient numbers of patients to capture adequate samples of the less common forms of PTC (e.g., follicular variant or tall-cell PTC). However, given the fact that the vast majority of the patients have CVPTC, a study powered to detect meaningful differences among patients with classical PTC may provide, at a minimum, genetic insights into common pathways. The principal improvement in understanding the relationships between miR levels and outcomes available from a prospective study involves the elimination of selection bias in CLND. The majority of retrospective studies examined CLN pathology only in patients who underwent CLND, thus biasing the sample of patients studied toward those with possibly more aggressive or advanced disease, or because of surgeon preference.
In addition, PPV and NPV are extremely important factors in determining the usefulness of any test. It is not possible to determine the PPV and NPV of miR levels without including patients who did not undergo CLND. Moreover, PPV and NPV may be very different across PTC subtypes or in the presence of certain disease features.
Although definitive studies are currently lacking, miRs may hold a potential as prognostic indicators in PTC. Measurement of miR expression might facilitate and optimize surgical management of patients with PTC. Yet, currently, information is insufficient to guide clinical decision making. In particular, future development of assays analyzing FNA samples and validation of these findings regarding miRs in the preoperative setting will be needed. Further prospective studies, however, that overcome the aforementioned limitations, including bias in selecting patients for lymph node dissection, are required before incorporating expression levels of miRs as predictive markers of aggressive clinicopathologic features in PTC into clinical practice. It is important that potential markers be tested within relevant clinical scenarios. Simply testing molecular markers for diagnosis or prognosis without placing them into clinical context will not inform us of their true clinical utility.
Conclusion
This systematic review reveals that some miRs are associated with aggressive clinicopathologic features, such as large tumor size, ETE, multifocality, LVI, LNM, distant metastasis, advanced AJCC stage, and presence of the BRAFV600E mutation. However, most of the studies examined were retrospective, and did not include patients who had undergone routine CLND. Further studies are needed to investigate whether miRs are independent predictors of aggressive clinicopathologic features before it can be recommended that miR expression be incorporated into the management algorithm for patients with PTC. A well-designed prospective study is needed to assess these potentially clinically useful associations.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose related to this work.