
Abstract
Background:
Low doses of antithyroid drugs (ATD) for extended periods may be an alternative for Graves' disease (GD) patients who relapse after a course of ATD.
Methods:
Patients with GD relapse (n = 238) after discontinuation of ATD therapy for 12–24 months were retrospectively analyzed in a nonrandomized study. Radioiodine (RAI) treatment and L-thyroxine replacement was used in 114 patients, and a low dose of methimazole (MMI; 2.5–7 mg/daily) was used in 124 patients. Thyroid dysfunction, Graves' ophthalmopathy (GO) evolution, quality of life (QoL), and body weight were evaluated during the follow-up.
Results:
The mean follow-up was 80.8 ± 35.3 months for the RAI group, and 71.3 ± 40.3 months for the low-dose MMI group. No notable side effects were observed in either group. Thyroid dysfunction was predominant in the RAI group (p < 0.001), and euthyroidism was more common in the MMI group (p < 0.001). GO deterioration was mainly evaluated by clinical activity score (CAS)—it was higher in the RAI group (p < 0.0005) over all periods of follow-up. Multivariate logistic analysis showed that RAI treatment was associated with no improvement in CAS during follow-up (24 months: OR = 3.51 [CI 1.02–12.03], p < 0.05; 36 months: OR = 8.46 [CI 1.47–48.58], p < 0.05; 48 months: OR = 19.52 [CI 1.70–223.10], p < 0.05; 60 months: OR = 21.1 [CI 1.5–298], p < 0.05). Kaplan–Meier survival analysis confirmed this finding (p < 0.0003). Assessment of QoL using the Short Form Health Survey's 36 parameters in stable euthyroid patients (at least six months) was similar in both groups. The RAI group patients gained more weight (p < 0.005), particularly after 24 months of follow-up.
Conclusions:
The use of low doses of MMI is efficient and safe, and offers better outcomes for GO than RAI treatment. Prolonged low doses of MMI may be an alternative choice for relapsed GD patients, particularly for GO patients or for patients who refuse a definitive treatment.
Introduction
D
The duration of ATD treatment is in general 12–24 months. Currently, there are two well-established treatment options for hyperthyroidism due to GD. The first one is the conventional ATD dosing regimen using the titration method to keep serum thyrotropin (TSH) and free thyroxine (fT4) in the euthyroid range with the lowest ATD dose. The second method is the “block and replacement” technique, which is frequently initiated with a standard dose of ATD and the addition of L-thyroxine (LT4). A systematic review (8) demonstrated that the two regimens result in similar relapse rates (30–70%). In view of the elevated recurrence rate, a definitive approach such as RAI treatment or thyroid surgery has been recommended for the resolution of hyperthyroidism. Because hyperthyroidism is a syndrome that affects quality of life (QoL) (9) and cardiac function (10), a rational alternative for the relapse of hyperthyroidism could be the reintroduction of a low-dose regimen of methimazole (MMI) aimed at controlling GD for a long period of time. This regimen has been proposed by some authors (11,12), especially in children (13) and patients with Graves' ophthalmopathy (GO) (14,15). Unfortunately, there is still a lack of high-quality data concerning safety, GO, and QoL evaluation of the low-dose MMI treatment. Therefore, the objective of this study was to compare the use of prolonged low-dose MMI with RAI and LT4 treatment for patients with relapsed GD after a conventional course of ATD therapy. During a long-term follow-up, the frequency of thyroid dysfunction was evaluated, and QoL, GO, and body weight changes were measured.
Patients and Methods
Patients
After institutional research ethics approval, all patients who were diagnosed with GD between 1995 and 2013 were retrospectively reviewed. A group of 238 relapsed hyperthyroid patients were eligible to enter the study out of 423 GD patients treated with the conventional regimen of ATD for 12–24 months. The enrolled 238 relapsed hyperthyroid patients met the inclusion criteria: diagnosis of GD and hyperthyroidism characterized by diffuse goiter, increased serum levels of fT4 and/or free triiodothyronine (fT3), a suppressed serum TSH level, as well as the presence of positive serum thyroid-receptor antibody (TRAb) and/or diffuse goiter by ultrasonography and increased thyroidal uptake of 99mTc-pertechnetate thyroid uptake. Relapse was defined as the presence of clinical signs of hyperthyroidism with a suppressed or decreased serum TSH simultaneous with elevated serum fT4 and/or fT3 levels. Remission was defined as at least 12 months of clinical and laboratorial euthyroidism or hypothyroidism in the absence of ATD. Patients were excluded if they were younger than 18 years old, were pregnant at diagnosis or became pregnant during the follow-up, were using medications interfering with thyroid function, such as amiodarone, lithium, and chronic corticosteroids, or had had previous thyroid surgery or were already received RAI treatment.
Study design
All 238 patients were evaluated every three months during the first year and every six months thereafter. All patients were examined before the beginning of the treatment and underwent a complete physical examination, along with the collection of data on smoking habits, symptoms of hyperthyroidism, and comorbidities (hypertension, diabetes mellitus, as well as other autoimmune diseases). Experienced clinicians examined patients at the outpatient clinic, and at each appointment, data on body weight, symptoms of thyroid dysfunction, and adverse effects of each treatment were investigated. The laboratory tests carried out at each visit included TSH, fT4, blood cell count, serum alanine aminotransferase, aspartate aminotransferase, gamma-glutamyltransferase, fasting glucose, and creatinine.
Relapsed GD patients were offered two methods of treatment (MMI or RAI), and 124 out of 238 individuals preferred a prolonged treatment with low-dose of MMI (low-dose MMI group). These patients were informed of all possible adverse effects of the drug, and all patients signed written consent forms. During the first three months of the treatment, the initial dose ranged from 10 to 20 mg daily of MMI. Thereafter, the dose was titrated to reach a maintenance dose of 3.98 ± 1.7 mg (range 2.5–7.5 mg) per day. The goal was to keep the serum TSH between 0.4 and 3.0 mIU/L. After a follow-up of 71.3 ± 40.3 months, 114 patients completed the study and were submitted to a complete evaluation. The remaining 114 patients who chose RAI treatment (RAI group) were also informed about the possible therapy side effects, and were treated with a fixed dose of 15 mCi of RAI and LT4 replacement. After 80.8 ± 35.3 months of follow-up, 102 patients completed the study and were submitted to a complete evaluation (Fig. 1). During the follow-up, all patients were given appropriate information and encouraged to maintain compliance with the chosen treatment.

Design of the study.
GO evaluation
GO severity was estimated using the clinical activity score (CAS) according to Mourits et al. (16) giving one point for each of the characteristics (ranging from 0 to 7): spontaneous retrobulbar pain, pain on attempted upwards or downwards gaze, redness of the eyelids, redness of the conjunctiva, swelling of the eyelids, inflammation of the caruncle, and conjunctival edema. Furthermore, intermittent and permanent diplopia was evaluated; eyelid width was measured with a scale rule, and proptosis was measured using a Hertel exophthalmometer. Worsening of GO was defined as an increase in the CAS value of two or more points, whereas GO improvement was defined as a decrease in the CAS value by two or more points. The RAI group patients with active GO (CAS ≥3) received prophylactic prednisone at 0.5 mg/kg on the same day as the RAI treatment; the prednisone administration was tapered down until dose withdrawal 30–40 days later.
Short Form Health Survey evaluation
At the end of the follow-up, the patients who completed the study were evaluated with the Short Form Health Survey (17) also known as SF-36. The SF-36 consists of eight scaled scores; each scale may be directly transformed into a 0–100 scale on the assumption that each question carries equal weight. Lower scores imply greater disability, and higher scores suggest little disability. Only patients in stable euthyroidism for at least six months had their questionnaire selected for further analysis.
Thyroid dysfunction
Thyroid status was evaluated using serum TSH and fT4 levels at each visit during follow-up. Patients were classified as presenting overt hyperthyroidism (serum TSH suppressed or below the reference range associated with elevated serum levels of fT4); subclinical hyperthyroidism (serum TSH suppressed or below the reference range in the presence of normal concentration of fT4); euthyroidism (serum TSH and fT4 levels within the reference range); subclinical hypothyroidism (elevated serum TSH levels in the presence of normal concentration of fT4); or overt hypothyroidism (elevated serum TSH with serum fT4 levels below the reference range). The percentage of patients classified within each category was determined at 12, 24, 36, 48, and 60 months.
Laboratory methods
Serum concentrations of TSH, fT4, fT3, thyroglobulin antibody (TgAb), and thyroid peroxidase antibody (TPOAb) were measured by chemiluminescent assays (DPC Immulite system). The reference values were 0.4–4.1 mIU/L, 10.3–24.4 pmol/L (0.8–1.9 ng/dL), 2.75–4.89 pmol/L (1.8–3.2 pg/mL), positive >40 IU/mL and >35 IU/mL, respectively. Serum TRAb levels were measured by a radio-receptor assay (RSR Ltd.), and the reference value was <10 IU/L. The thyroid size was estimated by ultrasound (reference value range 6–15 mL), and the 99mTc-pertechnetate thyroid uptake reference values ranged from 0.35% to 1.7%.
Blood glucose levels were estimated using the glucose oxidase method. The serum creatinine level was analyzed colorimetrically, and hepatic enzymes were determined enzymatically.
Statistical analysis
Continuous variables are expressed as the mean ± standard deviation (SD), and categorical variables are expressed as percentages. For GO parameters such as CAS, proptosis, eyelid width, and diplopia, the most prominent eye was considered. For the independent samples, Student's t-test was used to compare continuous variables with normal distribution. The Mann–Whitney U-test was used to compare continuous variables without normal distribution. A chi-square test or Fisher's exact test was used to compare the differences between qualitative categorical variables. Univariate analyses of clinical parameters predicting no improvement of GO were assessed followed by multivariate models with a stepwise procedure for variable selection. These were used to identify factors associated with no improvement of GO. p-Values ≤0.05 were considered statistically significant. No improvement in GO was a dependent variable, while patient clinical characteristics were used as putative independent variables. The factors that might have influenced the worsening of GO could not be analyzed because of the small number of cases in the low-dose MMI group. The cumulative probability of the risk of GO worsening was evaluated using Kaplan–Meier analysis between the two groups. All analyses were performed with SAS for Windows v9.4 (SAS Institute, Inc.). p-Values ≤0.05 were considered significant.
Results
The two groups had similar characteristics during the first course of ATD regarding sex, age, thyroid volume, and thyroid antibodies. After relapse, the baseline characteristics of the two groups remained similar (Table 1) concerning age; sex; body mass index (BMI); smoking habits; frequency of TgAb, TPOAb, and TRAb; thyroid volume; concentrations of TSH, fT4, and fT3; duration of previous ATD therapy; euthyroidism before the current therapy duration; and GO features.
Data are mean ± standard deviation.
To convert pmol/L to ng/dL, multiply by 0.077; to convert pmol/L to pg/mL, multiply by 0.651.
Most prominent eye.
RAI, radioiodine; MMI, methimazole; BMI, body mass index; TSH, thyrotropin, fT3, free triiodothyronine; fT4, free throxine; ATD, antithyroid drugs; TPOAb, thyroperoxidase antibody; TgAb, thyroglobulin antibody; TRAb, thyroid receptor antibody; CAS, clinical active score (0–7; severity classification).
Thyroid dysfunction
Thyroid function assessment throughout the follow-up showed a higher frequency of euthyroid status in the low-dose MMI dose group versus the RAI group at 12, 24, 36, 48, and 60 months. In contrast, the percentage of overt hypothyroidism and subclinical hypothyroid patients was higher in the RAI group at 12, 24, 36, 48, and 60 months (Fig. 2).
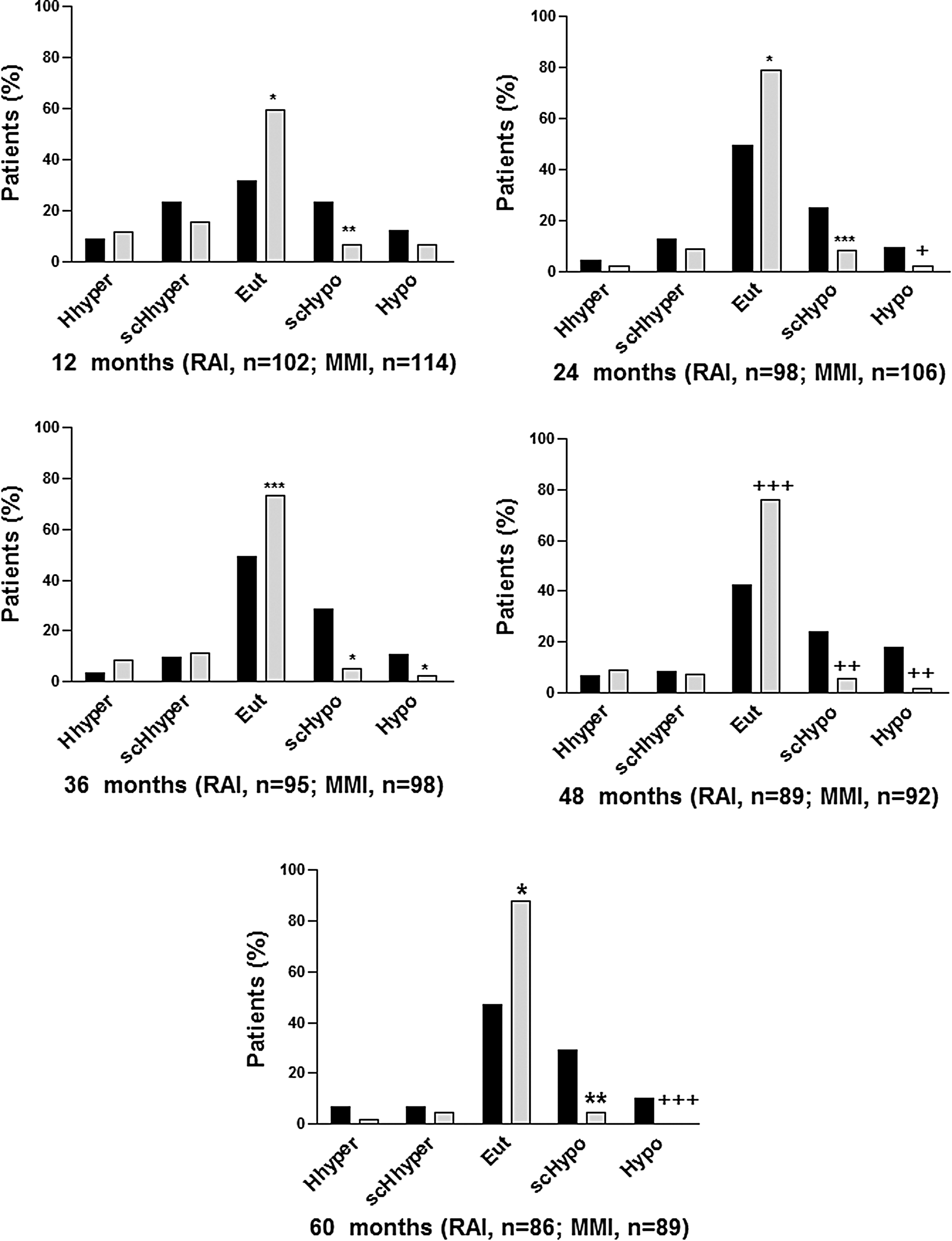
Percentage of patients with thyroid dysfunction during the follow-up of Graves' disease treatment by Fischer's exact test. Black bars, radioiodine (RAI) and L-thyroxine (LT4) treatment; gray bars, low-dose methimazole (MMI) treatment. Hhyper, hyperthyroidism; scHhyper, subclinical hyperthyroidism; Eut, euthyroidism; scHypo, subclinical hypothyroidism; Hypo, hypothyroidism. *p < 0.0001; **p < 0.001; ***p < 0.002; +p < 0.004; ++p < 0.01; +++p < 0.03.
Compliance was carefully checked at each visit, and the proportion of noncompliant patients was similar. In fact, 29.9% of the RAI group patients and 32.2% of the low-dose MMI patients reported missing at least one dose once a week of the MMI or the LT4 tablets during the entire study.
GO evolution
There were no baseline differences in GO parameters such as CAS, diplopia, eyelid width, and proptosis between the two groups (Table 1). The distribution of the outcome (improved, stable, or worsened) was more favorable in the low-dose MMI group during the long-term follow-up than it was in the RAI group (Fig. 3). As Table 2 shows, univariate logistic analysis demonstrated that smoking was the only independent factor that contributed to a lack of improvement in CAS across the entire follow-up. Age (at 12 months), RAI treatment (at 48 months), and female sex (at 24 and 36 months) were also associated with no improvement in CAS. In addition, multivariate analysis revealed that RAI treatment was also associated with no CAS improvement at 24, 36, 48, and 60 months but not at 12 months. The Kaplan–Meier analysis is shown in Figure 4. It demonstrates that worsening of GO as evaluated by CAS was more frequently (p < 0.0003) associated with RAI treatment.
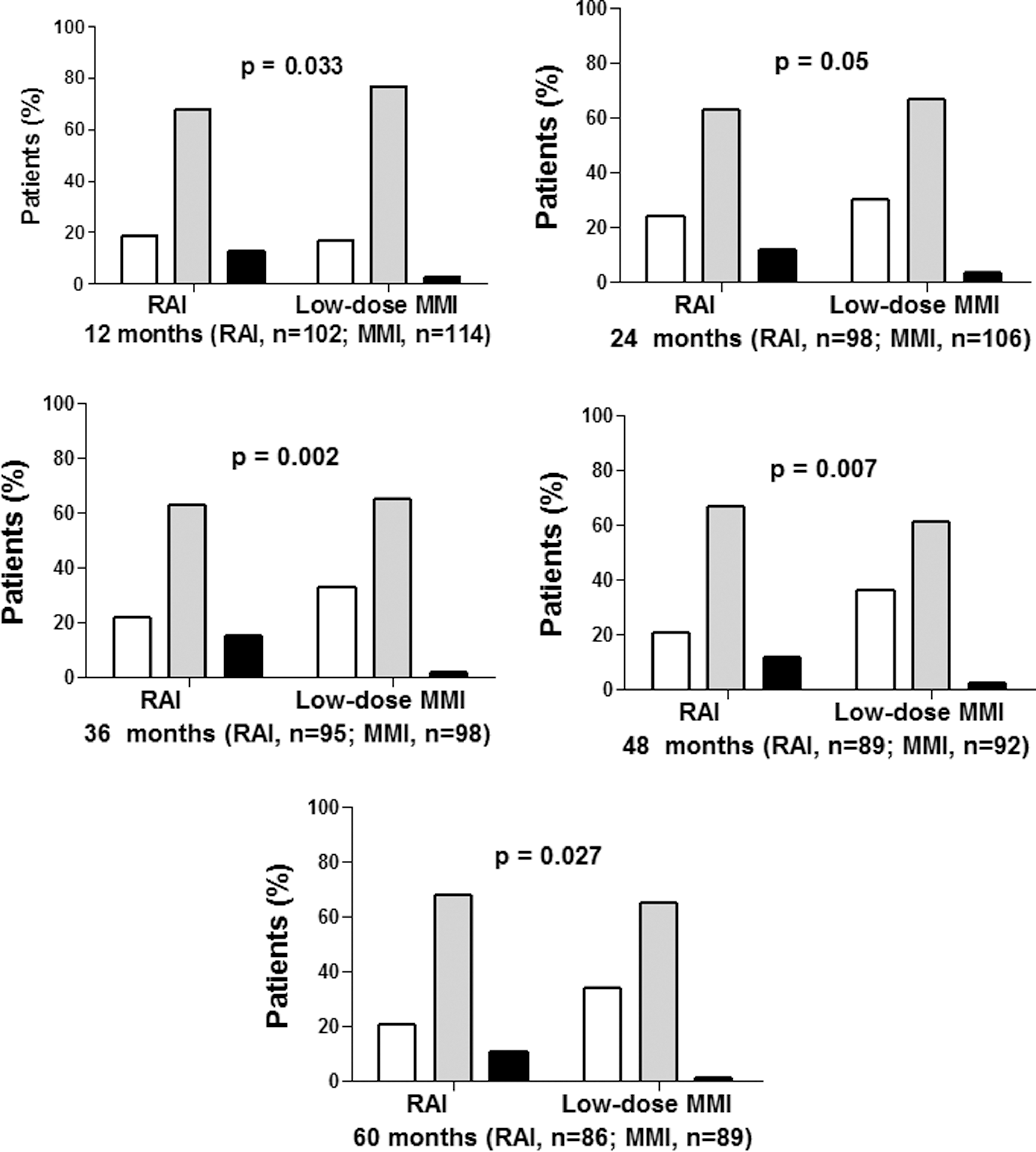
Clinical outcome of Graves' ophthalmopathy assessed by the clinical activity score (CAS) at 12, 24, 36, 48, and 60 months of follow-up in the two treatment groups. Comparison between RAI and low-dose of MMI group by chi-square test. White bars, improved; gray bars, stable; black bars, worsened.

Kaplan–Meier curve of Graves' ophthalmopathy worsening (determined by the increase of the CAS in two or more points) compared with the RAI + LT4 replacement group of 102 patients and the low-dose MMI treatment group of 114 patients. p < 0.0005.
Months of follow up.
Denotes reference group.
Body weight changes
The two groups had similar BMI and body weight at baseline. However, there was a trend to body weight increase in the RAI group during follow-up, especially at 24 months (Fig. 5).
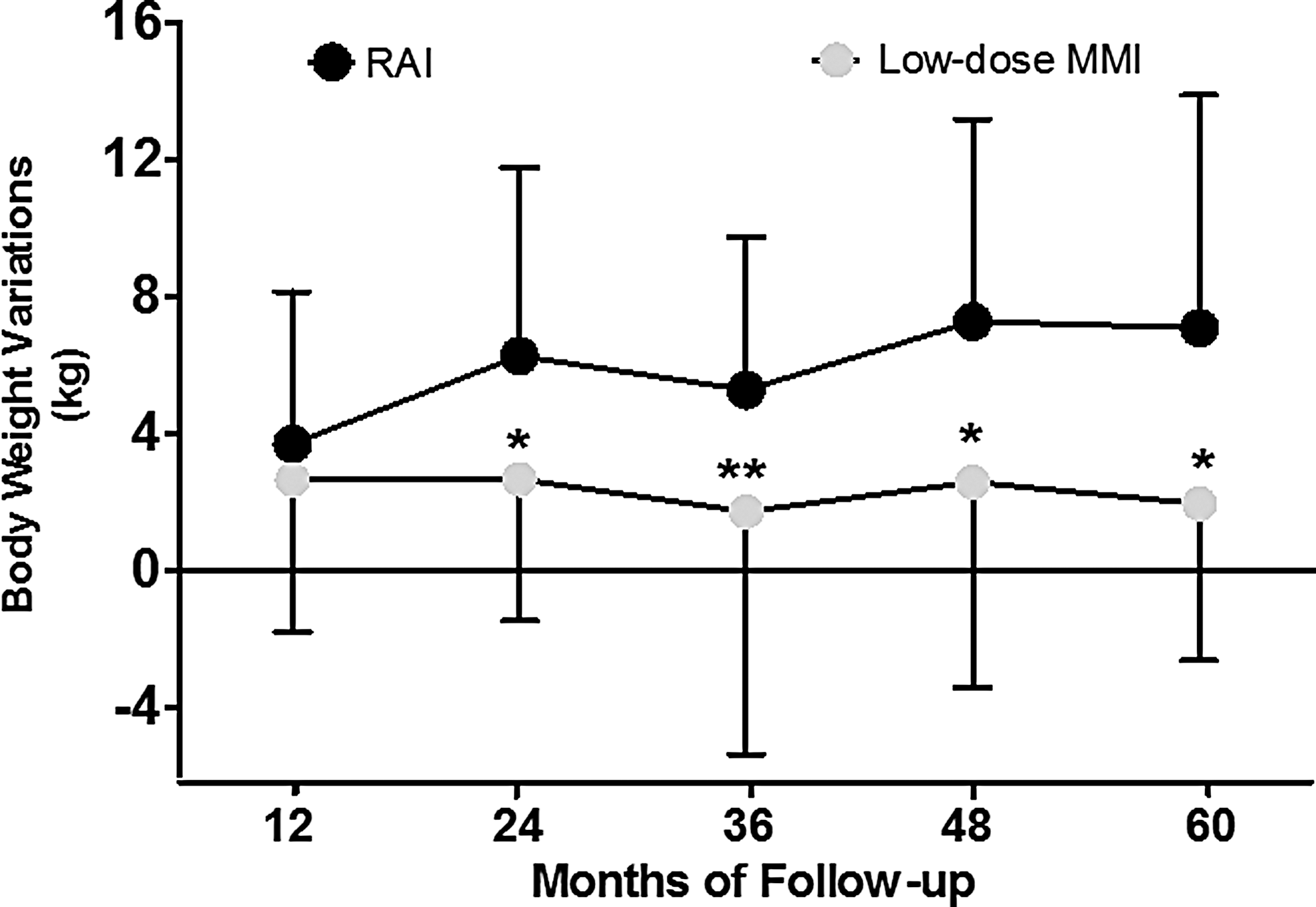
Body weight variation during follow-up and comparison between the two treatment groups. The number of patients during the follow-up periods at 12 months RAI group (n = 102) and low-dose MMI group (n = 114); 24 months RAI group (n = 98) and low-dose MMI group (n = 106); 36 months RAI group (n = 95) and low-dose MMI group (n = 98); 48 months RAI group (n = 89) and low-dose MMI group (n = 92); and 60 months RAI group (n = 86) and low-dose MMI group (n = 89). Data represent mean ± standard deviation. Mann–Whitney U-test *p = 0.0001; **p = 0.001.
QoL measurements
There were no differences in the SF-36 questionnaire results obtained at the end of follow-up in stable euthyroid patients for at least six months (RAI group: n = 63; low-dose MMI group: n = 73). Physical health scores were also similar: physical functioning 83.33 ± 20.98 (RAI group) and 83.59 ± 16.17 (low-dose MMI group); physical role functioning 70.45 ± 36.69 (RAI group) and 66.55 ± 40.08 (low-dose MMI group); body pain 67.97 ± 30.22 (RAI group) and 65.90 ± 25.60 (low-dose MMI group); and general health perceptions 70.36 ± 24.08 (RAI group) and 72.55 ± 23.36 (low-dose MMI group). Also, the mental health scores were similar: vitality 64.02 ± 23.26 (RAI group) and 66.97 ± 21.74 (low-dose MMI group); emotional role functioning 83.33 ± 21.80 (RAI group) and 81.16 ± 25.95 (low-dose MMI group); social role functioning 78.79 ± 35.18 (RAI group) and 63.85 ± 42.45 (low-dose MMI group); and mental health 74.79 ± 18.67 (RAI group) and 68.68 ± 20.86 (low-dose MMI group).
Side effects
There were no reports of major adverse effects of MMI. Five patients in the group remained hyperthyroid after six months of administration of RAI and received a second dose. Subsequently, these patients also developed hypothyroidism.
Discussion
This study demonstrates that over seven years of follow-up, the prolonged low-dose MMI treatment for GD patients who relapsed after a conventional course of ATD is safe and effective at keeping thyroid function under control. It provides a better GO outcome than RAI treatment. In fact, restoring euthyroidism is the major aim of GD treatment. However, in spite of the almost six decades of experience in the use of ATD and RAI, the approach to GD therapy is still controversial (1). In several centers, RAI treatment is the first choice and is considered safe and easy to manage, particularly in GD patients without GO. However, subclinical and overt hypothyroidism may occur months or even years after the administration of RAI. Hence, long-term follow-up of thyroid function and GO as well as management of LT4 replacement is necessary.
It was observed that the frequency of thyroid dysfunction over seven years of follow-up was significantly greater in patients treated with RAI than in patients receiving a prolonged low-dose MMI treatment. In the Colorado Study (18) and other epidemiological studies (19,20) the prevalence of euthyroidism among patients taking thyroid medication was <70%. Therefore, patients under LT4 therapy may have a risk of clinical consequences as a result of under- or overtreatment.
Drug interaction and malabsorption have been reported in patients taking LT4 (21,22). This study excluded patients taking medications that may interfere with thyroid function such as lithium, amiodarone, or chronic corticosteroids in order to avoid these confounding issues. However, noncompliance is the main problem in long-term treatments (23). Although patients from both groups had compliance problems, thyroid function remained more stable in the low-dose MMI group, probably because of the difference in drug pharmacodynamics (24).
Most importantly, during follow-up, the prolonged use of low-dose MMI was associated with a better outcome in terms of CAS. As previously discussed by Lauberg et al. (14), hyperthyroidism per se may aggravate the autoimmune activity of GD, and thyroid stimulation by elevated serum TSH may also be associated with worsening GO. In fact, MMI treatment for more than 24 months may have important effects on GO evolution, mainly because a euthyroid status improves GO and decreases serum TRAb levels (25) and other inflammatory markers (26). On the contrary, the use of RAI has been associated with progression or de novo GO in 15–30% of patients (27,28), especially in smokers and individuals with active eye disease (29,30). This study demonstrates that RAI treatment, even in patients with mild GO, has a negative long-term effect regardless of the stage of the eye disease (progression or stability). Patients treated with RAI had a worse GO outcome with increasing CAS values, despite initial mild GO and previous ATD treatment.
RAI treatment was 3–20 times more likely to be associated with no improvement of CAS compared with low-MMI dose treatment. The differences in patient numbers in the two groups can explain differences between univariate and multivariate analyses during the follow-up, and the parameters evaluated (treatment, sex, smoking, TRAb, age at diagnosis, initial CAS, TSH, and fT4) affect the multivariate analyses. Using multivariate logistic analysis and stepwise procedures diminishes or avoids misinterpretation due to confounding factors, and only the variables with the highest correlation with the final outcome are identified.
Some studies have demonstrated that patients with hyperthyroidism have impaired QoL, which persists many years after treatment (9). The treatment modality per se can influence the final outcome, and there are possible confounders such as GO (31 –33), autoimmunity (9), and current thyroid function, even in subclinical forms, that can interfere with the final QoL result (34,35). The QoL of relapsed GD patients has rarely been studied, especially when comparing two different treatment regimens. To determine if the treatment type could influence QoL, only patients with stable euthyroidism (at least for six months) were submitted to SF-36 questionnaires. Similar to what has been previously described, no differences in QoL related to the treatment modality were identified (36). However, it should be pointed out that patients had mild GO—a factor that may influence QoL, sometimes even more than thyroid status (37). On the other hand, all patients submitted to the SF-36 questionnaire were in stable euthyroidism for at least six months, and thus the usual confounders influencing this type of evaluation were diminished.
None of the patients using a low-dose of MMI developed any relevant side effect. However, 12 out of the initial cohort of 423 patients developed some side effects (skin reaction and arthralgia). The most serious side effects (agranulocytosis and severe hepatoxicity) usually occur within the first three to six months after initiation of therapy; they are extremely rare in patients with continuous use of ATD particularly after one year. Nakamura et al. (38) reported only one case (0.13%) after one year of MMI therapy in a series of 754 cases of agranulocytosis. In addition, the development of agranulocytosis after the first six months of MMI therapy is mostly associated with periods of discontinuation and reintroduction. It is extremely rare with continuous use of MMI (12,14,15).
The reasons for the change in body composition during treatment of GD are controversial, and there are few studies on this matter. Overall, an increase of 2.5–16% of body weight has been described (39). One hypothesis is that during the hyperthyroid state, a disturbance occurs in the neurochemical regulation of appetite and body weight regulation. It is possible that the central control of appetite does not signal the reduction of metabolism during the treatment of hyperthyroidism and the restoration of euthyroidism (39). Another possibility may be that the response of resting energy expenditure that could be affected by small serum TSH elevations is likely associated with significant changes in body weight and adiposity (40). In the present study, RAI treatment was associated with increases in body weight, particularly after 24 months of follow-up. Knudsen et al. (41) demonstrated that small increases in serum TSH levels can influence the prevalence of obesity. An alternative explanation for the present finding is that there was a larger number of subclinical and overt hypothyroid individuals in the group of RAI-treated patients that may associated with body weight gain.
The strengths of the present study include the sample size, the large follow-up period, the inclusion of a RAI-treated patients for comparison, the assessment of thyroid dysfunction, the careful evaluation of GO, QoL assessment, and body weight measurements during the follow-up rather than just the final clinical outcome. The main limitation is the retrospective nature of the study and the fact that all patients were treated by thyroid experts, which could lead to some sort of bias.
In conclusion, use of prolonged low-dose MMI treatment may be a viable therapeutic alternative for relapsed GD patients, particularly in GO or patients who are opposed to ablative treatment with RAI or surgery.
Footnotes
Acknowledgments
We thank Cleide A. Moreira Silva, Statistician, Research Commission Epidemiology, and University of Campinas, Brazil, for provided statistical advice and revising the manuscript.
Author Disclosure Statement
The authors having nothing to disclose.