
Abstract
Background:
Cyclooxygenase (COX-2) has been associated with tumor growth and metastasis in several cancers, including thyroid cancer. For this reason, several investigators have studied COX-2 inhibitors in preclinical models of thyroid cancer and found antineoplastic effects. Thus, the primary aim of this study was to assess if the use of nonsteroidal anti-inflammatory drugs (NSAIDs) is associated with a reduced incidence of thyroid cancer. A second aim of the study was to determine additional risk or protective factors for thyroid cancer.
Methods:
Three large prospective population-based studies (the NIH-AARP Diet and Health Study; the Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial; and the U.S. Radiologic Technologists Study) were pooled to investigate the association between self-reported frequency of aspirin and nonaspirin NSAID use one year prior to baseline (no use, ≤2/week, >2–6/week, and ≥7/week) and subsequent risk of thyroid cancer. A Cox regression proportional hazard model was used to estimate aggregated hazard ratios (HR) adjusted for cohort, sex, race/ethnicity, weight, smoking status, and alcohol intake.
Results:
There were 388,577 participants in the pooled cohort, with 481 cases of thyroid cancer. No significant risk reduction was observed with regular use of nonaspirin NSAIDs (HR = 1.14 [confidence interval (CI) 0.84–1.55]), and/or regular use of aspirin (HR = 1.06 [CI 0.82–1.39]). The multivariate regression analysis confirmed as previously reported in the literature that female sex, obesity class I (body mass index [BMI] = 30–34.99 kg/m2), and obesity class II (BMI = 35–35.99 kg/m2) were independently associated with an increased thyroid cancer risk. Current smoking status and moderate and excessive alcohol use were also confirmed as independent risk factors associated with a reduced thyroid cancer risk.
Conclusions:
Neither nonaspirin NSAIDs nor aspirin use is associated with a reduced risk of thyroid cancer. Women and obesity are associated with an increased risk of thyroid cancer, whereas smoking and alcohol use are associated with decreased risk of thyroid cancer.
Introduction
T
Cyclooxygenase-2 (COX-2) has been closely associated with tumor growth and metastasis in a number of cancers such as lung, breast, colorectal, and cervical cancer (3,4).
Patients with chronic lymphocytic thyroiditis were three times more likely to have thyroid cancer, suggesting an association between chronic inflammation and cancer development (5,6). Overexpression of COX-2 has been observed in thyroid follicular cells of patients with Hashimoto's thyroiditis but not in normal thyroid or multinodular goiter tissue (7,8). Several studies have demonstrated an overexpression of COX-2 in papillary thyroid cancer (PTC) compared with normal thyroid and multinodular goiter tissue (7,9,10).
In addition, the expression of COX-2 is associated with older age, lymph node metastasis, and advanced stage in patients with thyroid cancer (11,12). In vitro studies of thyroid cancer cell lines have shown that a selective inhibitor of COX-2, NS-398, can inhibit proliferation (13), and reduce cellular migration and invasion (14). In esophageal cancer, COX-2 expression has also been shown to be associated with anti-apoptosis (15). These findings suggest a role of COX-2 in thyroid cancer development, and the potential of COX-2 as a chemopreventive and therapeutic target. This approach has been studied most notably in colorectal cancer. Chan et al. analyzed a large prospective cohort study of 82,911 women enrolled in the Nurses' Health Study and reported a multivariate relative risk (RR) of 0.77 [confidence interval (CI) 0.67–0.88] among women with regular long-term aspirin use. The use of aspirin and the multivariate RR was also found to be dose dependent, and a similar trend was seen for NSAIDs as well (16). Given the findings of in vitro studies and the promising results of this study in colorectal cancer, aspirin and NSAID use may reduce thyroid cancer incidence.
While the evidence strongly supports the chemopreventive effect of NSAIDs in colorectal cancer (17), there is no population-based study that addresses whether NSAIDs may reduce the risk of thyroid cancer. It was hypothesized that the incidence of thyroid cancer would be lower in individuals taking NSAIDs. Therefore, the primary objective of this study was to evaluate whether NSAID use reduces the risk of thyroid cancer in a large prospective population-based cohort.
Materials and Methods
Data sources
The data source consisted of three National Cancer Institute (NCI) cohorts: (i) the National Institutes of Health-the American Association of Retired Persons Diet and Health Study (NIH-AARP); (ii) the Prostate, Lung, Colorectal and Ovarian (PLCO); and (iii) the U.S. Radiologic Technologist (USRT) Study. Each cohort met the following criterion: individual assessment of aspirin and nonaspirin NSAID use within a similar time frame. Each cohort had individual questions for the use of aspirin and nonaspirin NSAID use. The three studies all had Institution Review Board approval at the National Institutes of Health.
NIH-AARP Study
NIH-AARP, initiated in 1995–1996, is a prospective cohort study examining the diet and lifestyle factors of AARP members aged 50–71 years in six U.S. states (California, Florida, Louisiana, New Jersey, North Carolina, and Pennsylvania) and two metropolitan areas (Atlanta, Georgia, and Detroit, Michigan). A self-administered baseline questionnaire was mailed to 3.5 million members of AARP aged 50–71 years in 1995–1996 and was returned by 617,119 individuals (17.6%) (18). In 1996–1997, a second questionnaire containing information on NSAID use was completed by 334,908 participants. The study follow-up period was from 1996 to 2003.
PLCO Cancer Screening Trial
PLCO, a multicenter trial, evaluated the effectiveness of prostate, lung, colorectal, and ovarian cancer screening with respect to disease-specific mortality (19,20). Between October 1993 and July 2001, 154,952 subjects (49.5% men) aged 55–74 years were enrolled at 10 U.S. screening centers (Washington, DC; Detroit, Michigan; Salt Lake City, Utah; Denver, Colorado; Honolulu, Hawaii; Minneapolis, Minnesota; Marshfield, Wisconsin; Pittsburgh, Pennsylvania; St. Louis, Missouri; and Birmingham, Alabama). At the initial screening, a questionnaire (completed by 96.8% of participants) was administered that included items about NSAID use. The study follow-up period was from 1993 to 2005.
USRT Study
USRT, a prospective cohort study, was designed to evaluate the health history of radiologic technologists who had been certified for at least two years by the American Registry of Radiologic Technologists between 1926 and 1980 (21,22). From 1994 to 1998, a questionnaire was sent to all living individuals (126,628 participants), which ascertained NSAID use. The questionnaire was returned by 90,972 participants (71.8%). The study follow-up period was from 1994 to 2004.
Thyroid cancer case ascertainment
The pooled population consisted of 388,577 individuals, with 481 individuals (163 male) with thyroid cancer, as ascertained by follow-up questionnaires for NIH-AARP, PLCO, and USRT. Screening protocols for thyroid cancer were not instituted in any of the three pooled protocols.
Assessment of NSAID use and aspirin use
The frequency of NSAID and aspirin use was ascertained by analyzing data from self-administered questionnaires. NIH-AARP and USRT questionnaires investigated aspirin and general nonaspirin NSAID use (USRT: Ibuprofen, Motrin, Naprosyn, Advil; NIH-AARP: generic ibuprofen, Advil, Nuprin, Motrin, Aleve, Orudis, Ketoprofen, Naprosyn, Anaprox, Feldene, Piroxicam, Clinoril, Sulindac, Indocin, Indomethacin, Relafen, Nalfon, Nambumetone, Fenoprofen). PLCO investigated specifically aspirin- and ibuprofen-containing products (Advil, Nuprin, Motrin, etc.). Participants were advised to not include Tylenol or other pain relievers in their reports. Four categories for frequency of NSAID and aspirin use within the past 12 months were created based on previous literature and analysis (23): no use (referent), no regular use (≤2 times/week), regular use less than daily (>2–6 times/week), and regular daily use (≥7 times/week). The total duration of NSAID or aspirin use was not captured in any cohort. Nonaspirin NSAID and aspirin use were both included as independent variables in the multivariate analysis.
Covariate information
All of the studies collected information regarding sex, race/ethnicity, weight and height, smoking status, and alcohol status. In order to assess whether the cohorts were comparable and appropriate to be pooled, a hazard ratio (HR) of heterogeneity between studies was calculated. The HRs of heterogeneity between studies were assessed using the I2 index and the Mantel–Haenszel test for heterogeneity (24,25).
Statistical methods
A Cox proportional hazard model was used to calculate study-specific hazard ratios and confidence intervals for the association of aspirin and NSAID use with thyroid cancer risk with age as a time metric. Follow-up started at age at baseline, which was defined as the time when NSAID exposure was recorded. The follow-up ended at age at thyroid cancer diagnosis or age at censoring, which included diagnosis of any other cancer, death, or the end of the study.
The three cohorts were aggregated into one pooled cohort. Cohort-specific confounding variables were included in the final model. The NIH-AARP cohort assessed smoking status and smoking intensity by measuring cigarettes per day (never use, former use of 1–20, former use of 21–40, former use of ≥41, current use of 1–20, current use of 21–40, current use of ≥41), race/ethnicity (white, other), body mass index (BMI; 18.2 ≤ 25 kg/m2, 25 ≤ 30 kg/m2, and ≥30 kg/m2), alcohol use (g), and sex. The PLCO and USRT cohort assessed smoking status (nonsmoker, former, current), race/ethnicity (white, other), BMI, alcohol use (g), and sex.
Confounding variables were homogenized between the studies by creating common variables: smoking (nonsmoker, former, current), race/ethnicity (white, other), BMI (<25 kg/m2, 25–29.99 kg/m2, 30–34.99 kg/m2, and >35 kg/m2), and alcohol status (nondrinker, moderate <14 g, heavy >14 g). Additional analyses assessing thyroid pathology by histologic subtype were not completed given that the number of patients with thyroid cancer incidence was low. Analyses were stratified by sex, smoking status, alcohol status, and BMI.
Results
There were 388,577 individuals (200,601 male) in the pooled cohort, with 481 cases of all subtypes of thyroid cancer (163 male). A total of 4,302,158.84 person-years were accrued in the cohort analyzed. Characteristics of thyroid cancer incidence, NSAID use, and aspirin use are summarized in Table 1. Selected demographic characteristics of the cohort are summarized in Table 2. Heterogeneity of the data due to cohort variability was assessed and shown to be similar (Fig. 1).
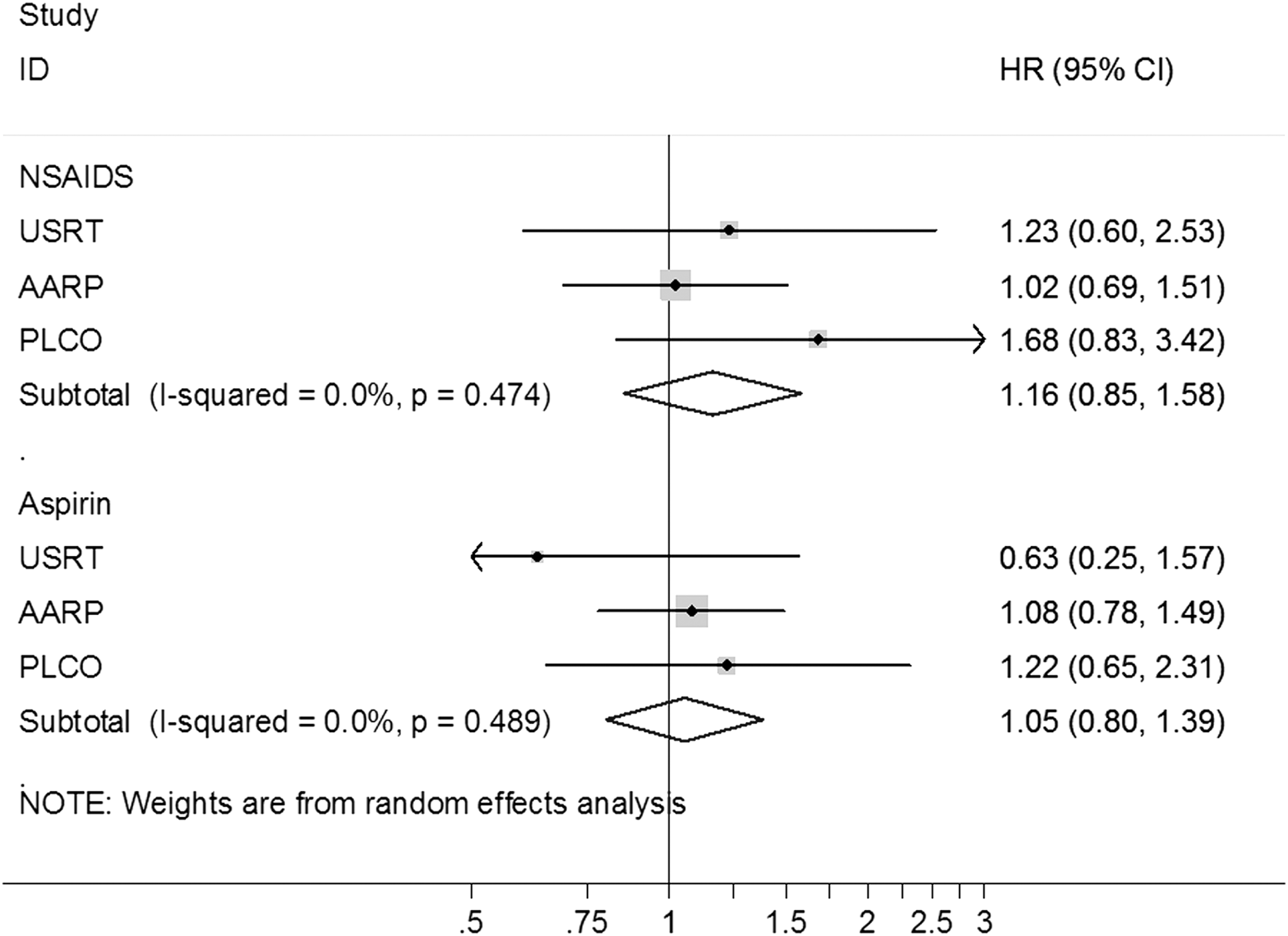
Forest plot of hazard ratios separated by cohorts for both nonaspirin nonsteroidal anti-inflammatory drugs and aspirin use. P-heterogeneity scores calculated to assess for cohort heterogeneity.
NSAIDs, nonsteroidal anti-inflammatory drugs; NIH-AARP, the National Institutes of Health-the American Association of Retired Persons Diet and Health Study; PLCO, the Prostate, Lung, Colorectal and Ovarian; USRT, the U.S. Radiologic Technologist.
BMI, body mass index.
No significant risk reduction in thyroid cancer incidence was observed with nonaspirin NSAIDs and/or aspirin use (Table 3). The independent factors (Table 4) associated with increased thyroid cancer risk confirmed by a multivariate analysis included female sex (HR 1.71 [CI 1.40–2.10], p < 0.001), obesity class I (BMI 30–34.99 kg/m2; HR 1.41 [CI 1.08–1.84], p = 0.010), and obesity class II (BMI 35–35.99 kg/m2; HR 1.69 [CI 1.21–2.36], p = 0.002). As previously documented in the literature, current smoking status and moderate and excessive alcohol use was associated with a reduced risk compared to nondrinkers (HR 0.65 [CI 0.46–0.92], p = 0.015; HR 0.78 [CI 0.63–0.97], p = 0.024; HR 0.68 [CI 0.50–0.93], respectively). USRT cohort affiliation was associated with an increased risk of thyroid cancer (HR 2.21 [CI 1.78–2.75], p < 0.001).
HR, hazard ratio; CI, confidence interval.
Bold indicates p < 0.05.
Subanalysis of risk factors did not show any lower risk of thyroid cancer with the consumption of either aspirin or NSAID. Given the relatively low incidence of thyroid cancer, a subtype analysis was not sufficiently powered and not evaluated. Data on the type of thyroid cancer and extent of disease were also not available.
Discussion
The current study is the largest prospective multicohort analysis evaluating the role of NSAID use and risk of thyroid cancer. This study shows that the use of nonaspirin NSAID or aspirin was not associated with a reduced incidence of thyroid cancer. The pooled analysis confirms the protective association of thyroid cancer incidence and smoking and alcohol use, and the higher risk of thyroid cancer associated with obesity and female sex.
Tissue analysis of thyroid cancer has shown that COX-2 expression is upregulated in patients with thyroid cancer compared with adjacent normal thyroid tissue (10), and these findings were validated with immunohistochemistry findings showing COX-2 expression to be higher in patients with PTC (26). Furthermore, chronic inflammation with increased expression of COX-2 has been associated with cancer (27) and PTC (5,6). Thus, it was postulated that NSAID use could potentially reduce inflammation and reduce the risk of cancer, as demonstrated in colorectal cancer (16,28). Therefore, NSAID use could potentially reduce the risk of thyroid cancer, which has financial and health-related consequences. However, the present analysis did not reveal a reduced risk of thyroid cancer with NSAID use in a population-based cohort study. This may be due to many factors including an older median age of the cohort, short duration of known NSAID use, an insufficiently large enough study cohort given the low incidence of thyroid cancer in these three pooled cohorts, and relatively short duration of follow-up period. In the Nurses' Health Study, Chan et al. did not see a relative risk reduction of colorectal cancer incidence until patients were ingesting aspirin or NSAIDs for at least a decade (16). The lack of screening and the indolent natural history of thyroid cancer may have confounded the results.
The increasing incidence of thyroid cancer has been associated with the detection of occult disease by numerous authors. Udelsman et al. showed that the incidence rates were significantly correlated with the density of endocrinologists and the employment of cervical ultrasonography (29). Access to care is associated with the incidence of PTC, as documented by Morris et al. in an analysis of the Surveillance, Epidemiology, and End Results (SEER) database. In that study, thyroid cancer incidence was significantly higher in those over older than 65 years of age (annual percentage change 8.8%) compared with those younger than 65 (annual percentage change 6.4%) who do not have universal healthcare (30). Increasing access to healthcare may explain the negative association with obesity. Obesity may be a surrogate for increased use of healthcare resulting in an increased incidence of thyroid cancer due to increased imaging use. Morbidly obese patients have an 81% greater per capita healthcare expenditure compared with normal-weight adults. Among the reasons for increased expenditures, morbidly obese adults had increased office-based visits and outpatient hospital care (31). Likewise, smoking and alcohol may be associated with a lowered incidence by a lower healthcare access or use by that subset of patients. The lack of association between NSAID use and thyroid cancer incidence might be explained by the presence of these confounding factors. Nevertheless, the protective effects of smoking and alcohol have to be weighed against the well-documented known associated diseases, especially given the low morbidity of thyroid cancer and excellent prognosis for early stage disease.
Radiation exposure may be a confounding variable, since the USRT cohort was included in this pooled analysis. However, an analysis of these patients with occupational radiation exposure has shown that total duration of occupation, employment below the age of 20, and years performing diagnostic, therapeutic, and nuclear medicine procedures was not associated with thyroid cancer incidence (32). The USRT cohort has also been compared to age-specific, sex-specific, and race-specific matched individuals in the SEER program. The incidence of thyroid cancer is increased, but has been attributed to this population having increased access to imaging studies. An analysis showed that the frequency of thyroid tumors ≤1 cm was twice as high in the USRT cohort (30% vs. 15%) compared with data obtained from the SEER tumor registries. Furthermore, larger thyroid tumors (1.5–2.5 cm) were found in 19% of participants in the USRT cohort compared with 28% of registrants in the SEER database (21). Therefore, occupational radiation exposure in the USRT cohort was unlikely to have compromised the pooled analysis results.
In summary, the use of NSAIDs was not associated with a reduced risk of thyroid cancer. The data analysis confirms, as previously reported in the literature, that obese patients have a higher risk of thyroid cancer, and that current smoking and moderate alcohol use are associated with a lower risk of thyroid cancer. Therefore, contrary to the chemopreventive effects of NSAIDs in colorectal cancer, the present analysis does not support the use of NSAIDs to reduce the risk of thyroid cancer.
Footnotes
Acknowledgments
The authors would like to acknowledge the staff and data managers who have worked to establish the PLCO, NIH-AARP, and USRT databases. The authors would like to acknowledge David Venzon for his statistical assistance. We are indebted to the participants in the NIH-AARP Diet and Health Study for their outstanding cooperation. We also thank Sigurd Hermansen and Kerry Grace Morrissey from Westat for study outcomes ascertainment and management and Leslie Carroll at Information Management Services for data support and analysis. This research was supported in part by the Intramural Research Program of the NIH, National Cancer Institute.
Cancer incidence data from the Atlanta metropolitan area were collected by the Georgia Center for Cancer Statistics, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta, Georgia. Cancer incidence data from California were collected by the California Cancer Registry, California Department of Public Health's Cancer Surveillance and Research Branch, Sacramento, California. Cancer incidence data from the Detroit metropolitan area were collected by the Michigan Cancer Surveillance Program, Community Health Administration, Lansing, Michigan. The Florida cancer incidence data used in this report were collected by the Florida Cancer Data System (Miami, Florida) under contract with the Florida Department of Health, Tallahassee, Florida. The views expressed herein are solely those of the authors and do not necessarily reflect those of the FCDC or FDOH. Cancer incidence data from Louisiana were collected by the Louisiana Tumor Registry, Louisiana State University Health Sciences Center School of Public Health, New Orleans, Louisiana. Cancer incidence data from New Jersey were collected by the New Jersey State Cancer Registry, The Rutgers Cancer Institute of New Jersey, New Brunswick, New Jersey. Cancer incidence data from North Carolina were collected by the North Carolina Central Cancer Registry, Raleigh, North Carolina. Cancer incidence data from Pennsylvania were supplied by the Division of Health Statistics and Research, Pennsylvania Department of Health, Harrisburg, Pennsylvania. The Pennsylvania Department of Health specifically disclaims responsibility for any analyses, interpretations or conclusions. Cancer incidence data from Arizona were collected by the Arizona Cancer Registry, Division of Public Health Services, Arizona Department of Health Services, Phoenix, Arizona. Cancer incidence data from Texas were collected by the Texas Cancer Registry, Cancer Epidemiology and Surveillance Branch, Texas Department of State Health Services, Austin, Texas. Cancer incidence data from Nevada were collected by the Nevada Central Cancer Registry, State Health Division, State of Nevada Department of Health and Human Services, Las Vegas, Nevada.
Author Disclosure Statement
No competing financial interests exist.