
Abstract
Background:
The Hounsfield unit (HU) ratio of thyroid nodules was assessed compared to the contralateral thyroid lobe on noncontrast computed tomography (CT) to stratify further the risk of malignancy in thyroid incidentalomas found on 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography/CT (PET/CT).
Methods:
This retrospective analysis included 82 patients who had thyroid incidentalomas on PET/CT in 2011. On PET/CT, the maximal standardized uptake value ratios of the thyroid nodule compared to liver (T/BSUV) and the HU ratios of the thyroid nodule compared to contralateral thyroid lobe (T/BHU) were calculated. Diagnostic performances of the T/BSUV and T/BHU were compared.
Results:
The area under the curve of T/BHU was higher than that of T/BSUV (0.941 vs. 0.689, p < 0.0001). The sensitivity, specificity, and accuracy of T/BHU were significantly higher than those of T/BSUV (100% vs. 77.8%, p = 0.0313; 80.0% vs. 60.0%, p = 0.0433; 86.6% vs. 65.9%, p = 0.0041, respectively). The risk of malignancy was much higher (71.1%) in nodules with a T/BHU cutoff value ≤0.68, whereas it was 0% in nodules with a T/BHU of >0.68. In this study, there were 18 nodules with nondiagnostic (n = 7) or atypia of undetermined significance or follicular lesion of undetermined significance cytologies (n = 11) after fine-needle aspiration biopsy (FNAB). When the T/BHU cutoff value was applied, three (60%) of the five nodules with a T/BHU of ≤0.68 were found to be papillary carcinomas. The remaining 13 nodules with a T/BHU of >0.68 were all benign with a risk of malignancy of 0%.
Conclusions:
T/BHU is a simple and effective parameter to stratify the risk of malignancy in thyroid incidentalomas found on PET/CT. This may be of clinical relevance in those nodules with nondiagnostic or undetermined significance cytologies upon FNAB in the scheme of current clinical practice.
Introduction
18F-F
Differentiation between malignant and benign thyroid nodules is essential for reducing unnecessary operations and determining the patient's prognosis. Although malignant thyroid nodules tend to have higher maximum standardized uptake values (SUVmax) values than benign nodules, SUVmax alone is limited in differentiating malignancy from benignity in a single nodule (13 –15). Thus, medical guidelines on the diagnosis and management of thyroid nodules, including the American Thyroid Association (ATA) guidelines amongst others, recommend US and fine-needle aspiration biopsy (FNAB) for thyroid incidentalomas detected by 18F-FDG PET imaging (16,17). However, indeterminate FNAB results are obtained in 12–20% of cases, which poses a treatment dilemma (18 –20). In most cases, repeat FNAB or diagnostic surgery is performed, even though the majority turns out to be benign. Therefore, there is a need for more accurate diagnostic techniques in order to avoid unnecessary additional invasive procedures.
The value of contrast-enhanced CT seems inconclusive in differentiating benign from malignant thyroid nodules. Thus, US is generally recommended for all incidental nodules on contrast-enhanced CT (21 –23). In contrast, thyroid scintigraphy using 123I has been used to select nodules for further diagnostic workup based on iodine metabolism within the nodules (24). Noncontrast CT is similar to thyroid scintigraphy in that a low iodine concentration in the thyroid presents as low attenuation on noncontrast CT scans (25 –28). This study investigated whether the iodine content of thyroid nodules on noncontrast CT scans taken during PET/CT imaging could further stratify the risk of malignancy in thyroid incidentalomas with focal 18F-FDG uptake.
Materials and Methods
This study was approved by the Institutional Review Board at Yonsei University College of Medicine, and the need for written informed consent was waived.
Patients
This retrospective analysis included 143 patients who had thyroid incidentalomas with focal 18F-FDG uptake upon PET/CT in 2011. Of these 143 patients, 61 were excluded for the following reasons: (a) lesions with a poor CT image quality due to beam hardening artifacts (n = 18); (b) nodules with gross calcification, which have a different risk of malignancy compared with noncalcified nodules, based on the pattern of calcification (n = 3); and (c) follow-up loss without further investigation (n = 40).
Finally, 82 patients (19 men; M age = 58.8 years, range 32–82 years) with a final diagnosis made on the basis of FNAB (n = 52) or surgery (n = 27) were included. There were four patients with multiple foci on PET/CT, and only one nodule with the highest FDG uptake per patient was selected for analysis. Patients with benign results upon US were followed up by US for at least 12 months (n = 3). The mean size of the 82 thyroid nodules was 16.1 mm (range 5–49 mm). PET/CT was performed for the following reasons: cancer staging (nonthyroidal cancers, n = 33), cancer surveillance (n = 32), and health screening examination (n = 17).
18F-FDG PET/CT protocol
All patients were requested to fast for at least 6 h, and blood glucose concentrations of <140 mg/dL were confirmed before the study. About 5.5 MBq of 18F-FDG per kilogram of body weight was administered intravenously. Imaging was performed using a PET/CT scanner (DSTe; GE Healthcare, Milwaukee, WI) with an axial field of view of 157 mm and a spatial resolution of 4.0 mm in full width at half maximum at 10 mm from the center. An hour after 18F-FDG injection, a low-dose CT scan was obtained for attenuation correction with an 8-slice helical CT unit (Light Speed; GE Healthcare), using the following parameters: 140 kVp, 30 mA, 0.8 s rotation time, 3.3 mm scan reconstruction, 500 mm field of view, and 512 × 512 matrix. PET imaging was then performed from the skull base to the level of the mid-thigh in a three-dimensional mode for 2 min per bed position. PET data were iteratively reconstructed using an ordered subset expectation maximization algorithm with low-dose CT data sets for attenuation correction.
Imaging and data analysis
On PET images, semi-quantitative analysis was performed by drawing a region of interest (ROI) in order to measure the SUVmax of the thyroid nodule and the SUVmean of the liver. The SUV ratios of the thyroid nodules to the liver (T/BSUV) were then calculated. On noncontrast CT images, 5 mm × 5 mm ROIs were placed over the thyroid nodule and the contralateral thyroid lobe in order to measure mean Hounsfield units (HUs) as a parameter for iodine content. Then, the HU ratios of the thyroid nodules to the contralateral thyroid lobe (T/BHU) were obtained. Finally, the additional value of T/BHU was investigated, as well as T/BSUV on top of the results of initial FNAB in reducing the need for further biopsy.
Statistical analysis
All statistical tests were conducted using MedCalc v14.8.1 (MedCalc Software, Mariakerke, Belgium). Student's t-test was used to compare T/BSUV and T/BHU values of benign and malignant nodules. Receiver-operating characteristic curve analysis was performed to obtain the cutoff values of T/BSUV and T/BHU for differentiating malignant from benign lesions. Sensitivities, specificities, and accuracies of the cutoff T/BSUV and T/BHU values were calculated. Correlated U statistics were used to compare the area under the curve (AUC) of T/BSUV and T/BHU. McNemar's test was used to compare sensitivities, specificities, and accuracies of T/BSUV and T/BHU for differentiating malignant from benign thyroid nodules. To confirm the reliability of T/BHU in nodules <10 mm, the Mann–Whitney U-test was used to compare T/BHU values between the nodules <10 mm and nodules ≥10 mm. Fisher's exact test was used to assess the performance of T/BHU according to the size of nodules. A p-value of < 0.05 was considered statistically significant.
Results
Malignant incidentalomas had significantly higher T/BSUV values than benign nodules (malignant: 2.69 ± 1.86; benign: 1.62 ± 1.15; p = 0.0019; Fig. 1). The AUC was 0.689, with the best cutoff T/BSUV value being >1.5 ([CI 0.577–0.787], 77.8% sensitivity and 60.0% specificity; Fig. 2). As a result, 6/27 malignant nodules were misclassified as benign, whereas 22/55 benign nodules were misclassified as malignant (Fig. 3).
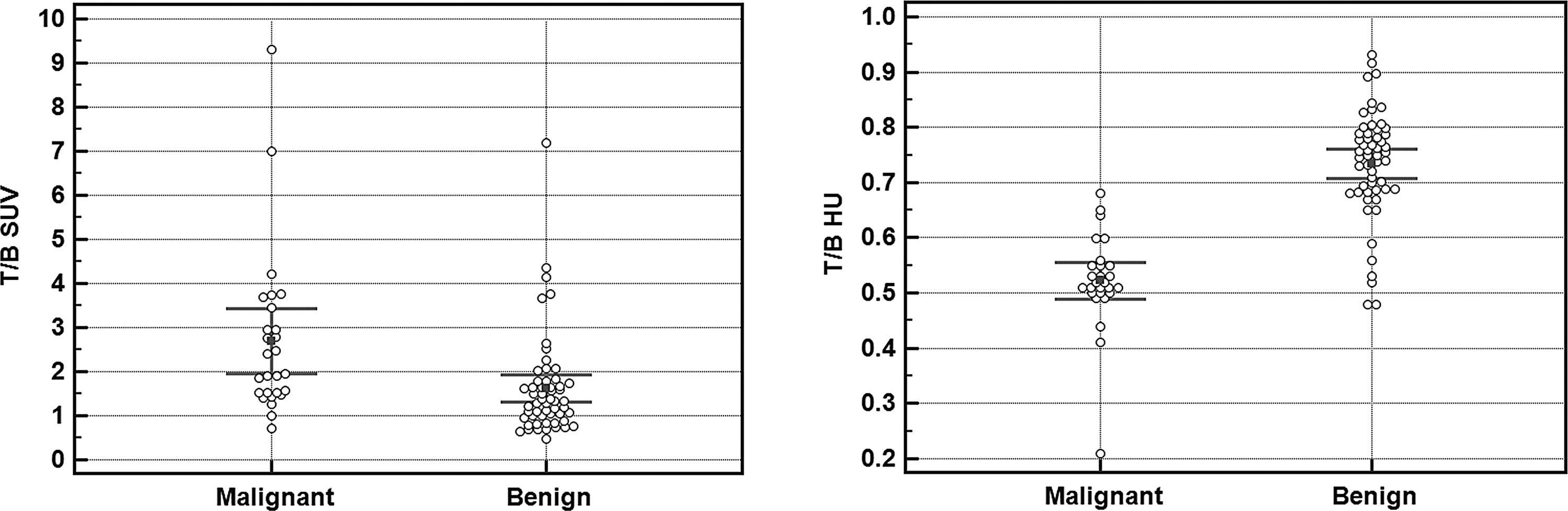
Maximal standardized uptake value ratios of the thyroid nodule compared to liver (T/BSUV) and Hounsfield unit (HU) ratios of the thyroid nodule compared to contralateral thyroid lobe (T/BHU) of malignant and benign thyroid nodules on 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT).

Receiver-operating characteristic curves of 18F-FDG PET/CT when T/BSUV and T/BHU was applied for differentiating between benign and malignant thyroid nodules. The area under the curve of T/BHU cutoff ≤0.68 was significantly higher than that of T/BSUV cutoff >1.5 (p < 0.0001).

(
In contrast, the mean T/BHU value of malignant incidentalomas was significantly lower than that of benign nodules (malignant: 0.52 ± 0.08; benign: 0.73 ± 0.09; p < 0.0001; Fig. 1). The AUC was 0.941 ([CI 0.866–0.981], 100% sensitivity and 80.0% specificity; Fig. 2). Of the 38 nodules with a T/BHU of ≤ 0.68, 27 (71.1%) were malignant and 11 were benign. The 44 nodules with a T/BHU of >0.68 were all benign (Fig. 3). Therefore, the risk of malignancy was much higher (71.1%) when a T/BHU cutoff value of ≤0.68 was applied, and it was absent in nodules with a T/BHU of >0.68.
The AUC of T/BHU was higher than that of T/BSUV (0.941 vs. 0.689, p < 0.0001). Both the sensitivity and specificity of T/BHU were significantly higher than those of T/BSUV (100% vs. 77.8%, p = 0.0313; 80.0% vs. 60.0%, p = 0.0433, respectively). In addition, there was a statistically significant difference in accuracy between the two parameters (86.6% vs. 65.9%, p = 0.0041).
There were 64 nodules ≥10 mm with a mean T/BHU of 0.67 ± 1.4, whereas there were 18 nodules <10 mm with a mean T/BHU of 0.66 ± 1.3. There were no statistically significant differences in T/BHU between nodules ≥10 mm and nodules <10 mm (p = 0.800). In nodules <10 mm, all benign nodules (n = 8) showed a T/BHU > 0.68, whereas all malignant nodules (n = 10) had a T/BHU of ≤0.68. The specificity of T/BHU seemed higher in nodules <10 mm than that in nodules ≥10 mm, although the difference was not statistically significant (100% vs. 76.6%, p = 0.188).
Finally, the potential value of T/BHU and T/BSUV in addition to the results of initial FNAB was evaluated. There were 18 nodules with nondiagnostic (n = 7) or atypia of undetermined significance or follicular lesion of undetermined significance cytologies (n = 11) upon initial FNAB in which a second FNAB was performed for further management. Of them, only one (11%) of the nine nodules with a T/BSUV of >1.5 was malignant, whereas two (22%) of the nine nodules with a T/BSUV of ≤1.5 turned out to be malignant. When the T/BHU cutoff value was applied, three (60%) of the five nodules with a T/BHU of ≤0.68 were found to be papillary carcinomas. The 13 nodules with a T/BHU of >0.68 were all benign, with a risk of malignancy of 0%.
Discussion
The risk of malignancy in thyroid cancer is significant if focal FDG uptake is found incidentally upon PET/CT. The degree of 18F-FDG uptake has been used to stratify the risk of malignancy. However, this poses a diagnostic challenge, primarily due to benign nodules with a high 18F-FDG uptake and thyroid cancers showing a low 18F-FDG uptake (13 –15). In fact, SUVmax has been shown to have a sensitivity of 70–77% and a specificity of 62–79% for differentiating incidentalomas in the literature. The results of the current study were in line with these previous reports. An AUC of 0.689 was found for T/BSUV, with the best cutoff T/BSUV value being >1.5 ([CI 0.577–0.787], 77.8% sensitivity and 60.0% specificity). As a result, 6/27 malignant nodules were misclassified as benign, whereas 22/55 benign nodules were misclassified as malignant.
In the process of dedifferentiation of thyroid cancer, the expression of genes related to iodine metabolism is reduced, while the expression of genes related to cellular proliferation and glucose uptake is increased (29 –33). Accordingly, the use of iodine metabolism in imaging modalities such as 123I thyroid scintigraphy has been utilized to select thyroid nodules for further diagnostic work-up. Nonfunctioning nodules without radioiodine uptake have a 5–10% probability of being malignant. In contrast, the risk of malignancy is extremely low in hyperfunctioning nodules with increased radioiodine uptake (24). In the present study, it was hypothesized that nodules with different functional states might have different levels of iodine concentration. Therefore, the use of T/BHU was assessed calculated from noncontrast CT scans taken during PET/CT for the differentiation of benign from malignant incidentalomas.
In the current study, there were 38 nodules with a T/BHU of ≤0.68. Of these nodules, 27 (71.1%) were malignant and 11 were benign. The 44 nodules with a T/BHU of >0.68 were all benign. With a T/BHU cutoff value of ≤0.68, the AUC was 0.941 [CI 0.866–0.981], which was higher than that of T/BSUV (0.941 vs. 0.689, p < 0.0001). Both the sensitivity and specificity of T/BHU were significantly higher than those of T/BSUV (100% vs. 77.8%, p = 0.0313; 80.0% vs. 60.0%, p = 0.0433, respectively). In general, the risk of malignancy when focal thyroid 18F-FDG uptake is found incidentally upon PET/CT has been reported to be 26–50% (5 –12). In the present study, the risk of malignancy increased to 71.1% when the T/BHU cutoff value of ≤0.68 was applied. Interestingly, no malignant nodules with a T/BHU of >0.68 were found.
The T/BHU was found to be reliable in small nodules <10 mm. There were no statistically significant differences in T/BHU between nodules ≥10 mm (n = 64) and nodules <10 mm (n = 18; 0.67 ± 1.4 vs. 0.66 ± 1.3; p = 0.800). In nodules <10 mm, all benign nodules (n = 8) showed a T/BHU > 0.68, whereas all malignant nodules (n = 10) revealed a T/BHU of ≤0.68. The specificity of T/BHU seemed higher in nodules <10 mm than that in nodules ≥10 mm without a statistical significance. In this study, 17 (27%) of the 64 nodules ≥10 mm were malignant, and 10 (56%) of the 18 nodules <10 mm were malignant. In nodules <10 mm, there were fewer benign nodules causing more false positive results with the T/BHU. The difference in the prevalence of benign nodules according to the size could explain the potential difference in specificity of T/BHU.
Although T/BHU seems to be a simple and effective method for stratifying the risk of malignancy, further studies are needed to incorporate T/BHU in the evaluation of thyroid incidentalomas with increased 18F-FDG uptake on PET/CT in routine clinical practice. Meanwhile, the additional value of T/BHU was investigated when combined with the results of FNAB. There were 18 nodules with nondiagnostic or undetermined significance after initial FNAB and 3/18 nodules were eventually found to be malignant upon a second FNAB. Of these 18 nodules, 13 had a T/BHU of >0.68 and all were benign; malignancy was found in three (60%) of the five nodules with a T/BHU of ≤0.68. Therefore, the application of T/BHU could have saved a second FNAB of benign nodules in a significant portion of the patients with nondiagnostic or undetermined significance cytology.
This study has several limitations. First, grossly calcified nodules on noncontrast CT scans were excluded, since certain calcification patterns in thyroid nodules are related to a different risk of malignancy. However, analyzing the pattern of calcification was beyond the scope of this study. Second, the imaging quality of noncontrast CT of PET/CT might be inferior to full diagnostic noncontrast CT in measuring the HUs of nodules, since only low-dose noncontrast CT scanning was performed for attenuation correction of PET/CT.
In conclusion, thyroid incidentalomas detected upon PET/CT generally indicate a high risk of malignancy and require a prompt diagnostic work-up. In the current study, it was found that T/BHU was a simple and effective parameter to stratify further the risk of malignancy in thyroid incidentalomas on PET/CT. A T/BHU value of ≤0.68 identified nodules with a higher risk of malignancy, whereas there was no malignancy in nodules with a T/BHU of >0.68. This may have clinical relevance in those nodules with nondiagnostic or undetermined significance cytologies upon FNAB in the scheme of current clinical practice. Further studies using various thyroid nodules should be performed to validate the clinical significance of these findings in a prospective way.
Footnotes
Acknowledgments
This work was partially supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP; No. NRF-2011-0030086) and the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT, and Future Planning (2012R1A1A3008042).
Author Disclosure Statement
No competing financial interests exist.