
Abstract
Background:
While the association of the BRAFV600E mutation with aggressive histopathological tumor features and clinical behavior has been extensively studied in papillary thyroid carcinoma (PTC), the BRAFK601E mutation has not been well characterized. This study reports what is currently the largest series of BRAFK601E mutated thyroid nodules.
Methods:
Histopathologic, cytologic, and molecular reports over a period of seven years (June 2007 to June 2014) were reviewed to identify thyroid cases with various types of BRAF mutations. All cases positive for the BRAFK601E mutation were reviewed to confirm histopathologic diagnosis and establish tumor variant, and clinical charts were reviewed to obtain clinical characteristics and follow-up information.
Results:
The BRAFK601E mutation was identified in 39 patients and comprised 5.3% of all BRAF mutations noted in thyroidectomy specimens. Twenty-seven out of 29 nodules (93%) with BRAFK601E mutated tumors with surgical pathology results available for review were PTC, one (3.4%) was a follicular thyroid carcinoma, and one (3.4%) was a follicular adenoma. The majority of K601E-mutant PTCs (20 cases) were follicular variant PTC. Encapsulation was present in all but one case, and one case showed capsular invasion. Coexisting mutations overall were not identified in BRAFK601E mutated thyroid nodules except in a case that exhibited a complex K601E + T599I mutation and had a classic PTC phenotype. The majority of K601E mutant nodules were T1 lesions (69%) and T2 lesions (28%) by TNM staging. With a median follow-up of 19.6 months, no structural or biochemical recurrence or metastases were found in patients with an isolated BRAFK601E mutation.
Conclusions:
The BRAFK601E mutation is the second most common BRAF mutation found in thyroid nodules. Unlike BRAFV600E , the most common mutation, K601E is strongly associated with follicular-patterned cancer, particularly with the encapsulated follicular variant of PTC, and may also be found in follicular thyroid carcinomas. Overall, BRAFK601E mutant tumors show better clinical outcomes than BRAFV600E positive tumors, and preoperative BRAFK601E analysis may provide important prognostic information for use in clinical management.
Introduction
T
The BRAF oncogene is a member of the RAF kinase family that mediates cellular signaling through the RAS–RAF–MAPK signal-transduction cascade, a pathway involved in the regulation of cell proliferation, differentiation, and apoptosis (8,9). The most common mutation is an activating mutation located in exon 15 of the B isoform of the RAF genes, resulting in a valine-to-glutamic acid substitution at amino acid 600 (BRAFV600E ) (10). Several additional, rare types of BRAF mutations have also been seen in thyroid tumors, including small in-frame deletions and insertion surrounding codon 600 and the A>G transition at nucleotide 1801, resulting in a lysine-to-glutamic acid substitution at amino acid 601, yielding the K601E variant (11 –13). Both V600E and K601E mutations are located in the activation loop of the protein between two major BRAF phosphorylation sites, T599 and S602, and lead to activation of the BRAF kinase (14). Another mechanism of BRAF activation in thyroid cancer occurs through chromosomal rearrangements such as AKAP9-BRAF (11,12,15).
The BRAFV600E mutation is most commonly found in tall-cell variant PTC (77% of cases) and conventional PTC (60% of cases), with the lowest prevalence among FVPTC (12% of cases) (16). It is usually associated with aggressive phenotypic features such as lymph node metastases, advanced stage, extrathyroidal extension, larger tumor size, male sex, multifocality, and absence of a capsule (16,17). A small number of reports on tumors carrying the BRAFK601E mutation suggest that these tumors may have a different phenotypic and likely different biological properties compared with BRAFV600E positive tumors, although only small series of tumors with this mutation have been reported so far (8,13,18).
Table 1 summarizes the series of BRAFK601E positive thyroid tumors reported to date. It is notable that the FVPTC is often reported in association with this mutation. Reported series overall tend to be small. Here, what is currently the largest series of thyroid neoplasias harboring the BRAFK601E mutation is reported, and detailed characterization of histopathologic and clinical features associated with this mutation is provided.
PTC, papillary thyroid carcinoma; PDC, poorly differentiated carcinoma; FTC, follicular thyroid carcinoma; FA, follicular adenoma.
Materials and Methods
Case selection
The study was approved by the University of Pittsburgh Institutional Review Board. Prospective determination of BRAF mutation status on thyroid cytology specimens began at the study institution in 2007. Histopathologic, cytologic, and molecular reports from June 2007 to May 2014 were reviewed to identify thyroid cases with BRAF mutations. During the study period, a total of 1117 surgical specimens (formalin-fixed paraffin-embedded [FFPE] tissue samples and fresh frozen samples) were tested for BRAF mutations.
Molecular analysis
Testing for BRAF mutations was performed using real-time polymerase chain reaction (PCR) and post-PCR melting curve analysis (June 2007–September 2013) or a next-generation sequencing panel (Thyroseq; October 2013–May 2014), as previously described (19,20). Briefly, real-time PCR with post-PCR melting curve analysis was performed on the LightCycler platform (Roche), and confirmed by Sanger sequencing of the PCR products on ABI13130 (Applied Biosystems). For targeted next-generation sequencing analysis, the custom primers were designed using a Life Technologies design tool to generate a pool of 34 primers for amplification of genomic regions of interest. It was used for amplification of isolated DNA in a multiplex PCR (Ion AmpliSeq Library Kit 2.0). Multiplexed barcoded libraries were enriched by clonal amplification using emulsion PCR on Ion Sphere particles (Ion PGM Template OT2 200 kit) and loaded on an Ion 318 Chip. Massively parallel sequencing was carried out on a Personal Genome Machine sequencer (Ion Torrent) using the Ion PGM Sequencing 200 Kit version 2, with a minimum coverage of 500×.
Review of histopathologic features
Glass slides of surgical resection of all cases positive for the BRAFK601E mutation were retrieved from the archives of the Department of Pathology, UPMC, and reviewed to confirm histopathologic diagnosis, characterize the tumor variant, and assess for other salient features.
Review of clinical information
Patient data were reviewed through the electronic medical record to summarize clinical characteristics, including date and extent of surgery, patient sex, delivered dose of radioiodine, and evidence for tumor recurrence. Determination of tumor recurrence was based on findings of the most recent physical exam, results from imaging studies (including neck ultrasound, 123I or 131I whole body scanning, positron emission tomography/computed tomography [PET/CT] scanning), or a significant rise in the thyroglobulin (Tg) level on follow-up.
Results
Molecular analysis
Molecular analysis identified a total of 45 BRAF c.1801A>G substitutions leading to p.K601E mutations, including 21 in thyroidectomy samples and 24 in fine-needle aspiration (FNA) samples obtained from 39 patients (Fig. 1). Among the 39 patients, there were 30 (77%) females and 9 (23%) males, with a mean patient age of 50.3 years (range 23–86 years). Among the 24 FNA specimens, site-specific histologic follow-up was available in 14 cases, of which six cases had BRAF molecular testing on both FNA and surgical specimens with concordant results.
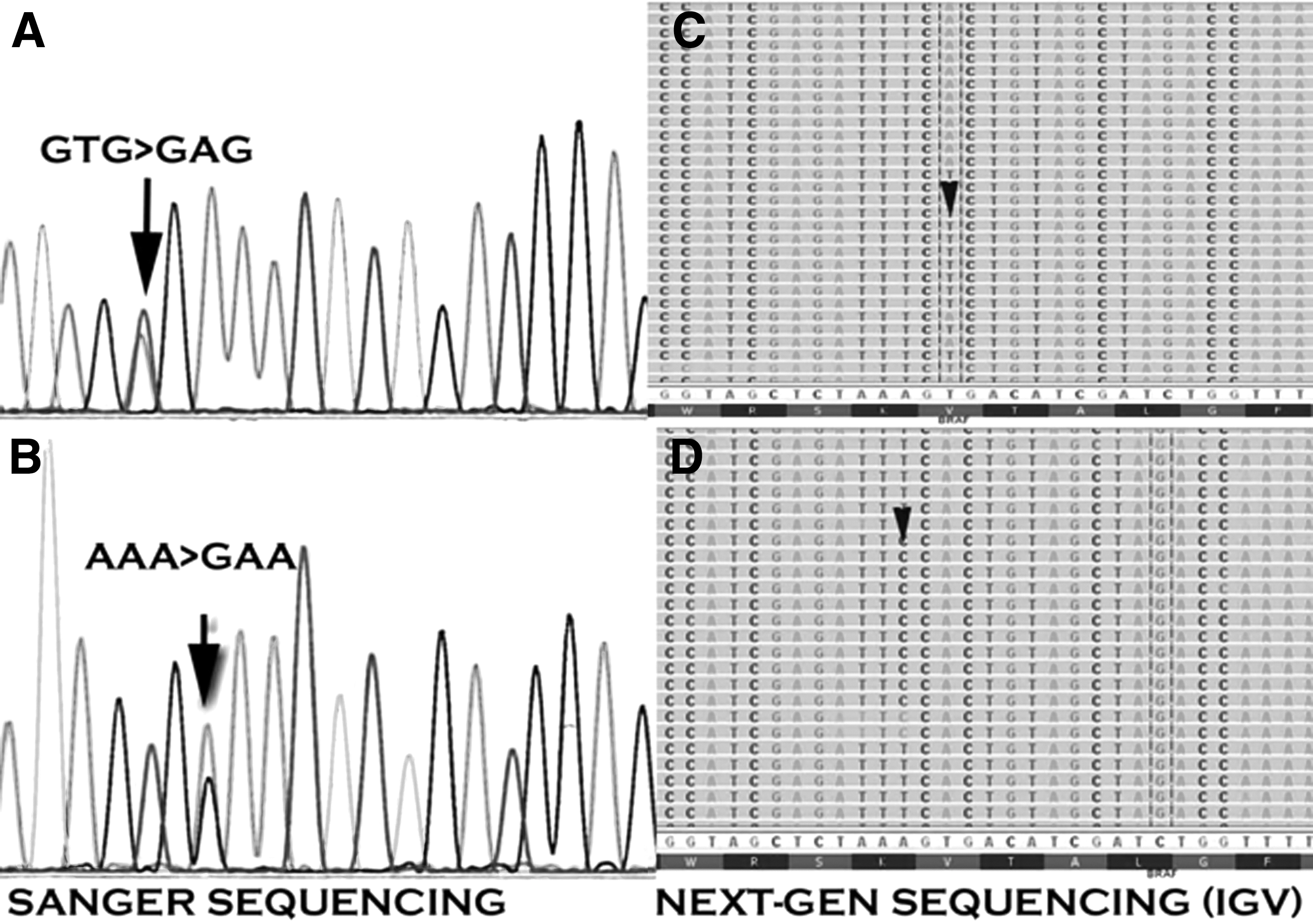
Detection of BRAF V600E and K601E mutations in thyroid samples. (
Overall, during the study period, there were 1117 thyroid surgical specimens with available molecular testing results, of which 399 cases showed BRAF mutations (35.7%). Among the BRAF mutated specimens, 373 cases (93.4%) were positive for the BRAFV600E mutation, and 21 cases (5.3%) were positive for the BRAFK601E mutation (Fig. 2).
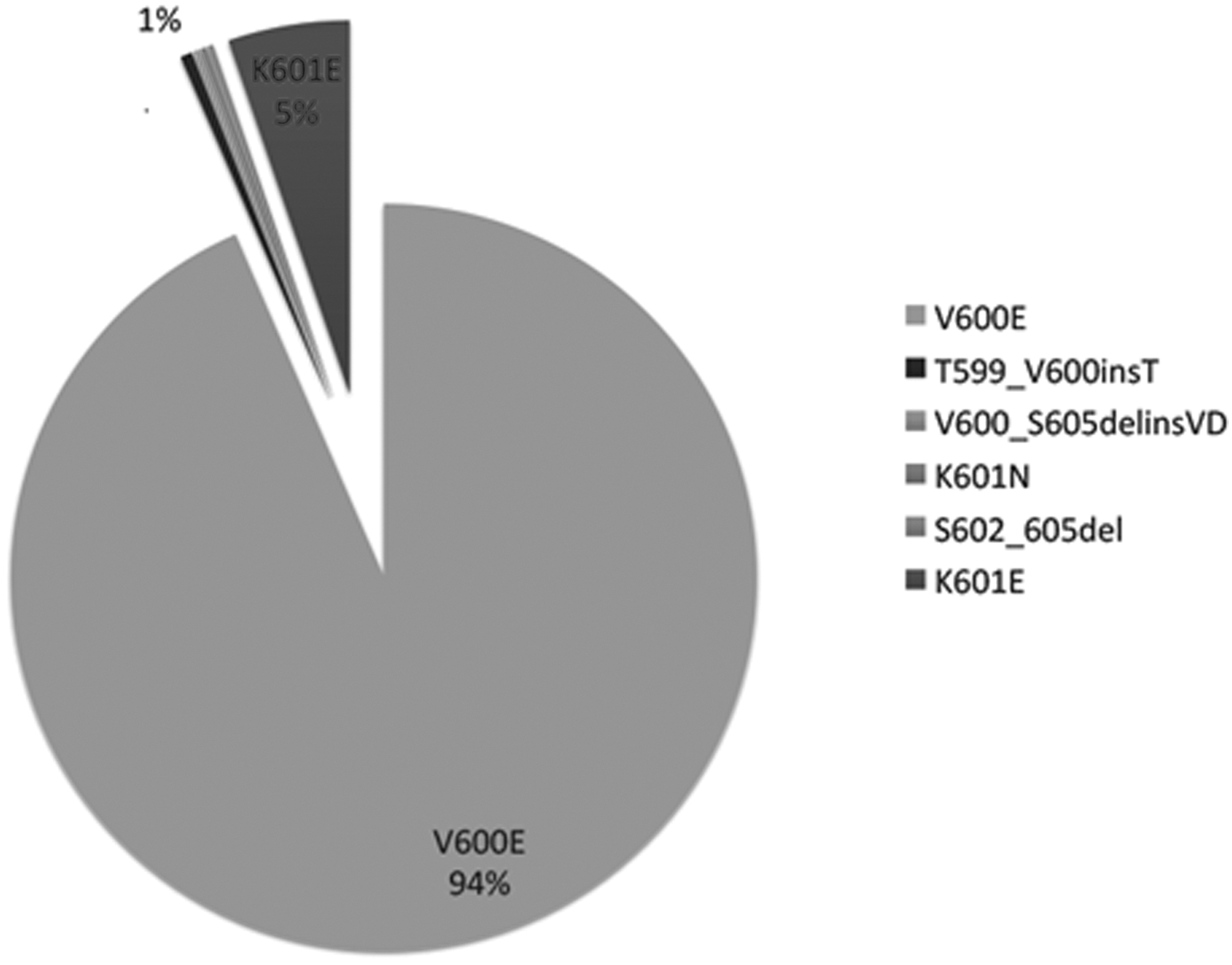
Study period results.
All study samples were tested for RAS, RET/PTC, and PAX8/PPARγ mutations, and no mutations coexisting with BRAFK601E were identified within the same thyroid nodule. One nodule had a complex BRAF mutation consisting of a T599I and a K601E substitution. In addition, in 10 patients, different nodules within the same thyroid gland were found to have other mutations, including a BRAFV600E mutation in four patients, a HRASQ61R mutation in three patients, a NRASQ61R mutation in two patients, and a KRASG12R mutation in one patient.
Correlation with histopathologic and cytologic features
Thyroidectomy specimens from 29 patients with thyroid nodules positive for BRAFK601E nodules were available for histopathological review. The size of these thyroid nodules ranged from 0.3 to 4.5 cm (M = 1.5 cm), including T1 tumors in 20 cases, T2 tumors in eight cases, and T3 tumors in one case. Histopathological diagnoses of these nodules included PTC in 27 (93%) cases, follicular thyroid carcinoma in one case, and follicular adenoma in one case (Table 2). Among the BRAFK601E mutated PTCs, the majority were FVPTCs (20 cases; 69%), and encapsulation was present in 19 of them (Fig. 3). One case of encapsulated FVPTC did exhibit capsular invasion, but no vascular invasion or extrathyroidal extension was noted. One case of unencapsulated FVPTC was identified. Five (17%) cases were microcarcinomas, all of which showed a follicular growth pattern with microfollicules and macrofollicules containing abundant colloid. One tumor was a solid variant PTC, and the one PTC that had the complex K601E + T599I was a classic PTC (Fig. 3).
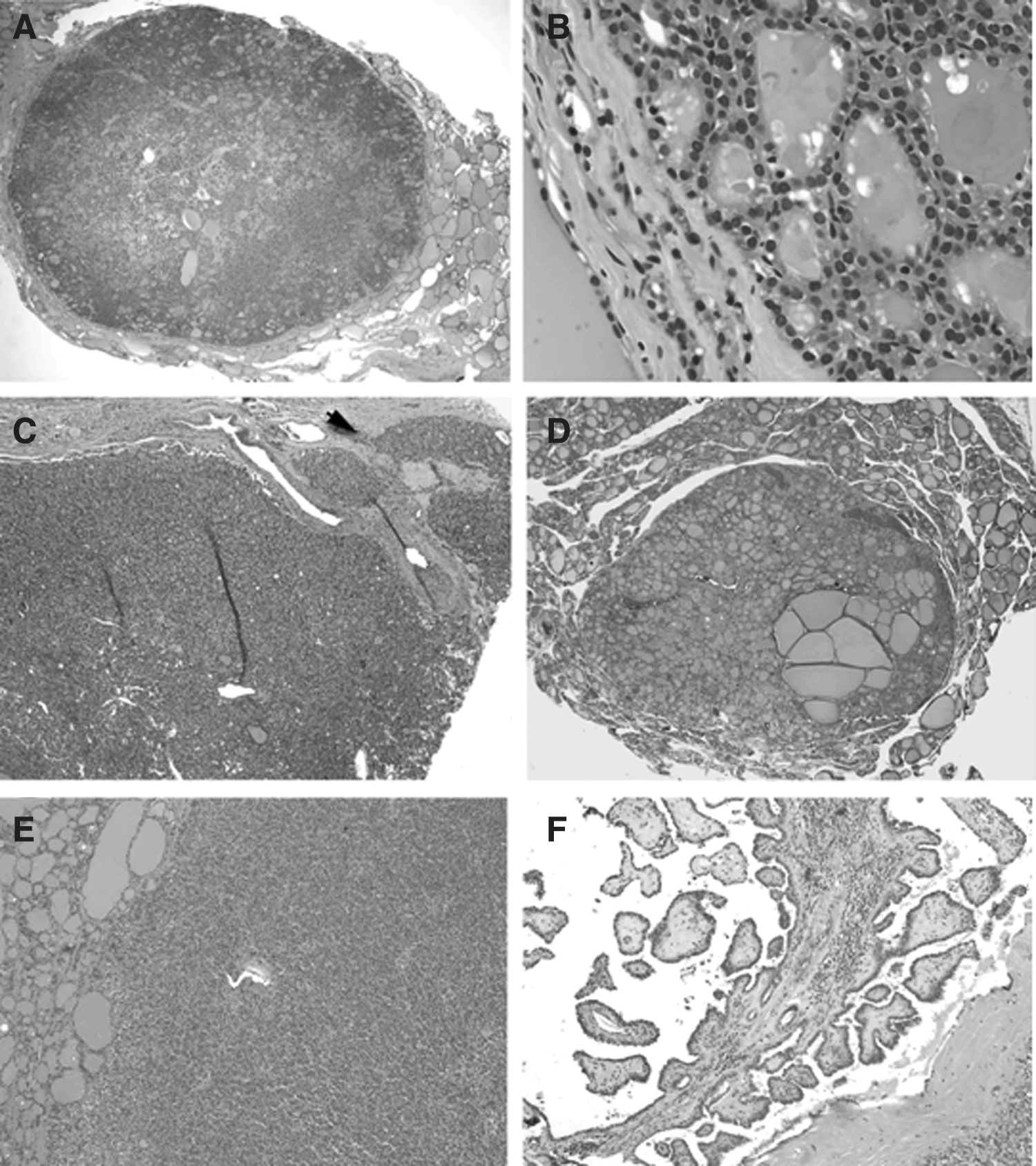
Histopathologic features of BRAFK601E
-mutated papillary thyroid carcinomas. (
Papillary thyroid carcinoma positive for a complex mutation BRAF T599I and K601E.
FN, follicular neoplasm; LUS, lesion of uncertain significance; NA, not available.
A follicular carcinoma positive for the BRAFK601E mutation had a thick capsule with microfollicular growth pattern, and revealed one focus of capsular and vascular invasion (Fig. 4). A follicular adenoma with the K601E mutation had a thin capsule and was composed of closely packed follicles in microfollicular arrangement (Fig. 4).
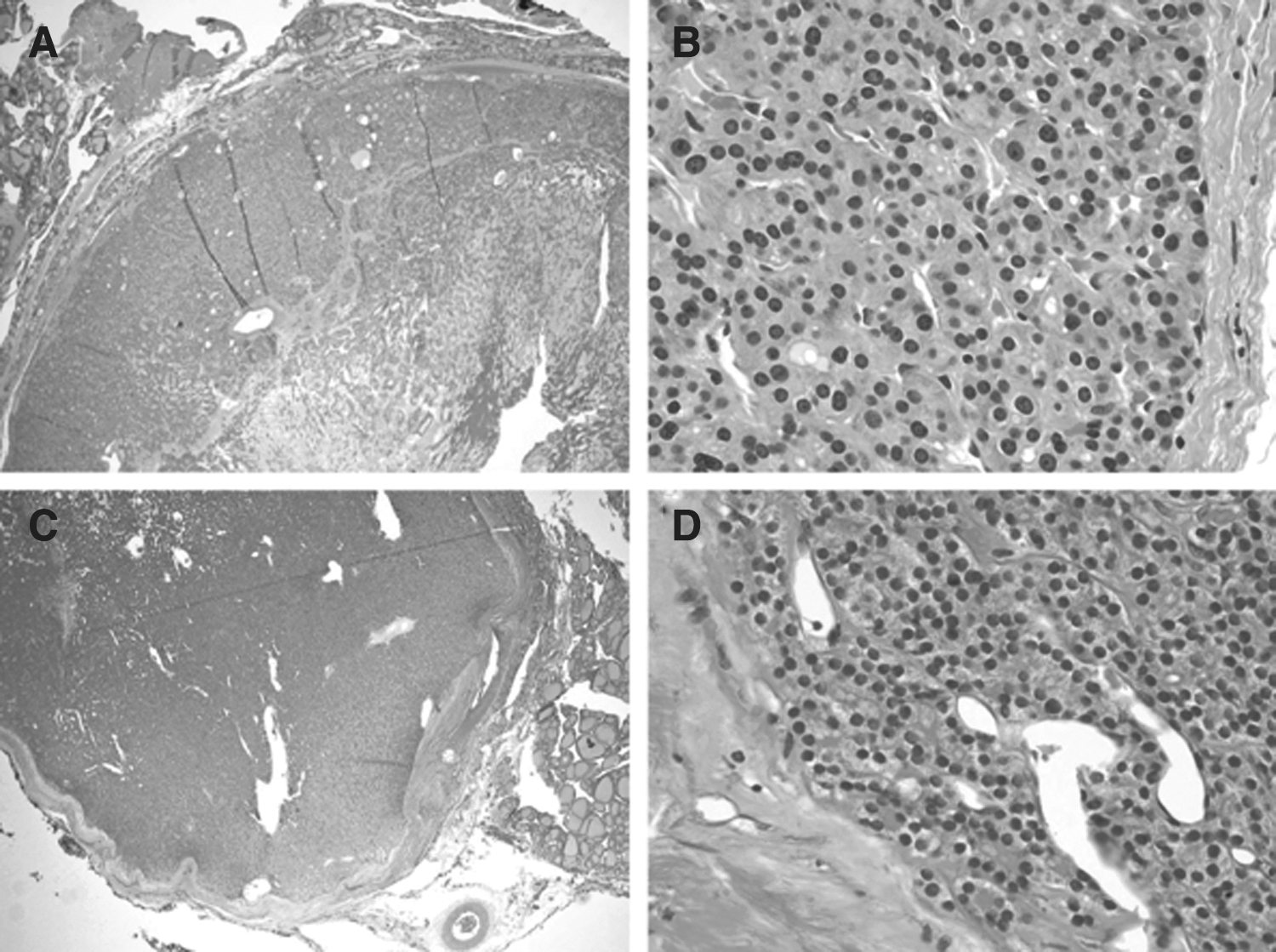
BRAFK601E
positive follicular thyroid tumors (
Preoperative FNA cytology results were available for 23 BRAFK601E mutated nodules and showed a cytological diagnosis of follicular neoplasm (Bethesda category IV) in 12 cases (52%), an atypia of undetermined significance (Bethesda category III) in 10 cases (43%), and negative for malignancy (Bethesda category II) in one case (4%).
Overall, none of the patients with an isolated BRAFK601E mutation had extrathyroidal tumor extension or lymph node metastasis. One patient had a level 3 lymph node with metastatic PTC. This patient had two PTCs, one positive for the BRAFV600E and another for the BRAFK601E mutation. The lymph node metastasis was positive for BRAFV600E .
Clinical features and follow-up findings
Of the 39 study patients, 29 underwent total thyroidectomy, either as initial surgery or as a lobectomy followed by completion thyroidectomy. Follow-up information was available in 16 of these patients. Eleven patients were treated with radioactive iodine after surgery, with doses ranging between 30 and 150 mCi, with an average dose of 74.3 mCi. Surveillance consisted of regular visits with physicians, interval imaging with neck ultrasounds, and Tg testing. In some cases, imaging also included 123I or 131I whole body scans or PET/CT scans, the latter typically done for reasons other than thyroid cancer follow-up. The median time to last follow-up was 19.6 months (range 3.7–47.3 months). No recurrences or metastases were diagnosed over the observed period in patients who had tumors positive for an isolated BRAFK601E mutation. The majority of patients maintained an undetectable Tg level. One patient was notably anti-Tg antibody positive with a measured Tg of 4.5, and another patient who did not undergo remnant ablation maintained a positive Tg of 1.6.
Discussion
BRAF mutations are common in thyroid cancer. Among them, the BRAFV600E mutation is the most common and best described. Here, a relatively large series of another BRAF mutation, K601E, is reported, and its distinct histopathologic and clinical differences from BRAFV600E positive tumors are highlighted.
The BRAFK601E mutation was detected in 1.9% of all thyroidectomy specimens in the present series. Among the BRAF mutated specimens studied, 93.4% were positive for the BRAFV600E mutation, and 5.3% were positive for the BRAFK601E mutation, identifying K601E as the second most common BRAF mutation.
The results identified typical histopathologic features of K601E positive tumors. K601E positive nodules were predominantly associated with the FVPTC variant (86% of papillary tumors in the present series, including microcarcinomas), and encapsulation was a common feature in these tumors. In this series, capsular invasion was present in only one encapsulated FVPTC. Trovisco et al. found the BRAFK601E mutation in about 7% of cases of FVPTC, as well as in a unique case of a follicular adenoma (21,22). Similarly, a recent case report from Penneli et al. detected the BRAFK601E mutation in a patient with a follicular thyroid carcinoma (23). It is notable that BRAFV600E mutations have never been reported in follicular thyroid carcinomas, where genetic alterations instead involve NRAS, HRAS, or KRAS point mutations, PAX8/PPARγ rearrangements, or PI3K/AKT pathway mutations (5,24). Here, the fourth case of a follicular carcinoma with minimal capsular and vascular invasion harboring the BRAFK601E mutation is reported (see Table 1). Similarly to Trovisco et al., the K601E mutation was also found in one case of a follicular adenoma (3.5 cm).
Clinical information available for patients with K601E positive tumors in the present series confirmed histologic features suggestive of low-grade cancer. The majority of tumors positive for this mutation were T1 lesions. Most cases showed no aggressive tumor phenotypic characteristics, such as extrathyroidal extension or metastases. The indolent behavior of these tumors was confirmed on clinical follow-up; no clinical recurrences were noted in the studied group, and the majority of patients maintained undetectable Tg levels measured on thyroxine suppression. This information is in distinct contrast to the data reported for tumors with the BRAFV600E mutation that demonstrated a high rate of radioiodine treatment failure and a higher likelihood of tumor-related mortality, even in the papillary microcarcinomas (18,25 –27).
Cytologic results in the present series were variable. While most of the studied lesions showed a cytologic diagnosis of follicular neoplasm after FNA, a substantial number of cases (47%) showed either atypia of undetermined significance or a benign cytology.
Thus, identifying a K601E positive tumor is likely to be of significant benefit in clinical management of the patient, allowing appropriate treatment and avoiding costly therapy with the potential of significant associated morbidity. Duration of follow-up is, however, short in the present study, with a median duration of 19.6 months. Despite this, in light of the observed low-risk clinical behavior of these tumors, it appears likely that most patients with nodules positive for a BRAFK601E mutation may be treated with lobectomy alone.
In summary, the results of this study demonstrate that BRAFK601E mutated thyroid nodules are associated with a distinct histologic phenotype and are associated with a better clinical prognosis than BRAFV600E positive tumors. Preoperative BRAFK601E determination may provide important information over and above routine cytologic findings to assist in appropriate (and often less aggressive) clinical management of these patients.
Footnotes
Author Disclosure Statement
Yuri Nikiforov serves as a consultant for Quest Diagnostics. The other authors have nothing to disclose.