
Abstract
Background:
Current guidelines used for establishing reference intervals for thyroid peroxidase antibodies (TPOAb), recommended by the National Academy of Clinical Biochemistry, have been a matter of controversy. The present study sought to determine TPOAb reference intervals for different age and sex groups, as well as the TPOAb cutoff points for subclinical and overt hypothyroidism in an iodine-sufficient population.
Methods:
This cross-sectional study was conducted within the framework of the prospective Tehran Thyroid Study (TTS), in which 4174 healthy euthyroid individuals were followed for 10 years. Thyroid function tests and TPOAb were assessed.
Results:
The mean age ± standard deviation of participants was 39.3 ± 15.2 years. Estimated reference intervals for TPOAb corresponding to the 2.5th and 97.5th percentiles were 1.5–32.8 and 2.1–35 IU/mL in males and females, respectively. There were no significant variations in the different age groups in either sex. The optimal cutoff points for TPOAb were 18.38 and 14.77 IU/mL for predicting clinical and subclinical hypothyroidism, respectively.
Conclusions:
This study establishes the reference intervals and the optimal cutoff points for TPOAb in an iodine-sufficient population.
Introduction
A
The aims of this study were to determine both the normal reference limits of TPOAb in an iodine-sufficient population, according to their age groups and sex, and the TPOAb cutoff points for predicting the occurrence of subclinical and overt hypothyroidism.
Materials and Methods
Study population
The present study was conducted within the framework of the Tehran Thyroid Study (TTS), a prospective population-based cohort study performed on residents of district 13 of Tehran, the capital of Iran. The aim was to evaluate the prevalence and natural course of thyroid diseases and their long-term consequences in terms of ischemic heart disease and cardiovascular and all-cause mortality in the urban, iodine-sufficient population of Tehran. Details of the study design have previously been described (15).
The subjects were recruited from the selected population, and a baseline assessment was done. This study was conducted during the first cross-sectional phase of the TTS (implemented from March 1999 to December 2001).
In brief, to determine TPOAb reference limits, of the initial 4174 individuals, aged ≥20 years who had thyroid function tests at baseline, 15 individuals were excluded because of missing TPOAb data, 59 for having thyroid surgery, 122 subjects for taking thyroid hormones, 13 for taking antithyroid drugs, 73 for taking glucocorticoids, 37 for pregnancy, 608 for abnormal thyroid function tests (100 and 273 individuals had overt and subclinical hypothyroidism, respectively; 72 and 158 individuals had overt and subclinical hyperthyroidism, respectively; 5 individuals had both free thyroxine [fT4] and TSH levels higher than the reference range), 219 individuals for being smokers, and 205 individuals with outlier data (Fig. 1). Finally, data on a total of 2823 participants without any family history of thyroid or other autoimmune diseases remained for analysis.
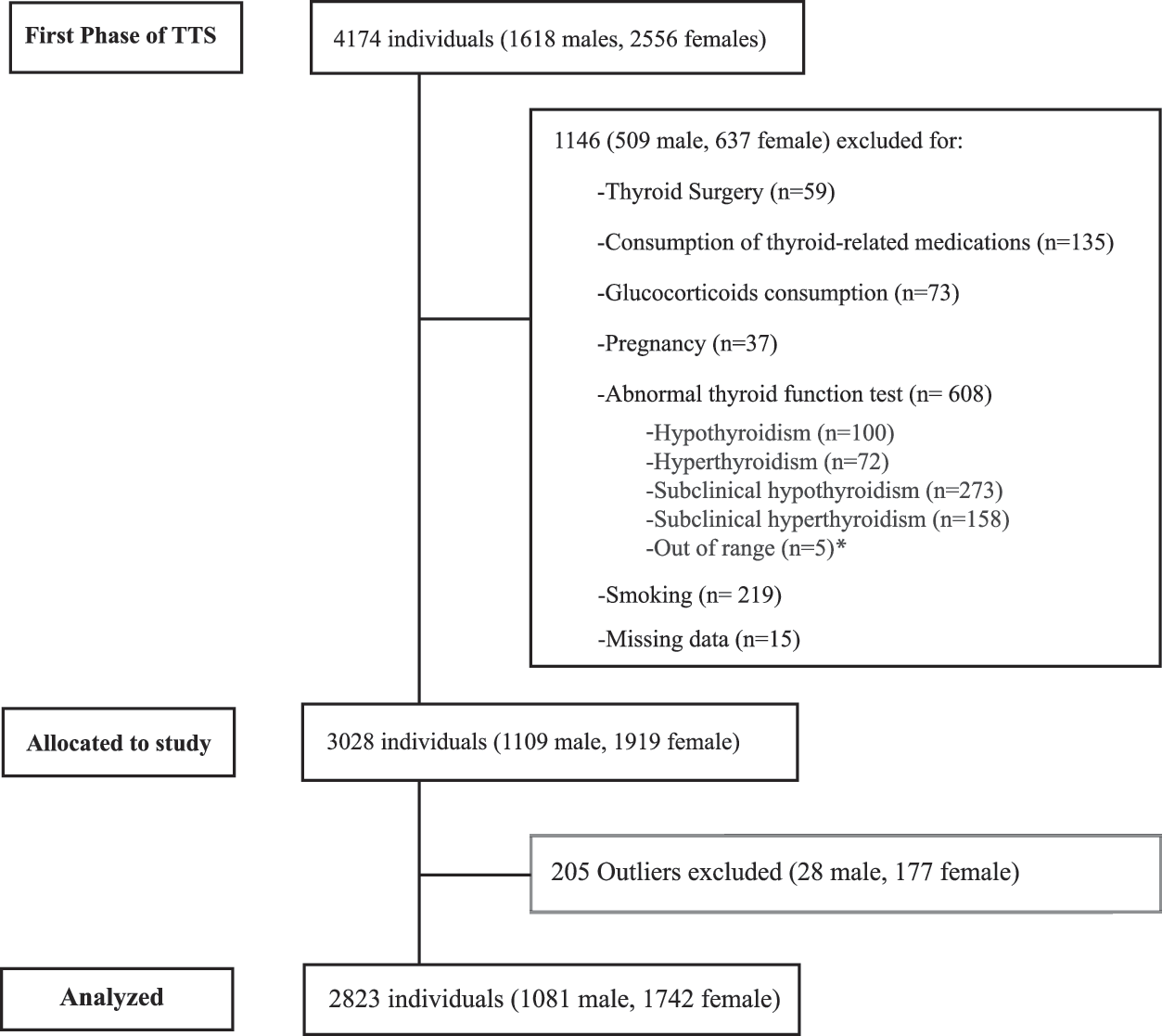
Flowchart demonstrating selection of study participants for determination of thyroid peroxidase antibodies (TPOAb) reference range, Tehran Thyroid Study. *Individuals who had both free thyroxine (fT4) and thyrotropin (TSH) levels higher than the normal reference range.
To determine cutoff points, the data of 3272 individuals were considered only if they had not had thyroid surgery; were not taking thyroid hormones, antithyroid drugs, or glucocorticoids; were not pregnant; were non-smokers; and were not hyperthyroid.
Demographic data and information regarding smoking habits, history of radioiodine ablation, thyroid surgery, and detailed medication use such as antithyroid drugs, thyroxine, or any medication interfering with thyroid function tests were documented.
Two decades ago, Iran was known to be a severely iodine-deficient country. However, salt iodization began in 1990, and universal salt iodization was implemented in 1994. In 2000, Iran was declared free of iodine-deficiency disorders by the World Health Organization/UNICEF. Ongoing monitoring national surveys in 1996, 2000, and 2006 indicated an adequate median urinary iodine concentration, with >95% of households consuming iodized salt (16).
Laboratory measurements
Fasting blood samples were drawn from all participants between 7:00am and 9:00am into vacutainer tubes at baseline and at each reassessment. Samples were centrifuged within 30–45 minutes of collection, and separated serums were stored at −70°C until analyses.
fT4 and TSH were evaluated by the electrochemiluminescence immunoasaay (ECLIA) method, using Roche Diagnostic kits and Roche/Hitachi Cobas e-411 analyzer. Lyophilized quality-control material (Lyphochek Immunoassay plus Control; Bio-Rad Laboratories) was used to monitor the accuracy of the assays. The mean values of three levels of control for fT4 was 0.89, 2.43, and 4.60 ng/dL, and for TSH these were 0.49, 5.76, and 38.43 mIU/L. Intra- and inter-assay coefficients of variation (CVs) were 1.3% (range 0.7–1.7%) and 3.7% for fT4 and 1.5% (range 1–2%) and 4.5% for TSH determinations, respectively.
TPOAb was measured by a skilled laboratory technician using a microplate enzyme immunoassay (a sequential type 1 ELISA method-AccuBind™; Monobind) and the Sunrise ELISA reader (Tecan Co.). Once all reagents, serum references, and controls reached room temperature (RT), 2–25 μL of the appropriate serum reference, control or diluted patient specimen was put into the assigned well. Subsequently, 100 μL of the TPO Biotin Reagent was added, and the microplate was gently swirled for 20–30 seconds. After the covered microplate was incubated for 60 minutes at RT, the contents of the microplate were removed by aspiration, and the washing step was repeated three times by adding and aspirating 350 μL of wash buffer, after which 100 μL of the x-TPO enzyme reagent was added to all wells in the same order without shaking. After incubation for 30 minutes at RT, the contents of the microplate were removed, and washing procedures were done as mentioned previously. Then, 100 μL of working substrate solution was added to each well without shaking, and the microplate was incubated (15 minutes at RT) followed by the addition of 50 μL of stop solution and gentle mixing for 15–20 seconds. Finally, absorbance in each well was read at 450 nm within 30 minutes of adding the stop solution. For specimens with TPOAb ≥500 IU/mL, the assay was repeated with a 1:10 diluted sample using original diluting material. The TPOAb AccuBind™ ELISA test system has a sensitivity of 0.92 IU/mL, and has been compared with a reference TPOAb ELISA microplate using specimens with both normal and diseased states. The results have shown a good correlation (r = 0.989 based on the authors' study; unpublished results). A subgroup of the samples with different ranges of TPOAb concentrations were also assayed by an electrochemiluminescence immunoasaay using the Cobas e-411 analyzer (Roche Diagnostics). The results of the two methods showed an acceptable correlation (r = 0.890). The intra- and inter-assay CVs for TPOAb assay were 3.9% (range 3.5–4.1%) and 4.7%, respectively, in the laboratory.
The ethics committee of the Research Institute for Endocrine Sciences (RIES) of Shahid Beheshti University of Medical Sciences approved the protocol for this study. Written informed consent was obtained from all subjects.
Definitions and terms
For data analysis, individuals at baseline were categorized as having subclinical hyper- or hypothyroidism according to population-based normal reference ranges. Subclinical hypothyroidism was defined as serum TSH levels >5.06 mIU/L with a normal fT4 level. Overt hypothyroidism was defined as a serum TSH level >5.06 mIU/L with a fT4 <0.91 ng/dL. Subclinical hyperthyroidism was defined as a serum TSH level <0.34 mIU/L and normal fT4 levels. Overt hyperthyroidism was defined as a TSH concentration <0.34 mIU/L with a serum fT4 concentration >1.55 ng/dL (14).
Statistical analysis
Continuous baseline demographic and clinical variables are presented as mean ± standard deviation (SD), and categorical variables are summarized as frequency and percentage. The chi-square test or Fisher's exact test were used to determine the independence of the two categorical variables. The relationship between TPOAb levels and quantitative variables in the study was explored using Spearman's correlation and partial correlation coefficients. The normal-based methodology described in Altman and Chitty (17) and Royston and Wright (18) was used to estimate age-specific TPOAb percentiles. Fractional polynomial (FP) regression models were fitted separately to estimate the mean and SD of log TPOAb values as functions of age. SD was modeled using the scaled absolute residuals from the estimated regression model for the mean. For selection of FP degrees, the likelihood-ratio test was used to compare different degrees, and based on the results, the best-fitted degrees in both sexes were different. Finally, for the male population, an FP of first degree with power 1 and a second degree FP with powers 2 and 3 were selected for the mean and SD, respectively. For the female population, FPs of first degree with power 1 were selected for both mean and SD. Sex- and age-specific percentiles were obtained by combining two regression models for mean and SD, based on the assumption that the conditional distribution of log TPOAb values at a given age is normal. The normal plot of the Z-scores from the normal model described above showed that normality does not hold (p < 0.001) for the male and female populations. As TPOAb distribution in males was skewed, the exponential-normal (EN) model was used. However, as this distribution had both skewness and kurtosis, the modulus exponential-normal (MEN) model provided a better fit for females. The deviance of both models was significantly lower than the normal model (p < 0.001), and the normal plots of the Z-scores from the EN and MEN models appeared reasonably linear. The EN and MEN models were fitted by maximum likelihood using the Stata command xriml. Prior to percentile estimation, the data regarding the outlier values were trimmed using the mcd command in Stata. Before implementing any multivariate statistical analysis based on empirical covariance matrices, it was important to check whether outliers are present because their existence could cause significant bias. In brief, the minimum covariance determinant estimator was applied, which is frequently used in robust statistics to approximate the location parameters and multivariate scales. These estimators could be easily used to produce robust Mahalanobis distances and detect outliers. Traditionally, the expected percentage of outliers existing in the data set by default is e(0.2), but it can have any value ranging from 0 to 0.5. The e(0.05) was used here for definition of the outliers in the data set based on observations (19).
The R package optimal cutoff points were used to determine the area under the receiver operating characteristic (ROC) curve for the following comparisons: (i) subclinical hypothyroidism subjects versus euthyroid healthy individuals, and (ii) overt hypothyroidism subjects versus euthyroid healthy individuals, as well as to determine the best cutoff point based on the Youden index method, along with the corresponding sensitivity, specificity, positive and negative predictive values, and positive and negative diagnostic likelihood ratios (with confidence intervals [CI] for indexes).
Results
Data collected on 2823 individuals (1081 males) were analyzed in this study. M age ± SD was 39.3 ± 15.2 years. Median TSH and interquartile range (IQR) was 1.55 (1.02–2.36) mIU/L, (median TSH for the male and female populations being 1.37 and 1.63 mIU/L, respectively), and M ± SD of serum fT4 was 1.19 ± 0.17 ng/dL. The results of this study show that the estimated reference interval for TPOAb corresponding to the range between the 2.5th and 97.5th percentiles was 1.5–32.8 IU/mL in males and 1.5–35.0 IU/mL in females. Age-specific TPOAb and its equivalent percentiles for males are given in Table 1, and corresponding values for females are shown in Table 2. With increasing age, levels of the 2.5th and 97.5th percentiles of TPOAb did not increase significantly in any age group or either sex. The 2.5th level of TPOAb in males increased from 1.27 in the 20–30 year age group to 2.64 IU/mL in the 70–80 year age group. The corresponding rise in the 2.5th percentile of TPOAb levels in females was from 1.38 to 2.15 IU/mL. The 97.5th percentile of TPOAb in males decreased from 34.15 in the 20–30 year age group to 26 IU/mL in the 70–80 year age group, and the corresponding decline in females was from 35.1 to 35.06 IU/mL respectively.
TPOAb, thyroid peroxidase antibodies.
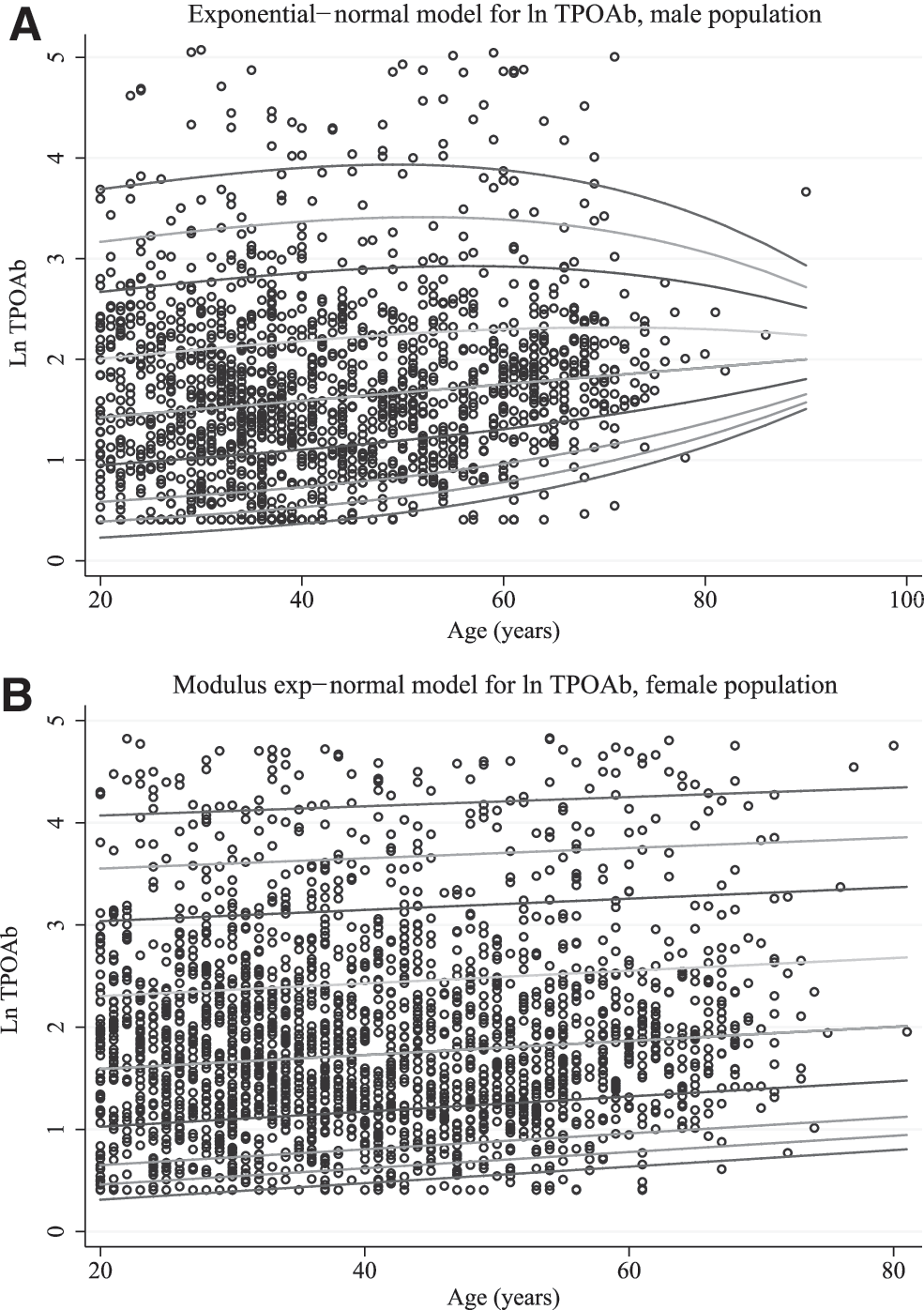
It should be noted that because the shape of the association between the average levels of TPOAb in relation to age was monotone, the median age was chose for each age interval to be representative of age class based on FP regression models. Various percentiles of TPOAb values are shown in Figure 2A and B, and illustrate log TPOAb values as a function of age along with the 2.5th, 5th, 10th, 25th, 50th, 75th, 90th, 95th, and 97.5th percentiles for male and female participants, respectively. These figures determine TPOAb distributions in a large number of individuals aged 20–80 years in an iodine-sufficient area, and they provide more data for individuals of both sexes.
(
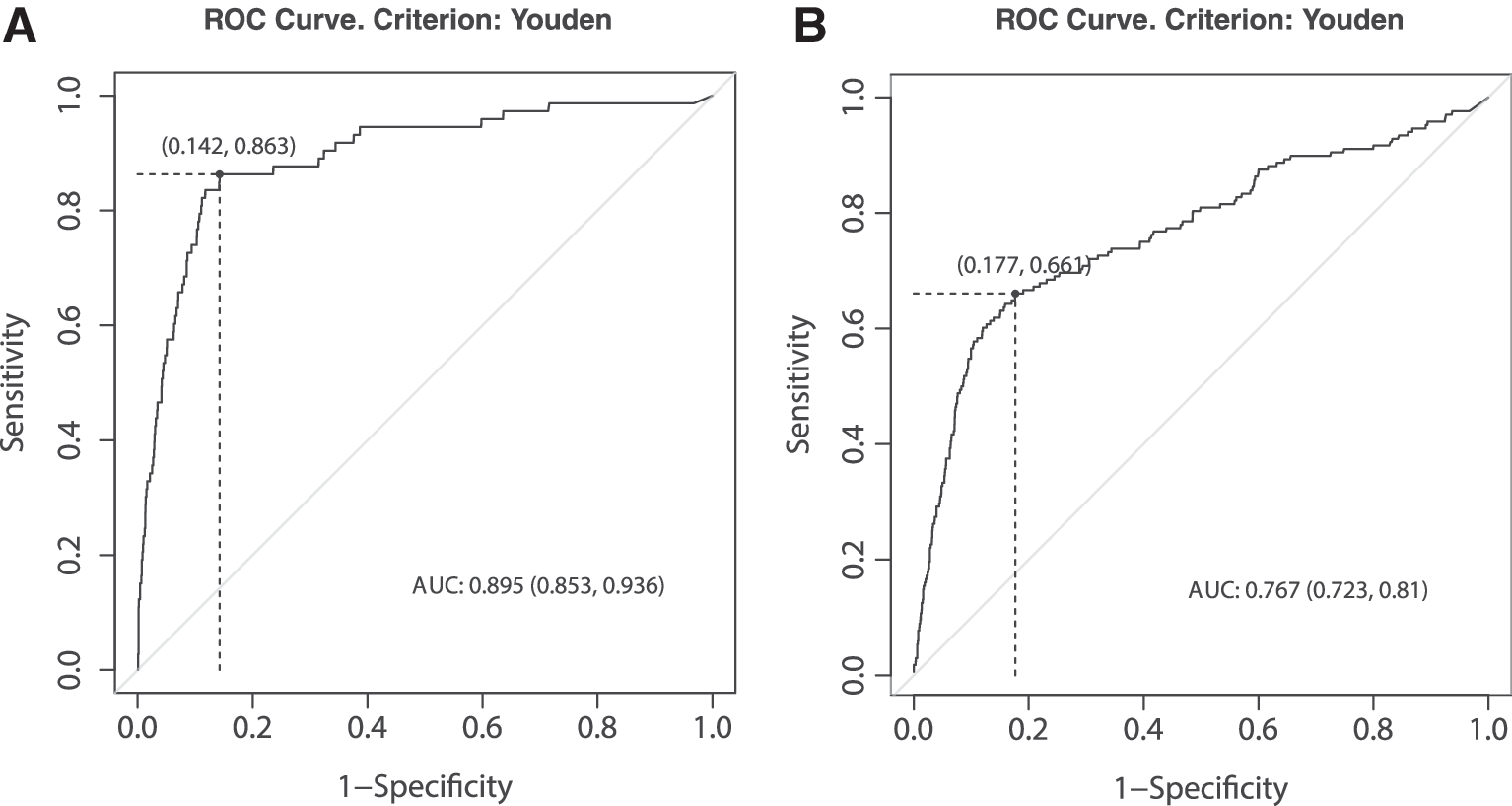
As shown in Table 3, the optimal cutoff points for TPOAb were 18.38 and 14.77 IU/mL for predicting clinical and subclinical hypothyroidism, respectively. As the number of hypothyroid subjects was inadequate, these cut points cannot be reported for each sex separately. The negative predictive value (NPV) of TPOAb for clinical hypothyroidism was 99.5% [CI 99.3–99.7] and 98% [CI 97–97.5] for subclinical hypothyroidism. Since the prevalence of hypothyroidism was low in this population (subclinical hypothyroidism: 168 individuals aged 41.9 ± 14.8 years with a median TSH of 6.5 mIU/L, M ± SD fT4 of 1.1 ± 0.13 ng/dL, and median natural logarithm [Ln] TPOAb of 3.8 IU/mL; overt hypothyroidism: 73 individuals aged 45.1 ± 12.5 years with a median TSH of 12.6 mIU/L, M ± SD fT4 of 0.73 ± 018 ng/dL, and median Ln TPOAb of 5.1 IU/mL) and as the positive predictive value (PPV) depends on the prevalence of subclinical or overt hypothyroidism in the sample, a low PPV was obtained in this study. The area under the ROC for predicting clinical hypothyroidism using the TPOAb level was 0.89 ([CI 0.85–0.93]; Fig. 3A and B and Table 3), with 86% [CI 76–93%] sensitivity and 83% [CI 82–84%] specificity for the optimal cutoff point of 18.38 IU/L (Table 3). The area under the ROC for predicting subclinical hypothyroidism was 0.76 ([CI 0.72–0.8]; Table 3), and the corresponding optimal cutoff point of 14.77 IU/L had a sensitivity of 66% [CI 58–73%] and a specificity of 80% ([CI 79–81%]; Table 3).
(
Youden Index = (Sensitivity + Specificity) − 1.
AUC, area under the curve; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; FP, false positive; FN, false negative; DLR, diagnostic likelihood ratio.
Discussion
The present study determined the reference limits of TPOAb in males and females of different age groups in an iodine-replete population. The range was 1.5–32.8 IU/mL in males and 1.5–35.0 IU/mL in females; the cutoff points to predict the occurrence of subclinical and overt hypothyroidism were 14.7 and 18.3 IU/mL, respectively.
To the best of the authors' knowledge, no ideal method for estimation of reference intervals for thyroid antibodies has yet been developed; nor is there any consensus regarding normal reference intervals and the cutoff point for TPOAb. There are several reasons for this. First, the distribution of TPOAb levels is not Gaussian but skewed to the right, which makes it very difficult to estimate a reference interval. Second, the measurement of this antibody, as mentioned by the guidelines of the NACB (5), is method dependent. Therefore, the NACB recommends that reference intervals be estimated using euthyroid healthy males, aged <30 years, having serum TSH concentrations between 0.5 and 2.0 mIU/L, without a family history of thyroid disease. Despite this, Jensen et al. showed that the NACB guidelines may be insufficient, and may result in upper reference limits for thyroid antibodies that are too high and variable (20).
In health-related fields, a reference interval is the range of values for a physiologic measurement in healthy people; it is a basis for comparison (a frame of reference) for a physician or other health professionals used to interpret a set of test results for a particular patient. Values within the reference range are those within the normal distribution and are thus often described as within normal limits. The cutoff point is the minimum threshold value, which is associated with or can predict an abnormal condition. Determination of the reference range is totally different from identification of the cutoff points. To determine the reference range, a statistical approach is usually used, whereas an outcome-based approach is typically used to determine the cutoff point.
Some studies show that TPOAb reference limits are age and sex specific (7,21). In a study by Tozzoli et al., the upper reference limits for TPOAb were 15 IU/mL for females and 9 IU/mL for males, showing that sex differences in thyroid antibody levels are not statistically significant (22). A study of 1512 Danish Caucasians revealed reference intervals ranging between 2 and 10 IU/mL for TPOAb (20). Compared with the above-mentioned studies, the results of the present study showed higher levels but similar ranges of TPOAb in both sexes. In the Busselton thyroid study, which is a community-based study, the upper limit of the reference interval for TPOAb was <35 IU/mL, and it was higher than in the studies mentioned above (21). In the Busselton study, simple logarithmic transformations were used to calculate data sets; the 97.5th percentile was hence calculated as 33 IU/mL, and 11 IU/mL was considered as the median value, among those without a history of thyroid diseases. By applying the NACB guidelines, the reference interval for upper limits of TPOAb was 30 IU/mL. Table 4 shows a summary of worldwide studies reporting TPOAb reference values.
M, male; F, female.
The modulating role of dietary iodine on AITD has been clearly established in animal models, and circumstantial evidence exists for a similar role in humans (23 –25). The mechanism is complex, and it has recently been shown that iodide may exacerbate thyroiditis in NOD mice but does not affect the production of TSH receptor (TSH-R) antibodies in this strain (26). Therefore, iodine may affect several aspects of the autoimmune response; iodide stimulates thyroid follicular cells to produce chemokines such as CCL2, CXCL8, and CXCL14 (27), suggesting that iodide at high concentrations could induce AITD through chemokine upregulation, thereby attracting lymphocytes into the thyroid gland.
The main reasons for differences in TPOAb reference limits are probably the laboratory methods used for assessment of TPOAb, which in the present study was an ELISA. Overall, all laboratory methods used to measure thyroid antibodies show high variability and a high degree of dispersion in cutoff levels. Moreover, the different TPOAb ranges could be due to different factors such as iodine intake (e.g., mild iodine deficiency probably partly protects against autoimmune thyroid disease), genetic factors, and characteristics of the populations such as sex and age. Other reasons could be differences in definitions and selection criteria of the probands and the reference ranges of thyroid function tests used to define healthy subjects, which vary among different populations (6,7,20,28).
Although studies show that the percentage of subjects with antithyroid antibodies increases with age, the results of the present study differ. The results of NHANES III showed increasing serum TPOAb concentrations with increased age; mean TPOAb concentration increased from 13 IU/mL in the 12–19 year age group to 23.9 IU/mL in the ≥80 year age group. Similar to the results of the present study, Tozzoli et al. reported that the upper limit of normal in relation to age revealed no substantial differences among the different age groups, indicating no need to differentiate reference limits according to this parameter (20).
There are several limitations in this study. First, the study is cross-sectional and hence does not include individual changes over time. Second, although a detailed history was obtained at the time of the baseline examination, the use of thyroid or other medications and the presence of thyroid diseases and goiter were self-reported. Third, the number of events to determine a sex-specific reliable cutoff point for TPOAb is not sufficient and could only be determined for the whole study cohort. In addition, it should be emphasized that the reference range given in this study is specific to this study. Although, 24-hour urine samples could not be assessed for a better assessment of iodine intake due to logistic limitations, the study was conducted in an iodine-sufficient country. There are also several strengths to this study. First, fT4 was measured, yielding a more accurate thyroid status (as total T4 levels change with binding protein abnormalities) than if only a total T4 concentration had been available. Second, to the authors' knowledge, this is one of the few studies aimed at determining the age- and sex-specific reference limits for TPOAb based on more sophisticated statistical analyses in a cohort from an iodine-sufficient area.
In conclusion, this study establishes the reference intervals and the optimal cutoff points for TPOAb in a community-based sample of an iodine-sufficient area. To improve clinical interpretation, however, as the methods and criteria used to determine the reference intervals of thyroid autoantibodies differ in various populations, each reference laboratory should determine its own TPOAb reference limits.
Footnotes
Acknowledgments
We would like to acknowledge the laboratory personnel of the RIES for their assistance. The authors would like to acknowledge Ms. Niloofar Shiva for critical editing of the English grammar and syntax of the manuscript.
Author Disclosure Statement
No competing financial interests exist.