
Abstract
Background:
Treatment of advanced medullary thyroid carcinoma (MTC) was recently improved with the approval of vandetanib and cabozantinib. However, there is still a need to explore sequential therapy with more than one tyrosine kinase inhibitor (TKI) and to explore alternative therapies when vandetanib and cabozantinib are not available. This study reports the authors' experience with sorafenib as a treatment for advanced MTC.
Methods:
This is a retrospective longitudinal study of 13 patients with progressive metastatic MTC treated with sorafenib 400 mg twice daily between December 2011 and January 2015. The primary endpoints were to evaluate response and progression-free survival (PFS) in patients treated with sorafenib outside a clinical trial. The secondary endpoint was an assessment of the toxicity profile. One patient was excluded because of a serious allergic skin rash one week after starting sorafenib.
Results:
The analysis included 12 patients with metastatic MTC (median age 48 years), 10 with sporadic and 2 with hereditary disease. The median duration of treatment was 11 months, and the median follow-up was 15.5 months. At data cutoff, 2/12 (16%) patients were still on treatment for 16 and 34 months. According to Response Evaluation Criteria in Solid Tumors analysis, 10 (83.3%) patients showed stable disease, and two (16.6%) had progression of disease; no partial response was observed. The median PFS was nine months. However, three patients with extensive and rapidly progressive disease died within three months of sorafenib treatment. The median PFS excluding these three patients was 12 months. Adverse events (AE) occurred in nine (75%) patients. The main AEs were skin toxicity, weight loss, and fatigue. Five (41.6%) patients needed dose reduction, and one patient discontinued treatment because of toxicity.
Conclusions:
Treatment with sorafenib in progressive metastatic MTC is well tolerated and resulted in disease control and durable clinical benefit in 75% of patients. Sorafenib treatment could be considered when vandetanib and cabozantinib are not available or after failing these drugs.
Introduction
M
Until recently, the treatment of advanced MTC consisted in local tumor control with surgical resection of the primary tumor and regional lymph nodes (3) and cytotoxic chemotherapy for progressive and/or symptomatic metastatic disease. However, the efficacy of systemic chemotherapy, including dacarbazine, 5-fluorouracil, and anthracyclines, is poor, with response rates (RR) ranging from 10% to 20% (4 –7). Recently, a better understanding of the molecular biology of MTC and the development of anti-angiogenic tyrosine kinase inhibitors (TKI) such as vandetanib (8) and cabozantinib (9) has shed new light on the treatment of this disease.
Both of these drugs have been approved in the United States and Europe based on results obtained in randomized phase III trials. The ZETA trial investigated vandetanib—an inhibitor of RET, VEGFR, and EGFR—in 331 patients with advanced MTC who were randomized to receive vandetanib 300 mg/day or placebo until documented progression. Treatment with vandetanib was associated with significant improvement of median progression-free survival (PFS) by 11 months compared with placebo (30.5 months vs. 19.3 months, p < 0.001) (8). Another phase III study, the EXAM trial, evaluated the efficacy of cabozantinib—an inhibitor of RET, VEGFR2, and c-MET—in 330 patients with documented radiographic progression of metastatic MTC. Patients were randomized to cabozantinib or placebo (2:1), and treatment resulted in a seven-month PFS benefit compared with placebo (11.2 months vs. 4 months, p < 0.001) (9). A potential explanation for the difference in PFS of both arms between these two trials is the required radiological progression of disease in the previous 14 months for inclusion in the EXAM trial, which resulted in a selection of patients with more aggressive tumors.
Sorafenib is a kinase inhibitor with activity against RET, VEGFR 2 and 3, PDGFR, and RAF that has been approved for progressive, metastatic differentiated thyroid cancer (10). In MTC, its efficacy has been investigated in two phase II trials and in retrospective studies (Table 1) (11 –15). In these studies, treatment with sorafenib resulted in RR (stable disease + partial response) ranging from 80% to 100%, and PFS ranging from 10.5 to 17.9 months. Based on these results and because of the unavailability of both vandetanib and cabozantinib in the public health system of Brazil, sorafenib was initiated in patients with progressive metastatic MTC.
PR, partial response; SD, stable disease; MTC, medullary thyroid carcinoma; RR, response rate; PFS, progression-free survival; HFSR, hand–foot skin reaction.
Subjects and Methods
Patients and study design
This is a retrospective longitudinal study of 13 patients with progressive metastatic MTC treated with sorafenib 400 mg twice daily between December 2011 and January 2015 at the Instituto do Câncer do Estado de São Paulo (ICESP), Brazil. The study was approved by the local research ethics committee.
Patients were clinically evaluated every one to two months. Treatment efficacy was assessed by measurement of tumor markers (calcitonin and carcinoembryonic antigen [CEA]) every 8–12 weeks and by radiological studies, including computed tomography (CT) scans, magnetic resonance imaging (MRI), and bone scans every two to six months. The imaging studies were reviewed by an independent board-certified radiologist using Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 (16) for determining RR and PFS.
Tumor response was defined as progressive disease if there was at least a 20% increase in the sum of the diameters of target lesions (TLs) or appearance of new metastatic lesions; as stable disease (SD) if there was a change between a 19% increase and a 29% decrease; and as partial response (PR) if there was at least a 30% decrease in the sum of the diameters of target lesions.
Sorafenib dose adjustments were made according to toxicity profile, and toxicities were graded according to Common Terminology Criteria for Adverse Events—National Cancer Institute v4.0 (CTCAE—NCI v4.0) (17).
Study endpoints
The primary endpoints were to evaluate tumor and biochemical response and PFS in patients with progressive metastatic MTC treated with sorafenib outside of a clinical trial. The secondary endpoint was the assessment of the toxicity profile.
Statistical analysis
Descriptive statistics were performed using median and standard deviation for analysis of quantitative variables. Qualitative variables were expressed in percentages. Comparison of calcitonin and CEA were performed by Wilcoxon's rank-sum test. For each patient, pretreatment calcitonin and CEA levels were compared with the respective lowest levels obtained during treatment. Best tumor response was represented using a waterfall plot. PFS was defined as the time between onset of the treatment with sorafenib and occurrence of progression or death was estimated by the Kaplan–Meier method. Patients who did not have an event were censored at the date of last follow-up. Analysis was performed using PASW Statistics for Windows v18.0 (SPSS, Inc., Chicago, IL).
Results
Clinical characteristics
From December 2011 to January 2015, 13 patients with MTC were treated with sorafenib. One patient was excluded because of a serious allergic skin rash one week after starting sorafenib. The analysis included 12 patients (seven females and five males) with a median age of 48 years. All patients had disease progression documented by imaging studies prior to initiation of sorafenib. In addition to distant metastatic disease, three patients had locally advanced disease (Table 2). The main sites of metastatic disease included the liver (100%), bone (83%), lung (67%), and mediastinal lymph nodes (58%).
Cys634Arg/Cys620Arg.
Three patients with unresectable disease.
TT, total thyroidectomy; LND, lymph node dissection.
Germline RET mutational analysis was performed in all patients; 10 (83%) patients had sporadic disease, and two patients had a germline RET mutation (c.1900T>C p.C634R and c.1858T>C p.C620R). Nine (75%) patients were previously treated with total thyroidectomy and cervical lymph node (LN) dissection. Three (25%) patients had unresectable disease. Eight patients were previously treated with systemic chemotherapy that included dacarbazine and capecitabine in six (50%) patients, cisplatin and adriamycin in one patient, and dacarbazine and fluorouracil in one patient. Six patients were treated with palliative external radiotherapy: five for bone metastasis, and one for local control of cervical disease. One patient with brain metastasis was treated with stereotactic radiosurgery. One patient had been previously treated with cabozantinib as part of a randomized phase III trial (Table 2).
Therapy
Sorafenib was prescribed at a starting dose of 400 mg twice a day. The median duration of treatment was 11 months, ranging from 2 to 34 months, and the median follow-up was 15.5 months, ranging from 2 to 40 months from the initiation of sorafenib treatment. At data cutoff, 2/12 (16%) patients were still on treatment for 16 and 34 months.
Response rate and PFS
The waterfall plot for best tumor response is shown in Figure 1. According to RECIST analysis, among 12 patients treated with sorafenib, 10 (83.3%) showed SD, and two (16.6%) progressive disease with development of new lesions. No PR was observed. A durable clinical response (SD six months or more) was observed in 75% of patients, ranging from 7 to 24 months. The median PFS was nine months. However, three patients with extensive and rapid progressive disease died within three months of sorafenib treatment. Prior to initiating sorafenib, two of these patients had unresectable neck lesions that rapidly progressed with upper airway obstruction, and one patient had rapid progression of hepatic metastases and probably disease dedifferentiation based on increasing CEA with declining calcitonin levels. The median PFS, excluding these three patients classified as early deaths, was 12 months (Fig. 2).

Tumor best response. Waterfall plot of best tumor response showing maximum regression in target lesions (TLs) from baseline (Response Evaluation Criteria in Solid Tumors v1.1). Ten patients had stable disease (SD), and two patients, although presenting SD in TLs, developed new metastatic lesions and were considered to have progressive disease. No patients had a partial response (PR).
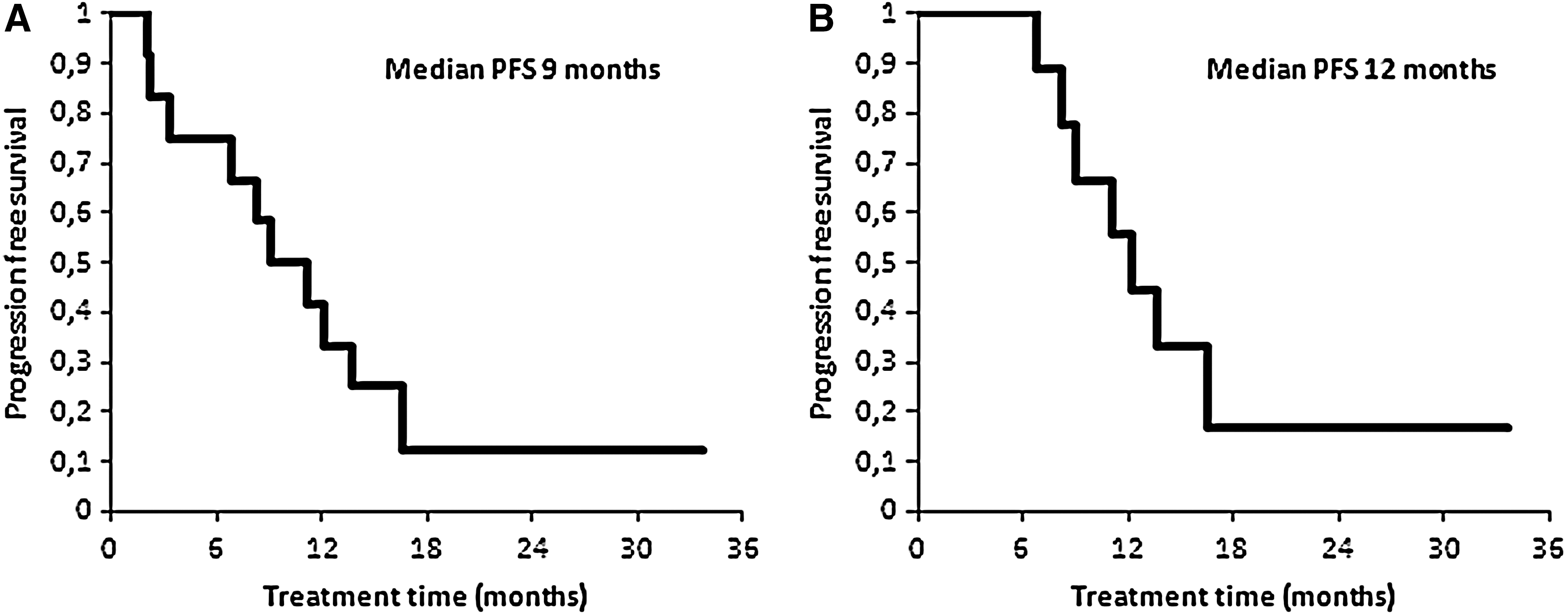
Progression-free survival (PFS). (
Biochemical response
Analysis of the biochemical markers revealed a significant reduction of the median calcitonin levels (pretreatment 17,294 pg/mL [range 7969–95,836 pg/mL] vs. post-treatment 5756 pg/mL [range 1660–46,608 pg/mL]; p = 0.002). While 92% of patients had a reduction in the calcitonin level, only 60% had reduction of CEA (350 ng/mL vs. 222 ng/mL; p = 0.241; Fig. 3).
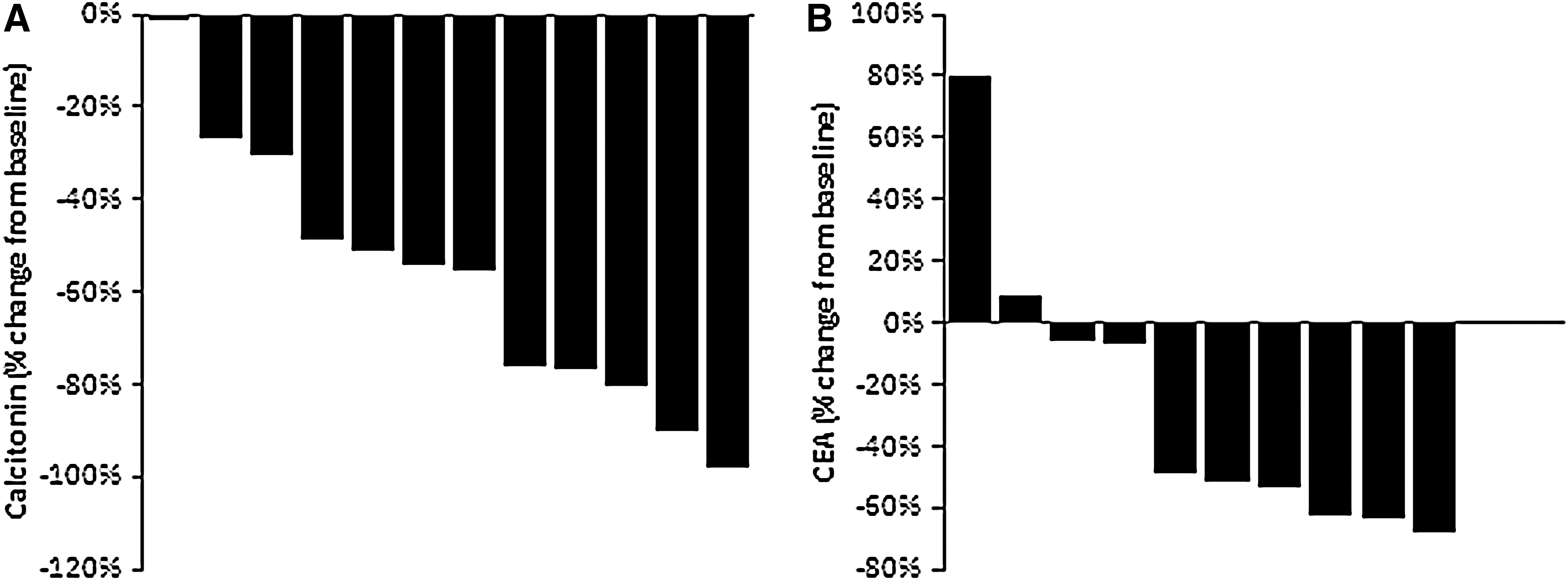
Best biochemical marker response during treatment. (
Clinical improvement of specific symptoms related to metastatic MTC, such as diarrhea, flushing, and bone pain, was seen in 40% of the patients. In addition, one previously reported patient with ectopic ACTH syndrome (18) had complete resolution of hypercortisolism. This patient remained on sorafenib for 14 months when hypercortisolism recurred, and imaging studies demonstrated progression of disease.
Treatment tolerability
Adverse events (AEs) were managed with medication to attenuate symptoms, dose interruptions, and dose reductions. Common AEs (any grade or grade 3 or higher) are summarized in Table 3. Five (41.6%) patients needed a sorafenib dose reduction to 600 mg/day, one patient needed two interruptions (dermatitis and diarrhea) with dose reduction to 400 mg/day for 15 days with return to 600 mg/day, and in one patient the drug was discontinued because of weight loss and anorexia.
Adverse events graded according to National Cancer Institute Common Terminology Criteria for Adverse Events v4.0.
Three (25%) patients had elevation of thyrotropin serum levels requiring a median increase of 33.5% in levothyroxine dosage.
Discussion
Despite significant advances in the treatment of advanced MTC with the recent approval of vandetanib and cabozantinib, there is still a need to explore more effective and more tolerable treatments. Both vandetanib and cabozantinib result in significant improvement of PFS and reduction in tumor volume and biochemical markers, but none result in cure (8,9). Therefore, sequential therapy with the use of more than one kinase inhibitor may be required. In addition, the availability of vandetanib and cabozantinib is not universal, and there may be a need to initiate alternative therapies. This study reported the authors' experience with sorafenib as a treatment for advanced MTC.
Twelve patients with locally advanced or extensive metastatic MTC who had progressive disease were treated with sorafenib from December 2011 to January 2015. These patients had large tumor burden (median baseline sum of target lesions 8.1 cm [range 2.8–17.9 cm], median calcitonin 17,294 pg/mL [range 7969–95,836 pg/mL], and median CEA 350 ng/mL [range 162–3151 ng/mL). All patients had metastatic disease to the liver, and several other sites such as the bone, lungs, and mediastinal lymph nodes were also frequently involved (Table 2). Most of the patients were symptomatic (92%), indicating extensive disease. The non-availability of vandetanib, cabozantinib, or active clinical trials was the main reason why these patients were started on sorafenib.
The best response rate observed in this cohort was stabilization of disease in 83% of the patients, with a median reduction of tumor volume <30% (6–23%) in eight patients; no patients achieved PR, and 16.6% had disease progression (Fig. 1). The median PFS was nine months, and duration of treatment ranged from 3 to 34 months. Two patients remain on treatment until the end of this study.
Sorafenib treatment in MTC was investigated in two phase II trials (11,12) and three retrospective studies (13 –15). Rates of SD observed in these studies are similar to those in the current series (Table 1). However, while PR was observed in 6–47% of patients in these published studies, no PR was observed in patients in the current study. One possible explanation is the aggressiveness and extent of metastatic disease observed in the present series. The response to sorafenib in this cohort was heterogeneous. It was observed that patients remaining on treatment for >14 months had less extensive disease, with a median tumor volume of 5.7 cm (range 2.8–6.7 cm). While there was a group of patients that benefited from the drug in terms of symptom control and stabilization of disease (median PFS 12 months [range 9–15 months]), there was another group (n = 3) that failed treatment with early deaths. These three patients had extensive and rapidly progressive disease and died within three months of starting sorafenib. One of the patients had extensive metastatic liver disease with a rapid rise of CEA, indicating disease dedifferentiation; two patients had unresectable locally advanced disease that progressed with upper airway obstruction, and one of these two patients had MTC with neurofibromatosis type 1 syndrome. This experience suggests that in patients who need rapid tumor volume reduction, sorafenib might not be an appropriate therapeutic option.
Another observation in the present series is that a patient previously treated with cabozantinib for 25 months was started on sorafenib after disease progression and remained with SD for 12 months. In the EXAM trial, approximately 21% of patients treated with cabozantinib had been previously treated with another TKI, including sorafenib and vandetanib. These patients showed a prolongation of PFS similar to TKI-naive patients. The current study presents the first description of sorafenib being effective after cabozantinib treatment. This is an important observation, suggesting that sorafenib could be an option as second-line therapy and that sequential use of a different TKI may be an approach for successive prolongation of PFS in the treatment of patients with metastatic MTC.
Sorafenib was reasonably well tolerated. Toxicities of any grade were observed in 75% of patients. Hand–foot skin reaction and weight loss were the most frequent adverse events, which were observed in approximately 50% of patients, and were grade 3 in 25% ofpatients. Diarrhea and dermatitis were classified as grade 3 in 8% of patients. Drug interruption and dose reduction were necessary in five (41.6%) patients. Six patients died, all related to disease progression and none related to treatment. One patient discontinued sorafenib due to grade 3 diarrhea and grade 3 weight loss after 12 months of treatment.
In the phase III trials, cabozantinib and vandetanib required dose reductions in 79% and 35% of the patients, respectively. In this series, five (41.6%) patients needed sorafenib dose reduction to 600 mg/day, and in one patient the drug was discontinued due to weight loss and anorexia. The most frequent AE observed with cabozantinib and vandetanib was diarrhea, which occurred in around 60% of patients (grade 3–4 in 11–16%). In the present study, sorafenib was associated with diarrhea in 16% of patients, and in 8% it was grade 3. The detection of diarrhea could have been impaired because of the retrospective nature of the data collection in which AEs grade 1–2 might have been overlooked and due to the fact that 50% of patients had diarrhea prior to treatment. Despite the observation that 66% reported improvement of the diarrhea, persistence of diarrhea after starting the treatment could have been secondary to the disease or due to sorafenib.
Conclusions
Treatment with sorafenib in progressive metastatic MTC is well tolerated and resulted in disease control and durable clinical benefit in 75% of patients. The approved drugs for progressive MTC are vandetanib and cabozantinib. Sorafenib treatment could be considered when these TKI are not available.
Although one patient previously treated with cabozantinib responded to sorafenib (SD 12 months), further studies are necessary to define the role of sorafenib clearly as a second- or third-line treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.