
Abstract
Background and Objective:
Maternal iodine nutrition and thyroid status may influence neurocognitive development in offspring. This study investigated the effects on the intelligence quotient (IQ) of children born to mothers with different levels of iodine supplementation, with or without the administration of levothyroxine (LT4), prior to and during pregnancy.
Patients and Methods:
This pilot, prospective, observational study included four study groups, each comprising 15 mother–child pairs, identified on the basis of maternal histories of iodized salt consumption and LT4 treatment prior to and during pregnancy. The groups were labeled as follows: iodine (I), no iodine (no-I), iodine + LT4 (I + T4), and no iodine + LT4 (no-I + T4). IQ tests were administered to children at 6–12 years of age with the Wechsler Intelligence Scale for Children–3rd Edition (WISC-III), with full-scale IQ (FSIQ), verbal IQ (VIQ), and performance IQ (PIQ) being evaluated.
Results:
Children of I and I + T4 mothers had similar verbal, performance, and FSIQs, which were 14, 10, and 13 points higher, respectively, than children born to no-I and no-I + T4 mothers. A positive association was found between VIQ and maternal urinary iodine (β = 1.023 [confidence interval (CI) 1.003–1.043]; p = 0.028), but not with maternal free thyroxine concentrations at any stage of pregnancy. Overall, the prevalence of borderline or defective cognitive function was more than threefold higher in the children of mothers not using iodized salt than of those mothers using it (76.9% vs. 23.1%, odds ratio 7.667 [CI 2.365–24.856], χ2 = 12.65; p = 0.0001).
Conclusions:
Neuro-intellectual outcomes in children appear to be more dependent on their mothers' nutritional iodine status than on maternal thyroid function. These results support the growing body of evidence that prenatal, mild-to-moderate iodine deficiency adversely affects cognitive development later in life, with a seemingly greater impact on verbal abilities.
Introduction
I
Several studies involving mildly iodine-deficient and iodine-sufficient populations have shown a strong association between either maternal subclinical hypothyroidism (7 –9) or hypothyroxinemia (10 –16) and impaired neuro-intellectual outcomes in progeny. However, other studies have failed to confirm these associations (17 –20), and some anecdotal reports have shown normal neurodevelopment in children born to severely hypothyroid mothers whose iodine intake during gestation was more than adequate (21 –23). The only randomized clinical trial to date that has investigated the effects of levothyroxine (LT4) given at a median gestational age of 13 weeks to mothers with mild gestational thyroid insufficiency (i.e., subclinical hypothyroidism and isolated hypothyroxinemia) and exposed to mild-to-moderate ID during pregnancy did not show improved cognitive outcomes in their offspring (24). Moreover, in recent years, a growing body of clinical evidence has emerged suggesting that gestational iodine supplementation, while improving infant cognitive development, does not have a clear impact on maternal thyroid function (25 –28).
Taken together, these data suggest that maternal iodine status during gestation may play a more critical role than maternal thyroid function in determining neuro-intellectual outcomes in progeny. To assess this hypothesis, a pilot prospective study was conducted to observe the long-term effects of different maternal iodine supplementation regimens with and without LT4 prior to and during pregnancy on the cognitive function of school-age children living in an ID area where endemic cretinism (29), endemic cognitive deficiency (30), and attention deficit and hyperactivity disorders (ADHD) (14) had previously been described.
Methods
Study design and participants
This study was observational in design and included 60 mother–child pairs from a small rural ID area in northeastern Sicily. Mean urinary iodine excretion (UIE) and goiter prevalence in local schoolchildren at conception (2000–2007) and at the time of cognitive evaluation (2012–2013) of the subjects were consistent with moderate (UIE 62.2 ± 38.2 μg/L; goiter in schoolchildren 16.3%) (14) and mild (UIE 95.6 ± 25.8 μg/L; goiter in schoolchildren 7.6%; unpublished data) ID, respectively.
The objective of this study was to assess global cognitive outcomes in children born to mothers under different conditions of iodine nutrition during gestation, either treated with LT4 or receiving no LT4 prior to and during pregnancy.
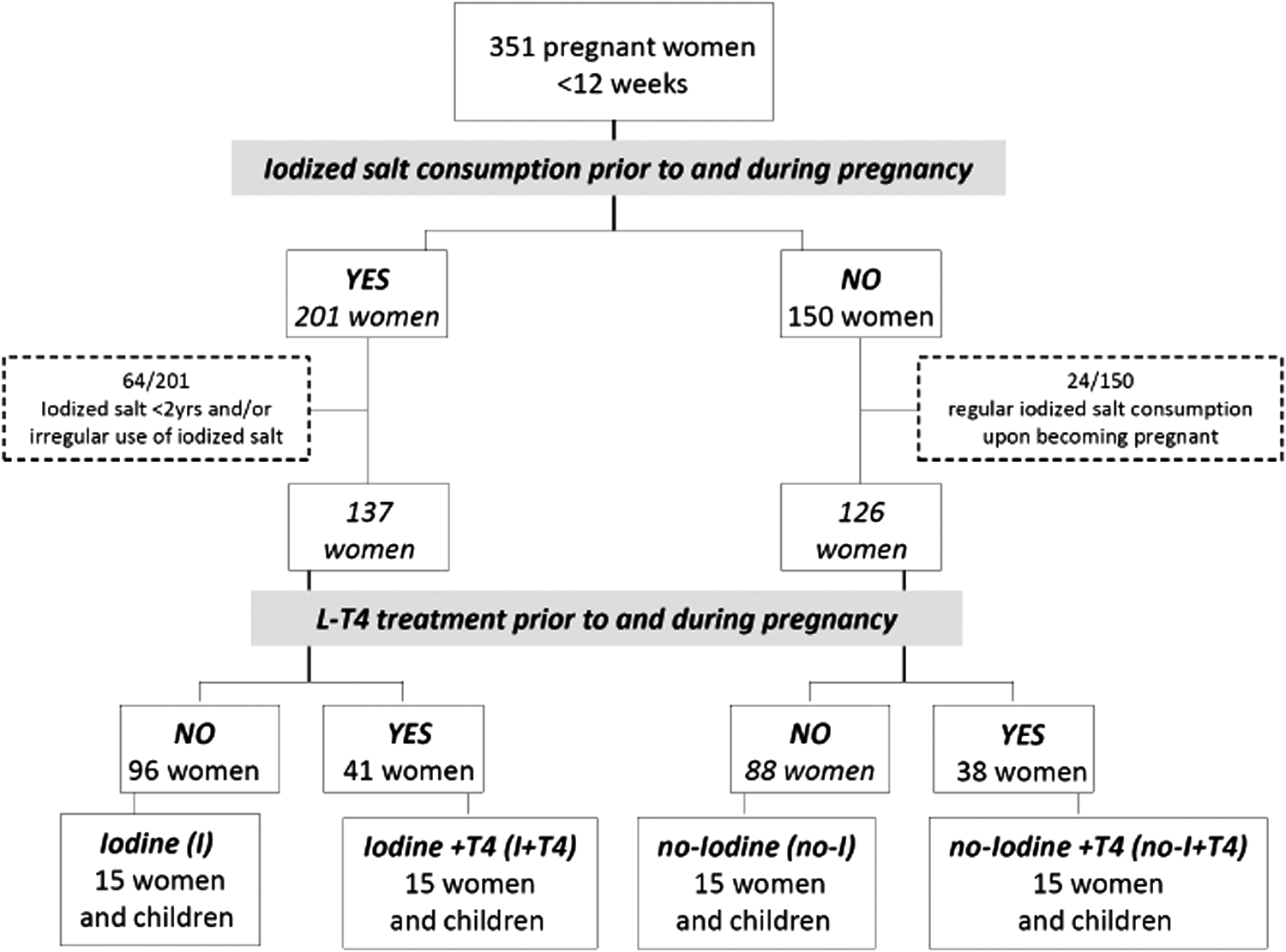
Between January 2000 and January 2007, 351 pregnant women (gestational age <12 weeks) were referred to the authors' antenatal clinic for the prevention and control of gestational thyroid disorders. At the time of enrollment, all women were administered a structured questionnaire about their dietary habits, specifically focusing on the regular use of iodized salt. They were then sampled for free triiodothyronine (fT3), free thyroxine (fT4), and thyrotropin (TSH), and were scheduled to have their thyroid function serially reassessed at six-week intervals throughout pregnancy. Serum antithyroglobulin (TgAb) and antithyroperoxidase (TPOAb) antibodies were also measured at initial and final sampling. With few exceptions, the women provided urine samples at every appointment. Adjustments to daily LT4 doses were made when needed in the women receiving semi-suppressive LT4 therapy for uni- or multinodular goiter (31) in order to maintain preconception TSH levels (0.1–0.5 mIU/L). All data were recorded in a specific database.
As shown in Figure 1, the initial population consisted broadly of two groups: the first included 201/351 (57.3%) women who reported using iodized salt prior to becoming pregnant; the second comprised 150/351 (42.7%) women who had never used iodized salt prior to conception. Women who had not used iodized salt regularly or had not used it for at least two years (32) (n = 64/201) were excluded from the former group; women who had started using iodized salt upon becoming pregnant (n = 24/150) were excluded from the latter group. The groups were further characterized according to whether mothers had uninterruptedly received LT4 treatment for uni- or multinodular goiters prior to and during pregnancy. The four groups identified were labeled iodine (I; n = 96 women), iodine + LT4 (I + T4; n = 41 women), no iodine (no-I; n = 88 women), and no iodine + LT4 (no-I + T4; n = 38 women). Since this was a pilot study, the first 15 mother–child pairs from each group who met the inclusion criteria were selected to make up the study groups. The size of 60 mother–child pairs (15 for each group) corresponds to 25% of the final study size of approximately 240 subjects, which was calculated by taking into account an expected difference of a mean IQ score of 13.5 points (26) between two main groups (I vs. no-I). Assuming α = 0.050, we estimated that 119 subjects per group would be needed in the final study in order to obtain a power level of 0.80.
Study population and design.
Inclusion criteria for mothers were: (i) age >18 years; (ii) uncomplicated singleton pregnancy; (iii) term delivery; (iv) no severe or chronic diseases (including thyroid autoimmune diseases); (v) no major postpartum complications or depression; (vi) TH determination throughout gestation (at least one testing at the 1st trimester and two at each subsequent trimester); (vii) full disclosure of diet and lifestyle information during and after pregnancy; and (viii) informed consent. Inclusion criteria for children were: (i) age 6–14 years; (ii) no major neonatal complications; (iii) no congenital hypothyroidism; (iv) no severe/chronic diseases; (v) no major cognitive deficits; (vi) regular school attendance; and (vii) approval for cognitive test administration.
Mother–child pairs included in the study (n = 60) did not differ from those not included (n = 291) in any of the variables reported in Table 1, except for the M/F ratio, which was significantly lower in the I and no-I groups compared with the whole sample (0.25 vs. 0.94, p = 0.031).
Data are expressed as M ± SD, median (IQR), and range for continuous variables, and as percentages for categorical variables. p-Values were calculated using the Kruskall–Wallis test (to compare all groups) and the Mann–Whitney U-test (to perform the two-by-two comparison between groups) for continuous variables and χ2 for categorical variables.
I, iodine group; no-I, no iodine group; I + T4, iodine + levothyroxine group; no-I + T4, no iodine + levothyroxine group; NS, not significant; IQR, interquartile range; SES, socioeconomic status; n.a., not applicable.
Procedures
Cognitive outcome
Each child's intelligence quotient (IQ) was assessed using the Wechsler Intelligence Scale for Children—Third Edition (WISC-III) (33,34), which was administered blind by trained psychologists. Three IQ scores (the full-scale IQ [FSIQ], the Verbal IQ [VIQ], and the Performance IQ [PIQ]), all with a mean of 100 and standard deviation of 15, were calculated. Full-scale IQ scores of 70–85 and <70 were considered to be indicative of borderline or defective cognitive function, respectively.
Biochemical evaluation
Serum concentrations of TSH, fT4, fT3, TgAb, and TPOAb were measured using the electrochemiluminescence immunoassay (ECLIA) system assay (Cobas; Roche Diagnostics, Mannheim, Germany). The detection limits of the assays were as follows: 0.005 mIU/L for TSH, 0.30 pmol/L for fT4, 0.39 pg/mL for fT3, 5 IU/mL for TPOAb, and 10 IU/mL for TgAb. The manufacturer's reference ranges were 0.27–4.20 mIU/L for TSH, 12–22 pmol/L for fT4, and 2–4.4 pg/mL for fT3. TPOAb and TgAb were considered positive for values >34 IU/mL and >115 IU/mL, respectively. Precision profiles showed inter- and intra-assay coefficients of variation <5% over the entire measurement range. UIE, expressed as μg/L, was measured using the modified Sandell–Kolthoff reaction (35) in random urine samples collected from the mothers throughout gestation and from the children at the time of cognitive evaluation. Since several urine samples were collected from each mother (M ± SD = 5.9 ± 0.9; range 4–7), adjusted mean UICs accounting for day-to-day variations in each subject were calculated (36) in order to estimate the overall median UIE for each study group. The study was approved by the local ethics committee.
Statistical analysis
Numerical data are expressed as means ± standard deviations (M ± SD), medians, and interquartile ranges (IQR), and categorical variables as numbers and percentages.
Although most variables under examination were normally distributed (Kolmogorov–Smirnov test), because of our sample size, the nonparametric approach was used to ensure valid asymptotic results. Accordingly, the Mann–Whitney (comparison of independent samples), Wilcoxon (comparison of dependent samples), and Friedman (comparison over the observation period of several dependent groups) tests were used. The chi-square test was used to assess the association between categorical variables. Finally, logistic regression models were used to assess the dependence of suboptimum cognitive outcomes (IQ scores <85, i.e., −1 SD) on various explanatory variables and confounders. Covariates were either continuous/discrete measures (maternal age; gestational age at birth; birth weight; child age at time of cognitive evaluation; maternal serum fT3, fT4, and TSH at the various points during gestation; maternal UIE; and family socioeconomic status [SES] evaluated by means of the Hollingshead Index) (37,38), or categorical variables (maternal parity [uniparous vs. pluriparous]; sex; breastfeeding [some vs. no]; major maternal stressful life-events [yes vs. no]; and maternal/paternal education [low, medium, high]). Statistical analyses were performed using SPSS Statistics for Windows v17.0 (SPSS, Inc., Chicago, IL). A p-value of <0.05 was considered to be statistically significant.
Results
Although all children successfully completed the tests administered, one result was excluded from analysis because the mother of the child concerned had helped him complete the test. Therefore, the results refer to 59 mother–child pairs (14 for the I + T4 group and 15 for each of the other groups).
No differences in epidemiological, socioeconomic, and clinical parameters were observed between the four study groups, except for child sex distributions and maternal UIE (Table 1). The latter, calculated on a total of 88 (I group), 83 (no-I group), 89 (I + T4 group), and 90 (no-I + T4 group) samples, respectively, was significantly higher in women who regularly used iodized salt (I and I + T4 groups) than it was in women who had never used it (no-I and no-I + T4 groups).
Changes in maternal thyroid function parameters over the course of pregnancy are reported in Table 2. Mothers in the I group displayed serum fT4 concentrations that were always significantly higher than that of those in the no-I group. The cognitive performances of children born to mothers in these two groups also differed, with significantly higher FSIQ and VIQ scores in the I than in the no-I offspring (FSIQ: I 93.1 ± 11.8 vs. no-I 81.7 ± 13.5; VIQ: I 90.1 ± 14.2 vs. no-I 80.3 ± 12.3; p = 0.028 and 0.034, respectively; Fig. 2A). Similar differences were found between I + T4 and no-I + T4 offspring (FSIQ: I + T4 96.1 ± 18.2 vs. no-I + T4 81.3 ± 13.1; VIQ: I + T4 97.2 ± 18.6 vs. no-I + T4 79.6 ± 13.9; p = 0.038 and 0.017, respectively), despite their mothers having had similar serum fT4 concentrations during pregnancy (Fig. 2B). Table 3 shows full comparisons between groups. Interestingly, there were no statistically significant differences in any of the three quotients between children born to supplemented mothers (i.e., I group vs. I + T4 group) and those born to mothers not using iodized salt (i.e., no-I group vs. no-I + T4 group). Accordingly, children were grouped in relation to their mothers' nutritional iodine status and irrespective of LT4 treatment to form the I ± T4 group (including 29 children: 15 from the I group and 14 from the I + T4 group) and the no-I ± T4 group (including 30 children: 15 from the no-I group and 15 from the no-I + T4 group). Mothers in the I ± T4 group displayed higher serum fT4 concentrations than mothers in the no-I ± T4 group at early gestation and at 13–18 weeks (p = 0.006 and 0.0008, respectively), but not at subsequent follow-up.
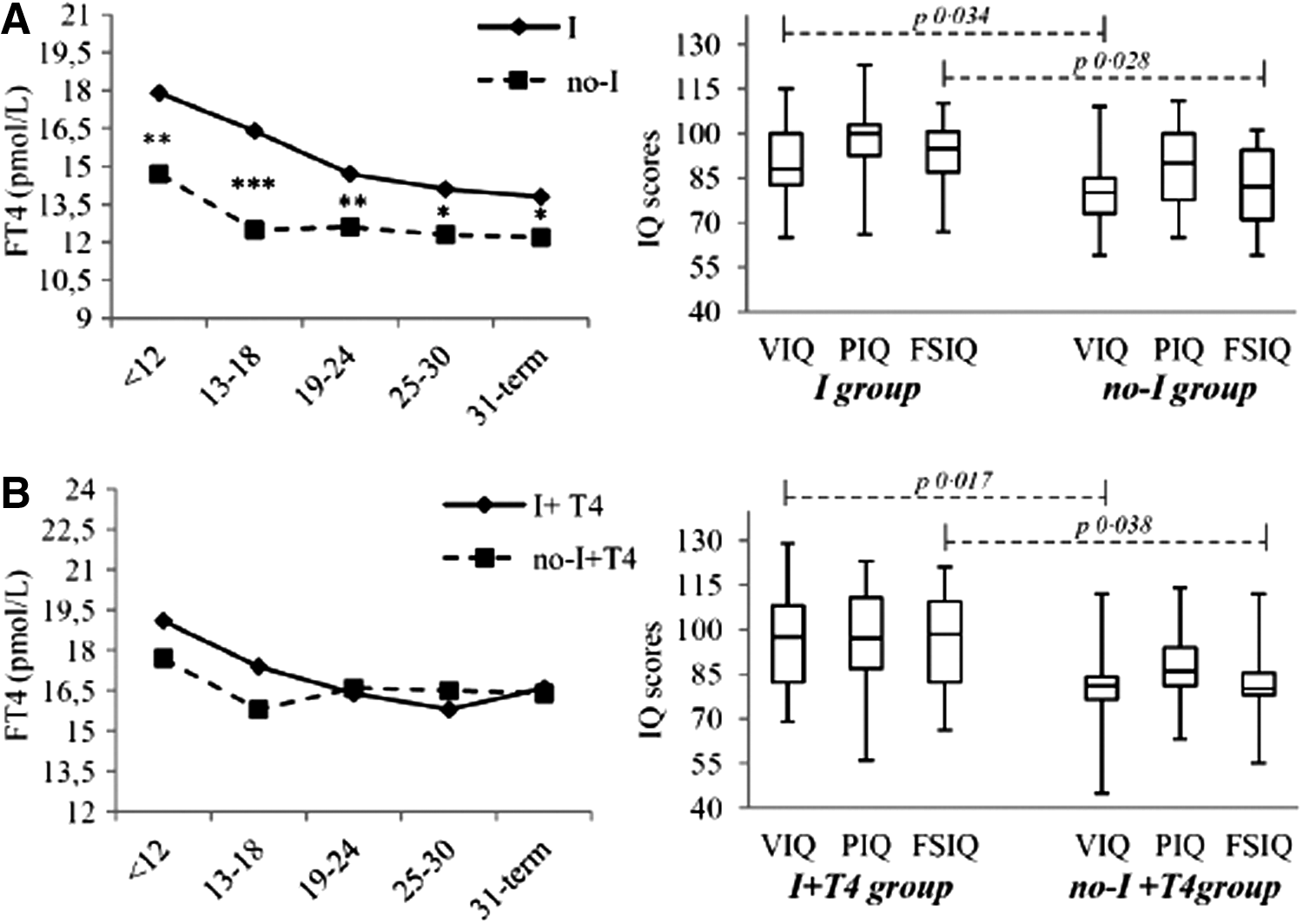
Mean maternal free thyroxine concentrations (line graphs) and median (interquartile range, minimum, maximum) cognitive outcomes (box plots) in (
Data are expressed as M ± SD. p-Values were calculated using athe Mann–Whitney U-test (comparisons between groups) and bthe Friedman test (comparisons within groups in different times).
Serum fT3 concentrations were significantly higher in I + T4 than in no-I + T4 and in I than in no-I women at very early and mid-gestation, respectively. Serum fT4 concentrations were significantly higher in I + T4 and no-I + T4 groups than in the no-I (at any point in time during gestation) and I groups (from week 19 to week 24 onwards). Also, serum fT4 concentrations were significantly higher in the I than in the no-I group at any point in time. Opposite changes, but similar statistical differences between the study groups, were observed in serum TSH concentrations over the study period.
fT3, free triiodothyronine; fT4, free thyroxine; TSH, thyrotropin.
Data are expressed as M ± SD; confidence intervals (CI), medians, and interquartile ranges (IQR) are also reported. p-Values were calculated using the Mann–Whitney U-test.
FSIQ, Full Scale Intelligence Quotient; VIQ, Verbal Intelligence Quotient; PIQ, Performance Intelligence Quotient; UIC, urinary iodine concentration.
FSIQ was on average 13 points higher in I ± T4 than in no-I ± T4 children (94.5 ± 15.1 vs. 81.5 ± 13.1; p = 0.00037), with the difference due to significantly better results on both verbal and performance subscales. More specifically, VIQ was almost 14 points (93.5 ± 16.6 vs. 79.6 ± 12.9; p = 0.00043) and PIQ 10 points (97.4 ± 15.9 vs. 87.4 ± 13.9; p = 0.0067) higher in I ± T4 than in no-I ± T4 children. It is noteworthy that while I ± T4 children performed similarly on verbal and performance subscales (p = 0.11), mean VIQ scores were significantly lower than PIQ scores for children from the no-I ± T4 group (p = 0.006).
Overall, nine children (3/9 born to I ± T4 women and 6/9 born to no-I ± T4 women) with FSIQs <2 SD (range 55–69 points) were diagnosed with mild mental retardation. Of the remaining 50 children, three from the I ± T4 group and 14 from the no-I ± T4 group (χ2 = 10.2, p = 0.0014) exhibited borderline intellectual functioning (FSIQ: 70–84 points). Therefore, the overall prevalence of borderline or defective cognitive function was more than threefold higher in the children of mothers not using iodized salt compared with those mothers using it (76.9% vs. 23.1%, OR 7.667 [CI 2.365–24.856], χ2 = 12.65; p = 0.0001).
Relationship between cognitive outcomes and possible confounders
In order to assess the possible dependency of IQs on explanatory variables and confounders, univariate logistic regression models were estimated (Table 4). These analyses showed a significant positive association of adjusted maternal UIEs with both FSIQ (exp β = 1.021 [CI 1.001–1.041]; p = 0.04) and VIQ (exp β = 1.022 [CI 1.002–1.042]; p = 0.03). After adjustment for maternal age, adjusted maternal UIE was the only factor independently associated with VIQ (exp β = 1.023 [CI 1.003–1.043]; p = 0.028).
Significant values are shown in bold.
Based on the high, although not statistically significant, exp β value associated with breastfeeding, the dependency of IQs on this factor in the two subgroups of mothers using and not using iodized salt was also calculated. However, no association was identified (exp β = 5.667 [CI 0.818–39.267]; p = 0.079).
Discussion
To examine associations of the iodine status of pregnant women or their thyroid function during pregnancy with the mental development of their children, this pilot, prospective, observational study was designed to compare school-age children born to women who had been using iodized salt long before becoming pregnant (supplemented mothers) with children born to women who had never used it (unsupplemented mothers). A further stratification based on maternal LT4 treatment that was started before conception and uninterruptedly continued during pregnancy, either in association or not in association with iodized salt consumption, eventually allowed the effect of maternal nutritional iodine status to be assessed against maternal serum fT4 concentrations on cognitive outcome in the progeny.
It was found that children born to mothers with similar nutritional iodine status showed comparable intellectual abilities. Specifically, no differences in IQs were observed between I and I + T4 children or between no-I and no-I + T4 children, which was largely independent of mothers' gestational fT4 concentrations. Conversely, the children of mothers on LT4 treatment (I + T4 and no-I + T4) performed differently in IQ tests, despite their mothers having had consistently similar fT4 concentrations throughout gestation. Taken as a whole, these findings suggest that neuro-intellectual outcomes in children may be more dependent on their mothers' nutritional iodine status than on maternal T4 levels throughout gestation. Indeed, logistic regression models designed to assess the dependence of suboptimum cognitive outcomes (IQ <85 points) on various explanatory variables failed to show a significant association with maternal thyroid parameters at any stage in pregnancy. Conversely, maternal nutritional iodine status proved to be positively associated with cognitive outcomes. Overall, children born to supplemented mothers had FSIQ, VIQ, and PIQ scores that were 13, 14, and 10 points higher, respectively, than those recorded for children born to unsupplemented mothers. In addition, individual data analysis showed that >40% of the children studied had defective cognitive outcomes, and the vast majority were born to mothers not using iodized salt. Accordingly, the risk of impaired cognitive function for children exposed to higher degrees of maternal ID was found to be almost eight times that of children whose mothers had more adequate iodine status. Notably, a high frequency (approximately 20%) of defective IQs was observed, even among children of supplemented mothers. Although other potential causes of poor neuro-intellectual development may not be excluded, the present findings suggest that iodine supplementation by means of iodized salt alone may be inadequate to guarantee normal neurodevelopment. The region where the study was conducted is a small and iodine-deficient mountain area (approximately 600 m above sea level), which is quite far from the coast. The diet of the population in this area is mainly based on a Mediterranean-style food system. Staple foods include starchy foods, vegetables, legumes, milk and dairy products, olive oil, and fruits, which are almost exclusively locally produced. Seafood is only occasionally consumed, and the protein supply generally comes from meat obtained from animals raised in local small-scale livestock farms. Due to the long-standing ID in this area, this food system proves to be inadequate for providing physiological iodine requirements, as demonstrated by the description of several iodine-deficiency disorders affecting people living in this region (14,29,30). In these circumstances, the contribution of iodized salt to iodine nutrition becomes quite relevant, although it is unlikely to be sufficient for meeting the increased iodine requirements during pregnancy and lactation.
Since cognitive development is affected by several factors, it cannot definitely be ruled out that confounders other than those controlled for in the study are to some extent involved. However, in the absence of any association between cognitive outcomes and maternal thyroxinemia, the less favorable cognitive outcomes observed in the children of unsupplemented mothers might be the result of the developing brain being exposed to insufficient fetal TH levels as a consequence of low iodine availability. This hypothesis would provide a unifying explanation both for the absence of differing IQs in children born to mothers not using iodized salt and for the much better cognitive outcomes of children born to mothers with more adequate iodine intake during pregnancy. In this view, the relative contribution of the fetal thyroid to neurodevelopment would not be secondary to that of the mother, which is a hypothesis that is in agreement with the evidence that children affected by congenital hypothyroidism, even when treated early, may still exhibit subtle and specific neurocognitive deficits (39,40). The relevance of fetal thyroid contribution to neurodevelopment is further supported by the evidence of poorer cognitive outcomes reported in preterm infants with hypothyroxinemia compared with preterm euthyroid infants (41).
To some extent, the present results are in agreement with those of Lazarus et al. in the Controlled Antenatal Thyroid Screening Study (CATS), who reported that use of LT4 therapy for mild maternal hypothyroidism made no difference to cognitive outcomes (24). Possible explanations for the negative results of this study were recently provided by Taylor et al. in a retrospective analysis of almost 500 mother–child pairs from the CATS population. The authors of that study postulated that exposure to perchlorate during intrauterine life might have played a role in reducing fetal TH production by disrupting fetal thyroidal iodine uptake. In fact, maternal perchlorate levels in the highest 10% of the population were associated with increased odds of offspring having an IQ of <80, with a greater negative impact observed on VIQ than PIQ (42). Interestingly, similar results for VIQ have also been reported in a recent study conducted in the UK aimed at investigating the association between maternal iodine status and child IQ at age 8–9 years (5). In their study, Bath et al. clearly demonstrated that, far from being confined to infants of mothers with very low iodine status, the children of mild-to-moderate ID mothers also had an enhanced risk of suboptimum cognitive scores. A decline in VIQ with decreasing maternal iodine status was also observed in the present small series of children. Significant differences were found between VIQ and PIQ only in the children of unsupplemented mothers, which is a finding further confirmed by evidence of an association between low maternal urinary iodine and defective VIQ.
A relatively low VIQ score may suggest underlying central auditory processing disorders (cAPDs), which are characterized by difficulties in the perceptual processing of auditory information in the central nervous system of individuals with normal peripheral hearing (43,44). Persisting abnormalities in auditory processing and selective attention has been reported possibly to influence cognitive development in children with congenital hypothyroidism who are diagnosed and treated early (45). Similarly, a cAPD that influences working memory has recently been proposed to be responsible for reduced outcomes in areas of literacy in children of mothers with a gestational UIE below the current established cutoff point for sufficiency (150 μg/L) (6). Interestingly, causes of cAPDs may include misplaced cells in the auditory cortical areas and/or delay in myelin maturation (46,47). Both of these processes are known to be TH regulated, the first occurring at early stages of neurodevelopment under the control of both maternal and fetal TH, and the second beginning in mid/late gestation and continuing during postnatal development (48).
cAPDs cover a wide range of behavioral disorders, including specific learning disabilities, autism, and ADHD (44,49). The latter, reported by the authors in a population of children from the same area as those included in this study, was found to be strongly associated with ID-related early gestation maternal hypothyroxinemia (14).
This pilot study has several limitations, the first two being the relatively small size of the population studied and the fact that the design of the study did not include parental IQ testing. However, these limitations are to some extent attenuated by the fact that the children included in the study all grew up in the same narrow rural area and were from homogeneous socioeconomic and educational backgrounds. Indeed, no differences in the SES, evaluated by means of the Hollingshead Index, were observed between the different subgroups, and no association was found at logistic regression between children IQs and maternal and paternal education. In addition, stringent inclusion/exclusion criteria for both mothers and children were adopted, thus limiting the bias of known confounders potentially affecting overall results. Third, UIEs were not corrected for urinary volume. Nonetheless, several urine samples were obtained for each pregnancy, and adjusted mean UICs were calculated to account for day-to-day variations, which reduces the risk of misclassification of individual nutritional iodine status. Finally, the observational design of the current study and an inadequate power for the sample size do not allow us to draw firm conclusions, and therefore the results would theoretically need confirmation from larger, randomized controlled trials to determine the precise effects on child cognition of maternal iodine supplementation and LT4 during pregnancy. Whether such intervention studies in conditions of even mild ID would be ethical is currently disputed (50 –52). In our view, similar trials might be difficult to implement because they should include a study group of pregnant women (and their fetuses) deliberately exposed to the potential risks of gestational ID.
In conclusion, there is evidence that brain development is vulnerable to TH deficiency. In addition to affecting maternal thyroid function, a less than adequate maternal iodine intake during pregnancy potentially leads to insufficient fetal TH output due to reduced iodine storage in the fetal gland. The present findings provide evidence that mild-to-moderate ID during fetal development, even with the lack of maternal thyroid insufficiency, may result in cognitive impairment later in life, with a seemingly greater impact on verbal abilities. Close monitoring of maternal iodine intake before and during pregnancy is therefore strongly recommended to prevent impaired neurodevelopment in offspring. Although the results of this preliminary study might be partly biased by the relatively small sample size, they may be informative for the design and implementation of future and adequately powered studies.
Footnotes
Author Disclosure Statement
No competing financial interests exist. No funding was secured for this study.