
Abstract
Background:
The recent increase in the incidence of thyroid cancer has been mainly attributed to papillary thyroid microcarcinomas (PTMCs), and many studies have suggested conservative strategies for the diagnosis and treatment of PTMC. However, PTMCs may be associated with distant metastasis. This study aimed to evaluate the clinicopathological features and identify the risk factors for distant metastasis in patients with PTMCs.
Methods:
The medical records of 8808 patients who were diagnosed with PTMC from 1999 to 2012 were reviewed, and 12 (0.1%) patients with distant metastasis were identified. Forty-one PTMC patients who initially had lateral cervical lymph node (LN) metastasis and were cured with no evidence of a distant metastasis were also selected as a control group.
Results:
Of the 12 patients with distant metastasis, nine had synchronous metastasis and three had metachronous metastasis. All 12 patients had primary tumors >0.5 cm and cervical LN metastasis at initial surgery. Ten patients had clinically apparent lateral cervical LN metastases, while two patients had only microscopic involvement of a central LN. Four patients died of thyroid carcinoma. Disease-specific mortality was associated with old age, large metastatic LNs with extranodal extension, and aggressive pathologic subtype of metastatic LNs. When the clinicopathological features of the patients with distant metastasis were compared with the control patients, the presence of extranodal extension and change to an aggressive pathologic subtype of metastatic LNs were significantly associated with distant metastasis and persistent structural distant PTMC metastasis.
Conclusions:
Most patients with PTMC demonstrate excellent clinical outcomes, and distant metastases rarely occur. However, distant metastasis of PTMC can be fatal. Performing a meticulous pathologic examination of metastatic LNs to identify the presence of extranodal extension and the pathologic subtype of metastatic LNs helps to assess the risk of a distant metastasis in patients with PTMC.
Introduction
R
PTMCs are, however, sometimes associated with clinical cervical lymph node (LN) metastasis, locoregional recurrence, and, much less frequently, distant metastasis. According to previous studies, recurrence occurs in 4–7% of PTMC patients, and up to 40% of PTMCs are accompanied by cervical LN metastases (11,12). Large PTMCs (>0.5 cm), multifocal cancers, the presence of extrathyroidal extension, and the presence of LN metastasis at the initial presentation are known prognostic factors for PTMC recurrence (13 –19). Because of the rarity of distant metastases from a PTMC, the incidence and clinicopathological features of PTMCs that results in distant metastasis remain largely unknown.
The aims of this study were to evaluate the clinicopathological features of PTMCs with distant metastases and to identify the risk factors for this occurrence. Distant metastases are the main cause of cancer-specific mortality in thyroid cancer patients, and it would be helpful to determine the clinical risk factors that are predictive of distant PTMC metastasis as part of the personalized treatment and management of patients with PTMCs and small thyroid nodules.
Materials and Methods
Study subjects
From 1999 to 2012, 8808 patients were diagnosed with a PTMC after initial thyroid surgery at the Asan Medical Center, Seoul, Korea. All PTCs were ≤1 cm in diameter on the pathology reports for these cases. The medical records of these patients were reviewed, and 12 patients were found to have had distant metastasis. To evaluate the risk factors for distant metastasis from PTMC, patients were selected to serve as a control group who had clinically apparent lateral cervical LN metastasis at their first surgery but were cured after initial treatment with no evidence of distant metastasis. Forty-one patients who satisfied the following criteria were included in this control group (Fig. 1): (i) N1b disease at the initial surgery according to the Tumor Node Metastasis (TNM) staging system (20) with no evidence of distant metastasis; and (ii) no evidence of disease (NED) for five or more years after initial treatment. This study was approved by the Institutional Review Board of the Asan Medical Center, Seoul, Korea.
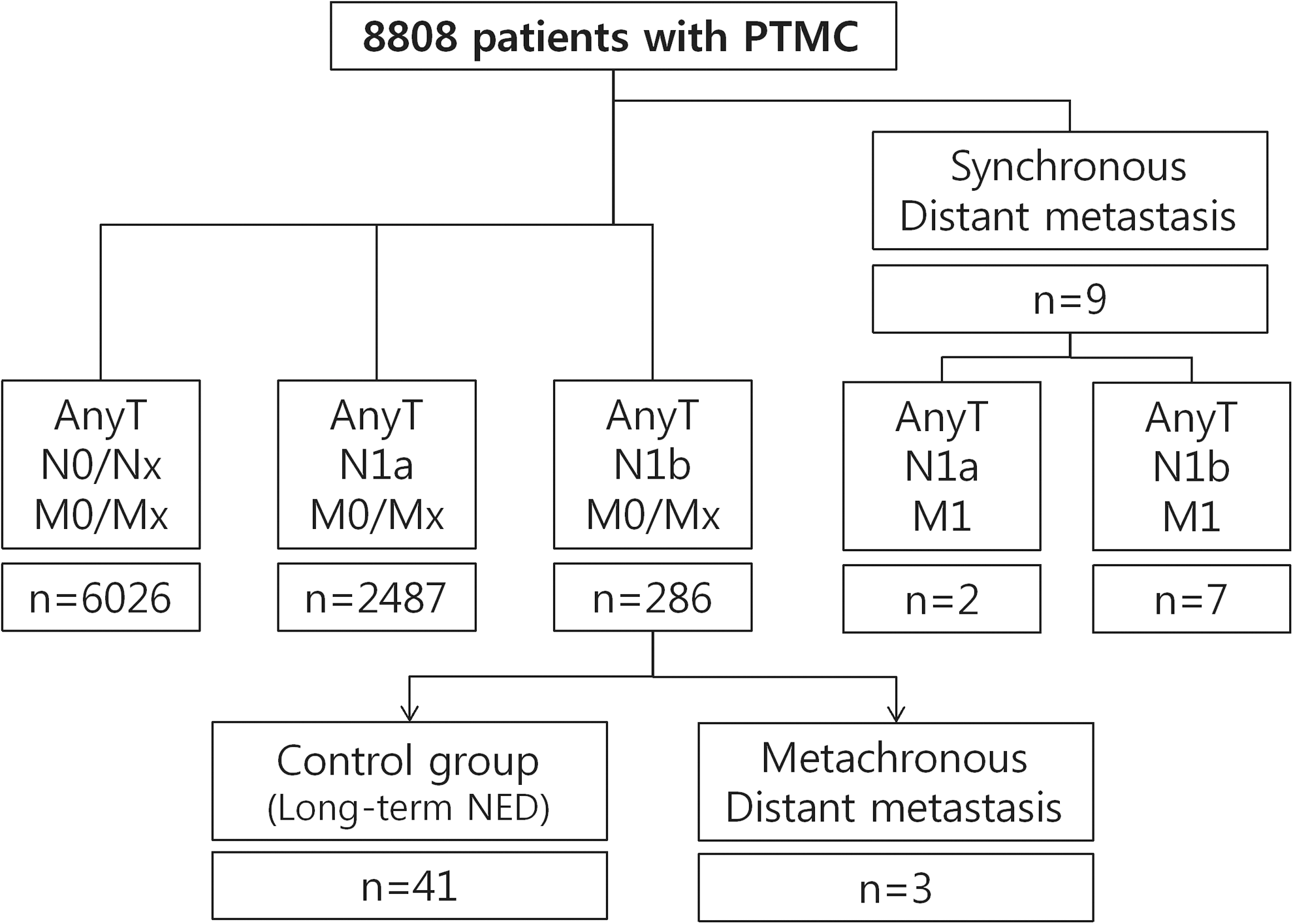
Description of the study cohort. The algorithm indicates how patients in the control group were retrieved. Forty-one patients who had N1b disease at the time of initial surgery and who were clinically cured for more than five years after initial treatment were classified as the control group. NED, no evidence of disease.
Histopathologic review
All the pathologic slides from patients with a distant metastasis and control patients were reviewed by an experienced pathologist (D.E.S.) without information of the clinical outcomes. The presence of aggressive (e.g., tall cell, columnar, and diffuse sclerosing variants) or other PTC variants of the primary thyroid tumors and metastatic cervical LNs were evaluated based on the World Health Organization's classification of endocrine tumors (21). For metastatic LNs, transformations into a poorly differentiated thyroid carcinoma or undifferentiated (anaplastic) carcinoma were also evaluated. The N category status of all patients was classified based on the TNM staging system (20). The maximal size of metastatic foci of the metastatic LNs was measured across the greatest dimension, and the presence of extranodal extension was diagnosed when tumor cells were identified in the extracapsular area in the background of a desmoplastic reaction.
Surgical treatment and radioactive iodine ablation
Patients who had clinically apparent cervical LN metastasis, bilateral multifocal PTMCs, or PTMCs with indeterminate nodules in the contralateral lobe were treated by total thyroidectomy, whereas the other patients were treated by hemithyroidectomy. Prophylactic central neck dissection was routinely performed, and therapeutic central and lateral neck dissection was performed in patients with clinically apparent lateral cervical LN metastasis. Radioactive iodine (RAI) remnant ablation after total thyroidectomy was performed in patients with cervical LN metastases, multifocal PTMCs, or extrathyroidal extension according to the pathology report.
Follow-up protocol
After initial therapy, patients took levothyroxine for thyrotropin (TSH) suppression, and were regularly followed up with physical examinations, as well as the measurement of thyroid function, serum thyroglobulin (Tg), serum anti-Tg antibody (TgAb), and neck ultrasound every 6–12 months. Diagnostic RAI whole-body scans (WBS) with measurement of the serum-stimulated Tg (sTg) level were also performed 12–24 months after the initial therapy in patients who underwent total thyroidectomy and RAI remnant ablation. Additional diagnostic imaging studies, such as computed tomography, magnetic resonance imaging (MRI), or whole-body fluoro-deoxyglucose (FDG)-positron emission tomography (PET), were also performed in patients with inappropriately high serum Tg levels (22).
Definitions
Synchronous metastases were defined as distant metastases that were confirmed prior to surgery for thyroid cancer, during RAI ablation, or within six months after RAI ablation, as previously described (23). Metachronous metastases were defined as distant metastases that were detected more than six months after RAI ablation. Patients were considered to have NED when they presented with a serum Tg level of ≤1 ng/mL, negative serum TgAb, and negative imaging findings at the end of follow-up. Patients were considered to have biochemical persistent disease if the serum-stimulated or suppressed Tg level was >1 ng/mL or if TgAb were positive but there was no pathological, cytological, or radiological evidence of persistent disease at the end of follow-up. Structural persistent disease was defined as pathologically or cytologically proven recurrent or metastatic disease and/or metastatic lesions in other distant organs on imaging studies (22).
Statistics
R studio v0.98.1091 and R libraries survival, pROC, and gdata were used to analyze data (R Foundation for Statistical Computing;
Results
Baseline characteristics of the PTMC patients
The median age of 8808 patients with PTMC was 49 years (IQR 41–55 years), and 7323 patients (83%) were female (Table 1). The median PTMC tumor size was 0.6 cm (IQR 0.5–0.8 cm). A total thyroidectomy was performed in 4183 patients (56%), and RAI remnant ablation was performed in 2689 patients (31%). Central cervical LN metastasis (N1a) and lateral cervical LN metastasis (N1b) were confirmed in 2489 patients (28%) and 293 patients (3%), respectively. Recurrent disease was found in 128 patients with PTMC (1.5%) during the median 7.7 years of follow-up. Twelve patients (0.1%) had distant metastasis, and four patients died due to PTC during follow-up.
Continuous variables are presented as medians with interquartile ranges. Categorical variables are presented as number with percentages.
PTMC, papillary thyroid microcarcinoma; LN, lymph node; RAI, radioactive iodine.
Clinicopathological features of the patients with a distant metastasis from PTMC
Nine of the 12 PTMC patients with a distant metastasis (75%) had a synchronous metastasis, and three of these patients had a metachronous metastasis (Fig. 1). The clinicopathological features of these 12 patients with distant metastasis are summarized in Table 2.
Stage was determined using the Tumor Node Metastasis staging system (7th edition).
Combined clear cell feature (<50%).
PTC, papillary thyroid cancer; LN, lymph node; ENE, extranodal extension; RAI, radioactive iodine therapy; S, synchronous metastasis; M, metachronous metastasis; NED, no evidence of disease; PD, poorly differentiated; ICH, intracranial hemorrhage; RFA, radiofrequency ablation; RTx, radiation therapy; CCRTx, concomitant chemoradiation therapy; GKRS, gamma-knife radiosurgery.
The median age of these patients was 58 years (IQR 55–63 years), and 11 patients (92%) were older than 45 years of age. Ten of these patients (83%) were female (Table 3). Five patients were asymptomatic, and PTMC had been detected by neck US screening. PTMC was detected in one case during an evaluation for lung nodules. Six patients had symptoms (e.g., palpable mass, hoarseness) at the initial diagnosis due to large metastatic cervical LNs.
Continuous variables are presented as medians with interquartile ranges; categorical variables are presented as numbers with percentages.
OR, odd ratio; CI, confidence interval; LN, lymph node.
All 12 patients had primary tumors >0.5 cm and cervical LN metastasis at their initial surgery. Ten patients had clinically apparent lateral cervical LN metastasis (N1b), but two patients had only central cervical LN metastasis (N1a) with small metastatic foci. Of these two patients, one presented with a pulmonary metastasis, and the other had tall-cell variant PTC. The pathology of the primary PTMC in 8/12 patients (67%) was classical PTC, two patients (17%) had an infiltrative follicular variant PTC, and one patient (8%) had a solid variant PTC. An aggressive tall-cell variant of primary PTMC was found in one patient (8%). In five patients (42%), the pathology of the metastatic cervical LNs changed to an aggressive subtype. The dominant pathologic subtypes in the metastatic LNs were tall-cell variant (patients 7 and 11), columnar cell variant (patient 9), poorly differentiated carcinoma (patient 12), and anaplastic carcinoma (patient 10; Fig. 2).
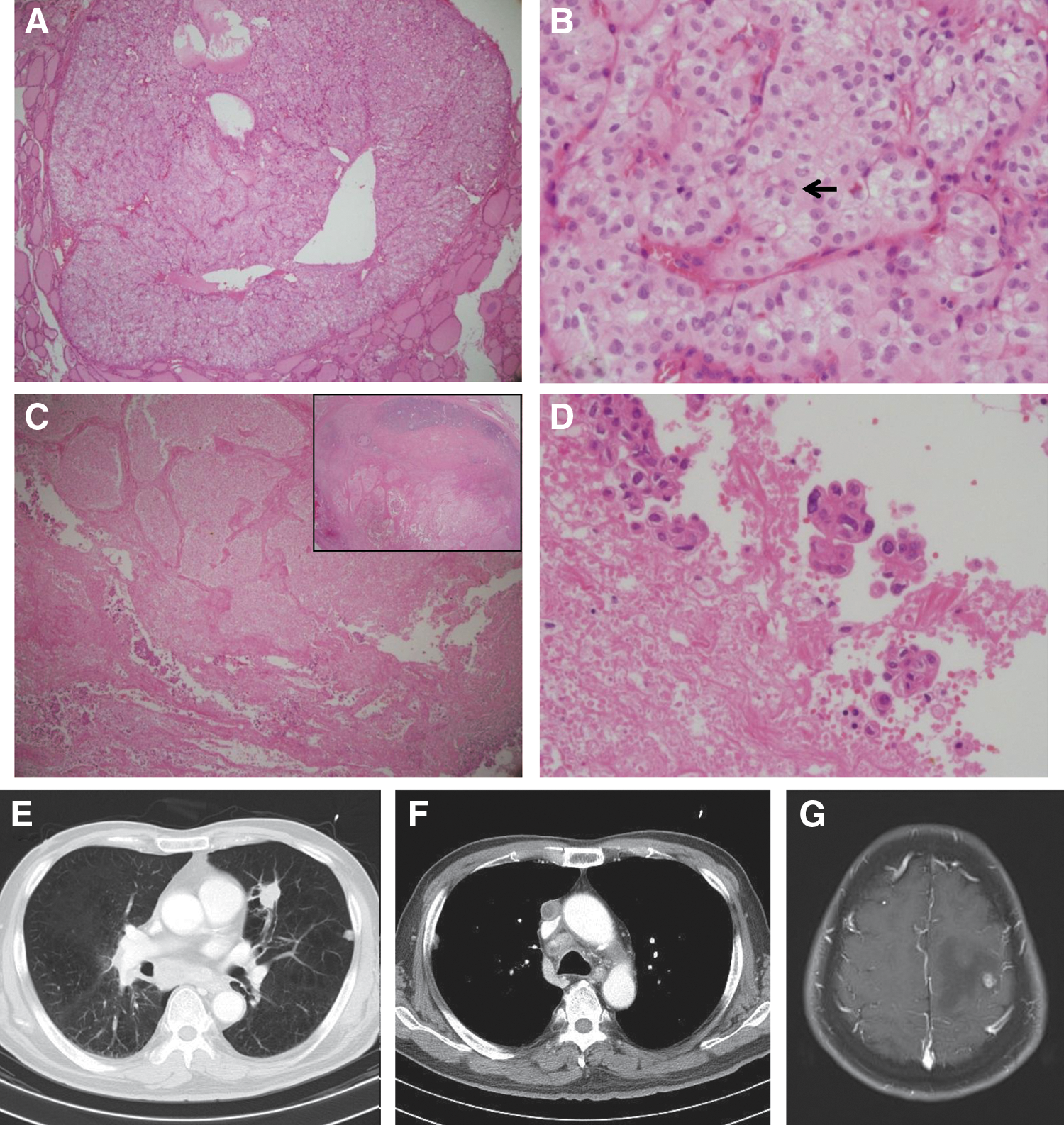
Pathologic and radiologic findings of patient 10 with distant metastasis of a PTMC. (
All 12 patients had lung metastasis. Five patients had an additional bone metastasis, and two patients had a brain metastasis. Patients were individually treated based on their disease status. High-dose RAI therapy was performed in all patients, and the tumors were RAI avid in seven patients (58%). At the end of the follow-up period, three patients were classified as NED after repetitive high-dose RAI therapy, and their metastatic lesions were RAI avid. Four patients had persistent disease, including one case of biochemical persistent disease and three cases of structural persistent disease. Five patients died during the follow-up, four due to the progression of metastatic PTC (cancer-specific mortality) and one with structural persistent disease who died due to intracranial hemorrhage.
Risk factors predictive of distant PTMC metastases
To evaluate risk factors that were predictive for distant metastasis of PTMC, the various clinicopathological features of the 12 PTMC patients with distant metastasis were compared with those of a control group of patients (Fig. 1 and Table 3). As a control group, 41 patients were selected who had N1b disease without distant metastasis and were classified as NED after initial therapy. The median follow-up period of the patients in the control group was 7.3 years.
The patients with distant metastasis were older and more likely to have large metastatic cervical LNs, a change to an aggressive pathologic subtype of metastatic LNs, and extranodal extension in comparison with the control patients. By univariate analysis, age ≥45 years, metastatic foci in LNs measuring ≥1.7 cm, change to an aggressive pathologic subtype of metastatic LNs, and presence of extranodal extension were significant risk factors for predicting a distant metastasis of PTMC. By multivariate analysis, extranodal extension of metastatic foci from cervical LNs was an independent risk factor (odds ratio [OR] 5.50; [confidence interval (CI): 1.08–33.64]; p = 0.045; Table 3). Change to an aggressive pathologic subtype of metastatic LNs was a marginally significant factor (OR 9.89 [CI: 1.07–227.35]; p = 0.068).
Additional analyses were performed to evaluate the risk factors for persistent structural metastasis in PTMC patients after additional therapy. Patients with persistent metastasis were all older than 45 years of age and were significantly older than control patients were. Change to an aggressive pathologic subtype of metastatic LNs (OR 34.55 [CI: 1.63–2451.42]; p = 0.039) and the presence of extranodal extension (OR 17.62 [CI: 1.56–629.36]; p = 0.042) were independent risk factors by multivariate analysis (Table 4).
Continuous variables are presented as medians with interquartile ranges; categorical variables are presented as numbers with percentages.
N/A, not available.
Discussion
The clinicopathological features of PTMC, particularly distant metastases from PTMC, were evaluated in 12 patients treated at the authors' hospital. The current study series of 8808 patients with PTMC is the largest reported to date, and this study is the first to describe the risk factors of distant metastasis in PTMC patients using statistical analysis (12,15,17,18). The incidence of distant metastasis from PTMCs was found to be only 0.1% in the current study. All 12 PTMC patients with distant metastasis had primary tumors >0.5 cm and cervical LN metastasis at the time of initial surgery. Ten of the 12 patients had clinically apparent lateral cervical LN metastases. Four of these 12 patients (33%) died due to the progression of distant metastasis, and only three patients (40%) were disease free after additional therapy. Disease-specific mortality was found to be associated with old age, large metastatic LNs with extranodal extension, and a change to an aggressive pathologic subtype of metastatic LNs. Patients who were disease free despite having distant metastases were asymptomatic and had RAI-avid metastatic lesions.
The clinicopathological features associated with distant metastasis of PTMC were also evaluated by comparison with a control group of patients with N1b disease and NED without distant metastasis over a five-year follow-up. Most patients with distant metastasis had lateral cervical LN metastasis at their initial treatment, and only one case of distant metastasis was confirmed after five years after initial therapy. These were the reasons for the selection criteria for the control group. The presence of an extranodal extension and change to an aggressive pathologic subtype of metastatic LNs were found to be significantly associated with distant metastasis and persistent structural distant metastasis of PTMC. These findings are consistent with previous studies, and confirm the prognostic role of extranodal extension and the pathologic subtype of metastatic cervical LNs (24 –28). The current data suggest that cervical metastatic LNs excised at the initial surgery should be carefully examined for extranodal extension and the pathologic subtype to assess the risk of distant metastasis in PTMC patients. The findings also suggest that there is little possibility of distant PTMC metastases if there is no preoperative evidence of any cervical LN metastasis.
The present study emphasizes the significance of LN metastasis in PTMC patients as a major source of further distant metastasis and supports the concept of a metastatic cascade, suggesting that cancers sequentially progress from primary tumors to LNs and then systematically to distant organs with sequential mutations (29). A certain specific LN microenvironment in metastatic LNs might induce indolent cancer cells from the primary tumor to develop aggressive properties and promote systemic progression with disease persistency (30). The presence of an extranodal extension and a change to an aggressive pathologic subtype of metastatic LNs was associated with distant metastasis and persistent metastatic PTMC in the analysis, and these morphologic changes might reflect the aggressive properties of the cancer cells. The size of the metastatic foci in metastatic LNs might also affect the LN microenvironment, but this was not found to be associated with prognosis.
Two of the PTMC patients with only central neck LN metastasis had synchronous distant metastasis. In these cases, there was no evidence of lateral cervical LN metastasis either preoperatively or during the follow-up period. These cases suggest that systemic dissemination of cancer cells may also occur during early cancer development, and their primary cancers may already have the intrinsic properties leading to metastasis (29). In these patients, molecular analysis would have helped to determine the mechanisms underlying the onset of the distant metastasis, but we could not perform mutational tests because the remnant primary tumor tissues in paraffin blocks were too small and old to perform adequate analyses. One recent study has reported that cyclin D1 overexpression in PTMC is associated with fatal outcomes, but common oncogene mutations such as BRAF or RAS mutations were not involved (27). Further studies that identify the molecular markers underlying PTMC aggressiveness are essential to develop personalized treatment regimens and avoid the under- or overtreatment of PTMC patients.
Despite the large number of patients in the initial study cohort, the incidence of distant metastasis from PTMC was too low to perform meaningful statistical analyses. Therefore, control patients were selected from the initial PTMC population who had N1b disease without distant metastasis. This approach limits the generalizability of the findings to all PTMC patients. Also, only non-incidental clinical PTMCs were analyzed (12), and the findings cannot be applied to surgical decision making. According to recent guidelines, patients with clinically suspicious cervical LN metastasis should undergo total thyroidectomy (31). However, the present findings might assist future decision making regarding RAI therapy and the doses for RAI remnant ablation (32). Based on the results of the current study, it would be appropriate to recommend RAI remnant ablation using high activity 131I for PTMC patients who have metastatic LNs with extranodal extension or an aggressive pathologic subtype. The findings also suggest that the pathologic extent of disease alone is insufficient for predicting disease aggressiveness (33). In general, PTMC is an early-stage thyroid cancer with a less extensive disease burden. However, clonal evolution in cancer, regardless of disease extent, might promote cancer progression.
In conclusion, most patients with PTMC demonstrate excellent clinical outcomes, and distant metastasis from PTMCs is a rare occurrence. However, distant metastasis from PTMCs can be fatal. Cervical LN metastasis with extranodal extension or aggressive pathologic subtypes are associated with distant metastasis in PTMC patients. A meticulous pathologic examination of metastatic LNs helps to assess the risk of distant metastasis from PTMCs.
Footnotes
Acknowledgments
This study was supported by a National Research Foundation (NRF) of Korea research grant (no. NRF-2012R1A1A2038383) and a research grant of the Korean Foundation for Cancer Research (no. CB-2011-03-02).
Author Disclosure Statement
The authors have nothing to disclose.