
Abstract
Background:
Studies have demonstrated an association of the BRAFV600E mutation and microRNA (miR) expression with aggressive clinicopathologic features in papillary thyroid cancer (PTC). Analysis of BRAFV600E mutations with miR expression data may improve perioperative decision making for patients with PTC, specifically in identifying patients harboring central lymph node metastases (CLNM).
Methods:
Between January 2012 and June 2013, 237 consecutive patients underwent total thyroidectomy and prophylactic central lymph node dissection (CLND) at four endocrine surgery centers. All tumors were tested for the presence of the BRAFV600E mutation and miR-21, miR-146b-3p, miR-146b-5p, miR-204, miR-221, miR-222, and miR-375 expression. Bivariate and multivariable analyses were performed to examine associations between molecular markers and aggressive clinicopathologic features of PTC.
Results:
Multivariable logistic regression analysis of all clinicopathologic features found miR-146b-3p and miR-146b-5p to be independent predictors of CLNM, while the presence of BRAFV600E almost reached significance. Multivariable logistic regression analysis limited to only predictors available preoperatively (molecular markers, age, sex, and tumor size) found miR-146b-3p, miR-146b-5p, miR-222, and BRAFV600E mutation to predict CLNM independently. While BRAFV600E was found to be associated with CLNM (48% mutated in node-positive cases vs. 28% mutated in node-negative cases), its positive and negative predictive values (48% and 72%, respectively) limit its clinical utility as a stand-alone marker. In the subgroup analysis focusing on only classical variant of PTC cases (CVPTC), undergoing prophylactic lymph node dissection, multivariable logistic regression analysis found only miR-146b-5p and miR-222 to be independent predictors of CLNM, while BRAFV600E was not significantly associated with CLNM.
Conclusion:
In the patients undergoing prophylactic CLNDs, miR-146b-3p, miR-146b-5p, and miR-222 were found to be predictive of CLNM preoperatively. However, there was significant overlap in expression of these miRs in the two outcome groups. The BRAFV600E mutation, while being a marker of CLNM when considering only preoperative variables among all histological subtypes, is likely not a useful stand-alone marker clinically because the difference between node-positive and node-negative cases was small. Furthermore, it lost significance when examining only CVPTC. Overall, our results speak to the concept and interpretation of statistical significance versus actual applicability of molecular markers, raising questions about their clinical usefulness as individual prognostic markers.
Introduction
T
The BRAFV600E mutation is the most common genetic mutation in PTC (11,12). The p.BRAFV600E mutation is caused by a c.1799 T > A transversion that results in a constitutively activated mitogen-activated protein kinase (MAPK) pathway, leading to tumorigenesis (13) and distinct biological consequences (14). The prevalence of the BRAFV600E mutation varies between the different histological subtypes of PTC (12). The tall-cell variant of PTC (TCVPTC) has the highest prevalence at 93% (15), followed by classical variant of PTC (CVPTC), comprising up to 75.3% (11), and lastly, follicular variant of PTC (FVPTC) at only 25% (16). Some studies have shown that the BRAFV600E mutation is associated with aggressive clinicopathologic features, such as extrathyroidal invasion, multifocality, lymphovascular invasion, large tumor size, local lymph node metastasis, distant metastasis, and advanced disease stages (17 –22), whereas others studies have demonstrated no association between the BRAFV600E mutation and aggressive features (23 –30). In a previous retrospective study, the BRAFV600E mutation was found to be an independent predictor of CLNM in the overall cohort of patients with PTC (23). However, this relationship lost significance when only CVPTC was included in the analysis (23). Despite the discrepancies that exist in the literature, some studies have suggested the incorporation of BRAFV600E mutation into the management algorithm of PTC to improve perioperative decision making (9,17,18,20,22). However, the usefulness of BRAFV600E in predicting the presence of LNM remains questionable (23,31).
The recent expansion of knowledge and the ongoing effort to characterize PTCs genetically by The Cancer Genome Atlas (TCGA) research thyroid working group have also suggested that micro-RNAs may influence the PTC phenotype and thereby play an important role in its prognosis (12). MicroRNAs (miRs) are small non-protein coding RNA molecules that are 21–25 nucleotides in length. They regulate gene expression at the post-transcriptional level by binding to imperfectly complementary sequences within target mRNAs, often in the 3′-untranslated regions, thereby leading to degradation or translational suppression (32). Although definitive studies are currently lacking, miRs may nevertheless have potential as prognostic indicators in PTC, thereby optimizing the surgical management of patients with PTC (28,33 –44).
The BRAFV600E mutation and miRs have the potential to guide surgical decision making. However, most previous studies were retrospective, and did not include patients who had undergone routine CLND, challenging the validity of the findings. This underscores the need for well-designed prospective studies involving routine CLND to investigate whether the BRAFV600E mutation and miRs are independent predictors of aggressive clinicopathologic features before it can be recommended that these molecular markers be incorporated into the management algorithm for patients with PTC.
Accordingly, a multi-institutional prospective study was carried out that included consecutive patients who underwent total thyroidectomy (TT) and routine CLND at four tertiary endocrine surgery centers between January 1, 2012, and June 30, 2013. The objective was to determine, by multivariable analysis, whether the BRAFV600E mutation and miR expression levels of seven selected miRs are associated with aggressive clinicopathologic features of PTC. Their association with CLNM was examined in the subset of patients undergoing prophylactic rather than therapeutic CLND, in order to explore their potential future value as factors to assist in guiding the treatment of patients with PTC, specifically whether to perform prophylactic CLND in the absence of clinically apparent LNM.
Material and Methods
Patients and data collection
Under Institutional Review Board approval and patient consent, a prospective multi-institutional study was conducted that included Johns Hopkins Hospital, Weill Cornell Medical Center, the University of Michigan Health Systems, and the Mayo Clinic. This study was designed as validation of an initial retrospective pilot study (23). Consecutive patients between January 1, 2012, and June 30, 2013, diagnosed with PTC preoperatively on cytopathology or intraoperatively on frozen section and with a tumor size ≥1 cm were prospectively enrolled and included. Patients were operated on by surgeons who routinely perform TT and prophylactic CLND for patients with PTC ≥1 cm. At all centers, a unilateral CLND was performed, as described by Carty et al. (45), unless there was evidence of positive disease midline or contra-laterally in which case bilateral dissection was performed. Patients with suspicious or cytologically positive lymph node metastasis detected on ultrasound or by intraoperative evaluation underwent therapeutic CLND and were excluded, whereas those patients that did not exhibit signs of lymphadenopathy either pre- or intraoperatively, by definition, underwent a prophylactic CLND.
Clinical variables examined included patient age, sex, history of radiation exposure, and family history of thyroid cancer. Surgical pathology reports were reviewed for the following: tumor size, PTC subtype, presence LNM, extrathyroidal extension (ETE), multifocality, lymphovascular invasion (LVI), involvement of surgical margins, and American Joint Committee on Cancer (AJCC) stage.
Nucleic acid extraction
All molecular analyses were performed at Johns Hopkins Hospital. DNA and total RNA were extracted from formalin-fixed paraffin-embedded (FFPE) tumor samples, according to the protocol outlined by Kotorashvili et al. (46). Final DNA and RNA quantitation was determined by absorbance and fluorescence spectroscopy–based nucleic acid quantification using NanoDrop 2000c UV-Vis Spectrophotometer (Thermo Scientific) and Qubit® Fluorometric Quantitation (Life Technologies). PTC subtype and follicular and tall-cell architecture percentage was reviewed and confirmed by a single head and neck/endocrine pathologist (J.A.B.). Tumors were classified as FVPTC if they were 99% follicular patterned, and as TCVPTC if they had ≥50% tall-cell features.
BRAFV600E mutation detection
Detection of the BRAFV600E
mutation was performed in all cases by pyrosequencing. Polymerase chain reaction (PCR) amplification of a 124-base region of BRAF exon 15 surrounding c.1799T was performed using 20–200 ng genomic DNA and 0.2 M 5′-GAA GAC CTC ACA GTA AAA ATA G-3′ (forward) and 5′-biotin-ATA GCC TCA ATT CTT ACC ATC C-3′ (reverse) primers, along with HotStarTaq DNA polymerase (Qiagen), according to the manufacturer's instructions. Thermocycling parameters were as follows: 95°C for 15 min, followed by 42 cycles of 95°C for 20 sec, 53°C for 50 sec, 72°C for 20 sec, followed by 72°C for 5 min. Pyrosequencing was performed using the Pyromark-24 and sequencing reagents (Qiagen), according to the manufacturer's instructions, with the sequencing primer 5′-GAC CTC ACA GTA AAA ATA GGT GAT TTT G-3′. The pyrosequencing assay used was designed to detect all reported COSMIC (catalog of somatic mutations in cancer;
miR analysis
Promising miR candidates for predicting aggressiveness were selected based on results from the TCGA thyroid study (12) and a recent systematic review of the literature (50). MiRs-21, -146-3p, -146-5p, -204, -221, -222, and -375 were measured along with candidate reference miR-16 in technical triplicates. Reverse transcription for each specific miR was performed using 2 μL (10 ng/μL) of total RNA for a total RT-PCR reaction of 12 μL. For the qPCR step, cDNA was diluted with 20 μL of water, and 2 μL of diluted cDNA added to 10 μL of master mix for total volume of 12 μL per qPCR reaction (TaqMan® MicroRNA Reverse Transcription kit, TaqMan ® Universal Master Mix II, not containing Uracil-N glycosylase [UNG], and TaqMan® MicroRNA assays; Life Technologies). MicroRNA TaqMan® assays and their part numbers from Life Technologies were: miR-21-5p (000397), miR-146b-5p (001097), miR-146b-3p (002361), miR-204 (000508), miR-221 (000524), miR-222 (002276), miR-375 (000564), and miR-16-5p (000391).
In order to minimize batch effects, samples from all contributing centers were randomized on the microtiter plates. Mean Ct values were calculated for each sample and normalized against miR-16 to obtain dCT values. MiR-16-5p was used as endogenous control to normalize miR expression levels based on prior publications (43,51 –55) as well as available TCGA thyroid data, where miR-16 appears as relatively invariant within thyroid tumor samples (12). Mean dCt values relative to expression of miR-16 were normally distributed in the data set.
Data analysis
Power calculation
The study sample size was calculated based upon the proportional prevalence of BRAFV600E mutations and the prevalence of lymph node metastases in patients treated for PTC reported in previous studies. The BRAFV600E mutation has been reported in 29–83% of patients with PTC overall (56), with the smallest proportion (29%) reported by Namba et al. (57). To be conservative, this sample-size calculation assumes that the BRAFV600E mutation will be present in 25% of study subjects overall. Based upon the assumption that LNM will be present in 18% of BRAFV600E -negative individuals and 38% of those who are BRAFV600E positive (58), a sample size of 224 individuals was required to examine the relationship between BRAFV600E status and lymph node metastasis with 80% power at an alpha level of 0.05 (two sided).
Statistical analysis
In order to explore the relationships between molecular markers, BRAFV600E
and miRs, and routine clinicopathologic features of PTC, a univariate analysis was performed on patient sex, age, tumor size, multifocality, LVI, involvement of surgical margins, ETE, CLNM, advanced AJCC stage, histological subtype, and follicular and tall-cell component percentage. In order to find significant molecular predictors of CLNM, a multivariable logistic regression analysis was performed, adjusting for established clinicopathologic predictors, including patient age ≥45 years, sex, tumor size >2 cm, multifocality, LVI, involvement of surgical margins, ETE, and follicular and tall-cell component. Since relative levels of expression of the studied miRs were highly correlated with each other, these analyses were performed examining one miR at a time. In addition, multivariable analysis was performed examining each molecular marker individually controlling for factors that potentially would have been available preoperatively, including patient age, sex, tumor size, BRAFV600E
mutation, and miR expression. To explore the possibility that variability in miR expression might be associated with the likelihood of CLNM in patients without indication of CLN involvement, only those patients who underwent prophylactic CLND both across the entire cohort and within the subset of patients diagnosed with CVPTC alone were examined. Since PTCs classified as CVPTC may harbor up to 98% follicular and up to 49% tall-cell components, the possibility that the follicular and tall-cell component percentages presented an influence in the CVPTC subgroup was also explored, and the respective percentages were included in the CVPTC analysis. Finally, statistical analyses for the entire cohort, including those who underwent therapeutic CLND, were performed and are presented in the Supplementary Data (Supplementary Data are available online at
Results
Demographics
A total of 237 patients underwent prophylactic CLND and were included in the study. The prophylactic cohort of 237 patients included 173 women (73%) and 64 men (27%) with a mean age of 47.7 ± 14.5 years and a mean tumor size of 2 ± 1.2 cm. Multifocality was observed in 95 (40%) cases, involvement of surgical margins in 34 (14%) cases, LVI in 30 (13%) cases, ETE in 55 (23%) cases, and CLNM in 101 (43%) cases. One hundred and seventy (72%) tumors were positive for the BRAFV600E mutation. In three cases (1.3%), the results were equivocal for at least one of the molecular analyses (BRAFV600E mutation or miR expression); these were therefore excluded from those specific analyses. One hundred and ninety-two cases had CVPTC (81%), 27 had FVPTC (11%), and 18 had TCVPTC (8%; Table 1).
Only includes those patients with positive disease.
Inverse dCt values relative to miR-16.
AJCC, American Joint Committee on Cancer; CLN, central lymph node; SD, standard deviation.
Predictors of CLNM in all PTC subtypes
Univariate logistic regression analyses in patients who underwent prophylactic neck dissection demonstrated significant positive association between the BRAFV600E mutation (p = 0.01), miR-146b-3p (p = 0.01), miR-146b-5p (p < 0.01), miR-221 (p = 0.04), miR-222 (p < 0.01), tumor size (p < 0.01), multifocality (p = 0.01), positive surgical margins (p < 0.01), LVI (p < 0.01), ETE (p < 0.01), and advanced AJCC stage (p < 0.01) with CLNM. Multivariable logistic regression analysis (Table 2), controlling for each molecular marker, sex, age, tumor size, multifocality, LVI, positive surgical margins, ETE, and histological subtypes, found only miR-146b-3p (p = 0.03), miR-146b-5p (p = 0.02), multifocality (p < 0.05), LVI (p < 0.01), and ETE (p < 0.01) to be independent predictors of CLNM. The BRAFV600E mutation (p = 0.05) was only found to have a borderline association with CLNM in this analysis (Table 2).
Formula: CLNM = molecular marker + sex + age (>45 years) + size (>2 cm) + FVPTC + TCVPTC + multifocality + LVI + ETE + involvement of margins.
Each row represents an independent postoperative predictor model performed for CLNM. In the prophylactic cohort, independent predictors for CLNM were miR-146b-3p, miR-146b −5p multifocality, LVI, and ETE.
Statistically significant.
CI, confidence interval; CLNM, central lymph node metastasis; ETE, extrathyroidal extension; FVPT, follicular variance of PTC; LVI, lymphovascular invasion; PTC, papillary thyroid cancer; RR, relative risk; TCVPTC, tall-cell variance of PTC.
In a second multivariable logistic regression analysis limited to predictors available preoperatively only (molecular markers, age, sex, and tumor size) in prophylactic CLND patients, the BRAFV600E mutation (p = 0.01), miR-146b-3p (p = 0.01), miR-146b-5p (p = 0.01), miR-222 (p = 0.01), and tumor size >2 cm (p < 0.05) were found to predict CLNM independently (Table 3). The relative expression levels of miR-146b-3p, miR-146b-5p, and miR-222 were associated with a 10%, 15%, and 16% increase in the relative risk of CLNM, respectively (Table 3 and Fig. 1). Notably, in the prophylactic CLND cohort, patients who were BRAFV600E positive had a 48% chance of harboring CLNM, whereas those who were BRAFV600E negative had a 28% chance, resulting in a sensitivity of 65.9%, a specificity of 46.5%, a positive predictive value of 47.6%, and a negative predictive value of 71.8% for the BRAFV600E mutation.
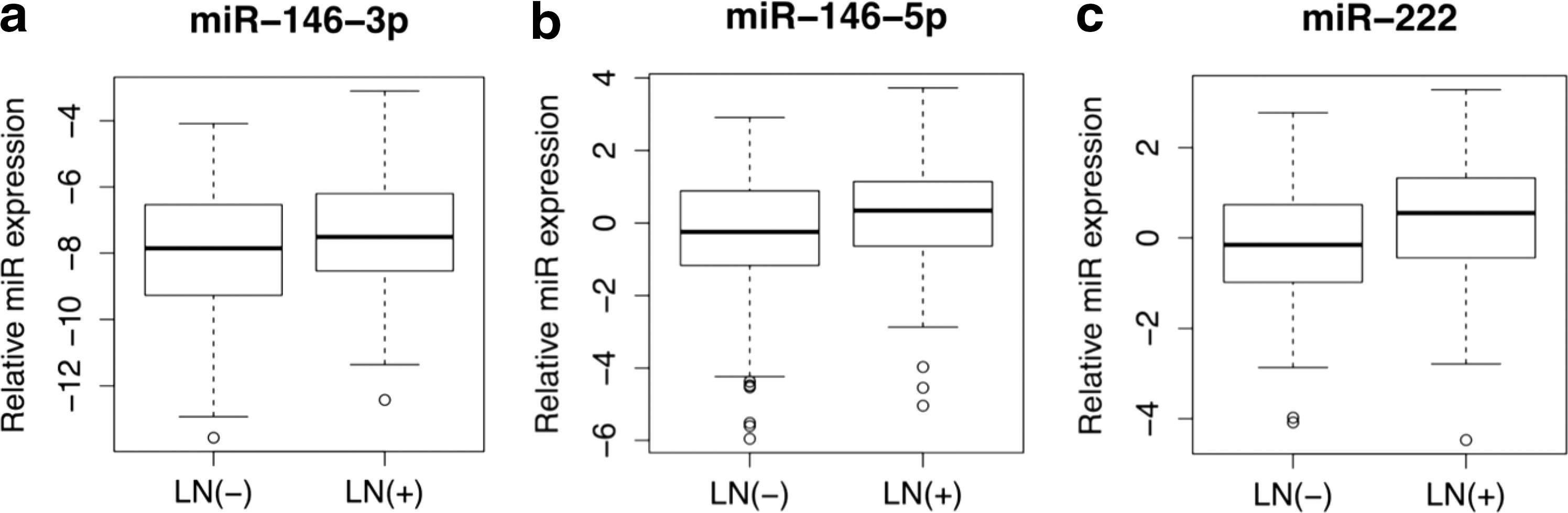
Micro RNA (miRNA) expression levels of predictive miRs in the prophylactic CLND subgroup (n = 237). Tukey boxplots showing medians, interquartile range (IQR), and whiskers extending to 1.5 × IQR showing the inverse dCt values of (
Each row represents an independent preoperative predictor model performed for CLNM. In the prophylactic cohort, independent preoperative predictors for CLNM were BRAFV600E mutation, miR-146b-3p, miR-146-5p, miR-222, and tumor size.
Statistically significant.
Predictors of CLNM in the CVPTC histological subtype
In univariate logistic regression analyses focusing on the 192 patients with CVPTC who underwent prophylactic neck dissection, miR-146b-3p (p = 0.03), miR-146b-5p (p < 0.01), miR-221 (p = 0.02), miR-222 (p < 0.01), tumor size >2 cm (p = 0.01), multifocality (p = 0.04), positive surgical margins (p < 0.01), LVI (p < 0.01), ETE (p < 0.01), and advanced AJCC stage (p < 0.01) were found to be associated with CLNM. Furthermore, miR-204 (p = 0.02) was inversely associated, and the BRAFV600E mutation (p = 0.12) and follicular and tall-cell component percentages were not found to be associated with CLNM. Multivariable logistic regression analysis of only CVPTC cases undergoing prophylactic neck dissections (Table 4), while controlling for each molecular marker, sex, age, size, multifocality, LVI, positive surgical margins, ETE, and follicular and tall-cell component, found only miR-146b-5p (p = 0.01) and miR-222 (p = 0.02), LVI (p < 0.01), and ETE (p < 0.05) to be independent predictors of CLNM. BRAFV600E was not significantly associated with CLNM in this subset (p = 0.09). Multivariable logistic regression analysis in all CVPTC patients, including only predictors available preoperatively (molecular markers, age, sex, and tumor size), found miR-146b-5p (p = 0.01), miR-221 (p = 0.03), miR-222 (p < 0.01), and size >2 cm (p < 0.05) to be independent predictors of CLNM. BRAFV600E was again not associated with CLNM (p = 0.09; Table 5).
Formula: CLNM = molecular marker + sex + age (≥45 years) + size (>2 cm) + FVPTC + TCVPTC + multifocality + LVI + ETE + involvement of margins.
Each row represents an independent postoperative predictor model performed for CLNM. In the prophylactic CVPTC subgroup, independent predictors for CLNM were miR-146b-5p, miR-222, LVI, and ETE.
Statistically significant.
CVPTC, classical variant of PTC.
Formula: CLNM = molecular marker + sex + age (>45 years) + size (>2 cm).
Each row represents an independent preoperative predictor model performed for CLNM. In the CVPTC prophylactic subgroup, independent preoperative predictors for CLNM were miR-146-5p, miR-221, miR-222, and tumor size.
Statistically significant.
Discussion
To the authors' knowledge, this is the largest prospective study to date examining the association of BRAFV600E and miRs with aggressive clinicopathologic variables of PTC, particularly the presence of CLNM. Due to current controversies in the surgical management of PTCs and prophylactic CLND as well as ambiguity in the literature, molecular markers that allow for risk stratification for the presence of CLNM would be invaluable in the clinical arena.
In the patients with no clinical indications of CLNM, where these molecular markers would be most valuable, miR-146b-3p, and miR-146b-5p were identified to be predictive of CLNM. Furthermore, because the clinical decision to perform a CLND is determined preoperatively, a multivariable analysis among prophylactic CLND patients, controlling for clinicopathologic variables that are available preoperatively (age, sex, and tumor size), is critical for the identification of molecular markers with clinical utility. This subgroup analysis of individual miRs identified elevated levels of miR-146b-3p, miR-146b-5p, and miR-222 as independent predictors of the presence of CLNM. More importantly, in this group, each doubling of expression of these markers was associated with a 10%, 15%, and 16%, increase in the risk of CLNM, respectively. These findings are consistent with previously reported studies that identified positive associations of these miRs with various features of PTC aggressiveness (28,33,34,37,39,40,42 –44,59). Three of the miRs investigated were found to predict CLNM in the multivariate model. Inspection of the bar graphs in Figure 1, however, clearly shows significant overlap in expression of these miRs in the two outcome groups, raising legitimate questions about their clinical usefulness as individual prognostic markers. Each doubling of expression of these markers was associated with increased risk of CLNM. Unfortunately, this only segregated CLND cases at higher levels of expression that were only seen in a few cases, providing only poor sensitivity at acceptable levels of specificity. These results speak to the concept and interpretation of statistical significance versus actual applicability of molecular markers clinically.
The BRAFV600E mutation was significantly associated with CLNM in patients undergoing prophylactic central neck dissection when specifically controlling for preoperatively available clinicopathologic variables in all PTC subtypes. One explanation for this result, as exhibited in TCGA Thyroid Project data, is that the BRAFV600E mutation prevalence varies across PTC subtypes (12). Thus, the incorporation of the BRAFV600E mutation with subtypes of PTCs with low rates of the BRAFV600E mutation (e.g., FVPTC), along with a favorable phenotype, may confound the results to identify a positive association between BRAFV600E and aggressive behavior, rather than simply being a result of subtypes having different mutation rates. TCGA has reported that the BRAFV600E mutation status is strongly enriched in CVPTCs, which are more aggressive than their FVPTC counterparts are. Indeed, when a subgroup analysis was performed only in the CVPTCs of our cohort, the BRAFV600E mutation was no longer an independent predictor of CLNM. This finding is similar to a retrospective study previously performed with the same institutions (23). These findings are attributed to the fact that the entire cohort consisted of CVPTC as well as FVPTC and TCVPTC, the latter two having a lower and higher BRAF mutation rate with correspondingly lower and higher rates of LNM. Thus, it is believed that the FVPTC and TCVPTC may have contributed to finding a correlation in the entire series, but not in the CVPTC-only group.
In the present study, while BRAFV600E mutation status was identified as being statistically significantly associated with CLNM in the analysis of all histological subtypes that underwent prophylactic CLND, the ability to predict the presence of LNM with BRAFV600E analysis (48% for BRAFV600E positive vs. 28% for BRAFV600E negative) would likely not have any useful clinical applicability. In other words, its positive and negative predictive value (48% and 72%, respectively) limit its clinical utility as a stand-alone marker.
The TCGA molecular characterization of PTCs has revealed distinct molecular signatures between the different PTC subtypes. Furthermore, many of these molecular differences are associated with the percent follicular component in the tumor. Therefore, studying molecular markers while treating PTC as a homogenous disease may lead to inaccurate conclusions being drawn based on molecular markers and tumor phenotypes. To that end, a subgroup analysis was performed to consider the significance of molecular markers in the CVPTC subtype alone, excluding FVPTCs and TCVPTCs, but including a measure of the follicular and tall-cell component percentages present in the CVPTCs, a variable heretofore not incorporated in similar analyses. CVPTCs represented the largest cohort (192 cases) in the study, and a subgroup analysis, controlling for all clinicopathologic variables in the prophylactic group, identified miR-146b-5p and miR-222 to be predictive of CLNM; an analysis limited to preoperative clinicopathologic variables only found miR-146b-5p, miR-221, and miR-222 to be associated with CLNM. As discussed, BRAFV600E was not significantly associated with CLNM in CVPTCs, nor was the extent of the follicular and tall-cell components of the CVPTCs.
This prospective study examining a consecutive cohort of patients was adequately powered to examine relationships between potentially useful molecular markers and the prevalence of pathologically confirmed CLNM among patients with no clinical indication of CLNM. Our multi-institutional study is also the largest prospective study of patients with prophylactic CLND that examines the association of BRAFV600E and miRs with aggressive clinicopathologic variables of PTC. Most existing studies are retrospective and include non-consecutive, heterogeneous CLND cohorts and therapeutic CLND cases (50). Only one previous prospective study included patients who underwent prophylactic CLND, but was comprised of only 148 patients and from a single institution (18). While this prospective study overcomes major patient selection biases arising from retrospective non-consecutive and heterogeneous CLND cohorts that include therapeutic CLND cases, there are some limitations that require consideration. First, the study contains PTCs of various subtypes, namely CVPTC, FVPTC, and TCVPTC, which have different degrees of aggressiveness. The low number of patients with FVPTC and TCVPTC did not permit an adequately powered subgroup analysis within each disease subtype. Second, bias may be introduced by including patients with a clear diagnosis of PTC and excluding patients with indeterminate and suspicious Bethesda cytology categories, as the latter would have included a larger number of FVPTCs. However, in general, surgeons would not consider prophylactic CLND unless the diagnosis of PTC was clear preoperatively. Third, the pathologic spectrum of LNM based on size was not available. Therefore, a risk-stratification analysis based on these factors could not be performed. Lastly, variations in the exact surgical techniques and surgical practice patterns may have introduced undetected biases.
The TCGA experience characterized molecular phenotypes of PTC and highlighted the importance of considering molecular differences in treatment of the disease. It has provided a great resource to researchers. However, unfortunately, aggressive PTC cases are under-represented, and follow-up information is incomplete at best. Therefore, there is a need for a comprehensive characterization of the relationships between miRs and CLNM in studies that are adequately powered to permit examination across benign and aggressive PTCs with complete follow-up information, while avoiding the selection bias introduced by selective CLND.
While the current findings suggest the potential for developing miR-related predictive tools that may have clinical utility, this study was performed on FFPE tumor samples, and any future applicability would need to be applied to FNA samples. It is well known, however, that mutational analysis of the BRAF gene is reliable in FNA samples and correlates with corresponding tumors (48,49). Importantly, this exploratory study relied upon patient-specific relative values of miR expression rather than absolute values. In order to maximize the clinical usefulness of miR expression as a decision tool for determining the need for CLND, developing and validating techniques for measuring absolute levels of target miRs may be required. Along with others, this study has shown the ability to identify molecular alterations in PTCs, both at the DNA level and in terms of gene expression, from these sample types (23), and further consideration should be made to investigate their clinical utility.
Conclusions
In patients undergoing prophylactic CLNDs, miR-146b-3p, miR-146b-5p, and miR-222 were identified as potential markers of CLNM. BRAFV600E mutation was significantly associated with CLNM among patients with all PTC subtypes examined as a single group. When present, the BRAFV600E mutation was associated with a 48% chance of node positivity, while BRAFV600E negative patients had a 28% chance of node positivity. This proportional difference in the BRAF-associated likelihood of CLNM may not be useful clinically when deciding whether a patient should undergo prophylactic CLND. Furthermore, this statistical significance is likely due to the BRAFV600E mutation prevalence in the different PTC subtypes (FVPTC and TCVPTC). The results also demonstrate, however, that statistical significance does not necessarily equal clinical usefulness (48% vs. 28% LNM). The usefulness of BRAFV600E and other markers will depend strongly on the context and pretest probability of a positive test result. In cases with a high likelihood of BRAFV600E positivity, such as patients diagnosed with PTC on FNA, BRAFV600E testing is unlikely to be helpful. In more ambiguous cases, for example patients with indeterminate and suspicious Bethesda categories, the presence of a BRAFV600E mutation may increase the likelihood of being associated with LNM, but this has to be balanced with the lower overall risk of associated LNM in these categories. Before consideration can be given to creating a clinically useful prognostic prediction model for CLNM for patients with PTC, substantial additional work will be required to understand the observed relationships, paying particular attention to parameters that impact pretest probabilities, such as therapeutic versus prophylactic CLND intent, or the histological subtype composition of a given study cohort.
Footnotes
Acknowledgments
We would like to acknowledge Derek Anderson, Katie Beierl, Elizabeth Neylan, and Rouzbeh Mashayekhi for outstanding technical assistance.
Author Disclosure Statement
The authors have nothing to disclose.