
Abstract
Background:
Arginine (ARG) derivatives and thyroid function independently influence atherosclerotic processes. Since thyroid hormones may mediate the association between ARG derivatives and atherosclerosis, this study investigated whether asymmetric and symmetric dimethylarginines (ADMA and SDMA, respectively) as well as homoarginine (hARG) are associated with parameters of thyroid function in the general population.
Methods:
Cross-sectional data from 3689 individuals aged 20–81 years from the population-based Study of Health in Pomerania (SHIP-0) were analyzed. Thyroid function was defined according to serum concentrations of thyrotropin (TSH), free triiodothyronine (fT3), and free thyroxine (fT4). Low and high serum TSH were defined by the cutoffs 0.3 mIU/L and 3 mIU/L, respectively. Serum concentrations of ARG, ADMA, SDMA, and hARG were measured using liquid chromatography-tandem mass spectrometry. ARG, ADMA, SDMA, and hARG were associated with serum concentrations of TSH, fT3, and fT4 by median regression and with categorized TSH values by multinomial logistic regression adjusted for age, sex, smoking status, physical activity, body mass index, and estimated glomerular filtration rate.
Results:
Levels of ADMA (relative risk [RR] = 5.40 [confidence interval (CI) 1.96–14.86]) and SDMA (RR = 3.55 [CI 1.01–12.70]) were associated with low TSH. In addition, ADMA (β = 0.38 [CI 0.23–0.45]) was positively associated with fT3, while both ADMA (β = 0.98 [CI 0.43–1.54]) and SDMA (β = 1.19 [CI 0.50–1.88]) were positively associated with fT4. No consistent associations of ARG and hARG with thyroid function were detected.
Conclusions:
The positive associations of ADMA and SDMA with low TSH, fT3, and fT4 argue for a relationship of arginine derivatives with increased thyroid function. This suggests that the atherogenic properties of ADMA and SDMA may be partially mediated by thyroid function.
Introduction
L-
Thyroid function is also tightly related to atherosclerosis and CVD. Population-based studies have reported significant associations between serum thyrotropin (TSH), free triiodothyronine (fT3), or free thyroxine (fT4) concentrations and vascular disease. For example, in population-based studies, low TSH was associated with increased carotid wall thickness (13) and the presence of atherosclerotic plaque (14), increased coronary artery disease (15), as well as left-ventricular hypertrophy (16). Interestingly, fT4 is positively associated with arterial stiffness (17), but inversely related to carotid intima-media thickness (cIMT) (18). In summary, population-based epidemiological studies demonstrated a significant relationship between thyroid function and cardiovascular disease.
The synthesis of thyroid hormones is regulated by the release of TSH from the pituitary gland. In response to TSH, fT3 and fT4 are released from the thyroid gland. While the physiological effects of fT4 are minor, this hormone also functions as the precursor (or prohormone) for the metabolically active fT3. Among many other tissues, the conversion of fT4 to fT3 also takes place in the liver and the kidneys (19). Since ADMA und SDMA are associated with both hepatic (20 –22) and renal function (23,24), ARG derivatives may influence the hepatic and renal synthesis of fT3 and thereby mediate the atherogenic properties of thyroid hormones. This hypothesis is supported by previous research, which reported significant associations between ARG derivatives and thyroid hormones in patient populations with an increased risk for CVD. Specifically, ADMA was positively related with fT3 in patients with Graves' disease (25). However, so far, no data are available on the potential association between levels of circulating ARG derivatives and thyroid function in the general population. Therefore, this study investigated associations between ARG, ADMA, SDMA, and hARG with serum levels of TSH, fT3, and fT4 in a large population-based cohort from northeast Germany.
Material and Methods
Study population
The Study of Health in Pomerania (SHIP-0) is a cross-sectional population-based study conducted between 1997 and 2001 in West Pomerania, a region in the northeast of Germany including the three cities Greifswald, Stralsund, and Anklam and 29 surrounding communities (26). The total population comprised 212,157 inhabitants. A sample from the population aged 20–81 years was drawn from population registries. A total of 7008 subjects were sampled with 292 persons of each sex in each of the 12 five-year age strata. The net sample (without migrated or deceased persons) comprised 6267 eligible subjects. Selected persons received a maximum of three written invitations. In cases of non-response, letters were followed by phone calls or by home visits if contact by phone was not possible. The SHIP population finally comprised 4308 participants (corresponding to a final response of 68.8%). All participants gave written informed consent. The study followed the recommendations of the Declaration of Helsinki, and was approved by the Ethics Committee of the University of Greifswald. A total of 619 individuals were excluded because of missing data in any of the considered variables, resulting in a study population of 3689 individuals.
Methods
Non-fasting blood samples were taken between 07:00am and 04:00pm. Serum TSH, fT3, and fT4 concentrations were analyzed in the central laboratory of the University Medicine Greifswald by a homogeneous, sequential, chemiluminescent immunoassay based on LOCI® technology (Dimension Vista® System Flex® reagent cartridge; Siemens Healthcare Diagnostics, Inc., Newark, DE). The analytical measuring range was 0.005–100 mIU/mL, 0.1–8.0 ng/dL, 0.50–30.00 pg/mL for TSH, fT4, and fT3, respectively. Low and high serum TSH concentrations were defined using the cutoffs 0.3 and 3.0 mIU/L, respectively (27). These cutoff values are clinically relevant TSH concentrations associated with hyper- and hypothyroidism. Serum creatinine concentrations were determined with the Jaffé method (Hitachi 717; Roche Diagnostics, Mannheim, Germany). The estimated glomerular filtration rate (eGFR) was calculated using the four-variable Modification of Diet in Renal Disease (MDRD) study equation: eGFR = 186.3 × serum creatinine–1.154 × age–0.203 × (0.742 if female) (28,29).
ARG, ADMA, SDMA, and hARG serum concentrations were analyzed by liquid chromatography–tandem mass spectrometry using previously validated methods (30 –32). In brief, 25 μL of serum was diluted with stable isotope labeled internal standards. Subsequently, proteins were precipitated with methanol and guanidine compounds and converted to their butyl esters. Intra- and interassay coefficients of variation were ≤7.5% for all metabolites. The ARG assay had an upper detection limit of 250 μmol/L, and 565 samples had values above this threshold. Thus, regarding ARG, the subject population was categorized into four groups: low (<132.4 μmol/L), medium-low (132.4–174.2 μmol/L), medium-high (174.2–250 μmol/L), and high (>250 μmol/L) serum concentration. Groups of low, medium-low, and medium-high ARG concentrations were defined by tertiles of the ARG distribution to a concentration of 250 μmol/L. Individuals with values above this threshold were placed in a separate group (high).
Smoking status and physical activity were assessed by computer-assisted personal interviews. Smokers were categorized into three categories (lifetime non-smokers, former smokers, and current smokers). Subjects who participated in physical training during summer or winter for at least one hour per week were classified as being physically active. Height and weight were measured in order to calculate each subject's body mass index (BMI = weight [kg]/height2 [m2]).
Statistical analyses
Population characteristics are expressed as median, 25th percentile, and 75th percentile (continuous data) or as absolute numbers and percentages (categorical data) stratified by ARG concentrations. ARG, ADMA, SDMA, and hARG were associated with serum concentrations of TSH, fT3, and fT4 by median regression adjusted for age, sex, smoking status, physical activity, BMI, and eGFR. For the categorical TSH outcome (low TSH, TSH in the reference range, high TSH), multinomial logistic regression was applied using TSH in the population-specific reference range (27) as reference category and the latter confounder set. To account for possible non-linear relationships of ARG and its derivatives with TSH, fT3 and fT4 fractional polynomials were tested (33). A p-value of <0.05 was considered statistically significant. All analyses were carried out with Stata v13.1 (Stata Corp., College Station, TX).
Results
Description of the study population
In the study population, 300 individuals (8.1%) had a TSH concentration <0.3 mIU/L, and 82 individuals (2.2%) >0.1 mIU/L. Subjects with lower ARG concentrations were significantly more often males compared with subjects with higher ARG concentrations (Table 1). Further, individuals with higher ARG concentrations were more often smokers and had a larger BMI than individuals with lower ARG concentrations did. Low TSH was less common in individuals with high ARG concentrations. Median fT3, fT4, ADMA, and SDMA concentrations were not significantly different between the ARG groups. hARG concentration increased with increasing ARG concentrations.
Data are expressed as median (25th and 75th percentile) for continuous data and as absolute numbers (percentages) for categorical data.
TSH, thyrotropin; fT3, free triiodothyronine; fT4, free thyroxine; ADMA, asymmetric and dimethylarginines; SDMA, symmetric dimethylarginines; hARG, homoarginine; eGRF, estimated glomerular filtration rate.
Multivariable analyses
ARG, ADMA, SDMA, and hARG were not significantly associated with TSH as a continuous variable (Table 2 and Fig. 1). Likewise, there was no consistently significant association between ARG concentrations and low or high TSH. ADMA and SDMA were also positively associated with a low TSH. Participants with high ARG concentrations had significantly lower fT3 levels than subjects with low ARG concentrations did. Further, ADMA was positively associated with serum fT3 concentrations (Table 2 and Fig. 2). No statistically significant associations for SDMA and hARG with fT3 were found. ADMA and SDMA were positively associated with serum fT4 concentrations (Fig. 2), whereas ARG and hARG were not associated with this outcome. Only SDMA was significantly inversely associated with the fT3-to-fT4 ratio.
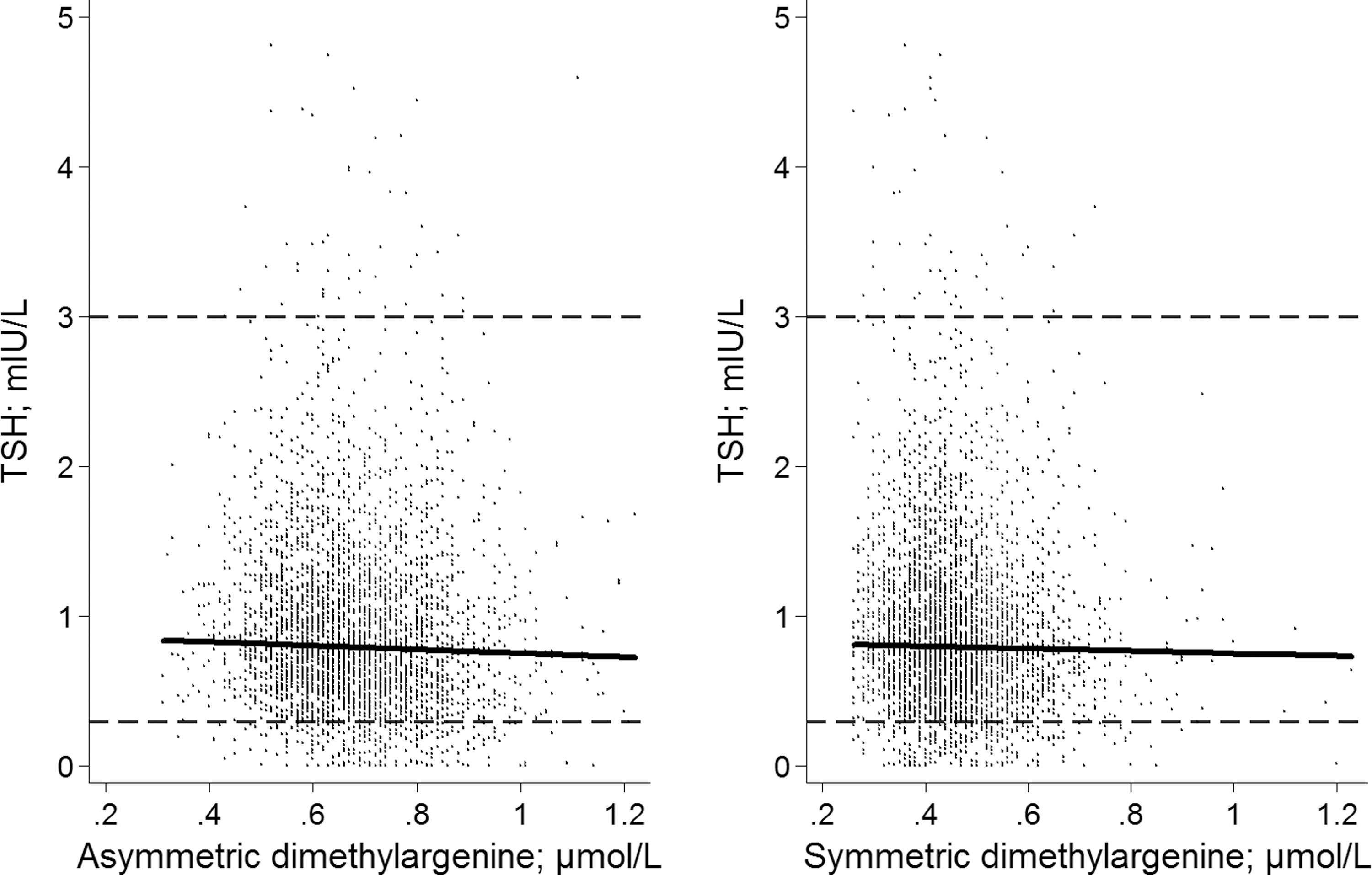
Scatter plots for asymmetric and symmetric dimethylarginines (ADMA/SDMA) and thyrotropin (TSH), including regression lines derived from median regression. Dashed lines represent the lower and upper limit of the TSH reference range.
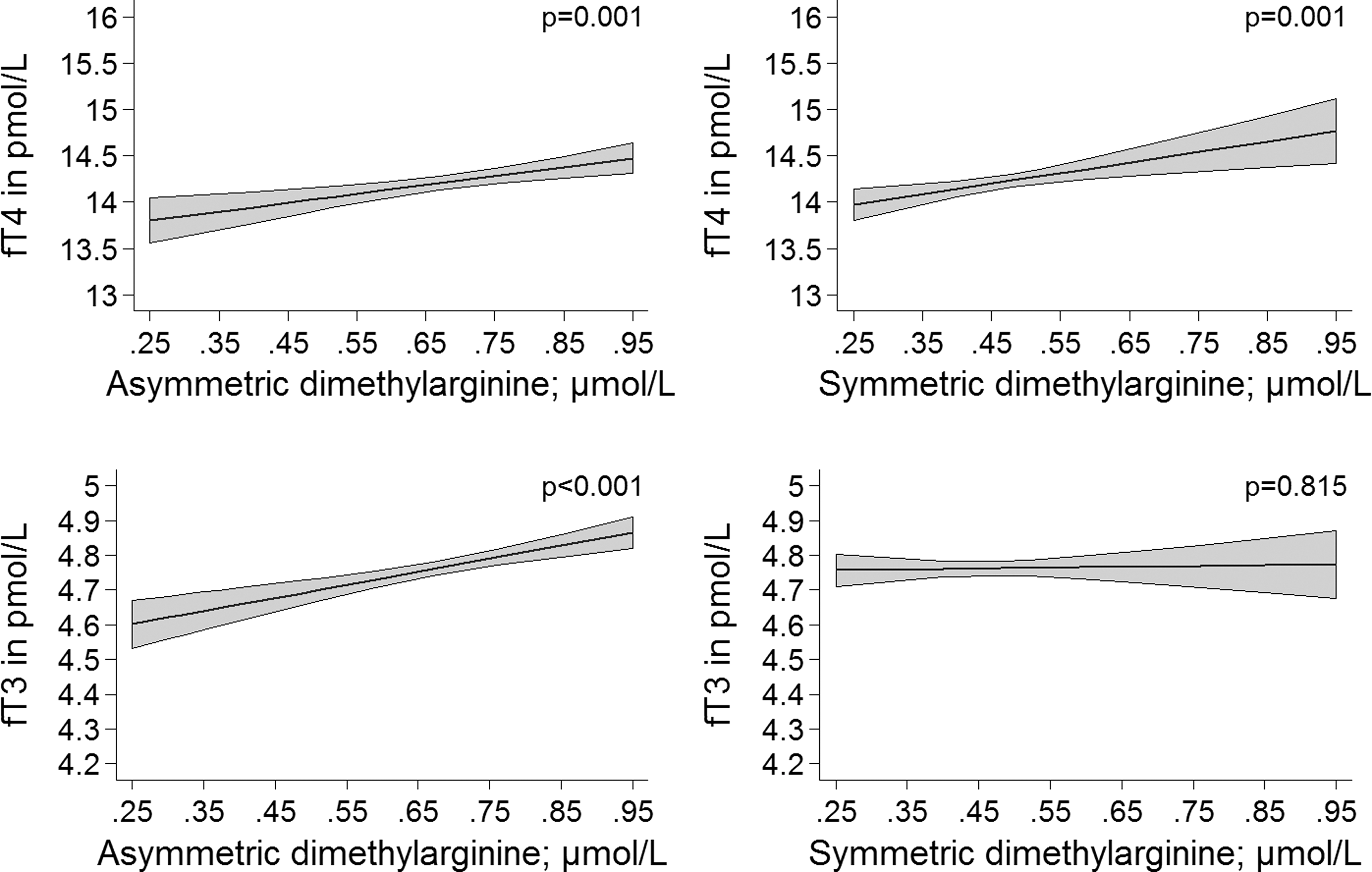
Association of ADMA and SDMA with free triiodothyronine and free thyroxine derived from median regression (including confidence intervals).
The outcomes TSH, fT3, and fT4 were analyzed by median regression; the outcomes high and low TSH were analyzed in comparison to TSH concentrations within the reference range in one model by multinomial logistic regression.
In comparison to L-arginine <132.4 μmol/L.
p < 0.05.
RRR, relative risk ratio; CI, confidence interval.
Discussion
This study explored associations between ARG derivatives and thyroid hormones in the general population. Positive associations were demonstrated for ADMA and SDMA with low TSH as well as for ADMA with serum concentrations of fT3 and fT4. For SDMA, such an association was only seen with serum fT4 concentrations. In summary, positive associations of ARG derivatives with fT3, fT4, and low TSH indicate a relationship of ARG derivatives with increased thyroid function. Thus, the atherogenic properties of ADMA and SDMA may be partially mediated by thyroid function. Even though subclinical hyperthyroidism has been associated with an increased risk for cardiovascular mortality (15,34), the direction of the association with arginine derivatives is not clear. One may speculate that either ADMA influences hepatic fT3 synthesis or that thyroid hormones alter hepatic and renal arginine metabolism. However, even in animal experiments, the directionality of this association could not be determined (35). The proposed influence of hepatic function is further supported by previous data. For example, serum fT4 concentrations were inversely associated with hepatic steatosis in population-based data (36) and with total cholesterol (TC) in euthyroid men (37). Furthermore, serum TSH concentrations are positively associated with TC, LDL cholesterol, and triglycerides in a general population of adults (38) and children and adolescents (39). Nonetheless, future research is needed to clarify how the interaction between thyroid hormones and arginine derivatives takes place and influences athero-susceptibility.
In healthy subjects, TSH release from the pituitary gland is controlled by circulating levels of fT3 and fT4. Specifically, high levels of these thyroid hormones reduce pituitary TSH synthesis, while low fT3 and fT4 concentration increase TSH release. In the present study, ADMA and SDMA were positively associated with low TSH. Furthermore, the current data also showed a significantly positive association of ADMA with fT3 and fT4 as well as SDMA with fT4. In agreement with the present findings, ADMA was also positively associated with fT3 and fT4 in patients with Graves' disease (25). Interestingly, the current data also showed a significant association for SDMA concentration with a reduced fT3-to-fT4 ratio. This means that an increase in SDMA may result in a decrease of fT3 in comparison to fT4. As outlined above, in healthy subjects, low TSH concentrations are only present when the thyroid gland produces too much fT3 and fT4. Therefore, the positive associations of ADMA and SDMA with fT3, fT4, and low TSH suggest a relationship between ARG derivatives and increased thyroid function.
The current findings are also supported by animal studies in mice. Specifically, dimethylarginine dimethylaminohydrolase-1 (DDAH-1) is the crucial enzyme for the degradation of ADMA (40). The DDAH-1 gene carries a farnesoid X receptor (FXR)-responsive element. Therefore, FXR agonists induce an upregulation of DDAH-1 (41). Interestingly, in mice lacking the nuclear fT3 receptor, liver FXR is activated and DDAH-1 transcription is enhanced (42). Likewise, similar to this observation, a reduced fT3 concentration in humans might result in higher DDAH-1 expression and thereby foster ADMA degradation. How ADMA and SDMA are regulated in detail is currently not clear. Both arginine derivatives are a result of post-translational modifications by specific protein arginine methyltransferases (PRMT-1 and PRMT-2, respectively) (43). However, the regulation of these PRMTs is yet to be fully understood (44). Since only ADMA, and not SDMA, is hydrolyzed by DDAH-1, one can assess that SDMA is regulated by PRMT activity and renal balance, while the ADMA/SDMA ratio serves as a marker for DDAH metabolism (24). Hepatocytes remove ADMA from the hepatic circulation and thereby regulate circulating levels of ADMA (45). In the kidneys, SDMA and ADMA are excreted equally, but ADMA can also be synthesized. Overall, renal and hepatic function most likely regulate arginine derivative concentration.
An early marker of atherosclerosis is decreased NO bioavailability. A reduction in NO may be due to higher circulating levels of ADMA and SDMA, which competitively bind to endothelial NO synthase. Increased arterial stiffness is also an early marker for atherosclerosis and can be caused by low NO. Since low fT4 is related to arterial stiffness (17) and an association was shown between ARG derivatives and fT4, the effect of ADMA and SDMA on arterial stiffness may be mediated by thyroid dysfunction. The present findings and those from Delitala et al. are in contrast to a study with Japanese women in which fT4 was inversely related to cIMT (18). However, arterial stiffness is a functional measure of elasticity of the large peripheral conduit arteries, while cIMT assesses intima-media thickening in the common carotid artery as a morphological criterion. Thus, arterial stiffness and cIMT represent two different disease markers of atherosclerosis. Furthermore, the heterogeneous results may also be related to region-specific iodine supply leading to a high prevalence of hypothyroidism in Japan and hyperthyroidism in Europe (46).
The presence of ARG is essential for the synthesis of the atheroprotective gas NO (1). No consistent association was found between ARG concentrations and serum TSH levels. Further, a positive association is reported between ARG and fT3 for subjects with high ARG concentrations, but no significant relationship between ARG and fT4 was found. Thus, in the present study, the association between ARG and thyroid hormones were inconsistent. Hence, the results suggest that either there is a non-linear relationship between ARG and thyroid function or that the findings are a significant by chance. It remains to be elucidated if the effects of ARG on the cardiovascular system are mediated by thyroid function.
hARG has been postulated to have anti-atherosclerotic effects by being a weak substrate for NO synthase (12). The current findings show no association between hARG and thyroid function in a general population setting. Thus, no indication was found that the atheroprotective properties of hARG might be mediated by thyroid function.
The major strength of this study is the population-based design, which allows inferences for the general population to be drawn from the results. In addition, highly standardized quality control was employed during the course of the study. It is acknowledged that based on the cross-sectional analysis, the direction of the investigated association cannot be conclusively determined. Furthermore, the upper detection limit of the ARG assay (250 μmol/L) does not allow ARG to be modeled continuously.
In summary, this study assessed the association between ARG derivatives and thyroid function in the general population. In particular, the results demonstrate an association between ADMA and SDMA with increased thyroid function. This may indicate that the atherogenic properties of these ARG derivatives may be partially mediated by thyroid function. Further studies are warranted to confirm these findings.
Footnotes
Acknowledgments
The Study of Health in Pomerania is part of the Community Medicine Research Network of the University Medicine Greifswald, which was funded by the German Federal Ministry for Education and Research, the Ministry for Education, Research, and Cultural Affairs, and the Ministry for Social Affairs of the State Mecklenburg-West Pomerania. Analyses were further supported by the German Research Foundation (DFG VO955/12-1) and the BMELV.
D.A. acknowledges the support of the European Union under a Marie Curie Intra-European Fellowship for Career Development. The excellent technical assistance of Mariola Kastner and Anna Steenpass is gratefully acknowledged.
Author Disclosure Statement
No competing financial interests exist.