
Abstract
Background:
Given the increasing incidence of papillary thyroid carcinoma despite stable disease-specific mortality rates, the potential for the disease to reoccur is a key outcome to predict. The BRAFV600E mutation has been associated with recurrent disease in larger tumors. However, its correlation in papillary thyroid microcarcinoma (PTMC) is not clear in individual series.
Methods:
The MEDLINE, EMBASE, Web of Science, and Cochrane databases were searched for studies including patients with PTMC undergoing initial surgical treatment. Studies with at least two years of follow-up, BRAF genotyping (the comparator), and recurrence as an outcome were included, as were unpublished primary data on 485 patients from two institutions. The metameter analyzed was odds ratio (OR) for recurrence between patients with BRAFV600E versus BRAF wild type (BRAFwt).
Results:
The initial search identified 431 references. After screening of the abstracts for inclusion, 44 manuscripts were reviewed in full by two independent reviewers. Four published studies and primary data from two institutional cohorts were included in the final analysis. A meta-analysis of 2247 PTMC patients revealed that patients with a BRAFV600E mutation had a higher likelihood for recurrence (odds ratio 2.09 [confidence interval 1.31–3.33], p = 0.002).
Conclusions:
This meta-analysis shows that BRAF mutational status correlates with recurrence of PTMCs, highlighting the potential utility of genotyping in preoperative and postoperative planning. BRAF mutation may be helpful in risk-stratifying patients with PTMC for surgical management versus observation.
Introduction
T
The new 2015 guidelines from the American Thyroid Association (ATA) for PTC <1 cm without extrathyroidal extension recommends thyroid lobectomy alone, unless there are high-risk clinical features (13). Therapeutic lymph node dissection is reserved for clinically or radiographically positive lymph node metastases (13). Given the largely indolent nature of the disease with a large review of the Surveillance, Epidemiology, and End Results (SEER) cancer database of 18,445 PTMC patients reporting just a 0.5% disease-specific 10-year mortality (14), selective observation has also been suggested (11,12). While the majority of patients with PTMC will do well, select patients will have poorer outcomes with the development of recurrent or metastatic disease that requires reoperation or radioactive iodine (RAI) ablation (15 –17). Given that so few patients die from PTMC, tools to help predict which patients have an increased risk of recurrence are valuable.
Activation of the BRAF kinase is associated with carcinogenesis in multiple human tumors including thyroid cancer (18). The most common alteration seen in PTC is a point mutation at codon 600 (BRAFV600E ), and it is found in up to 40–70% of all PTC cases (19 –23). Although initial studies reported contrasting findings, more recent series have demonstrated that the BRAFV600E mutation in PTC has been associated with more aggressive behavior, including increased incidence of extrathyroidal tumor extension, lymph node metastases, and recurrence (24 –26). However, these studies are enriched with larger tumors with other high-risk pathological features where extent of surgery and consideration of observation are less of a debate. If BRAF status holds true as a predictive factor in PTMC, sequencing performed at the time of fine-needle aspiration (FNA) could provide further information for risk stratification.
It has been shown that the presence of the BRAFV600E mutation in all PTC is independently associated with an increased risk of recurrence (19,27 –30). However, the correlation of BRAFV600E and recurrence in PTMC is not clear in individual series. Given the relatively low risk of recurrence, it was hypothesized that individual studies assessing the correlation of BRAF status with recurrence may be underpowered. A systematic review and meta-analysis was therefore performed, and primary data from two additional institutions were pooled in order to assess if BRAF status can guide treatment in patients with PTMC.
Materials and Methods
Research question and study design
The primary objective was to determine if BRAF mutational status predicts tumor recurrence in patients with PTMC. In designing and performing the study, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist was completed. The analytic framework is outlined in Figure 1.
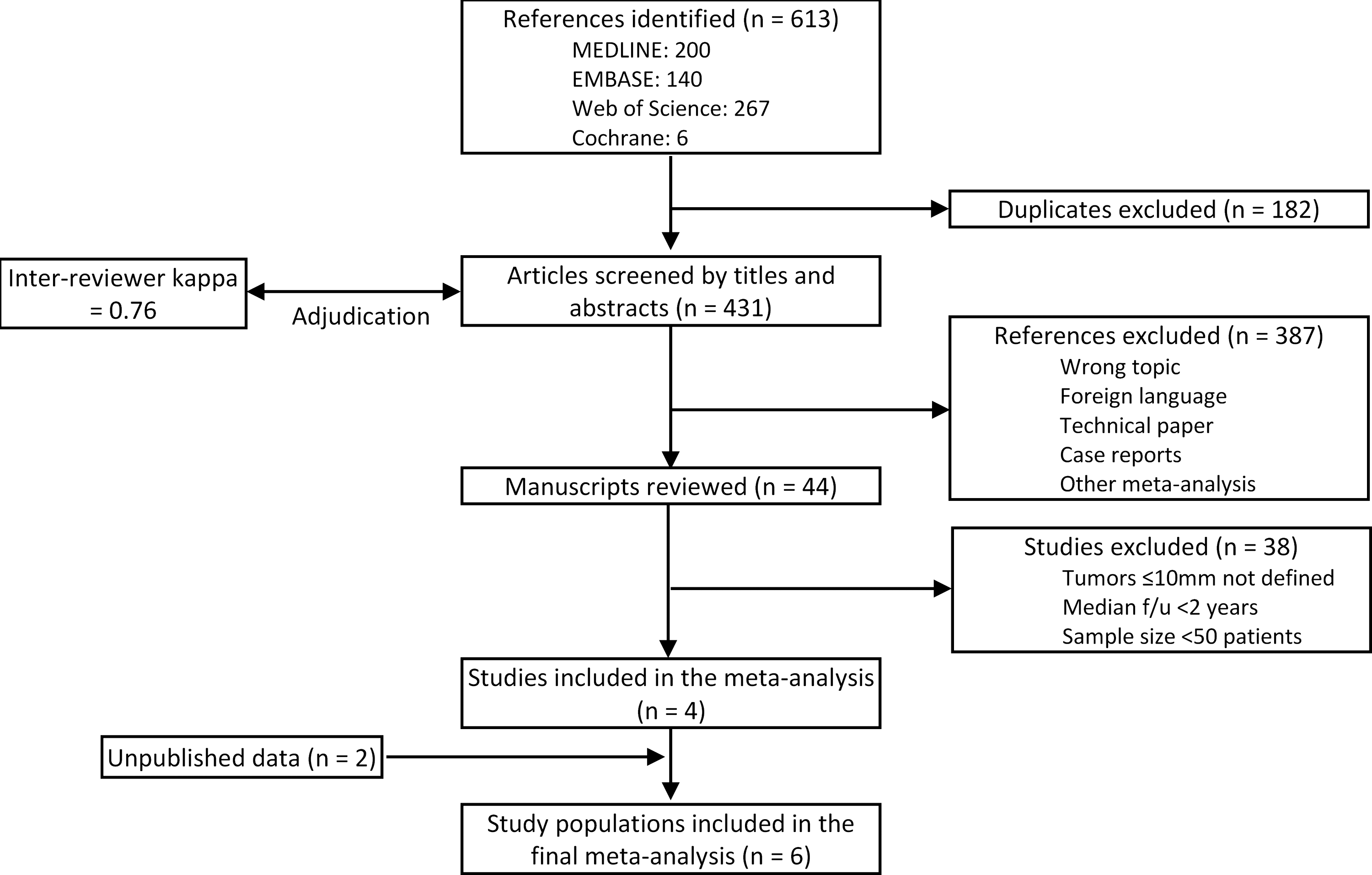
Flow diagram of systematic review.
Information sources for systematic review
An online search of the MEDLINE, EMBASE, Web of Science, and Cochrane databases was performed for studies published prior to March 2014 that assessed the correlation between BRAFV600E and recurrence in patients with PTMC. The following search terms and their synonymous terminology were used for searching the databases: thyroid neoplasm, BRAF, papillary, and recurrence. Cross-referencing of review articles and included studies was also performed, and only English language studies were included. Unpublished primary data were also included on 465 patients from two institutions: Massachusetts General Hospital, United States (MGH) and Seoul National University Hospital, Korea (SNUH).
Eligibility and trial inclusion criteria
Studies were assessed that included patients who underwent total thyroidectomy and reported data including PTMC ≤10 mm, BRAF genotyping (the comparator), and recurrence as an outcome (the metameter). Only studies that documented a period of clinical remission were included. Exclusion criteria included median follow-up of less than two years, failure of the study to report recurrence by tumor size <10 mm, and sample size <50 patients. When several studies reported on the same patient population, only the most recent study was included. Two investigators independently screened the manuscripts, and disparities were adjudicated by a third investigator. Primary data from MGH and SNUH were obtained under approval by respective Institutional Review Boards.
Data extraction
Reviewers independently extracted the data from the included studies into a custom spreadsheet, including sample size, patient demographics, clinicopathological features, BRAFV600E mutation status, and recurrence rates. If the odds ratio (OR) for recurrence was not reported, studies were only included if the OR could be calculated based on the data provided. Each study was also rated for overall methodological quality using the Newcastle–Ottawa Scale (NOS) (31).
Analyses
Data from all included studies were pooled, and unpublished data from the other two institutions were also included. The metameter analyzed was OR for recurrence between PTMC patients with BRAFV600E versus BRAFwt. Statistical analysis was conducted using Comprehensive Meta-Analysis v2.2.064 (Biostat, Englewood, NJ) with p-values of <0.05 considered statistically significant. The effect of the comparator on the risk of recurrence was presented as OR with confidence intervals (CI).
A random-effects model was used to synthesize the outcomes, given the independent nature of each study and the unlikeliness that they would be functionally equivalent. This accounts for study heterogeneity and allows the results of this meta-analysis to be extrapolated beyond the fixed patient populations of the included studies to the general population. Heterogeneity was assessed using the Q statistic and I2. Publication bias was assessed visually by funnel plot and Egger's test.
Sources of bias within studies and heterogeneity among studies
A priori potential sources of heterogeneity were considered: study design, inclusion criteria for the various studies, use of RAI, use of prophylactic central lymph node dissection, extent of surgery, and varying outcome measures. A lack of standardization was assumed for extent of surgery and use of RAI radiation (i.e., confounding by indication).
Results
Study selection
The initial literature search yielded a total of 613 citations relevant to the study question. After 182 duplicates were removed, 431 citations were screened by independent reviewers (C.C.L. and T.S.W.), and 387 abstracts were excluded for reasons including wrong topic, median follow-up of less than two years, sample size <50 patients, inclusion of pediatric patient population, and foreign language publication. Registry publications and meta-analyses were excluded in order to avoid double counting patients, although all citations included in the latter were individually cross-referenced. Two references were later excluded, as their patient population was included in a more recent multi-institutional study. Inter-reviewer kappa was 0.76, indicating good agreement between the two reviewers. Disagreements were adjudicated by a third reviewer (Y.C.). The remaining 44 manuscripts were read to assess for adequate reporting of the study group (tumor size ≤10 mm), outcome (recurrence rates), and availability of data to calculate the metameter of interest (OR for recurrence). Following this systematic review, four studies met the inclusion criteria for the meta-analysis. Additional unpublished data from two institutions were also included in the final analysis (Fig. 1).
Study characteristics
Of the six cohorts included in the analysis, four—Zheng et al. (20), Xing et al. (23), Walczyk et al. (21), and MGH—were historical cohorts, meaning that BRAF testing was performed retrospectively on the specimens and therefore did not bias treatment. Moon et al. (22) performed BRAF testing on FNA biopsies during staging ultrasound, although the authors did not state how BRAF results impacted immediate management. The remaining studies were prospectively collected data in unselected groups ((22) and SNUH). Three cohorts as well as the unpublished data were from individual institution studies located in Korea (n = 2), China (n = 1), the United States (n = 1), and Poland (n = 1). There was a single multi-institution study involving 16 medical centers in eight countries (23).
Study population characteristics are summarized in Table 1. The pooled sample size included 2247 patients. The average age of patients ranged from 44.8 to 49.9 years among the included studies, and all studies demonstrated a female predominance (77–88%) consistent with the literature. Four data sets included only patients who had undergone total thyroidectomy, with the remaining two having a rate of lobectomy alone of 14.2% and 49.2%. Moon et al. (22), Zheng et al. (20), and the primary cohort from SNUH routinely performed ipsilateral prophylactic central lymph node dissections, while the other cohorts only did lymph node dissections when suspicious lymphadenopathy was identified clinically or radiologically.
Data were unable to be extracted from this article.
NOS, Newcastle–Ottawa Scale (31).
Recurrence in the two included primary cohorts (MGH and SNUH) was defined as biopsy-proven structural evidence of disease after a period of radiographic and biochemical remission (stimulated Tg ≤2 ng/mL with negative Tg antibodies). Zheng et al. (20) and Moon et al. (22) defined recurrent disease as increased biochemical markers associated with radiographic disease with or without cytological evidence after a period of radiographic and biochemical remission. Walczyk et al. (21) did not report any recurrences but defined remission as absence of structural disease on imaging combined with undetectable or decreasing biochemical markers. Recurrence was defined per each institution in the study by Xing et al. (23), with references to the ATA and European Guidelines for “authoritative” definitions. In no study was recurrence defined by radiological (i.e., ultrasound) findings alone.
The BRAF mutation was detected utilizing formalin-fixed, paraffin-embedded histological samples in all studies except Moon et al. (22) who utilized FNA cytology. Direct sequencing was the most frequent method of detecting the BRAFV600E point mutation. NOS scores of the studies ranged from 5 to 9, representing moderate-to-good quality studies. NOS scale points were subtracted for deficiencies in controlling for surgical extent and adequacy of follow-up.
Outcome of interest (metameter)
The OR for recurrence in the BRAFV600E patients versus the BRAFwt patients was calculated using raw data provided in individual studies. A random-effects meta-analysis of the pooled OR was conducted with a combined OR of recurrence of 2.09 ([CI 1.31–3.33], p = 0.002; Fig. 2). A “one-study removed” analysis was also performed to verify that the observed effect was not unduly influenced by any one study (Fig. 3).
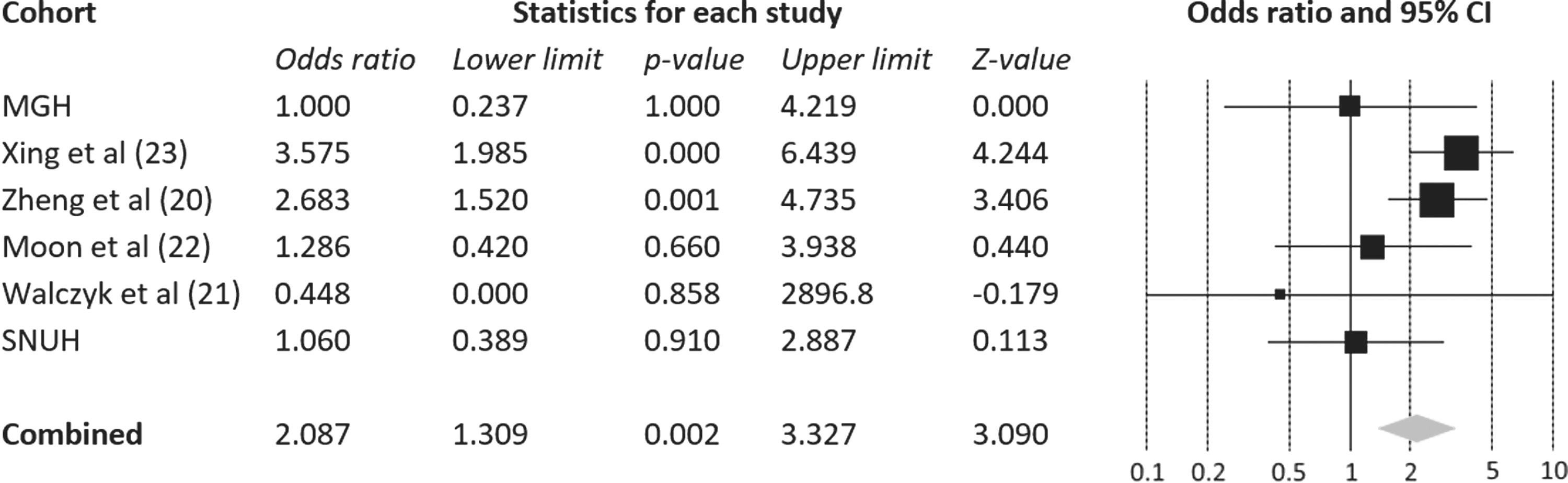
Random effect model of the odds ratio (OR) with confidence intervals of the risk of recurrence of BRAFV600E compared with BRAFwt in patients with papillary thyroid microcarcinoma (PTMC; tumor size <10 mm). The squares represent the OR of individual studies, and the diamond represents the summary OR.
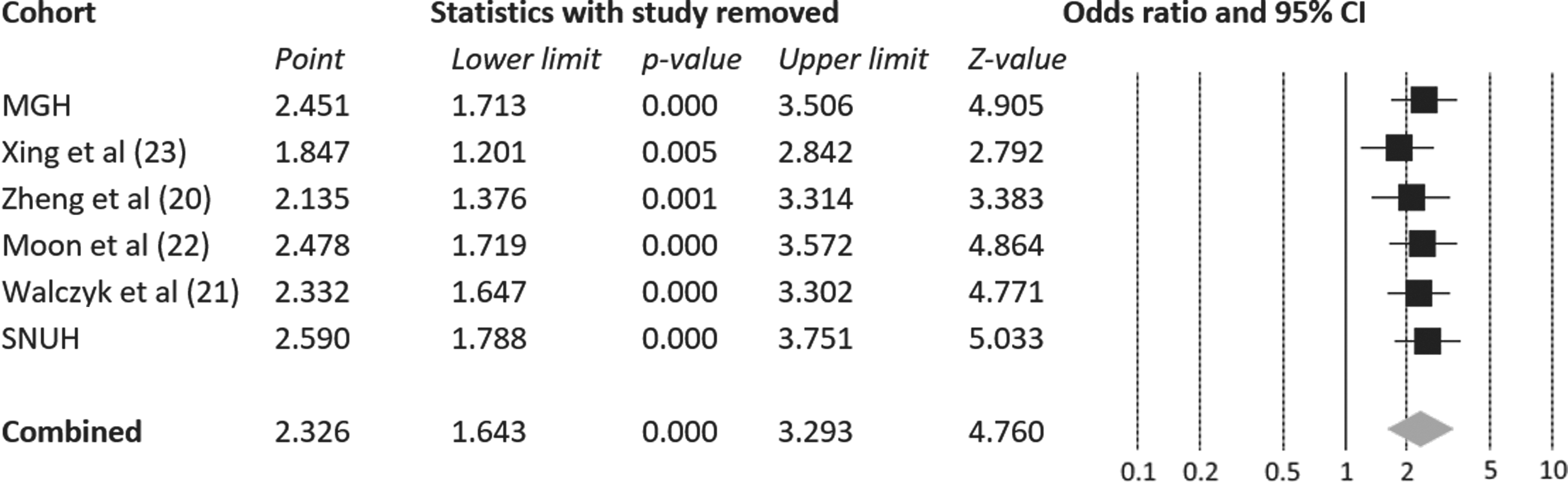
Risk of recurrence of BRAFV600E compared with BRAFwt in patients with PTMC (tumor size <10 mm)—“one study removed” analysis. The squares represent the OR of individual studies, and the diamond represents the summary OR.
Assessment of heterogeneity among studies
A fixed-effects analysis of OR was performed to assess the difference between the two models. A fixed-effects pooled OR did not differ significantly from the random-effects outcome (2.33 [CI 1.64–3.29]), with an I2 of 30 and Q statistic of 7. This is in comparison to the random effects model, wherein the I2 was 0 and Q statistic was 4.7.
Assessment for publication bias
A funnel plot analysis was performed to assess for publication bias (Fig. 4). While acknowledging that the number of studies meeting the inclusion criteria limits this assessment, it does not appear that there is significant publication bias. Egger's statistic is non-significant (p = 0.14).

Funnel plot analysis for assessment of publication bias.
Discussion
This study utilizes a systematic review, pooled primary data from two large institutional series, and meta-analytical techniques to investigate the association between BRAF mutation and recurrence in patients with PTMC. With the increasing incidence of PTMC, it is important to risk-stratify patients who may have more aggressive tumor biology in what is traditionally thought to be a more indolent disease. This will have management implications, including whether to observe, the extent of surgical resection, use of adjuvant RAI ablation, and frequency of follow-up. Especially in the United States, given the large proportion of thyroid cancer care cost attributable to initial treatment and continued surveillance, risk-stratification will also have significant financial impact (32). To the authors' knowledge, this is the first study to pool data from the published literature and primary data from two independent institutional cohorts to maximize the statistical power to detect differences in recurrence. The study has shown that patients with PTMC who carry the BRAFV600E mutation have an increased risk of tumor recurrence.
Worldwide guidelines for management of PTMC vary. The ATA and the European Thyroid Association both recommend total or near total thyroidectomy for PTMC, with a more limited resection only considered for low-risk tumors (13,33). Low risk is defined by these guidelines as patients without any evidence of nodal or distant metastases, extrathyroidal extension, history of radiation exposure, or multifocal disease (13,33). Japanese guidelines, which generally recommend for more limited thyroid resections combined with more aggressive prophylactic lymph node dissections compared with their Western counterparts (34), propose surgical treatment for PTMC with clinical lymph node metastasis, distant metastasis, or significant extrathyroidal extension. Patients without these features may be candidates for observation with significant counselling, although the authors acknowledge that current evidence is insufficient (35).
The increasing diagnosis of small thyroid cancers, unchanged clinical outcomes, and the mounting financial and quality-of-life implications of their diagnosis and treatment have led some to suggest that non-operative management and observation may be appropriate for certain tumors. Ito et al. reported on 1235 patients with low-risk PTMC and showed that with a mean observation period of 75 months, just 191 patients (16%) progressed to surgical management for reasons including tumor enlargement, concomitant thyroid disease, and patient choice (36). A prospective clinical trial of non-operative management for PTMC by Sugitani et al. also demonstrated favorable results with tumor enlargement in just 22/300 PTMC lesions, and only 7% of patients progressed to surgical resection (12). No patients in either study showed evidence of distant metastasis or tumor-specific mortality at the time of follow-up, although there was a single postoperative recurrence in the contralateral thyroid remnant reported by Ito et al. (11).
Despite these favorable reports, significant patient numbers with long-term follow-up is still lacking, and a small proportion of patients with this “indolent” disease still develop unfavorable outcomes. A SEER database analysis demonstrated that small T1 tumors <2 cm accounted for 12.3% of all thyroid cancer–related mortality, and PTMC specifically for almost half of those (37). Sugitani et al. reported on a subgroup of “symptomatic” PTMC patients who all had clinically apparent lymph node metastasis and underwent surgery. This high-risk group had a recurrence rate of 38% with disease-specific survival at 5, 10, and 20 years being 98%, 80%, and 53%, respectively, highlighting the potentially aggressive nature of the disease (12).
Several studies have demonstrated that in PTMC, factors that predict recurrence and mortality include male sex, regional or distant metastasis, multifocality, extrathyroidal extension, vascular invasion, or incomplete resection (37,38). Many of these factors are only assessable following surgery, which makes relying on these factors for determining which tumors are low risk difficult. Indeed, a significant proportion of patients diagnosed with PTMC are classified as “incidental,” where the lesion is only identified on postoperative histological examination of the thyroidectomy specimen (39). Preoperative FNA and subsequent molecular analysis may then be helpful in deciding who is able to be observed, and in those that do undergo surgical resection, molecular status may help define aggressiveness of adjuvant therapy and follow-up.
Whether the changes in management based on the mutational status in PTMC will have any impact on survival is unclear. However, given the low rates of PTMC-related disease-specific mortality and the extended follow-up period required, randomized controlled studies with sufficient power to compare the effect of different management on survival are unlikely to be performed (14,40). Tumor recurrence is thus a more useful and practical outcome measure and acts as a marker of tumor aggressiveness. Current ATA guidelines favor surgery for treatment of recurrent disease (13). Recurrent PTC, particularly if not locoregional, is associated with worse long-term survival and has significant clinical consequences with increased risk of postoperative complications (41). It could be argued that identifying and treating high-risk patients, such as those with the BRAFV600E mutation, more aggressively upfront could potentially improve outcomes. On the contrary, absence of high-risk features may identify patients who might be suitable for less extensive surgery or even observation. This is particularly relevant in the subset of patients with PTMC for whom the optimal treatment is under debate.
The true natural history of observed PTMC in which to compare outcomes by genotype can only be assessed in an unselected cohort of patients without treatment. While it would be unethical not to intervene in patients with progressive disease, this is a fertile area for modeling simulated populations. The best primary evidence is found in studies such as those published by Ito et al. (11) and Sugitani et al. (12) who have observed selected patients longitudinally, although BRAF mutational status has not been reported in these series. The authors are unaware of any prospective studies that base clinical strategies, including active surveillance, in PTMC by BRAF status, although this is an important next step.
This meta-analysis is inherently limited by the quality of the included studies. All data were non-randomized, and the majority of the studies were retrospective in nature. The extent of surgical resection and use of adjuvant RAI therapy was not standardized between institutions. However, the use of prophylactic central neck dissection or the use of RAI ablation in PTMC has not been shown to affect the rate of local recurrence (42,43). It is also acknowledged that the definition of recurrent disease was not uniform between studies. This is an area where there is still much variation in the literature and is highly institution dependent. Indeed, some authors argue that due to the indolent nature of PTC, much of the disease recurrence is actually undetectable persistent disease that subsequently becomes clinically detectable rather than a true recurrence (44). Further consensus is needed on this matter.
Risk-stratification is essential in maximizing quality of care for the increasing number of patients diagnosed with PTC, many cases of which are PTMC, and at low risk for disease recurrence. This meta-analysis shows that BRAF mutational status correlates with recurrence of PTMCs, highlighting the potential utility of genotyping in preoperative and postoperative planning and potentially to optimize healthcare utility and costs. Primary PTMC positive for the BRAFV600E mutation may represent a group of tumors that require more prompt surgical management and closer follow-up. Patients without these high-risk features may, after sufficient counseling, be suitable candidates for observation.
Footnotes
Author Disclosure Statement
There are no conflicts of interest to declare. There are no sources of funding to declare.