
Abstract
Background:
Lingual thyroid is a rare abnormality of thyroid development that is usually treated conservatively with levothyroxine replacement. Rarely, it becomes large enough to cause obstructive symptoms in the oral cavity, requiring definitive treatment.
Patient Findings:
This study reports on three patients with lingual thyroid treated with radioactive iodine-131 (131I) with successful radioablation of their ectopic thyroid tissues. Measurement of 24-hour radioactive iodine uptake within thyroidal tissues and hybrid single-photon emission computed tomography/computed tomography imaging using either iodine-123 or technetium-99m pertechnetate scans were performed in all patients demonstrating the location and size of lingual thyroid and absence of an orthotopic thyroid gland.
Summary:
The aim of this study was to describe nonsurgical management of obstructive lingual thyroid tissue with 131I therapy for lingual thyroid radioablation. Patients were prepared with a low-iodine diet and levothyroxine withdrawal prior to radioablation for optimizing 131I uptake in ectopic thyroid tissues. Hybrid single-photon emission computed tomography/computed tomography measurement of anatomic size of lingual thyroid tissue and radioactive iodine uptake guided the selection of therapeutic doses, resulting in administration of 10.7, 17.5, and 15.4 mCi of 131I, respectively. There were no post-therapy complications, and clinical follow-up demonstrated resolution of obstructive oropharyngeal symptoms.
Conclusions:
Ectopic lingual thyroid tissue is rarely associated with obstructive oropharyngeal symptoms due to progressive enlargement. Radioiodine therapy with 131I is an effective treatment modality for ablation of ectopic thyroid tissue as an alternative to surgery.
Introduction
L
This study reports on three patients with lingual thyroid referred to the authors' division for consideration of radioactive iodine-131 (131I) therapy following endocrine or otolaryngology surgical consultation. The University of Michigan Institutional Review Board approved the retrospective review of medical records. There were no immediate post-radioiodine therapy complications, and in two patients, there was successful ablation of their ectopic thyroid tissue with radioactive 131I, thereby avoiding surgery. The third patient had surgical resection of a thyroglossal duct mass followed by radioiodine treatment of a lingual thyroid with ectopic tissue uptake depicted on the post-radioiodine therapy 131I scan.
Methods of Calculation
As part of the diagnostic evaluation, thyroid scans were performed with either iodine-123 (123I) or technetium-99m (99mTc) radiotracers using hybrid single-photon emission computed tomography/computed tomography (SPECT/CT) that confirmed the presence of a lingual thyroid and absence of an orthotopic thyroid gland in all patients. One patient also had concurrent subhyoid ectopic thyroid tissue. Measurement of 24-hour radioactive iodine uptake (RAIU) was performed in all patients. The target volume of therapy was determined by tridimensional anatomic measurements (Anterior-Posterior (A-P) × Transverse (TV) × Cranial-Caudal (C-C)) of lingual thyroid tissue using the CT component of the SPECT/CT scans, based on an ellipsoid (π/6 × A-P × TV × C-C) model (8). In clinical practice, soft-tissue density is approximated at 1 g/mL. Therefore, the volumetric measurements of the lingual thyroid were approximated to the thyroid tissue mass.
A therapeutic 131I activity was used calculated to deliver a dose of 0.3 mCi per gram of thyroid tissue retained in the lingual thyroid gland at 24 hours by the formula:
According to this formula, the prescribed therapy 131I dose is directly proportional to the mass of thyroid tissue and inversely proportional to the RAIU (9). The intended dosing factor of 0.3 mCi per gram of thyroid tissue is a strategy used in pediatric hyperthyroidism when there is an emphasis on achieving successful RAI treatment with a single therapy administration (10). To optimize RAIU, patients were prepared with a low-iodine diet for one week prior to RAIU and subsequent administration of 131I therapy with the intent of maximizing radioiodine uptake and reducing the therapeutic 131I dose. In addition, levothyroxine (LT4) withdrawal for four weeks was performed with the goal of increasing the 131I uptake and the retention in the lingual thyroid tissue. Liquid 131I was used for treatment, with therapeutic 131I doses prepared on-site by the nuclear pharmacist.
The information obtained by SPECT/CT on the size of the lingual thyroid tissue and the 24-hour RAIU measurement within the glandular tissue may contribute valuable data that can guide selection of the therapeutic 131I dose, by highlighting potential problems with RAI treatment (e.g., very low uptake or very large ectopic deposits). In two patients, the actual administered RAI dose used was higher than the calculated dose. Influenced by prior reports that described the need for significantly higher doses of 131I administration for treatment of lingual thyroids, and with the intention of achieving rapid resolution of oropharyngeal obstructive symptoms, the treating clinician used a higher dose than indicated by the calculations to maximize the chance of successful treatment with a single RAI therapy. Dosing of RAI based solely on calculations obtained from SPECT/CT information still needs to be further investigated in this rare condition.
Patients
Patient 1
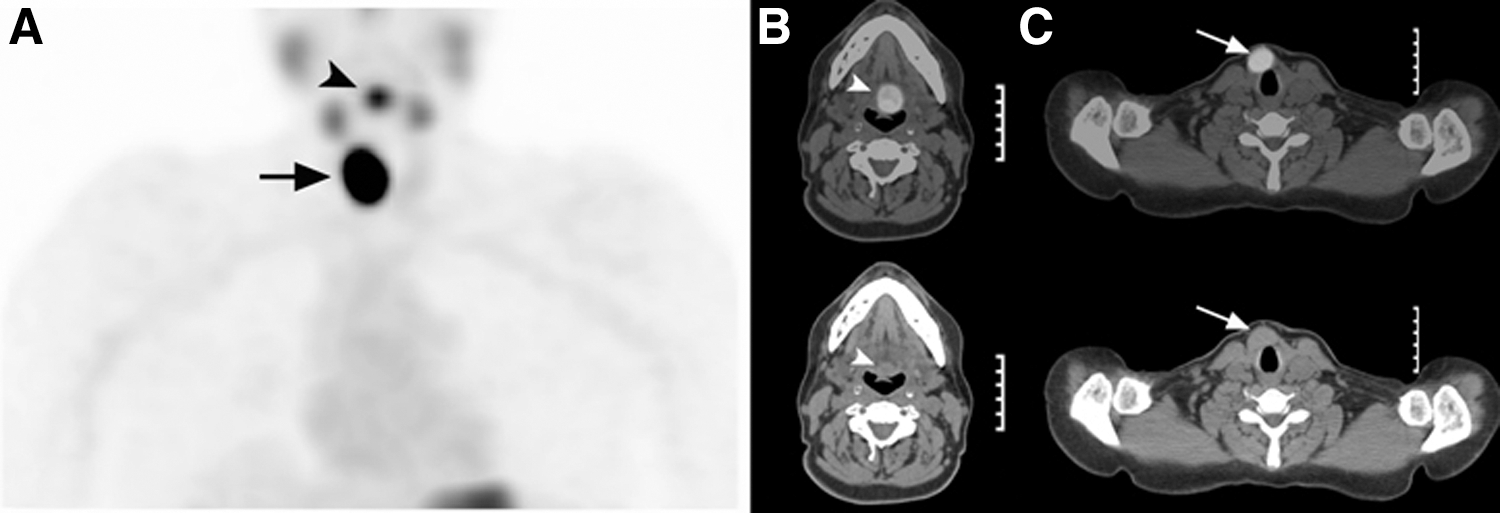
A 20-year-old woman presented with six to eight months of progressive dysphagia, intermittent odynophagia, and frequent upper respiratory infections. Her past medical history was significant for diagnosis of a lingual thyroid at three years of age. Evaluation for a sore throat at the time revealed the presence of a mass at the base of the tongue, which was proven to be thyroid tissue by direct biopsy. She was hypothyroid and was placed on LT4 treatment. She had an uneventful clinical course throughout her childhood and adolescence, but in early adulthood presented with progressive obstructive oropharyngeal symptoms with difficulties swallowing some solid foods, including tablets, which tended to “stick” at the base of the tongue. She did not report problems with liquids. After initial evaluation by an otolaryngologist, she was referred for non-surgical management of the lingual thyroid. Physical examination revealed the presence of an approximately 2.0 cm fleshy mucosal nodule in the midline of the posterior tongue that displaced the uvula to the right. The mass was easily visualized when the patient protruded her tongue. Her TSH was 1.1 mIU/L, free triiodothyronine (fT3) was 2.7 pg/mL, and free thyroxine (fT4) was 1.43 ng/dL while taking 0.075 mg of LT4 daily. She underwent four weeks of LT4 withdrawal, resulting in endogenous hypothyroidism and an elevation of her TSH to 15.0 mIU/L. A thyroid scan performed after administration of 123I demonstrated focal uptake in the oral cavity (Fig. 1A), which on SPECT/CT localized to a high attenuation soft-tissue mass at the base of tongue measuring 1.9 cm × 1.7 cm × 2.4 cm (Fig. 1B), resulting in a calculated volume of 4.0 g of glandular tissue. There was absence of an orthotopic, functioning thyroid gland. The 24-hour 123I uptake was 10.3%. The patient received 10.7 mCi of 131I for ablation of her lingual thyroid (calculated activity 11.7 mCi).

Baseline radioiodine (RAI) scintigraphy after oral administration of 0.4 mCi of iodine-123 (123I) was performed at 4 and 24 hours. (
After radioiodine therapy, the patient resumed therapy with LT4. At a six-month follow-up, she was well and noted resolution of her previously reported obstructive oropharyngeal symptoms. Physical examination revealed near complete disappearance of the lingual thyroid mass. The uvula had returned to a midline position. A repeat 99mTc pertechnetate thyroid scan depicted interval resolution of lingual thyroid tissue (Fig. 1C).
Patient 2
A 53-year-old woman presented with globus sensation and a choking sensation when lying supine that was present for the past two years. She was diagnosed with hypothyroidism at the age 40 years, and started on LT4. At the time of evaluation, she was on 0.112 mg daily. Physical examination revealed an unremarkable oral cavity and oropharynx. Indirect laryngoscopy revealed a round, symmetric midline mass at the base of the tongue. No thyroid gland was palpable in the lower neck. A SPECT/CT 99mTc pertechnetate thyroid scan demonstrated focal radiotracer accumulation at the base of the tongue, corresponding to a rounded, high attenuation, 2.5 cm tongue base mass without evidence of normal thyroid tissue in the expected anatomic location at the base of the neck.
A four-week LT4 withdrawal protocol produced subclinical hypothyroidism (TSH 7.81 mIU/L; fT4 0.72 ng/dL; fT3 2.4 pg/mL) and a 123I thyroid scan depicted radioactivity in lingual thyroid tissue measuring 2.5 cm × 1.8 cm × 2.4 cm, resulting in a calculated volume of 5.6 g of glandular tissue. A 24-hour 123I uptake was 13.5%. The patient was treated with 17.5 mCi 131I (calculated activity 12.6 mCi). She resumed LT4 replacement shortly after RAI therapy. At six months post-radioiodine therapy, she reported decreased globus sensation. A SPECT/CT 99mTc pertechnetate thyroid scan showed resolution of the increased radiotracer uptake in the lingual thyroid tissue, with a 65% interval reduction in size of the soft-tissue nodule at the tongue base, displaying a CT attenuation similar to that of surrounding tissues, consistent with residual post-therapy scar tissue.
Patient 3
A 38-year-old woman presented to medical attention with a one-year history of globus sensation and progressive dysphagia with both solids and liquids. CT of the neck demonstrated two homogenously enhancing soft-tissue nodules: the first was located anterior and parasagittal to the right thyroid cartilage, and the second was at the midline of the tongue base. A 99mTc pertechnetate thyroid scan performed five months later revealed increased radiotracer activity corresponding to these soft-tissues nodules, consistent with thyroid ectopy (Fig. 2). The anterior right paratracheal ectopic thyroid tissue nodule measured 3.9 cm × 2.7 cm × 1.5 cm, and the lingual thyroid measured 1.4 cm × 1.1 cm × 1.2 cm (calculated volume 0.97 g of glandular tissue). There was absence of an orthotopic, functioning thyroid gland. Yet, the patient was euthyroid. She underwent surgical excision of the right paratracheal ectopic thyroid tissue. However, the endocrine surgeon deferred operating on the lingual thyroid because of potential comorbidities (pain, bleeding, infection) associated with tongue surgery. Instead, the patient was referred for RAI ablation. Four weeks after surgery, the patient's TSH was 71 mIU/L, and her 24-hour 131I uptake was 3.9%. After low-iodine diet preparation, she was treated with 15.4 mCi of 131I (calculated activity 7.4 mCi). Following 131I treatment, thyroid hormone replacement was started with 0.15 mg of LT4 daily. A post-therapy 131I thyroid scan performed five days following treatment showed intense focal radiotracer uptake at the base of the tongue, consistent with RAI targeting the lingual thyroid tissue.
Baseline scintigraphy was performed 20 minutes after intravenous administration of 5 mCi of 99mTc pertechnetate. (
The patient demographics, presenting symptoms, imaging, RAI treatment, and outcomes are summarized in Table 1.
I, iodine-123; 131I, iodine-131; 99mTc, technetium-99m; LT4, levothyroxine; SPECT/CT, single-photon emission computed tomography/computed tomography.
Discussion
Ectopic thyroid tissue is a rare developmental anomaly affecting embryogenesis of the thyroid in its descent from the primitive foregut location to the final pretracheal location in the neck (1). The thyroid is the first endocrine gland to develop in the embryo. At approximately the third to fourth gestational week, the primordium of the medial part of the thyroid forms as an endodermal thickening of the midline floor of the pharynx between the first and second pharyngeal arches (11 –13). Primitive thyroid cells derived from the thyroid anlage penetrate the underlying mesenchymal tissue, migrating caudally anterior to the hyoid and the laryngeal cartilages to reach the normal pretracheal position around the seventh gestational week (2), with fetal thyroid hormone detectable by the 11th gestational week (13). The proximal segment of the thyroglossal duct regresses between the 5th and 10th weeks of development, leaving a permanent pit at the dorsum of the tongue, known as the foramen cecum (14,15).
The prevalence of thyroid ectopia is estimated at 1/100,000–300,000 persons (1). Reported locations of ectopic thyroid tissue include lingual, intralingual, sublingual, thyroglossal duct cyst, low neck ectopia, intratracheal, esophageal, mediastinal, aortic, intracardiac, and abdominal ectopias. Lingual thyroid is the most common type, accounting for 90% of reported cases (1). Ectopic lingual thyroid tissue was first reported in 1869 (3,16,17). About 75% of patients with a lingual thyroid lack thyroid tissue at the normal cervical location, and up to 70% are hypothyroid, although hyperthyroidism has rarely been reported (1,7). Ectopic thyroid tissue often has functional insufficiency, and undergoes compensatory enlargement, seen more commonly in patients who have increased physiological requirement of thyroxine during periods of active growth, puberty, and pregnancy. In the case of a lingual thyroid, this increase in size may result in clinical symptoms of dysphagia, dysphonia, or dyspnea. Occasionally, obstructive sleep apnea and difficulties with intubation have been noted in relation to lingual thyroid tissue, whereas malignancy is rare (1).
Ectopic thyroid tissue is diagnosed using ultrasound (US), CT, magnetic resonance imaging (MRI), fine-needle aspiration biopsy, and radionuclide scanning, performed in the context of differential diagnosis of a neck mass or during the workup of (congenital) hypothyroidism (1,18,19). The presence of normal thyroid tissue in the neck is easily ascertained with US or CT. Radionuclide scanning is virtually diagnostic, either with 99mTc pertechnetate, 123I, or 131I through uptake of this radionuclide by the sodium–iodide symporter (NIS). This allows the thyroid origin of the ectopic tissue to be confirmed, and whether there is an orthotopic thyroid gland present to be assessed (1). The frequency of ectopic thyroid tissue was studied in 11,905 thyroid scans over a period of five years for investigation of neck masses or hypothyroidism. The scans were grouped as (i) athyreosis with absence of discernable thyroid tissue, (ii) a single visualized site of ectopic thyroid tissue, or (iii) dual ectopia, defined as the simultaneous presence of two distinct populations of ectopic thyroid tissue (20). There were 121 patients with thyroid dysgenesis: 32 athyroid cases, 83 with a single site of ectopic thyroid tissue, and 6 with dual ectopic thyroid tissue (2). The authors reviewed cases of dual ectopic thyroid tissue in the neck, noting 42 published cases, comprised of lingual thyroid in 33%, sublingual in 27%, and subhyoid in 22% sites, with most patients <30 years old. Of these, 38% were euthyroid, 33% hypothyroid, and 21% had subclinical hypothyroidism (2). Typically planar or pinhole scintigraphic imaging is sufficient for diagnosis, although the benefit of 3D SPECT imaging for lingual thyroid has been reported (21). Both 99mTc pertechnetate SPECT/CT (7,22,23) or 123I SPECT/CT scans to depict radioiodine uptake within lingual thyroid have been reported (24,25). In one case SPECT/CT clearly demonstrated 99mTc pertechnetate uptake within a dual thyroid ectopia (lingual and sublingual sites) with absence of an orthotopic thyroid, similar to the third patient in this study (23).
Medical management with thyroid hormone replacement has been used to suppress the growth of lingual thyroid tissue, and to achieve shrinkage of ectopic thyroid tissue, thus providing relief of obstructive symptoms. Surgery is the traditional definitive treatment considered when conservative management is unsuccessful and if the patient develops oropharyngeal obstruction, bleeding, sudden enlargement of the lingual thyroid, or if there is evidence of malignancy (1). The intent of treatment of lingual thyroid glands consists in achieving a measurable reduction in the size of the gland with the goal to relieve symptoms such as dysphagia, odynophagia, or dyspnea. A range of surgical approaches have been described in the literature (26 –28), along with other targeted therapies (29). Surgical excision has been described via trans-oral, lateral pharyngotomy, and suprahyoid approaches. The trans-oral approach is ideally suited for small lingual thyroid masses located superior to the hyoid. Occasionally a mandibulotomy and midline tongue splitting approach is required for larger lesions (30,31). Bleeding and pain are common, as is post-surgical scar in excision of larger lesions. Trans-oral robotic surgery (TORS) and transposition flaps to shift the lingual thyroid to the lateral oral floor are newer surgical techniques (1,32). Successful use of TORS was reported in three symptomatic lingual thyroid patients, with resolution of symptoms and satisfactory cosmetic results, and no perioperative complications or significant bleeding (33). Other newer targeted treatments such as CO2 laser (34) and radiofrequency ablation (35) have been reported without bleeding complications.
RAI is another treatment option for symptomatic lingual thyroids (1), with the first case of RAI treatment reported by Schilling et al. in 1950 (36,37). In 1955, two siblings with lingual thyroid were treated as infants with RAI mixed in milk, with resultant shrinkage of their masses at the base of the tongue and resolution of symptoms (38). However, since that time, RAI therapy has not been widely used due to concerns regarding radiation exposure in younger individuals, the potential of possible airways obstruction after RAI administration, and concerns about delivering sufficient RAI activity to ablate the ectopic thyroid tissue. Despite these concerns, there are multiple reports of successful RAI treatment of lingual thyroid. Danner et al. reviewed their experience over a six-year period, and found two patients with lingual thyroid glands treated successfully with 30 mCi and 85 mCi 131I (36). These patients had complete resolution of symptoms at two months after RAI treatment, with no airway compromise and subsequent development of hypothyroidism (follow-up to 18 and 24 months). Iglesias et al. reported a patient treated with 20 mCi of 131I in two divided 10 mCi doses separated by nine months (39). The authors did not specify the therapeutic strategy for RAI dose fractionation, whether this represented a failure of the first dose of 131I therapy, or if the RAI therapy was planned as two separate doses from the outset. Park et al. reported successful treatment of a lingual thyroid with an unspecified 131I dose (24). A 27-year-old woman with a large 8 cm × 6 cm biopsy-confirmed submental ectopic thyroid mass was imaged with 99mTc pertechnetate and a correlative MRI. She was treated successfully with 26 mCi 131I, leading to resolution of swelling and compressive symptoms after three months, and she was well at two years of follow-up on thyroid hormone replacement (3). A 48-year-old woman with a 3 cm lingual thyroid presenting with obstructive sleep apnea and intermittent dyspnea and dysphagia was imaged with 123I SPECT/CT and was found to have a 24-hour 123I uptake of 14.5%. Due to high surgical risk, an alternative approach to surgical excision was preferred, and 30 mCi of 131I was used to ablate the lingual thyroid successfully, with an 83% reduction in the volume of the lingual thyroid and resolution of symptoms at two years of follow-up (24).
This study contributes an additional three cases to the prior nine cases reported in the literature. This report illustrates the use of SPECT/CT imaging for the diagnosis and planning of RAI therapy for ablation of ectopic lingual thyroid. Two of the patients returned for clinical follow-up: one patient reported resolution of oropharyngeal obstructive symptoms, and the other patient reported significant improvement of globus sensation. Follow-up 99mTc pertechnetate scintigraphy obtained at six months after 131I therapy demonstrated successful ablation of all lingual thyroid tissue. The third patient had two ectopic foci with surgical excision of a subhyoid thyroid mass followed by RAI treatment of a lingual thyroid. A RAI post-therapy scan depicted lingual thyroid, although the patient was lost to follow-up. All three patients reported in this study received oral liquid 131I formulation for radioablation. The therapeutic 131I formulation (i.e., liquid vs. capsule) used in other reported series is unknown, as is whether problems were encountered in administering RAI to patients with thyroid ectopia.
Each patient had specialist thyroid surgical consultation, with either an endocrine or otolarygology surgeon, and each case was discussed at multidisciplinary tumor boards. Lingual thyroid is a rare condition, it is not known how many surgeries (if any) were performed for lingual thyroids during the same six-year time period at the authors' institution. The decision to select patients for RAI treatment rather than surgery was based on numerous factors, including symptomatology, location of ectopic thyroid tissues, comorbidities, perceived concerns of complications of RAI versus surgery, suitability for robotic surgery via the transoral route (33), RAIU values, and willingness to adhere to post-RAI therapy radiation safety precautions. Patient preference played an important role in final decision making. Cases reported in the literature are characterized by variable approaches for the selection of RAI treatment. They report a range of lingual thyroid uptake values, and do not specify methods for calculation of therapeutic 131I activities that ranged between 20 and 85 mCi. In these cases, the estimation of lingual thyroid tissue volume was obtained from separately acquired CT or MRI imaging studies. The authors' experience is that hybrid SPECT/CT can give valuable information regarding size, location, the nature of the ectopic thyroid tissue, and RAIU values, which can then assist in the selection of a therapeutic 131I activity using well-established methods. 99mTc pertechnetate or 123I scintigraphy with SPECT/CT can also be used in the follow-up assessment of therapeutic efficacy.
Conclusion
Lingual thyroid is a rare developmental anomaly that may require size reduction when progressive enlargement of ectopic thyroid tissues causes obstructive or compressive oropharyngeal signs and symptoms. Surgery has been traditionally used to extirpate ectopic thyroid tissue at the base of the tongue. RAI treatment is a safe and effective alternative treatment to ablate lingual thyroid tissue, with marked improvement or resolution of symptoms.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose. No competing financial interests exist.