
Abstract
Background:
The impact of subclinical hypothyroidism (SCH) and of levothyroxine replacement in pregnant women with SCH is unclear. The aims of this study were to assess (i) the impact of SCH during pregnancy on maternal and neonatal outcomes, and (ii) the effect of levothyroxine replacement therapy in these patients.
Methods:
Ovid MEDLINE In-Process & Other Non-Indexed Citations, Ovid MEDLINE, the Cochrane Controlled Trials Register, Ovid EMBASE, Web of Science, and Scopus were searched from inception to January 2015. Randomized trials and cohort studies of pregnant women with SCH that examined adverse pregnancy and neonatal outcomes were included. Reviewers extracted data and assessed methodological quality in duplicate. Eighteen cohort studies at low-to-moderate risk of bias were included. Compared with euthyroid pregnant women, pregnant women with SCH were at higher risk for pregnancy loss (relative risk [RR] 2.01 [confidence interval (CI) 1.66–2.44]), placental abruption (RR 2.14 [CI 1.23–3.70]), premature rupture of membranes (RR 1.43 [CI 1.04–1.95]), and neonatal death (RR 2.58 [CI 1.41–4.73]). One study at high risk of bias compared pregnant women with SCH who received levothyroxine to those who did not and found no significant decrease in the rate of pregnancy loss, preterm delivery, gestational hypertension, low birth weight, or low Apgar score.
Conclusions:
SCH during pregnancy is associated with multiple adverse maternal and neonatal outcomes. The value of levothyroxine therapy in preventing these adverse outcomes remains uncertain.
Introduction
S
In comparison with OH where there is clear evidence for adverse events, the impact of SCH on pregnancy is unclear (4). Multiple studies have reported an association of SCH with an increase in the risk of adverse pregnancy and neonatal outcomes, including pregnancy loss, preterm delivery, gestational diabetes, gestational hypertension, preeclampsia, placental abruption, premature rupture of membranes, intrauterine growth restriction, low birth weight, small for gestational age, low Apgar score, and neonatal death (5 –16). Furthermore, high TSH levels in women during pregnancy have been associated with an increased risk of neurocognitive deficits in the offspring (17). Other studies, however, have not found any adverse outcomes associated with SCH (18 –21). Moreover, there is uncertainty regarding the impact of levothyroxine replacement on improving outcomes in pregnant women with SCH (4). A previous systematic review in 2011 included five articles reporting on the adverse outcomes associated with SCH, and the meta-analysis included a maximum of three studies for each of the evaluated outcomes (22). In 2013, a Cochrane review on interventions for SCH during pregnancy did not identify any studies evaluating the effectiveness of levothyroxine therapy on maternal and neonatal outcomes (23). Since the publication of those two reviews, more studies have become available, which justifies a new quantitative synthesis of the available evidence.
A systematic review was therefore conducted, summarizing the evidence for the adverse clinical impact of SCH during pregnancy and for the value of levothyroxine therapy in mitigating that impact.
Methods
A systematic review and meta-analyses were performed to estimate (i) the impact of SCH compared to euthyroidism on maternal and neonatal outcomes in pregnant women, and (ii) the efficacy of levothyroxine therapy in preventing adverse maternal and neonatal events in pregnant women with SCH. This report follows a review protocol adhering to current standards for reporting of systematic reviews (24).
Eligibility criteria
To assess the impact of SCH on maternal and neonatal outcomes, randomized trials and cohort studies were sought that compared pregnant women with SCH to euthyroid pregnant women. Participants were pregnant women who had thyroid function tests during pregnancy to determine their thyroid status. SCH was defined as an elevated TSH concentration with normal serum T4 level (either total of free) or as an elevated TSH concentration between 2.5 and 5 mIU/L. To determine the impact of levothyroxine therapy, randomized trials and cohort studies were sought that compared pregnant women with SCH who received levothyroxine replacement therapy to those who did not. Studies in which the required information to determine eligibility was not available in the manuscript and where no response from the authors seeking that information was obtained were excluded. Studies that reported on a mixed population of SCH and OH during pregnancy were also excluded.
The main outcome measure was pregnancy loss (miscarriage, intrauterine death, fetal loss). Other outcomes included: preterm labor (onset of labor ≤37 weeks' gestation), preterm delivery (delivery ≤37 weeks' gestation), gestational hypertension (variously defined), preeclampsia (variously defined), eclampsia (variously defined), gestational diabetes (variously defined), placental abruption (premature separation of a normally implanted placenta), placenta previa (placental completely or partially covering the internal cervical os), premature rupture of membranes (PROM; variously defined), cesarean delivery, intrauterine growth restriction (IUGR; variously defined), low birth weight (≤2500 g), low Apgar score (≤7 at 5 min), small for gestational age (variously defined), and neonatal death (variously defined). Pregnancy loss was chosen as the main outcome because it is an outcome important to patients (25) that has significant consequences for pregnant women.
Study identification
A comprehensive search from each database's inception to January 2015 was conducted with no language restrictions. The databases included Ovid MEDLINE In-Process & Other Non-Indexed Citations, Ovid MEDLINE, the Cochrane Controlled Trials Register, Ovid EMBASE, Web of Science, and Scopus. An experienced librarian (P.J.E.) designed the search strategy with input from the study's principal investigator (S.M.). Controlled vocabulary supplemented with keywords was used to search for studies of SCH during pregnancy. The search strategy is available in Appendix 1. The reference list of narrative reviews was reviewed, and experts were consulted to identify additional references.
The search results were uploaded into a systematic review software (DistillerSR, Ottawa, Canada). Reviewers working independently and in duplicate reviewed all abstracts and titles for inclusion. After abstract screening and retrieval of potentially eligible studies, the full-text publications were assessed for eligibility with excellent chance-adjusted inter-reviewer agreement (κ statistic = 0.87). Duplicate studies were excluded. Disagreements were resolved by consensus.
Data collection and management
Reviewers working independently and in duplicate using a standardized web-based form collected the following information from each eligible study: (i) baseline clinical features: gestational age at screening, race/ethnicity, body mass index (BMI), history of smoking, previous pregnancy, pregnancy loss, and preterm delivery, family history of thyroid disease, use of in vitro fertilization/assisted reproduction to achieve the index pregnancy, and educational level; (ii) TSH, T4, and thyroid peroxidase (TPO) antibody levels; (iii) main and other outcomes. The definition of SCH used in each study was also extracted. Disagreements were resolved by discussion and consensus. Unclear data were confirmed with the study author when possible.
Risk of bias assessment
The Newcastle-Ottawa risk of bias tool for observational studies was used to evaluate the methodological quality of included studies (26). This tool determines the comparability of the cohorts, their representativeness, and the ascertainment of exposure and outcomes. For the study assessing the impact of levothyroxine on SCH-related pregnancy and neonatal outcomes, risk-of-bias criteria for causal inferences about therapy were adapted (27). Reviewers working independently assessed the risk of bias of included studies in duplicate. Any disagreements were resolved by consensus.
Author contact
To reduce reporting bias, the authors of studies in which clarification or more information was needed to determine eligibility or to complete analyses were contacted. If no response was received from an initial e-mail contact, authors were contacted again after a four-week period by e-mail.
Meta-analysis
Random-effects meta-analyses were conducted using the DerSimonian and Laird method (28) to pool relative risk (RR) and estimate 95% confidence intervals (CI) for each of the outcome measures. Inconsistency was assessed using the I 2 statistic, with values <25% indicative of low and >75% indicative of high inconsistency not due to chance (29). Review Manager v5.2 was used for statistical analyses (30).
Subgroup and sensitivity analyses
Sensitivity analyses were conducted to explain possible inconsistencies across study results on the main outcome of pregnancy loss. To understand the effect of gestational age at screening for thyroid dysfunction, only studies that included women screened between 0 and 12 weeks of pregnancy (first trimester) and then studies that included women screened at early pregnancy (20th week of gestation or earlier) were analyzed. A sensitivity analysis omitting studies at high risk of bias was planned. Finally, a subgroup analysis was also planned based on the TPO antibody status of the study population.
Results
Study identification
The search identified 1108 potentially eligible studies, of which 18 cohort studies studying 3995 pregnant women with SCH were eligible (5
–8,10
–14,18
–21,31
–35) (Supplementary Fig. S1; Supplementary Data are available online at
Study characteristics
Table 1 summarizes study characteristics. Due to inconsistent reporting, it was not possible to present data regarding BMI, history of smoking, history of previous pregnancy, pregnancy loss, and preterm delivery, family history of thyroid disease, use of in vitro fertilization/assisted reproduction to achieve the index pregnancy, TSH, T4, and TPO antibody levels. Five studies screened women for thyroid dysfunction during the first trimester of pregnancy, and 14 studies screened women during early pregnancy (20th week of gestation or earlier). There was no eligible study reporting on eclampsia.
Data presented as mean (standard deviation).
Median (range).
This study reported the same outcomes in an overlapping population with Casey 2007 and was used for sensitivity analysis.
This study has the same population with the study Mannisto 2009 but reports different outcomes.
fT4, free thyroxine; NA, not available; Tx, treated group; Non-Tx, non-treated group; SCH, subclinical hypothyroidism; TSH, thyrotropin.
Study quality
The risk of bias of included studies comparing pregnant women with SCH to euthyroid women was low to moderate, mainly due to limitations in the representativeness of study samples, lack of blinding when assessing the outcomes, and lack of adjustment for confounders (Table 2). The risk of bias of the study assessing the effect of levothyroxine therapy in pregnant women with SCH was high due to lack of randomization and blinding.
Meta-analysis
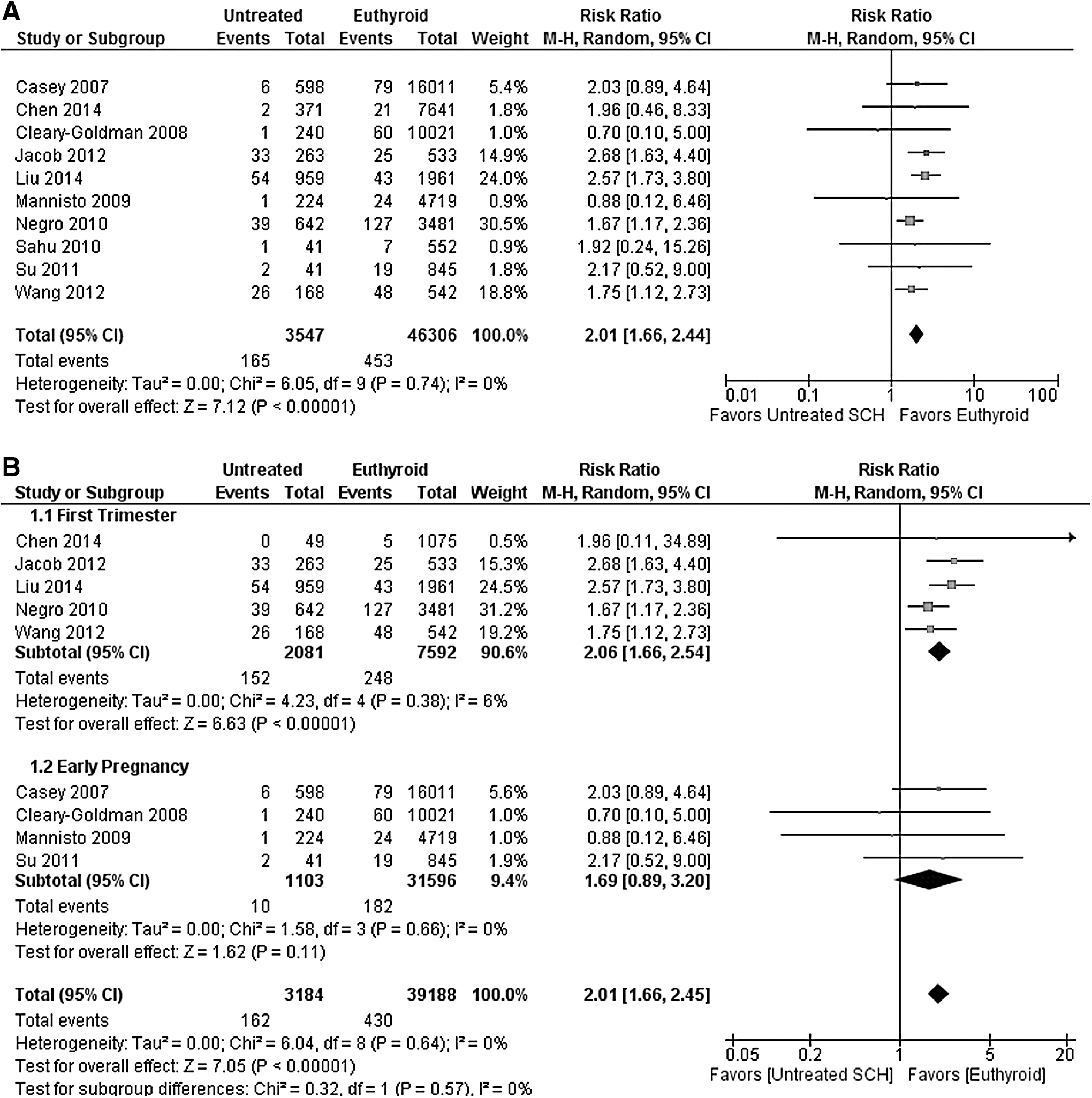
Table 3 presents the pooled estimates of association between SCH and pregnancy outcomes. Compared with euthyroid pregnant women, pregnant women with SCH had a higher risk of pregnancy loss (RR 2.01 [CI 1.66–2.44]; I 2 = 0%; Fig. 1A), placental abruption (RR 2.14 [CI 1.23–3.70]; I 2 = 0%), PROM (RR 1.43 [CI 1.04–1.95]; I 2 = 9%), and neonatal death (RR 2.58 [CI 1.41–4.73]; I 2 = 0%). There was no association found for gestational diabetes, preterm labor, preterm delivery, gestational hypertension, preeclampsia, placenta previa, cesarean delivery, IUGR, low birth weight, low Apgar score, and small for gestational age.
(
RR, relative risk; CI, 95% confidence interval; PROM, premature rupture of membranes; IUGR, intrauterine growth restriction.
Wang et al. (11) screened pregnant women in the first trimester (≤12 weeks) for thyroid dysfunction. Women with SCH were recommended to start on levothyroxine, but only 14% received therapy. The study found an increased risk of pregnancy loss in pregnant women with SCH compared with euthyroid pregnant women (RR 1.75 [CI 1.12–2.73]). However, comparing 28 pregnant women with SCH who received levothyroxine replacement therapy to 168 women who did not receive levothyroxine, the study did not find a statistically significant decrease in the rate of pregnancy loss (RR 0.46 [CI 0.12–1.84]), preterm delivery (RR 0.31 [CI 0.02–5.13]), gestational hypertension (RR 3.00 [CI 0.28–31.99]), low birth weight (RR 0.65 [CI 0.04–11.71]), and low Apgar score (RR 0.65 [CI 0.04–11.71]) with levothyroxine therapy. The confidence in these results is limited due to the small sample size and number of events (imprecision), as well as the high risk of bias (most importantly selection bias).
Subgroup and sensitivity analyses
Figure 1B shows the result of the pre-planned sensitivity analysis on gestational age: including only studies in which women were screened for thyroid dysfunction between 0 and 12 weeks of pregnancy (first trimester) resulted in a RR for pregnancy loss of 2.06 [CI 1.66–2.54], while including studies in which women were screened throughout early pregnancy (20th week of gestation or earlier) resulted in an RR of 1.69 ([CI 0.89–3.20]; p-value for difference = 0.57). We did not find any studies at high risk of bias for the comparison between pregnant women with SCH and euthyroid pregnant women. Therefore, no sensitivity analysis was conducted to explore the effects of risk of bias.
In addition to the pre-planned sensitivity analysis, sensitivity analyses analyzing the impact of certain decisions made during the conduct of the study were performed. First, a sensitivity analysis was conducted in which the study from Casey et al. from 2007 (12) was replaced with the overlapping study from Casey et al. from 2005 (5). The analysis revealed similar pooled estimate results (data not shown). Second, a sensitivity analysis in which the unpublished study from Jacob et al. from 2012 (35) was removed resulted in similar pooled estimates (data not shown). Finally, a sensitivity analysis was performed in which both the study by Negro et al. from 2010 (6) and Jacob et al. from 2012 (35) were removed on the basis of their different SCH definitions with no significant change in the results (Supplementary Table S1).
Finally, due to insufficient data, it was not possible to perform a subgroup analysis based on the TPO antibody status of the study population.
Discussion
Summary of evidence
In this systematic review of 18 studies at low-to-moderate risk of bias including 3995 pregnant women with SCH, it was found that pregnant women with SCH were at higher risk for pregnancy loss, placental abruption, PROM, and neonatal death compared with euthyroid pregnant women. Only one observational study on the effect of levothyroxine in pregnant women with SCH was identified, but this study was at high risk of bias and yielded imprecise results.
Limitations and strengths
Incomplete searching and arbitrary study selection represent potential limitations of systematic reviews. However, the rigorous and comprehensive nature of the overlapping search strategies should have minimized the possibility that studies were missed that could substantially change the inferences drawn from the study. The risk of publication bias is high, particularly when the body of evidence is based on small observational studies. The results of this meta-analysis are driven by 10 larger studies that included >100 pregnant women with SCH. Despite the inconsistency in the gestational age at screening for thyroid function and in the definitions of SCH used, this seemed to contribute little to the variability in the estimates of association, which was moderate at worst. Although it would have been clinically meaningful, due to insufficient data, it was not possible to stratify the results by TPO antibody status. Another limitation is the paucity of evidence regarding the effect of levothyroxine replacement therapy in pregnant women with SCH. Although these limitations cannot be overcome methodologically, this review exhibited important strengths, as the study sought to summarize the totality of the available evidence following a predesigned protocol, reproducible judgments about study selection and quality, author contact, and focused analyses including an assessment of the effect of gestational age at screening for thyroid dysfunction that has not been performed previously (36).
Implications for practice and research
The present results support an association of SCH during pregnancy with adverse maternal and neonatal outcomes. This association may not be causal, and its magnitude may be overestimated by publication bias. Limitations and variability in study design reduce confidence in the results, and direct reliable evidence of the extent to which levothyroxine treatment in these women could improve pregnancy and neonatal outcomes is not available.
The study shows that there is inconsistency in the definitions of SCH used in the included studies, underscoring the lack of consensus among clinicians and researchers. Currently, in the absence of a laboratory trimester-specific reference range for TSH, a fixed cutoff of 2.5 mIU/L for the first trimester and 3 mIU/L for the second and third trimester is used (2). However, the reference range for TSH and free T4 can vary with geographic area and race/ethnicity (4,37). Indeed, 12/14 recent studies on reference range found that the upper trimester-specific TSH limit was >2.5 or 3 mIU/L, suggesting that a large number of pregnant women could be overdiagnosed with SCH and subsequently be overtreated when using a fixed TSH cutoff (37). Therefore, adapting a population-based reference range could lead to a more accurate diagnosis of SCH. The real challenge is to establish the TSH level above which women experience adverse pregnancy outcomes and levothyroxine therapy prevents these outcomes.
Indirect evidence for the effectiveness of levothyroxine in preventing pregnancy and neonatal complications is provided by one large randomized study designed to compare “universal screening” versus “case finding” in detecting thyroid dysfunction (38). Tests for thyroid function were performed immediately in women who were assigned in the “universal screening” group and in women at the “case finding” group only if there were deemed to be at high risk for thyroid dysfunction. In contrast, the serum samples were frozen and assayed after delivery for women at low risk for thyroid dysfunction in the “case finding” group. Hypothyroid pregnant women who were found to have a TSH >2.5 mIU/L and positive TPO antibody levels were started on levothyroxine. The study found that the proportion of hypothyroid women with at least one adverse obstetrical or neonatal outcome was significantly higher in the low-risk “case finding” group (not diagnosed and thus untreated, 91%) compared with the low-risk “universal screening” group (diagnosed and treated, 34%), suggesting a benefit from levothyroxine replacement. Moreover, adverse outcomes were less likely to occur among women in the “universal screening” group than among women in the “case finding” group (OR 0.43 [CI 0.26– 0.70]). This effect was driven primarily by adverse outcomes experienced by low-risk hypothyroid women (p = 0.005) who received treatment in the “universal screening” group but not in the “case finding” group. Given that there was no cutoff for T4 level, this study by design could have included pregnant women with OH who have more severe thyroid dysfunction compared with those with SCH and who are therefore at higher risk for adverse pregnancy and neonatal outcomes. Finally, the most commonly reported adverse outcome in this study was cesarean delivery with no further clarification as to the indication.
The same group conducted a prospective study where euthyroid TPOAb+ pregnant women were randomly assigned to levothyroxine therapy or no treatment, while TPOAb– pregnant women served as controls (39). The study found that euthyroid pregnant women who were TPOAb+ had an increased risk for pregnancy loss, which was mitigated with levothyroxine replacement.
A multicenter randomized trial assessed the impact of levothyroxine on the cognitive function among children of women who had TSH >97.5th percentile or free T4 <2.5th percentile, or both, during pregnancy (40). The treatment had no effect on the mean offspring IQ at three years or the proportion of children with IQ <85. A post hoc analysis for the subgroup of pregnant women who met the criteria for SCH had the same non-significant results.
Based on the analysis of the concurrent evidence, the American Thyroid Association (ATA) released their guidelines in 2011; the strength of each recommendation was graded according to the United States Preventive Services Task Force (USPSTF) system. In the USPSTF system, the strength of a recommendation is graded A, B, C, D, or I (if insufficient) based on the quality of the evidence (good, fair, poor, insufficient). The ATA guidelines recommend treatment of pregnant women with SCH and positive TPO antibodies (Level B, fair evidence—USPSTF), but found insufficient evidence to recommend for or against universal levothyroxine treatment in pregnant women with SCH and negative TPO antibodies (Level I—USPSTF) (2). The Endocrine Society, in addition to the USPSTF system, followed the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system to evaluate the strength of each recommendation and the quality of the evidence. The Endocrine Society panel recommends levothyroxine replacement in all pregnant women with SCH (weak recommendation, low-quality evidence) (41). Implementation of these guidelines will result in diagnosis with SCH and treatment with levothyroxine of up to 15% of pregnant women. The guideline panel acknowledges that the evidence is not sufficient, but focuses on accruing any potential benefit from levothyroxine replacement therapy, noting that any adverse effects such as iatrogenic thyrotoxicosis are rare. However, clinicians and their patients need reliable evidence to decide whether pregnant women with SCH will have better outcomes with levothyroxine replacement therapy.
The uncertainty documented in this review, the variability in expert recommendations, and the impact on the pregnancy experience of a large proportion of pregnant women underscore the need for randomized trials to estimate the effectiveness of levothyroxine therapy in this population, a point that has been emphasized by others (2,22,41,42). An ongoing randomized trial will hopefully offer some answers in the near future (
Conclusions
The extant body of evidence supports an association of SCH during pregnancy with multiple adverse maternal and neonatal outcomes, but there is paucity of evidence for the value of levothyroxine therapy to mitigate this association. Clinicians and patients must engage in frank and shared decision making while awaiting the results of ongoing efficacy trials and the conduct of larger trials of levothyroxine therapy in high-risk women with SCH during pregnancy.
Footnotes
Acknowledgments
We are grateful to the authors of primary studies who responded to our requests for data confirmation and missing data (C. Daumerie, J. Walsh, J. Jacob, R. Negro, M. Penin, M. Poulasouchidou, and S. Prema). We would like to thank Dr. Ana Castaneda-Guarderas for technical support. This publication was made possible by CTSA Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NIH.
Author Disclosure Statement
The authors have nothing to disclose.
| # | Searches | Results | Search type |
|---|---|---|---|
| 1 | Hypothyroidism/or hypothyroidism.mp. | 34,300 | Advanced |
| 2 | Thyroxine/ad, tu [Administration & Dosage, Therapeutic Use] | 6409 | Advanced |
| 3 | ((l adj thyroxin * ) or levothyroxine).mp. or 2 [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] | 9424 | Advanced |
| 4 | thyroxine.mp. and hormone replacement therapy/ [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] | 516 | Advanced |
| 5 | or/2–3 | 9424 | Advanced |
| 6 | 1 and 5 | 4670 | Advanced |
| 7 | exp Pregnancy Complications/ or Pregnancy Trimesters/ or pregnancy.mp. or Pregnancy Maintenance/ or exp Pregnancy/ or Pregnancy Rate/ or Pregnancy Trimester, Second/ or Pregnancy Outcome/ or Pregnancy Trimester, Third/ or Pregnancy Trimester, First/ | 804,495 | Advanced |
| 8 | (pregnancy or pregnant or preterm or gestational or apgar or intrauterine or birth or prematur * ).mp. [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] | 1,046,192 | Advanced |
| 9 | abortion, spontaneous/ or premature birth/ or obstetric labor, premature/ or diabetes, gestational/ or stillbirth.mp. [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] | 42,777 | Advanced |
| 10 | fetal growth retardation/ or infant, low birth weight/ or infant, very low birth weight/ or infant, extremely low birth weight/ or infant, small for gestational age/ | 37,380 | Advanced |
| 11 | hypertension, pregnancy induced/ or hellp syndrome/ or eclampsia/ or abruptio placentiae/ or pre-eclampsia/ or apgar score/ | 34,310 | Advanced |
| 12 | pregnancy outcome/ or miscarriage/ or fetal membranes, premature rupture/ or placenta previa/ | 55,760 | Advanced |
| 13 | Cesarean Section/ | 35,016 | Advanced |
| 14 | cesarean * .mp. or 9 or 10 or 11 or 12 or 13 [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] | 172,657 | Advanced |
| 15 | or/7–8,14 | 1,082,749 | Advanced |
| 16 | 6 and 15 | 701 | Advanced |
| 17 | limit 16 to (clinical trial, all or clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or clinical trial or comparative study or controlled clinical trial or evaluation studies or meta analysis or multicenter study or observational study or randomized controlled trial) | 73 | Advanced |
| 18 | 16 and (followup.mp. or follow-up studies/ or cohort * .mp. or prospective * .mp. or retrospective * .mp. or “cross-section * ”.mp. or trial * .mp. or meta-analysis.mp.) [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] | 180 | Advanced |
| 19 | 17 or 18 | 203 | |
| Cochrane—same strategy, 21 | |||
| Embase 1988 to 2015 Week 04 | |||
| 1 | hypothyroidism/ or subclinical hypothyroidism/ | 31,682 | Advanced |
| 2 | thyroxine/ct, ad, dt | 5402 | Advanced |
| 3 | (l adj thyroxine * ).mp. [mp = title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword] | 2127 | Advanced |
| 4 | levothyroxine sodium/ or levothyroxine/ | 12,441 | Advanced |
| 5 | or/2–4 | 18,035 | Advanced |
| 6 | 1 and 5 | 7932 | Advanced |
| 7 | exp pregnancy/ or exp pregnancy complications/ | 377,906 | Advanced |
| 8 | spontaneous abortion/ | 22,634 | Advanced |
| 9 | exp labor complication/ | 106,863 | Advanced |
| 10 | exp pregnancy disorder/ | 312,598 | Advanced |
| 11 | intrauterine growth retardation/ | 16,924 | Advanced |
| 12 | exp low birth weight/ | 37,013 | Advanced |
| 13 | exp “eclampsia and preeclampsia”/ | 33,153 | Advanced |
| 14 | exp “parameters concerning the fetus, newborn and pregnancy”/ | 213,446 | Advanced |
| 15 | or/7–14 | 598,381 | Advanced |
| 16 | 6 and 15 | 976 | Advanced |
| 17 | exp evidence-based medicine/ | 687,624 | Advanced |
| 18 | exp cross-sectional study/ or exp incidence/ or exp seasonal variation/ | 420,077 | Advanced |
| 19 | follow up/ | 829,505 | Advanced |
| 20 | exp cohort analysis/ or exp correlational study/ or exp cross-sectional study/ or exp double blind procedure/ | 428,223 | Advanced |
| 21 | prospective study/ or retrospective study/ | 618,004 | Advanced |
| 22 | exp case control study/ or exp case study/ or exp clinical trial/ or exp “clinical trial (topic)”/ or exp longitudinal study/ or exp major clinical study/ or exp prospective study/ or exp retrospective study/ | 2,996,565 | Advanced |
| 23 | or/17–22 | 3,909,344 | Advanced |
| 24 | 16 and 23 | 321 | Advanced |
| 25 | limit 24 to human | 316 | Advanced |
| 26 | 25 not case report/ | 265 | Advanced |
WoS
Scopus
( TITLE-ABS-KEY (