
Abstract
Background:
Antithyroid drug (ATD)–induced agranulocytosis is a rare but life-threatening disease. Clinical features of ATD-induced agranulocytosis and outcomes remain incompletely understood.
Method:
Patients with clinically diagnosed ATD-induced agranulocytosis were retrospectively studied, involving 9690 patients who were referred for radioiodine treatment during a 15-year period (2000–2015) in China. There were 114 cases of agranulocytosis attributable to ATD included, and their clinical characteristics and therapy outcomes were analyzed.
Results:
The female-to-male ratio of ATD-induced agranulocytosis was 10.4:1. The mean age (±standard deviation) of the patients with ATD-induced agranulocytosis was 41.7 ± 12.3 years. The methimazole and propylthiouracil doses given at the onset were 22.9 ± 8.0 mg/day and 253.6 ± 177.5 mg/day, respectively. ATD-induced agranulocytosis occurred in 45.1%, 74.3%, and 88.5% of patients within 4, 8, and 12 weeks of the onset of ATD therapy, respectively. Fever (78.9%) and sore throat (72.8%) were the most common symptoms when agranulocytosis was diagnosed. The mean recovery time of agranulocytosis was 13.41 ± 7.14 days. Recovery time in the granulocyte colony-stimulating factor (G-CSF)-treated group (12.7 ± 6.0 days) did not differ from that in the group not treated with G-CSF (16.4 ± 10.6 days; p = 0.144). Treatment with 131I was successful in 87/98 patients (88.8%). The success rate of 131I was equivalent (p = 1.000) between the groups receiving methimazole (88.2%, 75/85) and propylthiouracil (92.3%, 12/13).
Conclusions:
This largest single-institution study in China shows that ATD-induced agranulocytosis tends to occur within the first 12 weeks after the onset of ATD therapy. For patients with ATD-induced agranulocytosis, G-CSF does not improve the recovery time of agranulocytosis, and 131I is an optimal treatment approach.
Introduction
A
Previous studies have described the clinical characteristics of ATD-induced agranulocytosis, such as its occurrence in the early stages of ATD therapy and the fact that it is more common in elderly patients and in those taking high doses of ATDs (2,8,9,15 –17). However, there are few reports of large-sample studies of the clinical course of ATD-induced agranulocytosis, especially regarding treatment details, time to recovery from agranulocytosis, and outcomes of hyperthyroidism. The aims of this study were to review experience of ATD-induced agranulocytosis at the authors' hospital, which is a large referral center for 131I treatment in Zhejiang province, China, over the last 15 years, and to analyze the patients' clinical characteristics, treatments, and outcomes to improve understanding of this rare entity.
Materials and Methods
Study patients
The medical records of patients with hyperthyroidism who were referred for 131I treatment at the Department of Nuclear Medicine at Zhejiang University (a tertiary referral center) between January 2000 and February 2015 were retrospectively reviewed. The data obtained from a total of 9690 patients who were diagnosed with hyperthyroidism in the authors' department included age, sex, drug treatment, time to onset of agranulocytosis, dose of ATD at onset, relevant laboratory records, treatment details, time to recovery, and outcome.
Diagnostic criteria for ATD-induced agranulocytosis
The diagnosis of ATD-induced agranulocytosis was based on the following criteria (1). First, patients with hyperthyroidism confirmed by increased concentration of plasma thyroxine (T4) and/or triiodothyronine (T3) and by decreased concentration of thyrotropin (TSH), together with elevated 131I uptake and/or diffuse uptake of technetium-99m (4). Second, patients confirmed to have a granulocyte count of 1.5 × 109/L before taking ATDs. Third, documentation of a granulocyte count decrease to a level <0.5 × 109/L after initiation of ATD therapy, and a subsequent recovery from agranulocytosis after discontinuation of ATD treatment. Finally, patients with agranulocytosis attributable to other drugs or medical illnesses were excluded. We defined resolution of ATD-induced agranulocytosis as recovery of the granulocyte count to ≥1.0 × 109/L (6).
Methods and outcome assessment
Before 131I treatment, all patients had been afebrile without infectious disease for at least three days. ATD therapy was discontinued for at least three days or two weeks in patients taking MMI or PTU, respectively. A fixed or thyroid weight-adjusted single dose of 131I was given according to American Thyroid Association guidelines (11). 131I therapy was considered to have failed if the patient suffered from recurrent hyperthyroidism, as determined by elevated T3 and T4 levels and a decreased TSH. Successful treatment was defined as either hypothyroidism or euthyroidism at least six months after radioiodine treatment (18).
The study was approved by the hospital's Institutional Review Board. Written informed consent was obtained from all patients before the 131I treatment, and all patients were aware of the radiation safety precautions following treatment.
Statistical analysis
SPSS for Windows v16 (SPSS, Inc., Chicago, IL) was used for all statistical analyses. Descriptive quantitative data were expressed as the mean ±standard deviation; qualitative data were expressed as percentages. Significant differences between groups were ascertained by analysis of variance (for quantitative variables) and the chi-square test or Fisher's exact test when appropriate (for qualitative variables). Tests were two-sided, and a p-value of <0.05 was considered to represent statistical significance.
Results
General condition
Between January 2000 and February 2015, 9690 patients with hyperthyroidism who were referred for radioiodine treatment were retrospectively reviewed. Among these patients, 9343 were diagnosed with Graves' disease; toxic multinodular goiter and toxic adenoma were confirmed in 343 and 4 patients, respectively. Among these 9690 patients (6912 female; female:male ratio of 2.49), 123 patients were identified who had been diagnosed with agranulocytosis. An average of 7.6 patients per year was reported. The number of reports increased to >10 every year after 2008, which is likely to be due to an increase in the morbidity of hyperthyroidism and awareness among endocrinologists of ATD-induced granulocytosis as a potentially life-threatening adverse effect. Six of the 123 patients were excluded from this study because their agranulocytosis was not attributed to ATD therapy (one had severe acute viral hepatitis E, one had a hemophagocytic syndrome, and four had agranulocytosis before taking ATDs). Three patients were excluded because their clinical information regarding ATD-induced agranulocytosis was incomplete. Four patients with thrombocytopenia and anemia in addition to agranulocytosis were considered to have ATD-induced pancytopenia (one patient developed pancytopenia after taking PTU for four weeks; two patients and one patient developed pancytopenia after taking MMI for four weeks and five months, respectively). Thus, over 15 years, 114 cases of ATD-induced agranulocytosis were identified among 9690 patients. The incidence of ATD-induced agranulocytosis and pancytopenia was 1.2% and 0.04%, respectively.
Clinical characteristics of patients with ATD-induced agranulocytosis
The clinical characteristics of the 114 patients with ATD-induced agranulocytosis are shown in Table 1. Age, sex, WBC, and granulocyte counts before taking ATDs, and the time of onset of agranulocytosis did not differ between the MMI and PTU groups. Patients overall comprised 104 females and 10 males (female:male ratio of 10.4; the incidences of agranulocytosis were 1.50% and 0.36% in females and males, respectively). Their mean age was 41.7 ± 12.3 years (range 13–67 years). The incidences of agranulocytosis in the cohort of 9690 patients were 1.39% (n = 2), 1.24% (n = 20), 1.38% (n = 25), 1.38% (n = 36), 1.33% (n = 24), and 1.0% (n = 7) for individuals aged <20, in their 20s, in their 30s, in their 40s, in their 50s, and ≥60, respectively (Table 2).
Excluding one patient in whom the time between initiation of MMI therapy and onset of agranulocytosis was uncertain.
Including four-week cases.
Including four- and eight-week cases.
Interval between diagnosis of agranulocytosis and recovery.
Excluding three patients who did not undergo 131I treatment.
ATD, antithyroid drug; MMI, methimazole; PTU, propylthiouracil; SD, standard deviation; WBC, white blood cell.
Most patients (87.7%) were treated with MMI; 14 were treated with PTU. Four patients had resumed treatment with MMI for relapse of hyperthyroidism after discontinuation MMI. Thirteen patients had taken another ATD, and two were switched from MMI to PTU (one developed a cutaneous reactions after taking MMI for four weeks, and one relapsed after taking MMI for 14 years). Eleven patients were switched from PTU to MMI for the following reasons: eight relapsed after taking PTU for several years; one developed granulocytopenia after taking PTU for four weeks; one developed arthralgia after taking PTU for six weeks; and one developed PTU-induced liver injury within 11 weeks. The mean dose of PTU given at the onset of agranulocytosis was 253.6 ± 177.5 mg/day; the mean dose of MMI was 22.9 ± 8.0 mg/day. Seventy-nine patients (79%) were given MMI at a dose of ≥20 mg/day; only five (5%) were given 5 mg/day of MMI. The mean time to onset of agranulocytosis after initiation of ATD therapy was 7.9 ± 9.6 weeks (n = 113, excluding one patient in whom the interval was unclear). There was no difference in time to onset of agranulocytosis between the MMI and PTU groups (p = 0.383). ATD-induced agranulocytosis developed in 45.1%, 74.3%, and 88.5% of patients within 4, 8, and 12 weeks, respectively (Fig. 1). Thirteen patients developed agranulocytosis after 12 weeks, and 1.8% (n = 2) were reported to have developed agranulocytosis more than a year after starting ATD treatment.
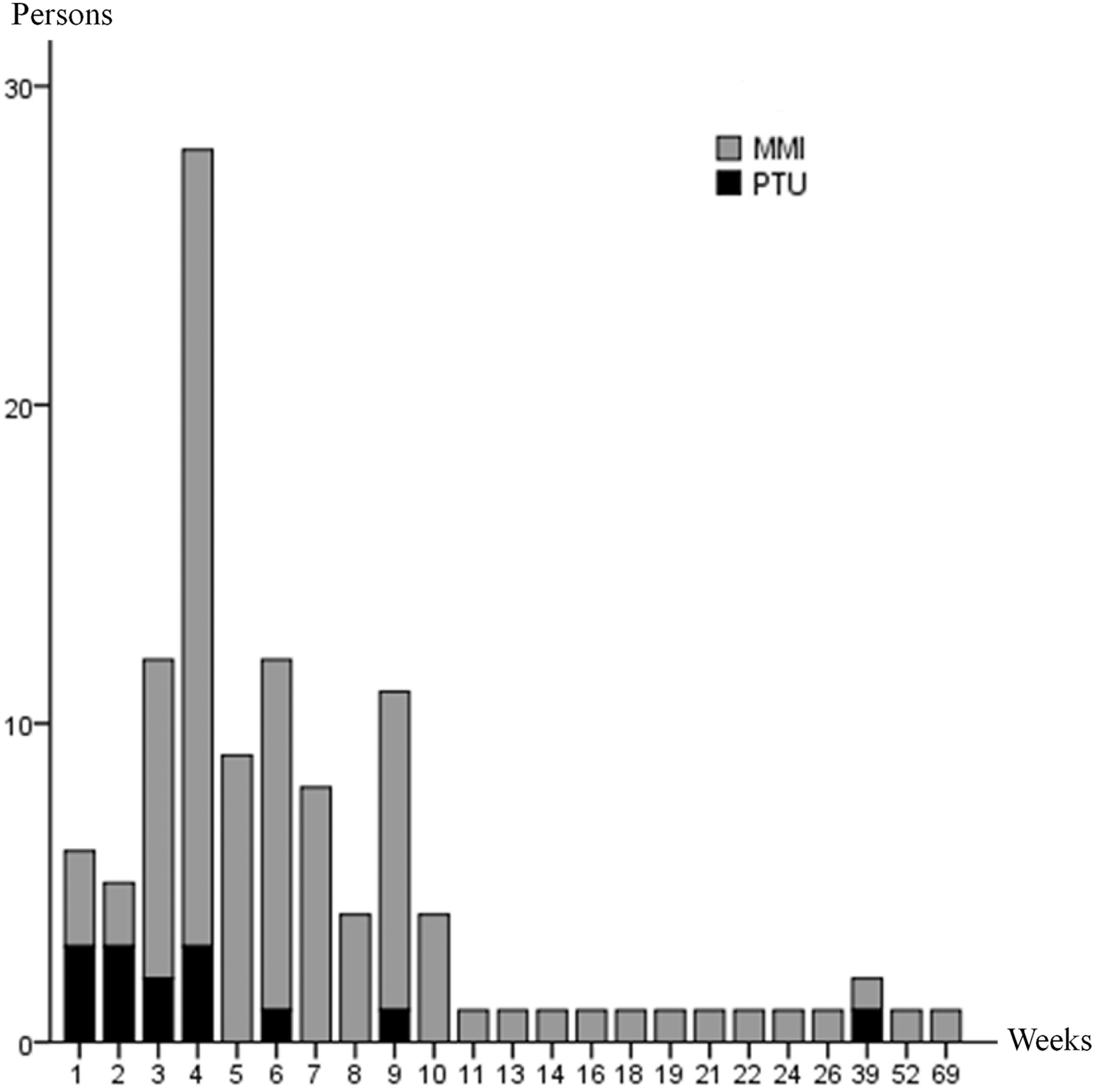
Time to onset of agranulocytosis after starting antithyroid drug (ATD) therapy in 114 patients. Agranulocytosis occurred in 45.1%, 74.3%, and 88.5% of patients after 4, 8, and 12 weeks of treatment, respectively. Thirteen patients developed agranulocytosis after 12 weeks. Two patients were recorded to have developed agranulocytosis more than a year after starting ATD treatment.
There was a trend toward lower WBC and granulocyte counts at the onset of agranulocytosis in patients taking MMI compared with patients taking PTU (WBC count 1.1 ± 0.7 vs. 1.9 ± 0.9, p = 0.001; granulocyte count 0.1 ± 0.2 vs. 0.2 ± 0.2, p = 0.037). Fever (78.9%) and sore throat (72.8%) were the most common symptoms when agranulocytosis was diagnosed, with no differences between the MMI and PTU groups (p = 0.168 and p = 0.523, respectively). Other infections occurred as follows: pneumonia in four cases (3.5%), skin infection in four cases (3.5%), gastrointestinal infection in two cases (1.6%), and gingivitis in one case (0.9%). Twenty patients (MMI group, n = 16; PTU group, n = 4) had no symptoms and were detected by routine WBC count monitoring. ATDs were stopped immediately in all patients who developed agranulocytosis. The mean time to recovery from agranulocytosis was 13.4 ± 7.1 days. Recovery time in patients given PTU or MMI was 12.1 ± 9.0 days (range 3–29 days) and 13.6 ± 6.9 days (range 2–44 days), respectively (p = 0.480). Recovery time in the G-CSF-treated group (n = 93, 12.7 ± 6.0 days; range 2–30 days) did not differ from that in the group not treated with G-CSF (n = 21, 16.4 ± 10.6 days; range 4–44 days; p = 0.144). In the G-CSF-treated and untreated groups, antibiotic therapy was given to 77.2% (71/92) and 14.3% (3/21) of patients, respectively (p = 0), while steroid therapy was given to 12.0% (11/92) and 14.3% (3/21), respectively (p = 0.722).
Therapy outcomes of patients with ATD-induced agranulocytosis
Once they had recovered from agranulocytosis and were afebrile, 111 patients were treated with 131I. Three patients were recommended for 131I therapy but chose to undergo another treatment (one patient switched from MMI to PTU and became euthyroid with a maintenance dose of PTU, one patient underwent subtotal thyroidectomy and developed hypothyroidism, and one patient was lost to follow-up). The mean time between recovery of the granulocyte count and 131I treatment was 15.5 days. The mean 131I dose was 281.0 ± 86.4 MBq (n = 111). Mean doses in the MMI and PTU groups were 284.8 ± 87.1 MBq and 255.0 ± 79.9 MBq, respectively (p = 0.231). Thus, there was no significant difference in dose between the two groups. Thirteen of the 111 patients who received 131I were lost to follow-up (Fig. 2). The median follow-up time was 19.5 months (range 6–104 months). The treatment success rate was 88.8% in the 98 patients who could be evaluated longitudinally. In the groups that received PTU or MMI, treatment success rates were 92.3% and 88.2%, respectively (p = 1.000). A second 131I treatment was administered to 10 patients who failed to respond (eight became hypothyroid, and two were euthyroid within the follow-up period). One patient received a third 131I treatment and had subclinical hyperthyroidism after two years of follow-up.
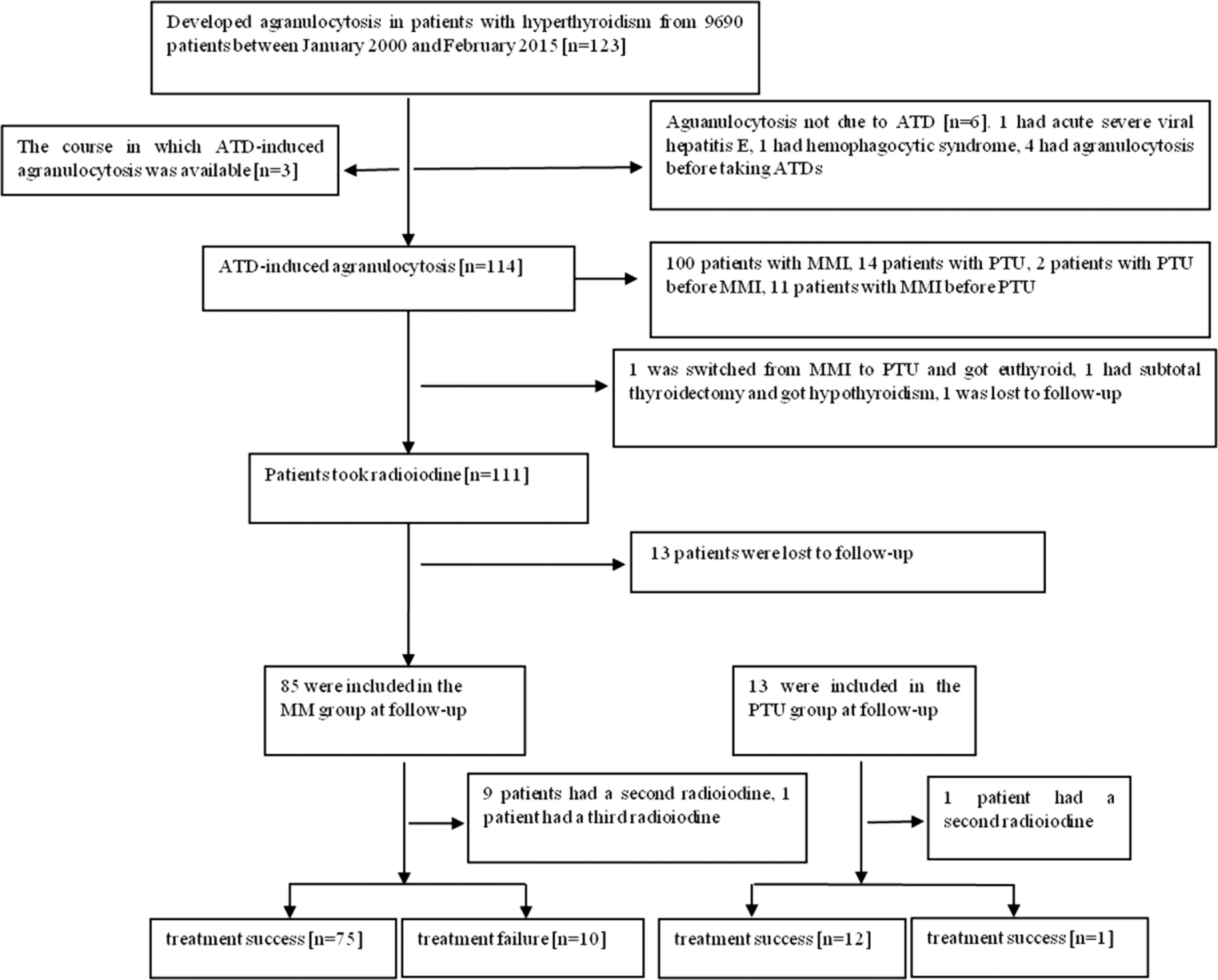
Flow chart and follow-up of study patients who developed agranulocytosis.
Discussion
This study evaluated the clinical features of ATD-induced agranulocytosis. Over a period of 15 years, 9690 patients were treated at the Department of Nuclear Medicine at Zhejiang University in China, and 117 of them developed agranulocytosis after taking ATDs. The incidence of ATD-induced agranulocytosis in this study (1.2%) was higher than that in previous reports in the literature in which the incidence was 0.1–0.4% (2,5,6,10,12,15), but is consistent with other reports (0.8–1.75%) (8,9). The discrepancies between studies may be explained by differences in study design. The current study found that ATD-induced agranulocytosis was more likely to occur in females than in males, which is in agreement with previous reports (2,15). In the present study, the incidences of agranulocytosis were 1.50% and 0.36% in females and males, respectively, suggesting a higher risk for women for developing agranulocytosis. The mean age of the 114 patients with ATD-induced agranulocytosis was 42 years, which was similar to the findings of previous studies (39–43 years) (2,10,15,19,20).
Agranulocytosis usually occurred within 12 weeks of the initiation of ATD therapy. The mean time to onset was 7.9 weeks; >70% of patients developed agranulocytosis within eight weeks and >88% within 12 weeks in this study, which is consistent with previous studies with smaller or larger numbers of patients (2 –9,20). Thirteen patients developed agranulocytosis after 12 weeks. Surveillance is necessary throughout the course of ATD therapy, especially when altering the dose or when patients are re-exposed to ATDs after a period of discontinuation. In the present study, the mean dose of PTU given at the onset of agranulocytosis was 253.6 ± 177.5 mg/day (14 patients; range 150–300 mg/day); the mean dose of MMI was 22.9 ± 8.0 mg/day (100 patients; range 5–40 mg/day). A previous study suggested that the side effects of MMI are dose related, whereas those of PTU are less clearly related to the dose of the drug (1). Some studies have suggested that the risk of agranulocytosis is greater in patients given higher drug doses (7 –9,17). In the present study, 79% of patients who developed agranulocytosis had been given ≥20 mg/day of MMI, which is in agreement with these reports. However, agranulocytosis developed in 5% of patients who were given only 5 mg/day MMI, suggesting that vigilance is also necessary at lower doses because agranulocytosis can occur irrespective of the dose (2,8).
Similar to other reports (19,20), patients with ATD-induced agranulocytosis typically presented with fever (78.9%) and sore throat (72.8%). Physicians should immediately discontinue the ATD and measure WBC and a differential blood count if fever or sore throat develops in a patient taking an ATD. Agranulocytosis is rare and develops rapidly, and some authors consider routine examinations to be worthless (3 –5). However, Tajiri et al. reported that 43/55 patients with ATD-induced agranulocytosis were asymptomatic at the time of diagnosis by routine monitoring of the WBC count (10). The present study also suggests that routine WBC count monitoring is useful in detecting ATD-induced agranulocytosis before symptoms appear.
The etiology of ATD-induced agranulocytosis is unclear but is thought to involve autoimmune activity and toxicity. Several studies have shown that targeting of an antigen on neutrophils, monocytes, and myeloid and erythroid progenitor cells is involved in the onset of agranulocytosis due to ATDs (21 –23). ATD toxicity is usually dose related, and toxic granules were found in the cytoplasm of myelogenous cells in a previous study (24). Destruction of granulocytes by ATDs usually takes a few weeks, but the immune-mediated mechanism proceeds rapidly. Both types of mechanism are thought to be present in the present cohort.
Severe infections occurred in 11 patients (9.6%), but all were successfully treated and there were no fatal cases. The prognosis of agranulocytosis has improved due to advances in early diagnosis and treatment (including G-CSF, antibiotics, and steroids) (12). In clinical practice, when a patient is diagnosed with agranulocytosis, broad-spectrum antibiotic therapy is given empirically, especially when the agranulocytosis is moderate or severe (3). In the present study, the preferential use of antibiotics in the G-CSF-treated group (72%) over the untreated group (14%) may imply that fewer moderate or severe cases were included in the untreated group. Fukata et al. reported that the recovery time in a G-CSF-treated group did not differ from that of an untreated group, even in patients with moderate or severe agranulocytosis (13). Although steroid treatment may affect recovery time for the treatment of ATD-induced agranulocytosis, as reported by Hamada et al. (25), there was no difference in the time required for granulocyte recovery between patients with and without steroid treatment (15.0 vs. 18.0 days) in another study (19). The limited data from the present study suggest that steroid treatment had no impact on the G-CSF-treated group (12.0%) and the untreated group (14.3%). Treatment of agranulocytosis with G-CSF seemed to shorten the time to recovery of granulocyte count from 16 to 13 days compared with treatment without G-CSF in the present large-sample study, but the difference was not significant. This finding is inconsistent with that of a retrospective study with a smaller patient sample (19) in which a significant difference was observed: time to recovery was 9.6 days in a G-CSF-treated group of five patients compared with 16.2 days in 11 untreated patients (p = 0.01). Fukata et al. reported a prospective study in which G-CSF-treated and untreated groups recovered in 6.9 days and 7.6 days, respectively (13). Andres et al. reported intervals of 10 days and 11.5 days, respectively (14). The discrepancies between these studies may be explained by differences in study design, sample size, dose of G-CSF, and criteria for recovery time. Further multicenter, randomized, controlled prospective studies with larger patient samples are needed to clarify the benefit of treatment with G-CSF.
Almost all of patients in the present study with ATD-induced agranulocytosis were treated with 131I; 90% of them became hypothyroid or euthyroid, which is consistent with the study by Alexander et al. (26), who reported treatment success rates for 131I of 80–90%. In the present study, one patient underwent subtotal thyroidectomy, and one patient switched from MMI to PTU because they refused to take 131I. Use of the alternative ATD is contraindicated in patients with ATD-induced agranulocytosis because cross-reactivity between PTU and MMI has been well-documented (3). In the present study, there were no fatal cases. This may be attributed to the fact that the study population included only those ATD-induced agranulocytosis patients who were referred for radioiodine treatment. There might have been other patients who died before being referred.
A limitation of the present study is that it was not systematic or prospective and was performed in a cohort from a single institution. The results may be subject to bias. Only patients referred for 131I treatment who developed agranulocytosis were included, which may explain why there were no fatal cases. In addition, some clinical information was incomplete, and the follow-time after 131I treatment was relatively short for some patients between July 2014 and July 2015. Nevertheless, this is a large study with data from a greater number of patients than has previously been studied. It confirms that ATD-induced agranulocytosis tends to occur within the first 12 weeks after starting ATD therapy and that G-CSF does not improve the time to recovery from agranulocytosis. These findings provide thought-provoking information that will be useful for further studies in this field.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (81471704), the Science, Technology Planning Project of Zhejiang Province (2013C33119), the Natural Science Foundation of Zhejiang Province, China (LY15180007), and the Health Bureau Project of Zhejiang Province, China (2013KYA069, 2015KYB153). We would like to thank Dr. Yi-li Yang and Dr. Hong-ye Fu for their contributions to the initial study performed on this cohort.
Author Disclosure Statement
No competing financial interests exist.