
Abstract
Background:
There is growing evidence that the external branch of the superior laryngeal nerve (eSLN) participates in thyroarytenoid (TA) contraction, but little data quantify its role in vocal cord adduction. Injury to the eSLN, such as in thyroid surgery, is difficult to diagnose and likely underappreciated. It is the authors' belief that eSLN injury contributes to aspiration by depriving its contribution to the laryngeal plexus. The goal of this study was to measure the glottic closing force (GCF) from eSLN stimulation in a porcine model.
Methods:
The recurrent laryngeal nerve (RLN) and eSLN were identified bilaterally in four porcine necks. Bilateral RLNs and eSLNs were stimulated simultaneously to obtain a control GCF using a pressure transducer placed in the glottis. Subsequently, bilateral eSLNs were stimulated and the GCF measured to quantify its percent contribution to the control value.
Results:
Stimulation of the RLNs and the eSLNs each led to TA muscle contraction and a measureable GCF in all four porcine necks. The control GCF was 1000.1 mmHg, while the eSLN mediated CGF was 800 mmHg. The percentage GCF attributable to the eSLN was thus 800/1000 = 80%.
Conclusions:
Reflex glottic closure is one of the most important mechanisms for the prevention of aspiration during deglutition. The biomechanical quantification of glottic closure can be shown as the GCF. This study has shown that the eSLN contributes in a significant way to the GCF in a porcine model, a finding that has not been quantified to the best of the authors' knowledge. Therefore, greater focus should be placed on preserving this nerve in thyroid surgery.
Introduction
T
Classically, the afferent arm of the GCR arc receives impulses from the mechanoreceptors and chemoreceptors in the laryngopharyngeal mucosa, which are sent through the ipsilateral internal branch of the superior laryngeal nerve (iSLN). The sensory afferent fibers from this nerve have their cell bodies in the nodose ganglion, and they first synapse at the ipsilateral nucleus tractus solitarius in the medulla of the brainstem. From here, the afferent signal projects to the ipsilateral and contralateral nuclei ambigui. The motor neurons of the nucleus ambiguus ultimately project through bilateral recurrent laryngeal nerves (RLN) that supply the thyroarytenoid (TA) muscles and other vocal cord adductors, leading to reflex vocal cord adduction and glottic closure (3). However, as knowledge of laryngeal neuroanatomy has evolved, several animal and human studies have shown the complexity of innervation of the GCR. In a morphologic study, but without neurophysiologic confirmation, Wu et al. demonstrated the human communicating nerve in 44% of 27 larynges, bridging the external branch of superior laryngeal nerve (eSLN) to RLN, potentially providing motor innervation to the ipsilateral thyroarytenoid (TA) muscle (4). Maranillo et al. studied 103 excised human larynges also demonstrating a connection between the eSLN and RLN in 85% of specimens overall (5). Laryngeal EMG has been used to confirm these anatomic findings and to quantify the contribution of the eSLN to intrinsic laryngeal muscles involved in the GCR. Björck et al. showed via EMG in the porcine model that the TA muscle has dual innervation from the RLN and eSLN, with the contribution from the latter quite high in certain cases (6). Despite the growing knowledge and evidence of a laryngeal motor plexus involving the eSLN (7 –9), the latter may still be one of the least understood nerves in the head and neck region. This may be due to the subtle laryngeal findings and variable clinical manifestations of isolated injury to the eSLN.
The prevalence of eSLN injury is unknown and often goes undiagnosed. This nerve has significant relevance surgically, as its rate of injury in thyroidectomy is reported to be as high as 58% (10). This is likely due to the close relationship between this nerve and the superior thyroid vessels. The most widely used classification for the surgical anatomy of the eSLN was proposed by Cernea et al. in which the most common variation is the type 1 nerve, which crosses the superior thyroid vessels >1 cm above the superior thyroid pole and is thus least prone to surgical injury (11). In types 2A and 2B, the nerve crosses <1 cm above the superior pole or below its upper border, respectively, and is thus more prone to injury. In contrast to the RLN, comparatively little has been written regarding the effects of eSLN paralysis. However, such patients are more likely to complain of vocal fatigue, decreased ability to raise vocal pitch, and increased effort to speak due to inactivation of the cricothyroid (CT) muscle to which eSLN provides primary motor innervation. Importantly, patients with superior laryngeal nerve injury from surgery also often complain of varying rates and degrees of unexplained dysphagia (12). While it is well known that injuries to the internal branch of the superior laryngeal nerve correlate with swallowing dysfunction and aspiration (3,13), eSLN related dysphagia is less well appreciated. It is the authors' belief that eSLN injury contributes to aspiration by depriving its contribution to the laryngeal plexus. This targeted study sought to measure the biomechanical effect, that is, the glottic closing force (GCF) generated from eSLN stimulation in a porcine model. Should this force constitute a significant contribution to the overall reflex sphincteric mechanism of the larynx, its surgical preservation as in thyroid surgery deserves reviewed attention.
Materials and Methods
Four Yorkshire pigs, each weighing approximately 40 kg, were used in our study. The pig larynx was selected because of its anatomic and physiologic similarities to the human larynx (14). An intramuscular injection of ketamine (2.2 mg/kg), dexmedetomidine (0.02 mg/kg), and tiletamine/zolazepam (4.4 mg/kg) was utilized for induction of anesthesia. Inhalational isoflurane was maintained at a level of 1.0 MAC (minimum alveolar concentration) throughout. No long-term muscle relaxants were used. A warming pad beneath each animal maintained core body temperature at 38°C. Using aseptic technique, a midline tracheotomy between the third and fourth tracheal rings was performed through which a 6 mm endotracheal tube was inserted for ventilation throughout the procedure. Bilateral RLNs were identified and carefully exposed along their course in the tracheoesophageal grooves. The eSLNs were exposed bilaterally along their course to the CT muscles. These nerves were typically of small caliber and easily injured by an uninitiated dissector. A pharyngotomy was then performed to visualize the vocal cords from above and to gain exposure of the TA muscles. The identity of the nerves of interest was confirmed by direct stimulation and observation of TA and CT muscle contraction, respectively. The eSLNs were sectioned 1 cm proximal to their insertion in the CT muscle, and the RLNs were sectioned 5 cm proximal to their insertion below the CT joint in preparation for electrostimulation of their distal segments. Bipolar 200 mΩ platinum-iridium stimulating electrodes were used to stimulate the nerves sequentially. Square-wave electrical stimuli of 0.1 ms duration were provided by a Nicolet EDX EMG machine (Natus, Pleasanton, CA) starting at 0.1 mA and increasing by 0.1 mA until maximal stimuli were achieved (above which further increase in stimulus amplitude caused no increase in amplitude of the muscle responses). The average stimulus intensity delivered to the target nerves was 1.5 mA. Adjacent muscles were carefully observed by the lead author in each dissection to ensure the absence of current spread and to isolate stimulation to target nerves. Thus, in stimulating the eSLN, positive confirmation was sought in each dissection by noting CT muscle twitch in the absence of adjacent strap muscle activity. This was a reproducible and reliable finding in each specimen. To measure the GCF, a catheter pressure transducer (SPC-330, Micro-Tip; Millar, Houston, TX) was placed with its pressure-sensitive tip positioned at the level of the mid-membranous vocal folds. This transducer was connected to a DC amplifier that displayed waveforms on an oscilloscope. Trials were repeated six times in each animal to ensure reproducibility. There were then two experimental protocols in each step. In step 1, bilateral RLNs and bilateral eSLNs were stimulated simultaneously to obtain a total control GCF. Simultaneous bilateral stimulation was technically possible with this Nicolet stimulator, as it allows for attachment of two stimulator probes. Each probe in turn is attached to two bipolar electrodes, thus allowing for stimulation of four nerves simultaneously. Stimulation characteristics are controlled by the operator, and include equalizing amplitudes delivered and setting lag time between probes to zero. In step 2, bilateral eSLNs were stimulated to obtain the GCF produced by eSLN alone, allowing calculation of the percentage GCF attributable to the eSLN. This study was performed in accordance with the PHS Policy on Humane Care and Use of Laboratory Animals, the NIH Guide for the Care and Use of Laboratory Animals, and the Animal Welfare Act (7U.S.C. et seq.); the animal use protocol was approved by the Institutional Animal Care and Use Committee (IACUC) of Yale University.
Results
Stimulation of the RLNs and the eSLNs each led to TA muscle contraction and a measureable GCF in all four porcine necks (Table 1). When bilateral RLNs and bilateral eSLNs were stimulated in step 1 (Fig. 1), the mean GCF was 1000.1 mmHg. When the eSLNs were stimulated bilaterally in step 2 (Fig. 2), the mean GCF obtained was 800 mmHg. The percentage GCF attributable to the eSLN was thus 800/1000 = 80%. Observation of adjacent pharyngeal and strap muscles again showed no current spread beyond the target nerves.
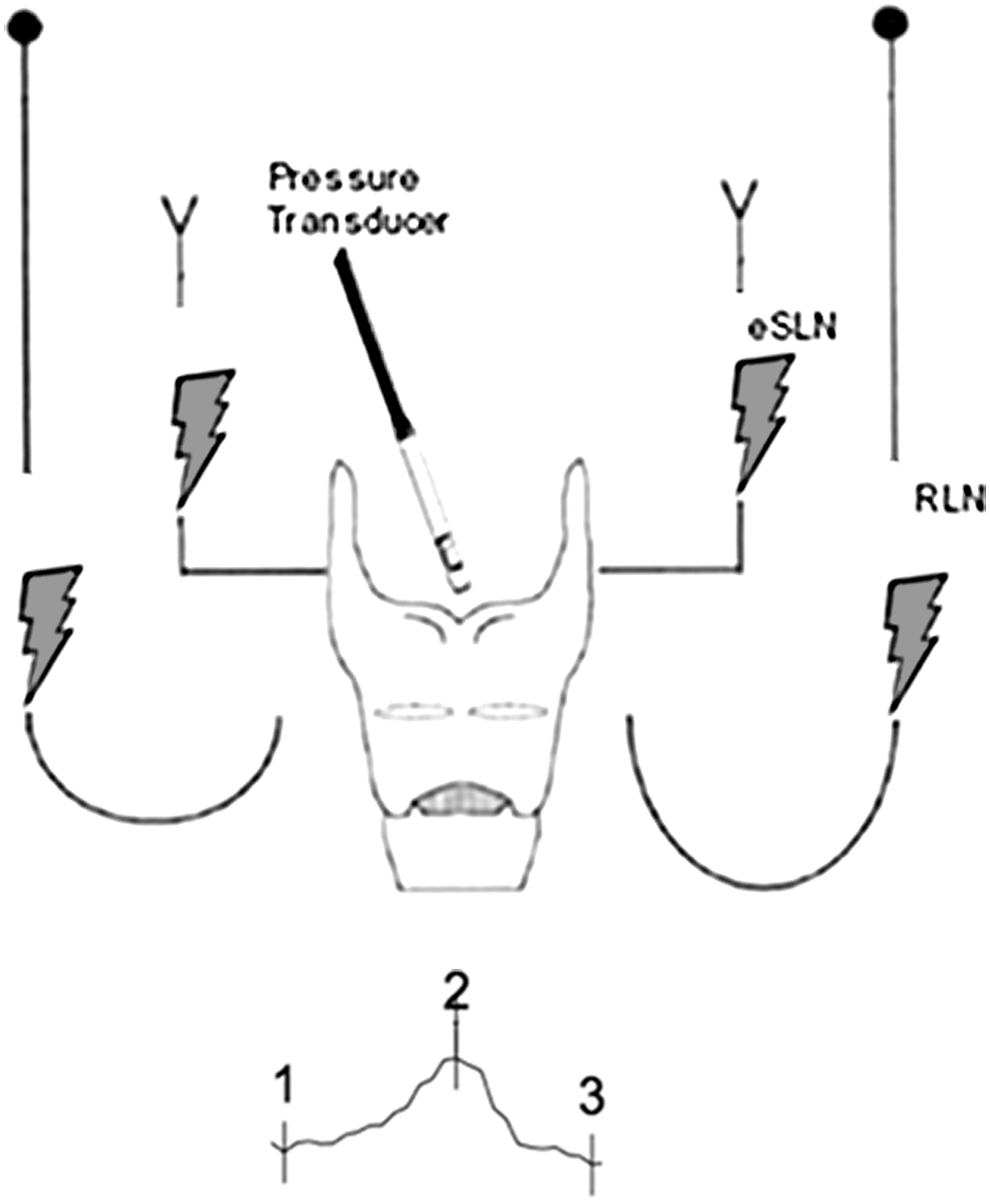
Stimulation of distal ends of bilateral recurrent laryngeal nerves (RLNs) and external branch of superior laryngeal nerve (eSLNs) to obtain control glottic closing force (GCF). Representative waveform obtained during measurement of control GCF from bilateral RLN and bilateral eSLN stimulation.

Stimulation of distal ends of bilateral eSLNs to obtain GCF. Representative waveform obtained during measurement of GCF from bilateral eSLN stimulation.
GCF, glottic closing force; RLN, recurrent laryngeal nerve; eSLN, external branch of superior laryngeal nerve; TA, thyroarytenoid muscle.
Discussion
In 1956, Andrew examined the EMG activity of various laryngeal muscles during swallowing in the rat model. In CT motoneurons, he found that the outflow of motor impulses ceased completely for 0.1–0.2 sec during a swallow. Activity then restarted at a greater level than before inhibition (15). These observations seemed to support the concept of a central pattern generator that activates various oral and pharyngeal muscles early in swallow, thus comprising a “leading complex” of muscles. Other muscles such as the CT are inhibited at the onset but are sequentially activated later during the swallow event. Such a patterned reflex exists not only to transit the food bolus properly but perhaps more importantly to protect the airway from aspiration.
There are two established clinical methods for intraoperative neural monitoring (IONM) of the eSLN. The first is by electrostimulation of the eSLN and observation of a twitch response of the CT muscle, present in all patients. The second is by stimulating eSLN and obtaining an electromyographic response via surface electrodes placed on the endotracheal tube. This finding occurs in 70–80% of patients (16). The latter phenomenon presumably relies on the innervation of the TA muscle by way of the communicating nerve from eSLN. Randomized controlled trials have shown that IONM can improve the identification rate of the eSLN during thyroidectomy (17).
The following reports measure EMG amplitudes from surface electrodes positioned on the endotracheal tube during thyroid surgery. Potenza et al. reported on normative data of EMG intraoperative nerve monitoring of the eSLN during 72 consecutive thyroid surgeries. An EMG response was noted in 80% of patients, and the glottic EMG amplitudes were around a third of those achieved by ipsilateral RLN stimulation (16). A later similar study showed that in 22 surgeries, the glottic EMG amplitude from eSLN stimulation was 26% of that from stimulating the RLN (18). Such studies provide further evidence of the potential role of the eSLN in reflex glottic closure.
Nevertheless, it could be argued that conclusions drawn from surface electrodes are inherently problematic due to the presence of confounding motion artifact, as well as undefined location of recording electrodes with respect to target muscles and the variable location or migration of the electrodes during the course of an operative procedure. Such factors may be especially important in the quantification of participating motor units by EMG amplitude discrimination and even more so in extrapolating their biomechanical effects in generating a GCF.
The experimental design confined stimulus presentation to the distal ends of sectioned eSLN and RLN to produce desired m-wave (motor) responses avoiding sensory involvement as would occur by generating evoked polysynaptic responses through brainstem nuclei. In so doing, the intention was to minimize even the smallest changes resulting from the influence of core body temperature, level of anesthesia, arterial pO2, and pCO2 on activated motor units. The design therefore solely captured the direct motor contributions of the eSLN and RLN separately or in combination in the production of measured GCF.
Altogether, there is growing appreciation of the role of the eSLN not only as motor nerve to the extrinsic CT muscle but also to intrinsic vocal cord adductors. In fact, the International Neural Monitoring Study Group released a guideline statement governing intraoperative neural monitoring (IONM) of this nerve to reflect the concern that eSLN injury is commonly underestimated, especially during thyroid surgery (19). The present study is an effort to address the contribution of eSLN in the biomechanical quantification of combined eSLN and RLN stimulation in the generation of total GCF. The current study demonstrates that the GCF attributable to the eSLN upon bilateral stimulation provides 80% of the total GCF in a porcine model. In conclusion, the contribution of eSLN is not trivial. Greater effort in preserving its function should be given to it during the conduct of head and neck surgery and during thyroid surgery specifically.
Footnotes
Acknowledgments
This project is supported in part by the Charles W. Ohse Endowment and the Virginia Alden Wright Fund.
Author Disclosure Statement
No competing financial interests exist.