
Abstract
Background:
Although ultrasonography (US) has an essential role in assessing the malignancy risk of thyroid nodules, a malignancy risk-stratification system has not been established. The purpose of this study was to develop a clinically feasible US risk-stratification system—the Thyroid Imaging Reporting and Data System (TIRADS)—primarily based on the solidity and echogenicity of thyroid nodules.
Methods:
From January 2010 to May 2011, a total of consecutive 2000 thyroid nodules (≥1 cm) with final diagnoses were enrolled from the database of low and high cancer volume institutions (1000 nodules from each institution). For the development of TIRADS, the type and predictive value of US predictors in the groups categorized by solidity and echogenicity were analyzed, and the US predictors were integrated and categorized according to the malignancy risk.
Results:
The suspicious US features of microcalcification, taller than wide shape, and spiculated/microlobulated margin were independently predictive of malignancy in the solid or hypoechoic nodule group (p < 0.001, respectively). Meanwhile, only microcalcification was independently predictive of malignancy in the partially cystic nodule group (p = 0.006), and microcalcification and spiculated/microlobulated margin were independently predictive of malignancy in the iso- and hyperechoic nodule group (p = 0.002 and p = 0.015, respectively). Although the presence of any suspicious US features had a high malignancy risk in the group of solid hypoechoic nodules, it had an intermediate malignancy risk in the group of partially cystic or iso- and hyperechoic nodules. The malignancy risk of thyroid nodules was stratified into five TIRADS categories by integrating the type and predictive values of US predictors based on solidity and echogenicity.
Conclusion:
The malignancy risk of thyroid nodules can be stratified by TIRADS according to US patterns by combining solidity, echogenicity, and suspicious US features. The proposed risk-stratification system based on solidity and echogenicity will be useful for risk stratification and management decision of thyroid nodules.
Introduction
U
The Thyroid Imaging Reporting and Data System (TIRADS) US malignancy risk-stratification system of thyroid nodules was initially introduced by Horvath et al. (6), and has been investigated for the quantitative estimation of the malignancy risk with scoring systems by categorization of US patterns (6 –8) or by calculating the number of suspicious US features and US risk scores (9 –11). Recent thyroid society guidelines (12 –15) suggest risk-stratification systems based on categorization of US patterns. Although US features are essential for predicting the malignancy risk of thyroid nodules, there is no standardized risk-stratification system.
Previous studies (8,16 –20) have suggested that US features predicting malignancy may differ according to the solidity and echogenicity of thyroid nodules. However, the type and predictive value of US predictors according to solidity and echogenicity are still controversial and may require further investigation. Although several guidelines (12 –14) have adopted this strategy for risk stratification and as a tool for selecting nodules for FNA, a US risk-stratification system that integrates solidity, echogenicity, and other US features has not been established.
The aim of this study was to develop a clinically applicable US risk-stratification system, TIRADS, primarily based on the solidity and echogenicity of thyroid nodules.
Materials and Methods
The Institutional Review Board approved this retrospective study, and the requirement to obtain informed consent was waived.
Study population
A total of 2000 consecutive thyroid nodules from 1802 patients (1387 women; M age = 51.2 ± 12.2 years) were enrolled in this study. Because the calculated malignancy risk of US features can be affected by the malignancy rate of the study population, patients were enrolled from low and high cancer volume institutions to estimate the malignancy risk. From January 2010 to May 2011, each of the 1000 nodules with final diagnoses were selected from a database of thyroid nodules (≥1 cm) of patients who underwent FNA or core needle biopsy (CNB) at low and high cancer volume institutions (two primary medical centers and two tertiary hospitals). Among 3256 consecutive nodules (≥1 cm) during the period of enrollment of a predetermined number of 2000 nodules with final diagnoses (1000 nodules from each low and high cancer volume institution), 1256 nodules were excluded because a final diagnosis was not obtained in 1242 nodules, and US characteristics could not be analyzed in 14 entirely calcified nodules (Fig. 1).

Flowchart of the study group. FNA, fine-needle aspiration; CNB, core needle biopsy.
Final diagnoses of malignant tumors and benign neoplasms were determined by surgical pathology, except for lymphomas. Final diagnoses of benign nodules were determined by (i) pathological results of surgical resections, (ii) benign cytology results of FNA or CNB that was repeated at least twice, (or iii) an initial benign result of FNA or CNB and decreased or stable nodule size at US follow-up >12 months. There was an overlap of data (616 thyroid nodules) that were included in a previous study (8).
US examination and image analysis
A high-resolution US scan using a 10–12 MHz or 5–14 MHz linear-array transducer (AplioXG, Toshiba, Otawarashi, Japan; iU22, Philips Medical Systems, Bothell, WA) was employed. US images were retrospectively reviewed by one of three experienced radiologists (D.G.N., J.H.B., and J.Y.S., who had 19, 16, and 12 years of experience in performing thyroid US and interventional procedures, respectively). All of the reviewers, who had no previous knowledge of the FNA result or final diagnosis, assessed the following US features of thyroid nodules based on a previous report (21): internal content, echogenicity, margin, shape, calcification, nodule vascularity, spongiform appearance, and comet-tail artifact. Internal content was categorized as solid (≤10% of the cystic portion), predominantly solid (>10% and ≤50% of the cystic portion), predominantly cystic (>50% and ≤90% of the cystic portion), and cystic (>90% of the cystic portion). Predominantly solid and predominantly cystic nodules were grouped into a single group of partially cystic nodules for the data analysis.
The nodule echogenicity was categorized as hypoechogenicity (marked or mild), isoechogenicity, and hyperechogenicity by the predominant echogenicity compared to the reference of normal thyroid tissue and anterior neck muscles. Spongiform appearance was defined as an isoechoic nodule with microcystic changes in >50% of the nodule volume. The comet-tail artifact was defined as an intracystic echogenic foci accompanied by reverberation artifacts. In partially cystic nodules, the configuration was categorized as concentric, eccentric with an acute angle, eccentric with a blunt angle, and unspecified patterns. Color Doppler US images were available in 1295 nodules, and the vascularity patterns were categorized as none, peripheral, central, and prominent central vascularity (>50% of a nodule).
US-guided FNA and CNB procedures
FNA was performed with a conventional method, and at least two samplings were performed for each nodule (22). CNB was performed using a disposable 18-gauge, single- or double-action spring-activated needle (TSK Acecut or Stericut; Create Medic, Yokohama, Japan), as described elsewhere (23). FNA was routinely performed for thyroid nodules >1 cm, with the exception of pure cystic nodules, partially cystic nodules with comet-tail artifacts, and spongiform nodules, which usually underwent FNA for therapeutic cyst aspiration or for ethanol or radiofrequency ablation therapy or when the nodule size was >2 cm (21). The interpretation of FNA was based on the Bethesda System for Reporting Thyroid Cytopathology (1), and CNB results were diagnosed with a six-tier pathology reporting system (23,24).
Data analysis and statistics
For the development of TIRADS, the type and predictive value of US predictors for malignancy in the groups categorized by solidity and echogenicity were determined. The chi-square test or Fisher's exact test were used for the delineation of US features significantly associated with malignancy. After univariate analysis, multivariable logistic regression analysis was performed to determine independent US predictors among US features that were statistically significant (p < 0.1). An independent two-sample t-test or chi-square test was used to compare the demographic data between low- and high-volume cancer data. The chi-square test or Fisher's exact test was used to compare the frequency of malignant tumors and malignancy risk of US features between low- and high-volume cancer data, and to compare the frequency of malignant tumors and malignancy risk of US features between each nodule group. Spearman's rank correlation test was used to assess the relationship between categories of TIRADS and FNA or CNB results. In the case of nondiagnostic results from the initial FNA, the results of repeated FNA or CNB were used for the correlation test. Statistical analysis was performed with SAS v9.2 (SAS Institute, Cary, NC) and R statistical software v3.1.0, and a significant difference was defined as a p-value of <0.05.
Results
Demographic data
The maximal size of nodules ranged from 10 to 100 mm (M = 20 ± 11.4 mm; median = 16 mm). The mean nodule size of low cancer volume data was slightly smaller than that of high cancer volume data (18.3 mm and 21.7 mm, respectively; p < 0.001). There was no significant difference in sex (p = 0.142), and the mean patient age was slightly older in low cancer volume data (p = 0.01).
Final diagnoses of 2000 nodules were 1546 (77.3%) benign nodules (1469 benign non-neoplastic nodules, 77 benign tumors) and 454 (22.7%) malignant nodules. Final diagnoses were determined by surgical resections in 239/1546 (15.5%) benign nodules, which included 149 nodular hyperplasias, 74 follicular adenomas, 13 cases of thyroiditis, and 3 other benign tumors. Final diagnoses of malignant tumors were diagnosed by surgical resection in 451 (99.3%) and by CNB in three (0.7%) cases of lymphomas. Of the 451 nodules that underwent surgery, there were 388 papillary thyroid carcinomas (PTC), including 43 follicular variant PTC, 48 follicular carcinomas, 7 medullar carcinomas, 2 lymphomas, and 6 other malignant tumors.
Frequency and risk of malignant tumors according to solidity and echogenicity
Table 1 demonstrates that the frequency and risk of malignant tumors were higher in solid nodules than they were in partially cystic nodules (p < 0.001) and were higher in hypoechoic (marked or mild) nodules than in iso- and hyperechoic nodules (p < 0.001). Although the malignancy risk of markedly and mildly hypoechoic nodules with any suspicious US features (microcalcification, taller than wide shape, spiculated/microlobulated margin) was very high (84.6% and 74.7%; p = 0.037), the malignancy risk of markedly and mildly hypoechoic nodules without suspicious US features was intermediate (44.1% and 21.9%; p < 0.001) in the group of solid hypoechoic nodules.
Numbers in parentheses are percentages.
Numbers in parentheses are number of thyroid nodules.
Type and predictive value of US predictors for malignancy according to solidity and echogenicity
Table 2 demonstrates that the suspicious US features of microcalcification, taller than wide shape, and spiculated/microlobulated margin were independently predictive of malignancy in the solid or hypoechoic nodule group (p < 0.001). Meanwhile, only microcalcification was independently predictive of malignancy in the partially cystic nodule group (p = 0.006), and microcalcification and spiculated/microlobulated margin were independently predictive of malignancy in the iso- and hyperechoic nodule group (p = 0.002 and p = 0.015, respectively).
US features associated with thyroid malignancy by univariate analysis.
Numbers in parentheses are percentages.
Chi-square test.
Numbers in square brackets are confidence intervals.
Binary logistic regression analysis.
Microcalcification, taller than wide shape, spiculated/microlobulated margin.
US, ultrasonography.
In the partially cystic nodule group, the predictive value of eccentric configuration with an acute angle for malignancy was intermediate (25%) and did not detect additional malignant tumors compared with microcalcification alone. The color Doppler US feature of central vascularity or prominent central vascularity was not significantly associated with malignancy in overall nodules and at each group according to solidity or echogenicity (p > 0.05; Table 2). However, prominent central vascularity showed a tendency of association with malignant tumors in the iso- and hyperechoic nodule group (p = 0.058). There was no malignant tumor in 28 partially cystic nodules with comet-tail artifacts and in 38 spongiform nodules.
Table 3 demonstrates US features associated with malignancy in overall nodules and each group by combining solidity and echogenicity. While three suspicious US features were independent predictors for malignancy in overall and solid hypoechoic nodules (p < 0.001), independent US predictors were microcalcification (p < 0.001) and spiculated/microlobulated margin (p = 0.036) in the partially cystic or iso- and hyperechoic nodule group. Subgroup analysis of partially cystic or iso- and hyperechoic nodules showed that independent US predictors were microcalcification and prominent central vascularity in solid iso- and hyperechoic nodules (p = 0.001 and p = 0.036, respectively), microcalcification in partially cystic hypoechoic nodules (p = 0.007), and none in the partially cystic iso- and hyperechoic nodules.
US features associated with thyroid malignancy by univariate analysis.
Numbers in parentheses are percentages.
Chi-square test.
Numbers in square brackets are confidence intervals.
Binary logistic regression analysis.
Although the presence of any suspicious US feature had a high malignancy risk in solid hypoechoic nodules (79.3%), it had an intermediate malignancy risk in the groups of partially cystic nodules, iso- and hyperechoic nodules, and partially cystic or iso- and hyperechoic nodules (23.8%, 19.6%, and 25%, respectively; Tables 2 and 4). Compared with the high malignancy risk of microcalcification in solid hypoechoic nodules, the malignancy risk of microcalcification was significantly lower in the partially cystic or iso- and hyperechoic nodule group (25.9%; p < 0.001) and in other nodule subgroups (partially cystic hypoechoic 52.4%, solid iso- and hyperechoic, 28.3%, and partially cystic iso- and hyperechoic 11.8%; p ≤ 0.005).
Microcalcification, taller than wide shape, spiculated/microlobulated margin.
Numbers in parentheses are number of thyroid nodules.
Chi-square test.
Although taller than wide shape was not an independent predictor for malignancy in each group of partially cystic or iso- and hyperechoic nodules, it was predictive of malignancy with a high positive predictive value (PPV) in the partially cystic nodule group by univariate analysis (p < 0.001; Table 2). The subgroup analysis showed that taller than wide shape was predictive of malignancy only in partially cystic hypoechoic nodules among partially cystic nodules by univariate analysis (p = 0.015) and was not significantly associated with malignancy in iso- and hyperechoic nodules (solid or partially cystic; p = 0.273). Meanwhile, the nodules with spiculated/microlobulated margin showed a high malignancy risk in each group of partially cystic and iso- and hyperechoic nodules (Table 2). However, the nodules with a spiculated/microlobulated margin or partially cystic nodules with taller than wide shape were only found in 11/1295 (0.8%) partially cystic or iso- and hyperechoic nodules.
Malignancy risk of suspicious US features in low and high cancer volume data
Table 4 demonstrates the malignancy risk of nodules with suspicious US features according to combination of solidity and echogenicity in low and high cancer volume data.
The prevalence of malignant tumors was 11.7% in low cancer volume data and 33.7% in high cancer volume data (p < 0.001). The frequency of hypoechoic nodules was significantly higher in high cancer volume data (53.3% vs. 25.9%; p < 0.001), but no significant difference was found in the frequency of solid nodules compared to low cancer volume data (p = 0.097). The malignancy risk of nodules with any three suspicious US features was significantly higher in high cancer volume data compared with low cancer volume data in the solid hypoechoic nodule group (84.9% vs. 60.9%; p < 0.001) and in the partially cystic or iso- and hyperechoic nodule group (41.7% vs. 14.5%; p = 0.001; Table 4).
US predictors for follicular carcinoma and follicular variant PTC
The proportion of follicular carcinoma and follicular variant PTC among malignant tumors was significantly higher in the partially cystic or iso- and hyperechoic nodule group than it was in the solid hypoechoic nodule group (39.8% vs. 13.1%; p < 0.001). While the independent US predictors for PTC including follicular variant were solid, hypoechogenicity, and three suspicious US features (microcalcification, taller than wide shape, and spiculated/microlobulated margin; p < 0.001), the independent US predictors for follicular carcinoma were solid (p = 0.018), hypoechogenicity (p = 0.002), and central vascularity (p = 0.043), and those for follicular variant PTC were only microcalcification (p = 0.001) by multivariable analysis. The sensitivity, specificity, PPV, negative predictive value (NPV), and accuracy of central vascularity for follicular carcinoma were 70.7%, 43.9%, 5.1%, 97.2%, and 45%, respectively. The frequency of any three suspicious US features found in overall PTC, follicular variant PTC, and follicular carcinoma was 64.4%, 25.6%, and 14.6%, respectively.
A proposal of TIRADS for risk stratification of malignancy based on solidity and echogenicity
The type and predictive value of US predictors were determined in each group according to solidity and echogenicity, and integrated for the creation of TIRADS. Although the US features of taller than wide shape and spiculated/microlobulated margin were less robust predictors for malignancy than microcalcification in the partially cystic or iso- and hyperechoic nodule group, these suspicious US features were included for US predictors in the partially cystic or iso- and hyperechoic nodule group, considering that these US features slightly increased sensitivity for malignancy with maintaining a similar PPV compared with microcalcification alone (Tables 3 and 4).
Therefore, the malignancy risk of thyroid nodules could be stratified into the simplified five categories of TIRADS according to US patterns by combining solidity, echogenicity, and suspicious US features (Table 5 and Figs. 2 –7). The suggested malignancy risk for each category was estimated by the range of calculated malignancy risk of low and high cancer volume data. With the criteria of TIRADS categories 4 and 5, the sensitivity, specificity, PPV, NPV, and accuracy for overall malignancy was 80.8%, 70.6%, 44.6%, 92.6%, and 72.9%, respectively, and with the criteria of TIRADS categories 4 and 5 and TIRADS 3 for nodules ≥1.5 cm, the values were 94.5%, 26.8%, 27.5%, 94.3%, and 42.2%, respectively. There was a significant correlation between categories of TIRADS and FNA or CNB results (R = 0.484; p < 0.001).
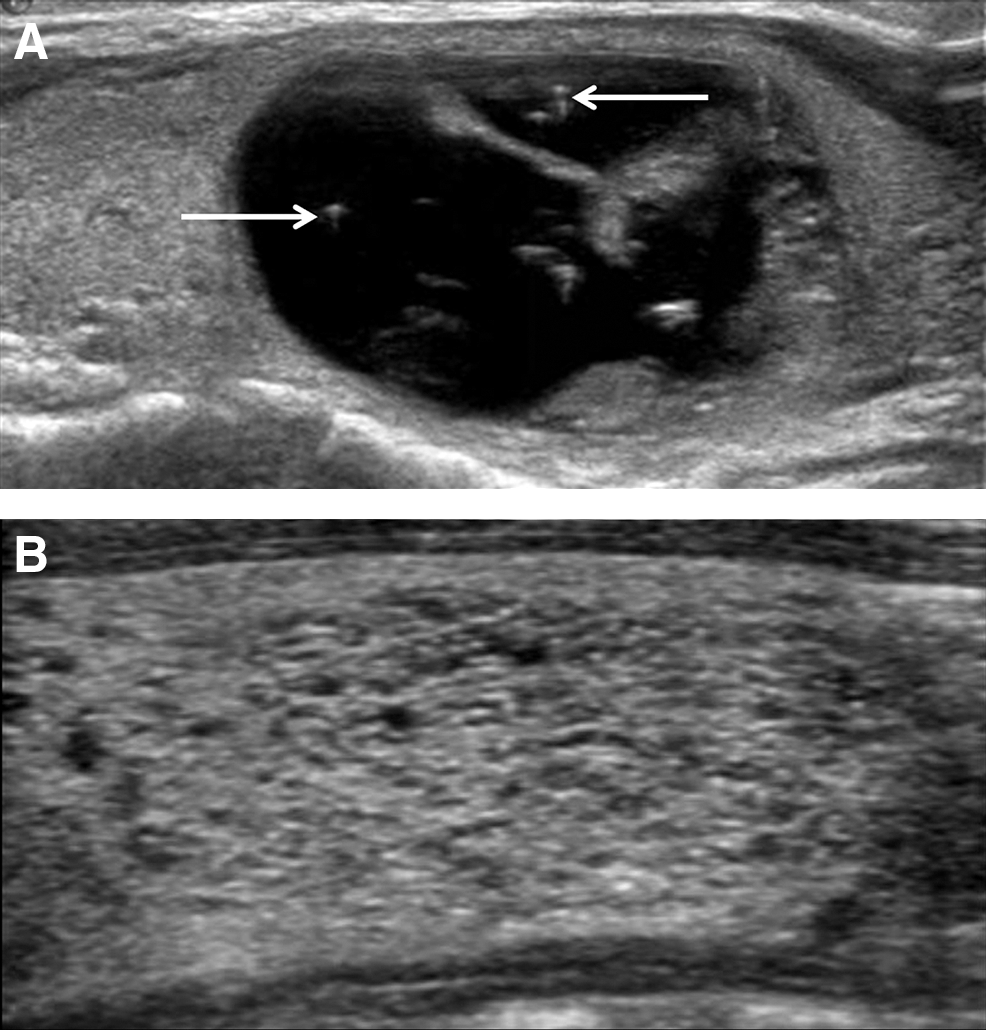
TIRADS 2 (benign) thyroid nodules. (
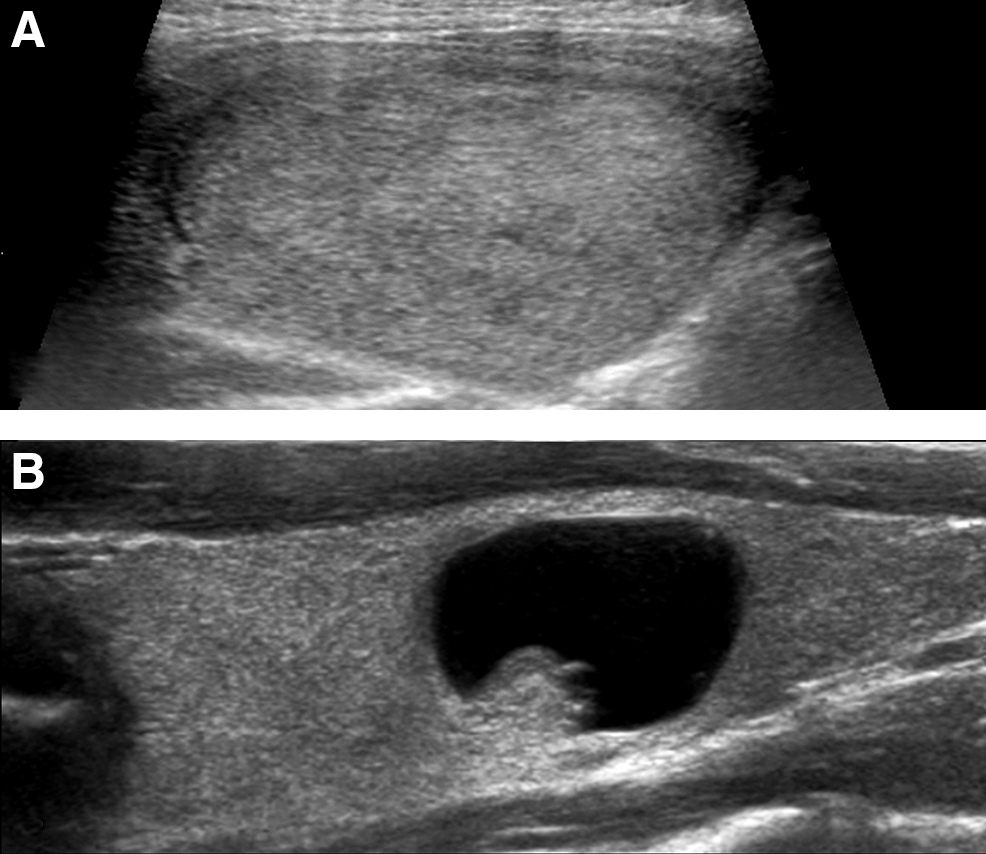
TIRADS 3 (low suspicion) thyroid nodules. (
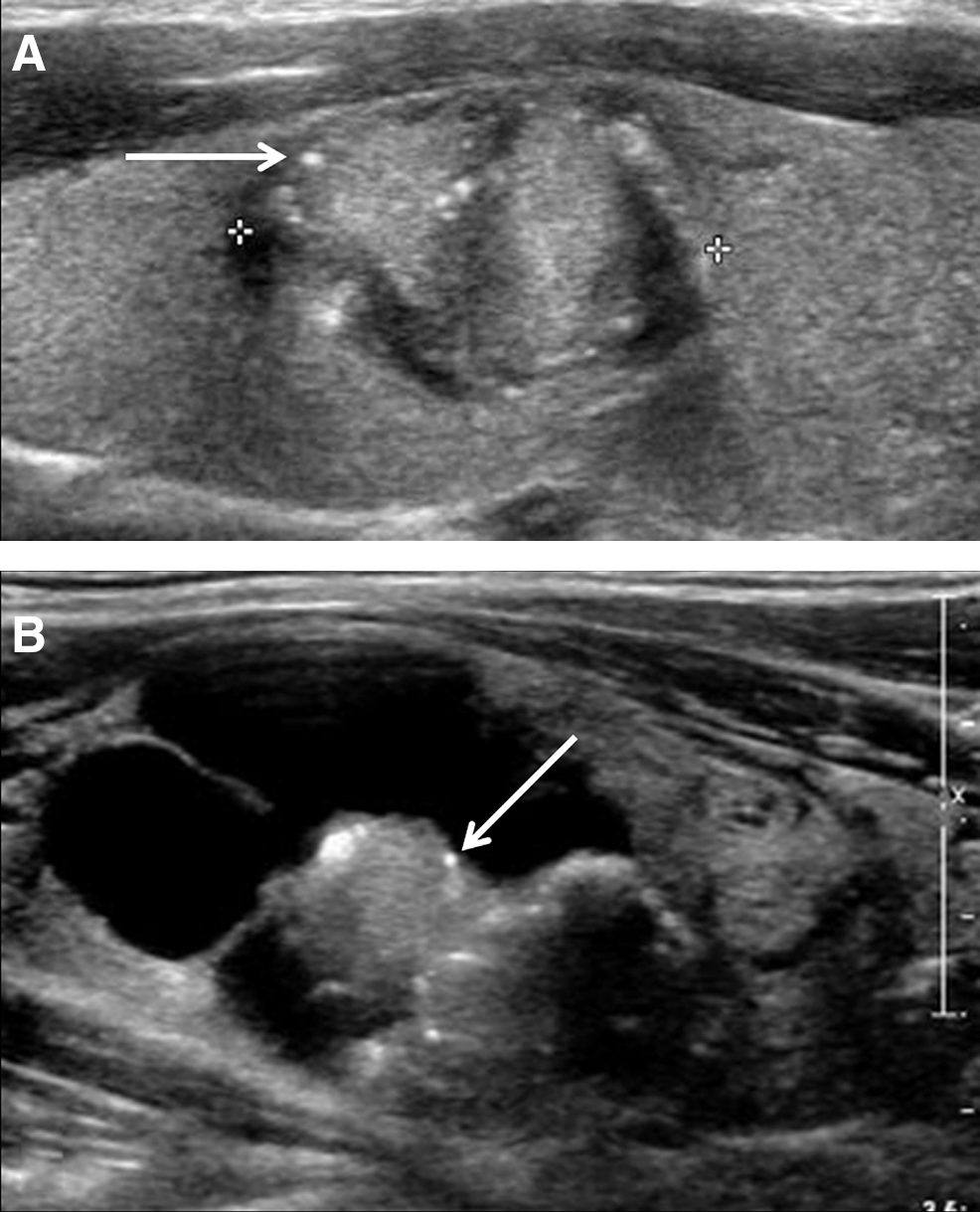
TIRADS 4 (intermediate suspicion) thyroid nodules. (

TIRADS 4 (intermediate suspicion) thyroid nodule. Solid hypoechoic nodule with smooth margin, ovoid shape, and no microcalcification.
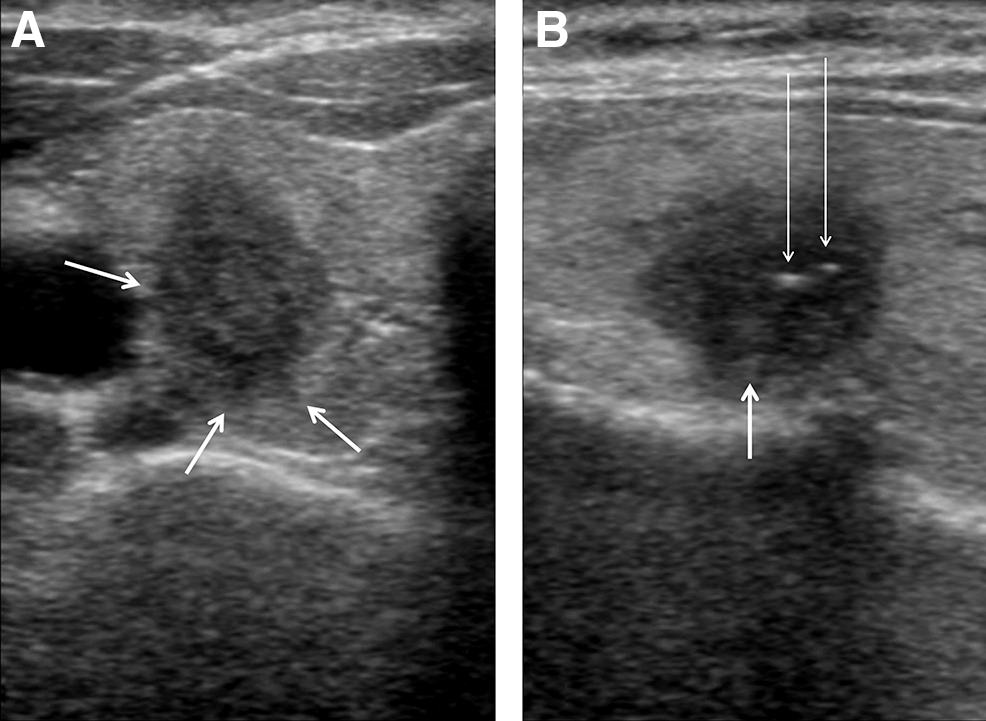
TIRADS 5 (high suspicion) thyroid nodule. Solid hypoechoic nodule with taller than wide shape (
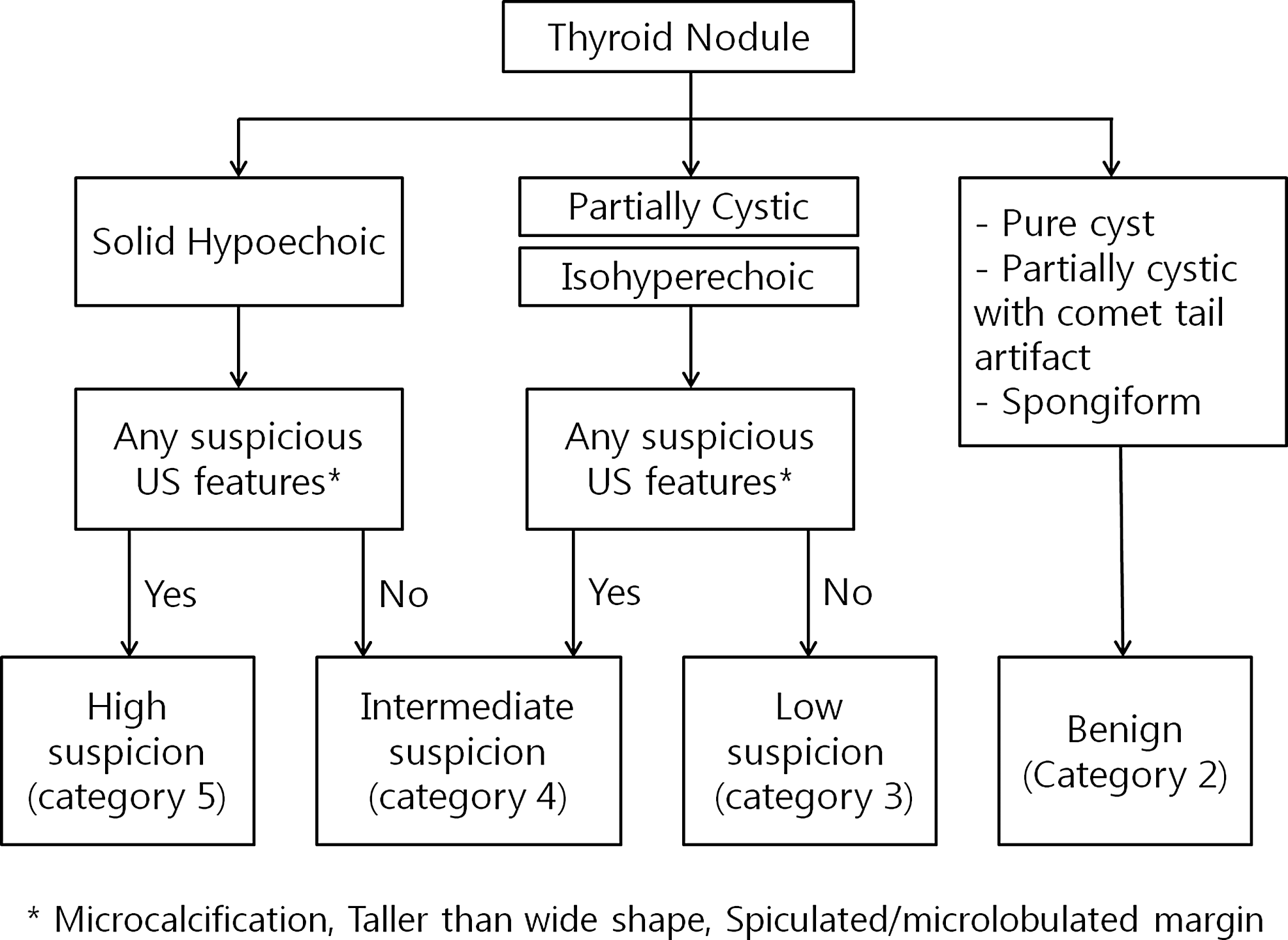
An algorithm of TIRADS for malignancy risk stratification based on solidity and echogenicity in thyroid nodules.
Solid hypoechoic nodules include solid nodules with marked or mild hypoechogenicity.
Microcalcification, taller than wide shape, spiculated/microlobulated margin.
Malignancy risk calculated from nodules excluding spongiform or partially cystic nodules with comet-tail artifacts.
LV, low-volume cancer data; HV, high-volume cancer data.
Discussion
The present data demonstrate that the type and predictive value of US predictors for malignancy were dependent on solidity and echogenicity of thyroid nodules. While suspicious US features of microcalcification, taller than wide shape, and spiculated/microlobulated margin were independent predictors for malignancy in solid hypoechoic nodules, only microcalcification was an independent predictor in partially cystic nodules and microcalcification and spiculated/microlobulated margin in iso- and hyperechoic nodules.
Partially cystic or iso- and hyperechoic nodules generally indicate benign nodules with a low malignancy risk (25). However, US features predictive of malignancy have not been established in these nodules (17 –20). Although the US feature of eccentric configuration with an acute angle was associated with malignancy in partially cystic nodules, it was less sensitive and had a similar PPV for malignancy compared with microcalcification (Table 2). The color Doppler US feature of central vascularity has been considered as a US predictor for malignancy (26,27) and one of the suspicious US features in several guidelines (14,28). However, the present data demonstrate that central vascularity was not significantly associated with malignancy in nodules in general and in each group of nodules. Although central vascularity may be useful for ruling out follicular carcinoma considering the high NPV, it is not a reliable predictor for ruling in malignancy in thyroid nodules in general. The data demonstrate that the malignancy risk of iso- and hyperechoic or partially cystic nodules are low to intermediate, regardless of US features in most cases.
The malignancy risk estimated by US is not determined by a single US predictor, but by a combination of coexisting US features of thyroid nodules, which is usually a combination of specific suspicious US features and less specific US features of solidity and echogenicity in thyroid nodules. The predictive value of a US predictor depends on the type and number of existing US predictors (7,8,10). The data also suggest that the predictability of suspicious US features has a heterogeneous dependency on solidity and echogenicity of nodules. Microcalcification had a high PPV (>60%) for malignancy only in solid hypoechoic nodules and taller than wide shape only in hypoechoic nodules (solid or partially cystic), and spiculated/microlobulated margin was highly predictive of malignancy, regardless of solidity or echogenicity of nodules. However, the frequency of partially cystic hypoechoic nodules with taller than wide shape and of partially cystic or iso- and hyperechoic nodules with spiculated/microlobulated margins was rare (<1%).
There are also several factors affecting the estimated malignancy risk determined by US, which include overall cancer volume, proportion of follicular carcinomas, applied US lexicons, and interpretation methods (real time or static). The lower malignancy risk of partially cystic or iso- and hyperechoic nodules showing any three suspicious US features may be explained by several factors. First, colloid material detected as echogenic foci within the solid portion of benign nodules can mimic microcalcification, and this effect will be more prominent in the group of partially cystic or iso- and hyperechoic nodules, which have a higher frequency of benign follicular nodules compared with the group of solid hypoechoic nodules. Second, nodules with a spiculated/microlobulated margin, which is a highly predictive US feature for malignancy, were rare among partially cystic or iso- and hyperechoic nodules. This may be caused by a higher proportion of follicular cancer and follicular variant PTC among malignant tumors, which have a lower frequency of suspicious US features compared with conventional PTC, have smooth margins in many cases, and frequently mimic US features of benign nodules (29 –31).
The indication for FNA can be stratified by the malignancy risk and the size of thyroid nodules. In patients without poor prognostic features, including suspected lymph node metastasis, extrathyroidal tumor extension, and distant metastasis, FNA should be routinely performed for TIRADS 4 or 5 nodules with a size ≥1 cm. For category 3 nodules, FNA may be performed if the nodule size is ≥1.5 cm, and FNA may be selectively performed only for spongiform nodules if the nodule size is >2 cm in category 2 nodules. Although 5.5% of malignant nodules, which are TIRADS 3 nodules <1.5 cm, are missed by the FNA criteria in this study, it seems reasonable to observe TIRADS 3 nodules <1.5 cm to reduce unnecessary FNA procedures, considering the low malignancy risk of TIRADS 3 nodules.
The sensitivity of TIRADS 4 and 5 categories for malignancy (80.8%) in this study was lower than those reported by Horvath et al. (6) and Russ et al. (7) (88% and 95.7%, respectively), and the PPV (44.6%) of TIRADS 4 and 5 was similar to the PPV (49%) by Hovath et al. (6) and higher than the PPV (9%) reported by Russ et al. (7). Compared with the TIRADS data reported by Russ et al. (7), which used similar US criteria for nodules categorized as TIRADS 4 or 5, the lower sensitivity of TIRADS 4 and 5 in the present study may be explained mainly by two factors. First, mixed echoic nodules without suspicious US features, which have predominantly isoechogenicity and partly hypoechogenicity, were categorized as TIRADS 3 in this study. However, those nodules were categorized as TIRADS 4A by Russ et al. (32). Therefore, some malignant tumors were not included in TIRADS 4 in the current study and may be the major cause for the lower sensitivity and relatively higher PPV compared with the TIRADS reported by Russ et al. Second, the proportion of follicular carcinomas among malignant tumors was higher in the present study compared with another study by Russ et al. (7) (10.6% vs. approximately 1.5%, respectively), which may be another causative factor for the lower sensitivity of the current TIRADS 4 and 5 criteria because many follicular carcinomas have no suspicious US features. Meanwhile, the recommended FNA criteria based on TIRADS and the nodule size showed a similar high sensitivity and higher PPV compared with TIRADS 4 and 5 criteria by Russ et al. (7).
Both low and high cancer volume data were included in the present study to minimize the effect by the difference of the data. In this study, high cancer volume data showed a higher malignancy risk of the same US predictor in hypoechoic nodules, which were more frequent in high cancer volume data. However, the calculated malignancy risk of US predictors at both low and high cancer volume data was within the range of suggested malignancy risk of each TIRADS category (Table 5). For the development of the TIRADS, the scoring system was selected by categorizing US patterns that are familiar and intuitive among physicians in clinical practice. An attempt was also made to simplify the risk-stratification system to enhance the feasibility for clinical practice.
There are several limitations to this study. First, selection bias may have existed because this study excluded some patients in whom a final diagnosis had not been obtained. Second, the retrospective assessment of static US images has an inevitable limitation to the accuracy of US interpretation, and a further prospective validation study using real-time US evaluation is required to establish the proposed risk-stratification system. Third, the proposed TIRADS has only been designed and tested on nodules ≥1 cm. Fourth, US elastography was not included, which might have a potential role for risk stratification (33,34). In conclusion, the malignancy risk of thyroid nodules could be stratified by integrating the type and predictive values of US predictors primarily based on solidity and echogenicity, and thyroid nodules could be categorized into five categories of TIRADS according to the malignancy risk by combination of solidity, echogenicity, and suspicious US features. The proposed risk-stratification system, TIRADS, will be useful for risk stratification and management decision of thyroid nodules.
Footnotes
Author Disclosure Statement
No competing financial interests exist.