
Abstract
Background:
There is little information regarding the natural history of subclinical hyperthyroidism (SH) due to Graves' disease (GD).
Methods:
A prospective analysis was conducted of patients with SH due to GD between 2007 and 2013 with at least 12 months of follow-up. SH was diagnosed if serum thyrotropin (TSH) was below the laboratory reference range (0.4–4.0 mIU/L) and when thyroid hormones were normal. GD was confirmed by either a raised TSH receptor antibody (TRAb) level or uniform uptake on Technetium scan.
Results:
Forty-four patients (89% female, 16% current smokers, and 5% with active Graves' orbitopathy) were diagnosed with SH due to GD. Over the follow-up period (median 32 months), approximately one third (34%) of the cohort progressed to overt hyperthyroidism, one third (34%) normalized their thyroid function, slightly less than one third (30%) remained in the SH state, while one person became hypothyroid. Multivariate regression analysis showed that older age and positive antithyroid peroxidase (TPO) antibody status had a positive association with risk of progression to overt hyperthyroidism, with hazard ratios of 1.06 ([confidence interval (CI) 1.02–1.10], p < 0.01) per year and 10.15 ([CI 1.83–56.23], p < 0.01), respectively, independent of other risk factors including, smoking, TRAb levels at diagnosis, and sex.
Conclusions:
A third each of patients with SH due to GD progress, normalize, or remain in the SH state. Older people and those with positive anti-TPO antibodies have a higher risk of progression of the disease. These novel data need to be verified and confirmed in larger cohorts and over longer periods of follow-up.
Introduction
S
A number of studies have reported on the natural course of SH (3,5 –10). The risk of progression to overt hyperthyroidism in SH patients has not been clearly defined. The risk of progression is higher in those with a greater degree of serum TSH suppression (3,5 –7), although this finding has not been seen in some other studies (8,9). In all these studies, the etiology of the SH has not been well defined, and this may play an important role in predicting the risk of progression of the disease (10,11).
One of the common causes of both overt and subclinical hyperthyroidism is Graves' disease (GD). GD is an autoimmune condition characterized by the production of antibodies that binds and activates the TSH receptor on the thyroid follicular cells (12). GD affects multiple organs either due to the autoimmune process (eyes and/or skin) or as a result of the accompanying hyperthyroidism (bones, heart, and liver, among others). The natural course of SH due to GD has not been studied in a systematic manner, and it is currently unknown what proportion of these patients progress to overt hyperthyroidism or revert to a euthyroid state. This study therefore analyzed the progress of SH patients with GD, and the findings are reported here.
Methods
Participants
Consecutive patients with sustained SH (on a minimum of two occasions at least three months apart) and no previous history of hyperthyroidism referred to a secondary care endocrinology clinic by their general (family) practitioners between August 2002 and December 2013 were evaluated, and the underlying cause of their thyroid dysfunction was assessed. All patients had thyroid function tests (TSH, free thyroxine [fT4], and free triiodothyronine [fT3]), thyroid peroxidase antibody (TPO), and TSH receptor antibody (TRAb), and also had a Technetium (Tc-99m) thyroid uptake scan. Patients with SH with raised TRAb levels (>1.0 IU/L) and/or having uniform uptake on their Tc-99m scans were classed as having GD and were followed up over a number of months. Individuals with raised TRAb levels but non-uniform uptake were still classed as having GD, as they probably had underlying nodular thyroid in addition to autoimmune GD. SH was graded as I (serum TSH 0.11–0.39 mIU/L) or II (serum TSH ≤0.1 mIU/L). Individuals on medication that could affect thyroid function such as levothyroxine, antithyroid drugs, amiodarone, or lithium were excluded. The presence of Graves' ophthalmopathy (GO) was assessed at presentation and at follow-up visits as per established criteria by experienced endocrinologists (13). Patients who completed at least 12 months of follow-up after presentation (if they remained SH or normalized their thyroid function) or those that progressed to overt hyperthyroidism or hypothyroidism were included in this analysis. For the first year, patients were assessed at 3, 6, and 12 months and then six monthly thereafter until the most recent thyroid function testing. SH was diagnosed on the basis of low TSH (<0.4 mIU/L) and with fT4 and fT3 concentrations within their respective reference.
Biochemical tests
Thyroid function tests, TRAb, and TPO antibodies were analyzed using the Roche Elecsys electrochemiluminescence immunoassay on the Cobas e602 analytical platform. The reference ranges were as follows: TSH (0.4–4.0 mIU/L), fT4 (10–25.0 pmol/L), fT3 (2.8–7.0 pmol/L), TPO (<50 IU/mL), and TRAb (<1.0 IU/L). The co-efficient of variation of all tests were <5%.
Technetium uptake scan
Anterior views of the thyroid were obtained using a gamma camera 20 minutes following injection of 100 MBq 99mTc pertechnetate.
Statistical analysis
For quantitative variables, results are expressed as mean ± standard deviation (SD) for normally distributed data and as median (range) for nonparametric data. Normal distribution of variables was tested by the Kolmogorov test. Categorical variables are described as percentages. For comparisons of means between two groups of patients, Student's t-test was used for normally distributed data. Data that were not normally distributed (TRAb) was log-transformed prior to analysis. A repeated-measures analysis of variance (ANOVA) corrected for multiple testing was used to compare more than two means. For ratio comparisons, the chi-square test or Fisher's exact test was used. Time from baseline to the development of hyperthyroidism was estimated by Kaplan–Meier curves, and survival curves were compared using the log-rank test. Univariate followed by multivariate Cox regression models were used to assess the independent effect of several quantitative and qualitative variables on the risk to progression to overt hyperthyroidism. From the univariate analysis, those variables that had p-values of <0.20 were included in the multivariable model. Two-sided tests were used, and differences were considered significant when p < 0.05. The statistical package IBM SPSS Statistics for Windows v21.0 (IBM Corp., Armonk, NY) was used to perform the statistical analyses.
Results
Baseline
The baseline characteristics of the cohort in relation to their subsequent progress are presented in Table 1. There were no differences in any of the characteristics between the groups at baseline, except that those that normalized thyroid function were younger and had lower fT4 concentrations at baseline. TSH levels were suppressed (<0.1 mIU/L) in the majority of patients, except for seven patients whose levels were between 0.1 and 0.39 mIU/L.
Data are presented as n (%), mean (± SD), or median (range).
One person whose data are not shown here developed overt hypothyroidism.
p < 0.05 as assessed with analysis of variance with post hoc Bonferroni correction.
SH, subclinical hyperthyroidism; OH, overt hyperthyroidism; fT4, free thyroxine; fT3, free triiodothyronine; TRAb, TSH receptor antibody; GO, Graves' orbitopathy; SH Grade II, TSH <0.1 mIU/L; Tc-99m, Technetium; SD, standard deviation.
Prior to referral to secondary care, two patients had been hypothyroid, requiring levothyroxine replacement therapy that had been reduced over a period of months and then discontinued completely; five patients had normal serum TSH levels in the preceding time period; 10 patients had SH on the very first thyroid function sample they ever had checked; three patients had mild overt hyperthyroidism prior to being referred (were not treated by general practitioners but had levels that improved to be in the SH category when assessed in clinic); two patients had mild subclinical hypothyroidism previously that was being monitored; and five patients had SH for varying time periods (ranging from 12 to 60 months). The remaining 16 patients had not had any previous thyroid function testing.
Follow-up
Overall, the median follow-up period was 32 months (range 2–111 months). However, the individual groups with varying outcomes had differing follow-up time periods. Over the median follow-up period of 13 months (range 2–77 months), 15/44 (34.1%) of patients with SH progressed to overt hyperthyroidism. In this group that progressed to overt hyperthyroidism, the mean ± SD) levels of fT4 and fT3 at progression were 29.5 ± 8.5 and 9.6 ± 3.2 pmol/L, and the median TRAb concentrations were 4.1 IU/L (range 1.1–33.2 IU/L). In relation to baseline values, fT4 and fT3 levels at progression were significantly higher (p < 0.001), and TRAb also tended to be higher than baseline, although it did not achieve statistical significance (p = 0.08).
Similarly, over 43 months (range 12–111 months) of follow-up, 5/44 (34.1%) of SH patients normalized their thyroid function. At normalization, the median TSH was 0.9 mIU/L (range 0.56–2.52 mIU/L), mean ± SD fT4 and fT3 were 14.5 and 4.5 pmol/L, respectively, and the median TRAb concentration was 6.2 IU/L (range 0.6–23.2 IU/L). Compared with baseline, TSH levels were significantly higher (p < 0.001) and fT4 and fT3 concentrations lower (p < 0.01). Interestingly, in only 1/15 patients, the TRAb levels had reduced to <1.0 IU/L. Overall, however, the levels were unchanged (p > 0.05) comparing baseline to normalization.
Over 19 months (range 12–42 months), of the patients who remained in SH state (29.5%), fT4, fT3, and TRAb levels were lower at their most recent thyroid function assessment compared to baseline, although only the reduction in the fT4 values reached statistical significance (20.4 to 17.4 pmol/L; p = 0.001).
One patient progressed to overt hypothyroidism with symptoms of weight gain, tiredness, and cold intolerance, and required replacement therapy with levothyroxine. She did not receive treatment with antithyroid drugs during the period of initial SH. Her TSH, fT4, fT3, and TRAb levels at baseline were 0.03 mIU/L, 17.9 pmol/L, 5.0 pmol/L, and 4.6 IU/L, respectively; six months later, her tests showed that the same parameters were 65.0 mIU/L, 5.8 pmol/L, 3.1 pmol/L, and 2.97 IU/L, respectively.
Univariate Cox regression analysis showed that TPO status was the only variable that had a significant relationship with progression to overt hyperthyroidism, whereas age, grade of SH, and family history had p-values between 0.05 and 0.20. However, multivariate analysis confirmed that TPO status (Fig. 1) and age were the only significant predictors of progression to overt hyperthyroidism: for positive TPO status, the hazard ratio (HR) was 10.15 ([confidence interval (CI) 1.83– 56.23], p < 0.01), and for each increase in age by a year, the increase in HR was 1.06 ([CI 1.02–1.10], p < 0.01; Table 2).
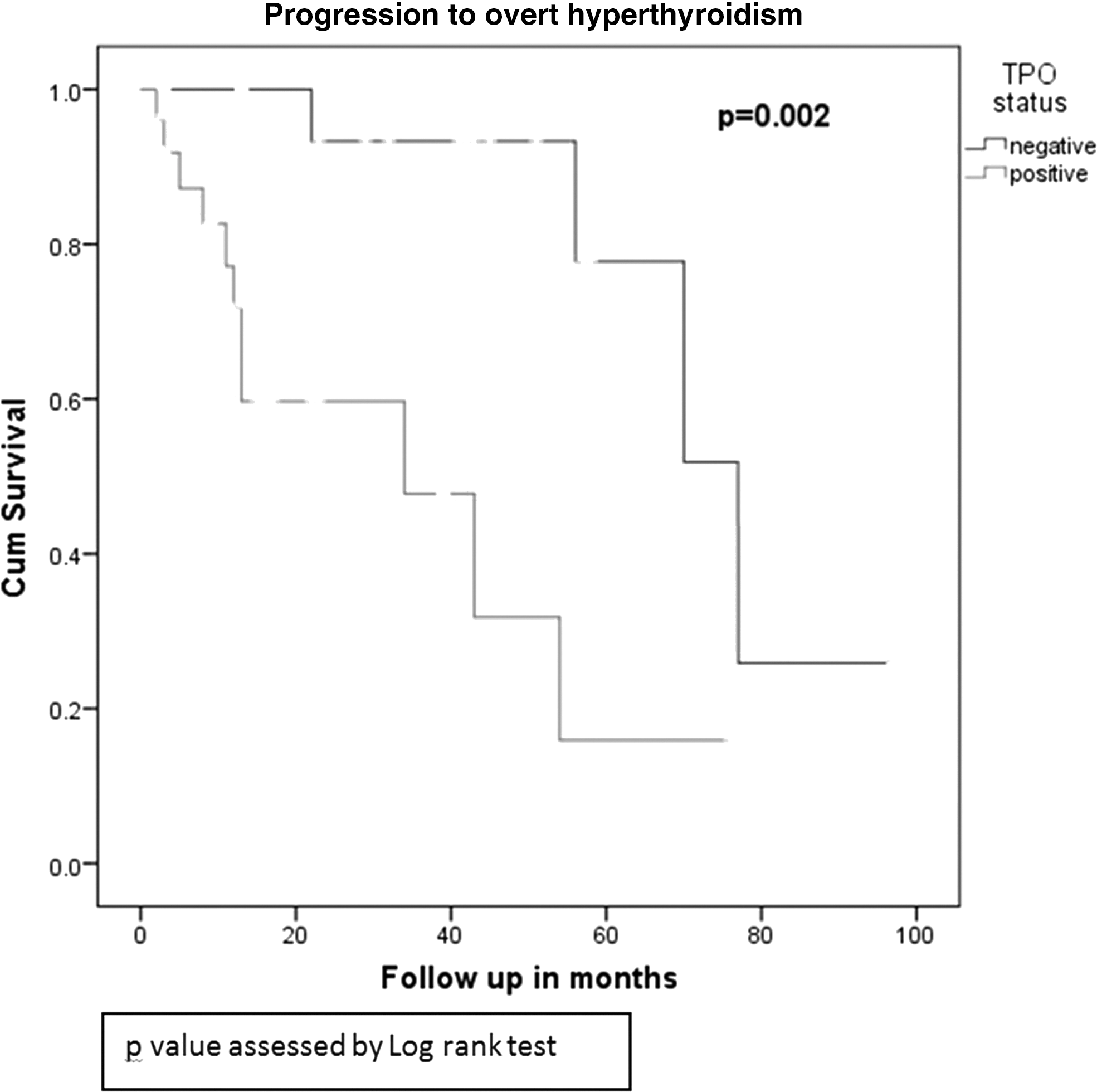
Progression to overt hyperthyroidism in relation to thyroid peroxidase antibody status at baseline (Kaplan–Meier curve).
HR of 1.0 is the reference value.
Only variables that had p < 0.20 on univariate analysis were included in the multivariate regression equation.
Log transformed.
CI, confidence interval; TPO, thyroid peroxidase.
Discussion
SH is relatively common, and GD is one of the frequent underlying causes. It is currently unclear what the natural course of this condition is. The results of the present study suggest that patients with SH due to GD have varying outcomes that range from reverting to euthyroidism, remaining in the SH state, or progressing to overt hyperthyroidism—roughly following a rule of thirds for each of the three outcomes. The significant predictors of risk of progression to overt hyperthyroidism are older age (4% increase for each year) and positive TPO antibody status (tenfold higher risk).
It is estimated that 5–13% of patients with SH have GD as the underlying cause (6 –11). There have been a number of studies that have suggested that SH is associated with adverse outcomes in relation to fractures, atrial fibrillation, or cardiovascular mortality (14). However, most of these longitudinal studies have utilized one index thyroid blood test to classify participants. Thus, it is likely that some of these patients may have normalized their thyroid function subsequently, as it may be related to non-thyroidal illness. Furthermore, these studies have not investigated the etiology underlying the SH. The results of the present study suggest that at least one third of patients with SH due to GD normalize their thyroid function, and there is a tendency toward lower fT4 concentrations in the group that remain in the SH state. This suggests that outcomes may vary depending on the underlying etiology of the SH and that this needs to be taken into account.
Several studies have reported on the natural course of SH generally. These studies either have not differentiated the underlying cause of SH or included a small number of patients with GD alongside those with multinodular goiter and performed mostly retrospective analysis (5 –11). The study by Diez and Iglesias included a small number of patients with GD, and no relationship between GD and risk of progression was seen (5). Das et al. retrospectively analyzed 323 SH patients, of whom 18 had underlying GD, and found that the only significant predictor of progression was the degree of TSH suppression at baseline (6). The retrospective study by Abdul Shakoor et al. showed that GD was present in 15/113 patients studied, and that no single factor predicted risk of progression (36 months of follow-up) (8). Another retrospective study by Poola et al. classed patients as having nodular or non-nodular thyroid disease, as not all patients were characterized by TRAb status (9). The study by Woeber examined 16 patients with SH (of whom seven were due to underlying GD) in a retrospective fashion and up to a maximum of 36 months duration (10). This showed that five patients with SH due to GD normalized thyroid function while one each progressed or remained in SH state. In this study, only 4% of patients with SH with a normal or diffusely enlarged thyroid required treatment (median follow-up of 3.2 years). In the two prospective studies reported by Rosario, progression of SH was seen in 7% of patients >65 years of age, although separate figures for GD are not reported (7), and in the second study of patients with SH <65 years of age, 6/15 patients (40%) with underlying GD progressed to overt hyperthyroidism (15). In the study by Schouten et al., the progression to overt hyperthyroidism was 9% over five years in 12 patients with SH due to GD (as determined by uniform pertechnetate scan) (11).
This study has revealed several interesting new findings. First, contrary to expectations, TRAb levels at baseline did not predict outcome. TRAb can be of two different types depending on its interaction with the TSH receptor: stimulatory or blocking. The stimulatory TRAb leads to hyperthyroidism, whereas the blocking antibody leads to hypothyroidism (16). In the present study, TRAb was measured by the inhibition of the TSH receptor binding immunoglobulin (TBII), which does not indicate whether the underlying action of the antibody is stimulatory or blocking. It is likely that a proportion of TRAb antibodies switched from one type to the other during the course of the follow-up period. This is evidenced by the fact that the SH group that reverted to euthyroidism had similar TRAb levels at baseline as at the point of subsequent euthyroidism. Similarly, the one patient who became hypothyroid had slightly lower TRAb levels subsequently (although still higher than the reference range). Second, a higher age seems to be a predictor for progression to overt hyperthyroidism in SH patients due to GD. Advancing age is associated with a higher risk of raised TPO antibody levels (17), but the two factors are independently associated with a greater risk of progression to overt hyperthyroidism in the current study. In a prospective study in Amsterdam by Strieder et al., investigating risk factors for the development of overt thyroid disease in female first- or second-degree healthy relatives of patients with autoimmune thyroid disease older age did not show a significant trend with the development of overt thyroid disease (p = 0.16), but the number of individuals >60 years was low (18). Third, patients with positive TPO antibody status also have a tenfold higher risk of progression to overt hyperthyroidism. In the above-mentioned study by Strieder et al., TPO antibody levels were significant predictors of development of overt autoimmune thyroid disease in a dose-dependent fashion (18).
This prospective clinical study of the natural course of SH in patients with underlying GD has several strengths. As far as the authors are aware, this is the first study that has investigated the course of SH due to GD exclusively. Furthermore, patients in this study have been studied in a systematic prospective manner at regular intervals and with thyroid hormone and immunology assessment for a longer period of time.
This observational study has limitations too. A modest number of patients were studied, and of course these data need to be confirmed in larger cohorts and for a longer time period. In addition, risks of complications on end organs such as the heart and bone have not been assessed. Therefore, it is unknown whether these risks differ in the groups with the varying outcomes. This study measured TRAb levels but did not ascertain whether these antibodies were stimulatory or blocking in nature—although levels of serum TSH and thyroid hormones provide a useful clue. Finally, it is possible that the small number of patients with negative TRAb levels at baseline (n = 2) could have had autoimmune thyroiditis rather than GD. However, this is unlikely to be the case, as Tc uptake scans were performed at baseline when the patients still had SH. Moreover, one patient (who became euthyroid) had a subsequently raised TRAb level after 103 months, whereas the other person remains SH and with negative TRAb and TPO antibody status at 32 months.
In conclusion, this study shows that individuals with SH due to underlying GD can have varying outcomes that roughly follow a rule of thirds: normalize, remain in the SH state, or progress to overt hyperthyroidism. Older individuals and those with positive TPO antibody status are more likely to progress to overt hyperthyroidism, and initial TRAb levels or tobacco smoking habits do not influence outcomes.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.