
Abstract
Background:
The role of telomerase reverse transcriptase (TERT) promoter mutations in differentiated thyroid cancer has been well established. These mutations have a significantly higher prevalence in aggressive thyroid tumors, including widely invasive oncocytic carcinomas, poorly differentiated carcinomas, and anaplastic thyroid carcinomas. Interestingly, in some studies, TERT mutations were found to be more common in tumors with a BRAFV600E mutation. However, mutational analysis of TERT promoter mutations in thyroid tumors has not been previously performed for patients in Korea, where the BRAFV600E mutation in papillary thyroid carcinoma (PTC) is particularly prevalent. This study analyzed TERT promoter mutations in various thyroid tumors and examined their relationship with clinicopathologic factors and the BRAFV600E mutation in PTC cases.
Methods:
Using 242 preoperative fine-needle aspiration biopsy specimens (including 207 PTCs) with confirmed histopathological diagnosis of the biopsied thyroid nodules, the TERT promoter status (C228T and C250T) was analyzed, and the relationship with clinicopathologic factors and the BRAFV600E mutation in PTC cases was examined.
Results:
Of 242 patients, 14.5% (30/207), 26.7% (4/15), 50% (1/2), and 60% (2/5) of PTCs, follicular thyroid carcinomas, poorly differentiated carcinomas, and anaplastic thyroid carcinomas harbored a TERTC228T mutation, respectively. The TERTC228T mutation was associated with recurrence (p = 0.03). However, no association with other clinicopathologic factors in PTC was found. Coexistence of TERTC228T and BRAFV600E mutations was found in 13.0% of PTCs and was significantly associated with older age and advanced stage compared with the group negative for either mutation. The TERTC228T mutation status was an independent prognostic factor for recurrence-free survival (hazard ratio = 3.08 [confidence interval 1.042–9.079]; p = 0.042) in patients with PTC in multivariate analysis.
Conclusions:
Identification of TERT promoter mutations in preoperative fine-needle aspiration biopsy specimens may help in better characterizing the prognosis and triaging thyroid cancer patients for appropriate treatment.
Introduction
T
Thyroid cancer, like other human cancers, is genetically driven, and over the last several years, significant progress has been made in understanding underlying genetic mechanisms. The activating point mutation BRAFV600E is the most common genetic alteration in PTCs and is present in approximately 29–77% of PTC cases (12 –14). The prevalence of the BRAFV600E mutation in PTC is much higher in Korea (73–87%) than it is in Western countries (15 –17). Therefore, mutational analysis for the BRAFV600E mutation in preoperative fine-needle aspiration biopsy (FNAB) specimens can increase the preoperative diagnostic accuracy for PTC in Korea (17,18). An increasing number of studies that include meta-analyses have been able to demonstrate an association between the BRAF status and aggressive tumor behavior (13,19 –21). Other studies, however, have failed to confirm these data, and this has resulted in uncertainty about the prognostic value of BRAF mutations in PTC (22 –27). The prognostic significance of the BRAFV600E mutation has been especially controversial in Korea. Although some studies have reported an association between the BRAFV600E mutation and extrathyroidal extension (ETE) and lymph node metastasis (4,28,29), most studies have failed to demonstrate an association with more aggressive clinicopathologic features in Korea (4,16,30 –33).
Recently, the role of telomerase reverse transcriptase (TERT) promoter mutations, which contribute to aggressive behavior in differentiated thyroid cancer, has been documented (34 –38). TERT promoter mutations have been observed in 4.7–25% of differentiated thyroid cancers (34 –39). These mutations have a significantly higher prevalence in aggressive thyroid tumor types such as widely invasive oncocytic carcinomas, poorly differentiated (PD) carcinomas, and anaplastic thyroid carcinomas (ATC) (34 –36,40). TERT is the catalytic subunit of the telomerase complex and is a predominant determinant for controlling telomerase activity. Telomerase plays a key role in increasing the longevity of cells by maintaining the length of telomere caps at the end of chromosomes. Telomerase activation is involved in mechanisms of tumorigenesis and telomerase activity is upregulated in 85–90% of cancers (41). The mechanisms of telomerase reactivation in cancer have yet to be fully explored. It is known that activating mutations in the promoter of the TERT gene lead to increased telomerase expression. These TERT promoter mutations include two hot spots (C228T and C250T) that have been identified in various types of tumors. TERT promoter mutations were first reported in melanoma (42) and have subsequently been identified in urothelial carcinomas, gliomas, and hepatocellular carcinomas (43 –45). TERT promoter mutations have been associated with bladder cancer recurrence and poor survival of glioma patients (44,45).
In thyroid cancer, TERT promoter mutations are prevalent in advanced tumors with a higher recurrence (35). Interestingly, a significant association of a TERTC228T with a BRAF mutation has been reported, and it has been proposed that their co-occurrence may define a more aggressive subgroup of PTCs (37). The TERTC228T promoter mutation creates a consensus binding site for E-twenty-six (ETS)/ternary complex factors (TCFs) transcription factors, including GA-binding protein (GABP) (42,46,47), and the BRAFV600E activated mitogen-activated protein kinase (MAPK) pathway induces expression of ETS transcription factor members (48). Hence, increased generation and interaction of ETS factors results in promoting the upregulation of the TERT promoter and subsequent telomerase activation. TERT promoter mutation analyses on thyroid FNAB specimens have not been performed in the Korean population, where the BRAFV600E mutation in PTC is prevalent. This study analyzed various thyroid tumors for the presence of TERT promoter mutations and examined their relationship with clinicopathologic factors and co-occurrence with the BRAFV600E mutation.
Materials and Methods
Patient selection and characteristics
Study approval was obtained from the Institutional Review Board (IRB) of Konkuk University Medical Center (KUH1210042). This study included 242 patients who underwent thyroidectomy for thyroid nodules between 2007 and 2014 at Konkuk University Medical Center in Seoul, Korea. Two hundred and forty-two FNAB specimens obtained preoperatively from the same number of patients with confirmed postoperative pathological diagnosis were evaluated. Also archival thyroid FNAB and resected pathologic specimens that had preoperative BRAF mutation analysis were blindly reevaluated according to the 2010 Bethesda System for Reporting Thyroid Cytopathology and 2004 World Health Organization (WHO) classification of thyroid neoplasm by two pathologists (T.S.H. [endocrine pathologist] and S.E.L.). In cases of a disagreement and to reach a consensus, another endocrine pathologist (C.K.J.) independently reviewed the cases. Among the 242 cases, six were classified as follicular adenomas (FA), 207 as PTC, 15 as FTC (six minimally invasive and nine widely invasive), two as PD carcinoma, five as ATC, six as medullary thyroid carcinomas (MTC), and one as squamous-cell carcinoma (SCC). Of 207 PTCs, 143 were classified as conventional, 24 as follicular variant, two as solid variant, two as Warthin-like variant, and one as oncocytic variant. Among 143 conventional PTCs (CPTCs), 18 were categorized as CPTC with ≥50% tall-cell component (TCC), 12 as CPTC with 10–50% TCC, two as CPTC with squamous-cell differentiation (CPTC with SD), and three as CPTC with ≥50% TCC and SD. The diagnosis of TCC was made on the basis of the definition in the 2004 WHO classification with tall columnar tumor cells having a height three times the width, having prominent cell borders, and a large amount of dense eosinophilic cytoplasm.
For PTCs, tumors >1 cm in diameter were selected. All samples of CPTC with ≥50% TCC, known as an aggressive variant of PTC, were selected in order to have a representative frequency of approximately 10% for the PTCs. All FTC, MTC, PD carcinomas, ATC, and some FA cases were analyzed. The total study population in the cohort consisted of 187 women (77.0%) and 56 men (23.0%), with a mean age of 48.4 ± 13.9 years.
DNA extraction
After slipping off the cover slips of FNAB cytology slides, atypical cells of interest were scraped, and DNA was extracted. Briefly, 20–50 μL of DNA extraction buffer solution (50 mM Tris buffer, pH 8.3; 1 mM EDTA, pH 8.0; 5% Tween 20 and 100 μg/mL proteinase K) with 10% resin was added to the scraped cells and incubated at 56.8°C for a minimum of 1 h. After incubation, the tubes were heated to 100°C for 10 min, followed by centrifugation to pellet the debris, and 5 μL of the supernatant was used in the polymerase chain reaction (PCR).
Detection of the BRAF mutation by PCR amplification and pyrosequencing
Each PCR mixture contained forward and reverse primers (each 0.4 pmol), 0.2 mmoL of each dNTP, 1.5 mmol/L of MgCl2, 1 × PCR buffer, 1.5 IU of Immolase DNA polymerase (Bioline, London, United Kingdom), and 5 μL of genomic DNA in a total volume of 50 μL. The PCR products were electrophoresed in a 2% agarose gel to confirm amplification of the PCR product. The biotinylated PCR product (20 μL) was attached to streptavidin–Sepharose beads (Amersham Biotechnology, Uppsala, Sweden) according to a standard protocol by incubating with shaking at room temperature for 10 min in binding buffer. The streptavidin–Sepharose beads were captured using a PSQ 96 sample prep tool with a 96 magnetic ejectable microcylinder (Biotage, Uppsala, Sweden). This tool was also used for a 1 min incubation of the biotin–streptavidin complex in 0.5 M of NaOH before washing in annealing buffer. Subsequently, the samples were hybridized to 15 pmol of sequencing primers in annealing buffer at 80°C for 2 min followed by cooling to room temperature. PCR primer and sequencing primer sequences were as follows: exon 15 (T1799A) forward, 5′-biotin-CTT CAT AAT GCT TGC TCT GAT AGG-3′; reverse, 5′-GGC CAA AAA TTT AAT CAG TGG AA-3′; sequencing reverse, 5′-CCA CTC CAT CGA GAT TT-3′. Pyrosequencing was performed using an SNP reagent kit (Biotage).
Identification of TERT promoter mutations by PCR amplification and direct sequencing
Standard PCR was carried out for sequencing to identify TERT promoter mutations. Briefly, a fragment of the TERT promoter was amplified by PCR using genomic DNA with the following primers: 5′-AGT GGA TTC GCG GGC ACA GA-3′ (sense) and 5′-CAG CGC TGC CTG AAA CTC-3′ (antisense). About 40–50 ng of genomic DNA was used in the PCR, which was carried out with an initial denaturation step at 95°C for 3 min, followed by 10 cycles of 95°C denaturation for 30 sec, 58–62°C annealing for 30 sec, and 68°C elongation for 1 min. This was then followed by 30 cycles of the same settings, except for elongation for an additional 5 sec in each cycle. The PCR was completed with a final elongation step at 68°C for 7 min. The PCR products were subsequently subjected to sequencing with a BigDye Terminator Cycle Sequencing Ready Reaction Kit (Applied Biosystems, Foster City, CA), with the following PCR cycles: 35 cycles of denaturation for 60 sec at 96°C, annealing for 5 sec at 50°C, and elongation for 4 min at 60°C. PCR was performed at a final volume of 10 μL containing 2.5 μL of 70 ng/μL of PCR product, 0.5 μL of sequencing primer (3 picomoles), 5 × buffer, and AmpliTaq DNA polymerase. The sDNA sequence was then read on an ABI 3730XL DNA Analyzer (Applied Biosystems). Sequences were aligned using the ContigExpress alignment program (InforMax, Frederick, MD).
Statistical analysis
For analysis of the relationship between clinicopathologic factors, including sex, multiplicity, extrathyroidal extension (ETE), and presence of TERTC228T/BRAFV600E mutation, Pearson's chi-square test and Fisher's exact test were used. A linear-by-linear test was used to examine the association between T stage, N stage, AJCC stage, and TERTC228T/BRAFV600E mutations. The time to recurrence-free survival (RFS) was defined from the day of first surgery until recurrence. The survival rates were calculated using the Kaplan–Meier method, and the survival curves were compared with a log-rank test. The Cox proportional hazard model was used to evaluate the associations between clinicopathologic factors and RFS. The hazard ratio (HR) and its confidence interval (CI) were assessed for each factor. All tests were two-sided, with 0.05 serving as the level of significance. Statistical analysis was performed using SPSS software version 18.0 (SPSS, Inc., Chicago, IL).
Results
Prevalence of TERTC228T/C250T and BRAFV600E mutations in various thyroid tumors
The status of two TERT promoter mutations along with the BRAFV600E mutation were analyzed in 242 thyroid tumors using FNAB specimens obtained preoperatively. Mutations in the TERT promoter and BRAFV600E were identified in 40 (16.5%) and 177 (73.1%) out of 242 tumor samples, respectively. All TERT promoter mutations were C228T mutations. None of the cases had a C250T mutation. The mutation frequency in each tumor type is shown in Table 1. The frequency of TERTC228T and BRAFV600E mutations was significantly different according to the histologic type of the thyroid tumor (p = 0.002 and p < 0.001, respectively). A TERTC228T mutation was found in 1/6 (16.7%) FAs. Of 222 WD thyroid cancers (207 PTCs and 15 FTCs), 34 (15.3%) harbored a TERTC228T mutation (14.5% of PTC and 26.7% of FTC). The mutation frequency in each PTC variant was as follows: 23/143 (16.1%) CPTCs without other component, 2/24 (8.3%) FVPTCs, and 1/2 (50%) Warthin-like variant PTCs. Among CPTCs with TCC, one case with 10–50% TCC (8.3%) harbored a TERTC228T mutation. No TERTC228T mutation was found in CPTC with ≥50% TCC, whereas all three CPTCs with ≥50% TCC and SD cases harbored a TERTC228T mutation (Fig. 1). Collectively, from 33 cases that contained at least 10% TCC, four cases (12.1%) harbored a TERTC228T mutation. Two CPTCs with SD, two solid variant PTCs, and one oncocytic variant PTC did not harbor a TERTC228T mutation. Even though the numbers are small, 50% of PD carcinomas and 60% of ATCs showed a TERTC228T mutation. One SCC, a rare primary thyroid epithelial tumor, had a TERTC228T mutation. On the other hand, a TERTC228T mutation was not observed in any of the six MTCs. The BRAFV600E mutation was found in 84.1% of PTCs, 50% of PD carcinomas, and 20% of ATCs, whereas none of the FAs, FTCs, and MTCs harbored a BRAFV600E mutation.
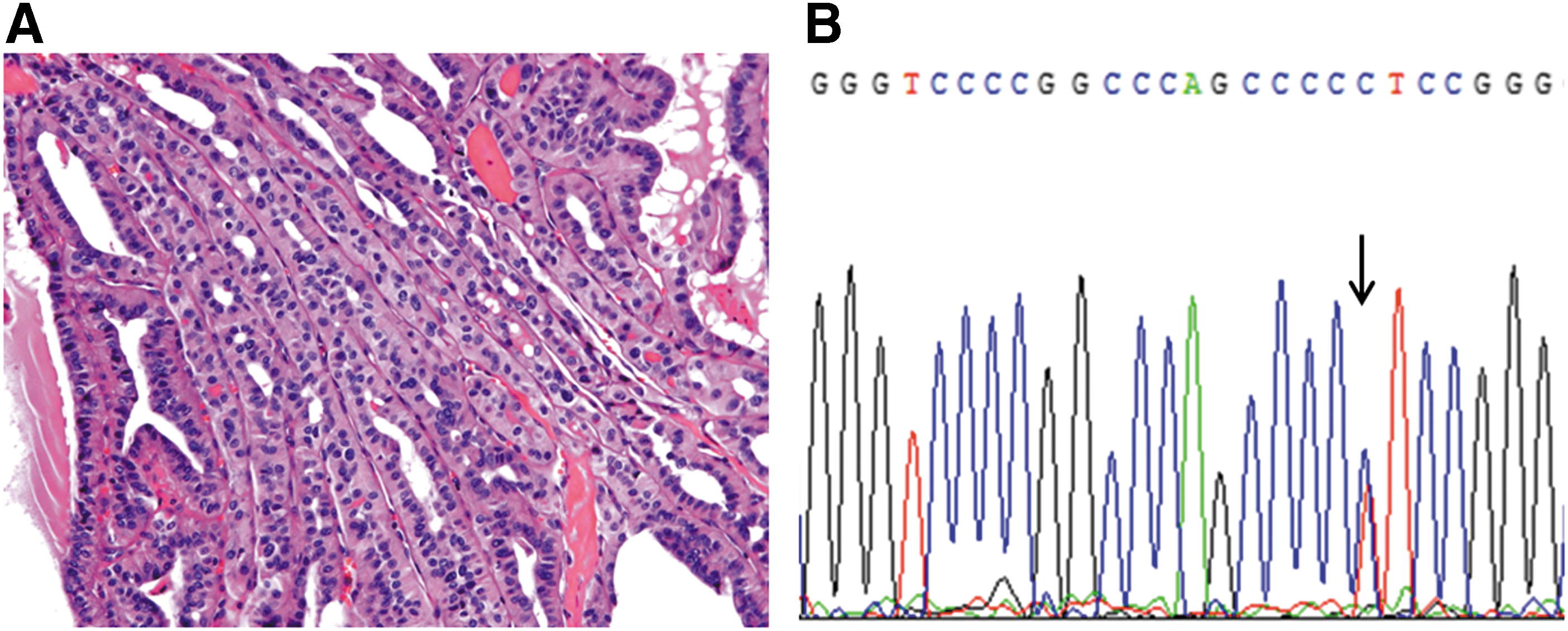
Representative case showing a papillary thyroid carcinoma histology with >50% of tall-cell component (
FA, follicular adenoma; CPTC, classical PTC; CPTC with SD, classical PTC with squamous differentiation; CPTC with TCC, classical PTC with tall-cell component; FVPTC-E, encapsulated follicular variant of PTC; FVPTC-I, infiltrative follicular variant of PTC; FTC-M, minimally invasive follicular carcinoma; FTC-W, widely invasive follicular carcinoma; PD, poorly differentiated; ATC, anaplastic thyroid carcinoma; MTC, medullary thyroid carcinoma; SCC, squamous cell carcinoma; N/A, not applicable.
Clinicopathologic demographics of the patients with PTC
The relationship with the TERTC228T mutation and the BRAFV600E mutation in 207 PTC cases was also analyzed. The study population consisted of 161 women (77.8%) and 46 men (22.2%), with a mean age of 47.5 ± 13.4 years. Eighty-eight patients (42.5%) were <45 years old, and 119 patients (57.5%) were >45 years old. Of these, 158 patients (90.8%) underwent total thyroidectomy, and 19 patients (9.2%) underwent lobectomy. Median duration of follow-up was 48 months (range 0–95 months) after surgery. Of 207 patients, recurrence occurred in 18 (8.7%) patients. Tumor recurrence was present in 10/143 (7.0%) CPTCs, 1/13 (7.7%) encapsulated FVPTCs, 1/11 (9.1%) infiltrative FVPTCs, 1/18 (5.6%) CPTCs with ≥50% TCC, 1/12 (8.3%) CPTCs with 10–50% TCC, 1/2 (50%) CPTCs with SD, 2/3 (66.7%) CPTCs with ≥50% TCC and SD, and 1/2 (50%) Warthin-like variant PTCs. No recurrence was identified in one solid and one oncocytic variant PTC. The recurrence rate according to the histologic type was statistically different (p = 0.022).
Association between TERTC228T/BRAFV600E mutations and clinicopathologic features of PTC
Of 207 patients with PTC, 30 (14.5%) and 175 (84.5%) harbored either a TERTC228T or a BRAFV600E mutation, respectively. The association of a TERTC228T or a BRAFV600E mutation and clinicopathologic factors in PTC patients was evaluated (Table 2). Patients with the TERTC228T mutation were more likely to have a recurrence (p = 0.029). However, there was no significant difference in TERTC228T mutation status regarding sex, age at diagnosis, size, tumor multiplicity, ETE, T stage, N stage, and AJCC stage.
Statistically significant values are shown in bold.
ETE, extrathyroidal extension.
The BRAFV600E mutation was significantly associated with age at diagnosis, multiplicity, and AJCC stage. Patients with a BRAFV600E mutation were older than those with wild-type BRAF (p = 0.001). The mutation was found more frequently in advanced stages, whereas wild-type BRAF was more prevalent in stage I cases (p = 0.009). However, recurrence rate was not different according to BRAFV600E mutation status (p = 1.000).
Association between TERTC228T and BRAFV600E mutations
A TERTC228T mutation was found in 15.4% (27/175) and 9.4% (3/32) of BRAFV600E mutant and wild-type BRAF cases, respectively. Conversely, the BRAFV600E mutation was found in 90.0% (27/30) and 83.6% (148/177) of TERTC228T mutant and wild-type TERT tumors, respectively. The TERTC228T mutation was not significantly associated with BRAFV600E mutation (p = 0.584).
The cases were also classified into four groups according to BRAF/TERT mutation status as follows: BRAF–/TERT– (n = 29; 14%); BRAF+/TERT– (n = 148; 71.5%); BRAF–/TERT+ (n = 3; 1.4%); and BRAF+/TERT+ (n = 27; 13.0%). The clinicopathologic characteristics among these four groups were also evaluated in Table 3. Both the TERTC228T and BRAFV600E mutant group was significantly associated with older age and advanced stage compared with the BRAF–/TERT– group.
p-Values are from the comparison of the indicated genetic group in the column immediately left of the p-value column with the no mutation group. Statistically significant values are shown in bold.
Relationship of clinicopathologic factors with RFS
When the patients were divided into two groups based on TERTC228T mutation status, the TERTC228T mutant group showed significantly lower RFS (p = 0.014) than the wild-type group did. Kaplan–Meier survival curves and corresponding p-values are shown in Figure 2.
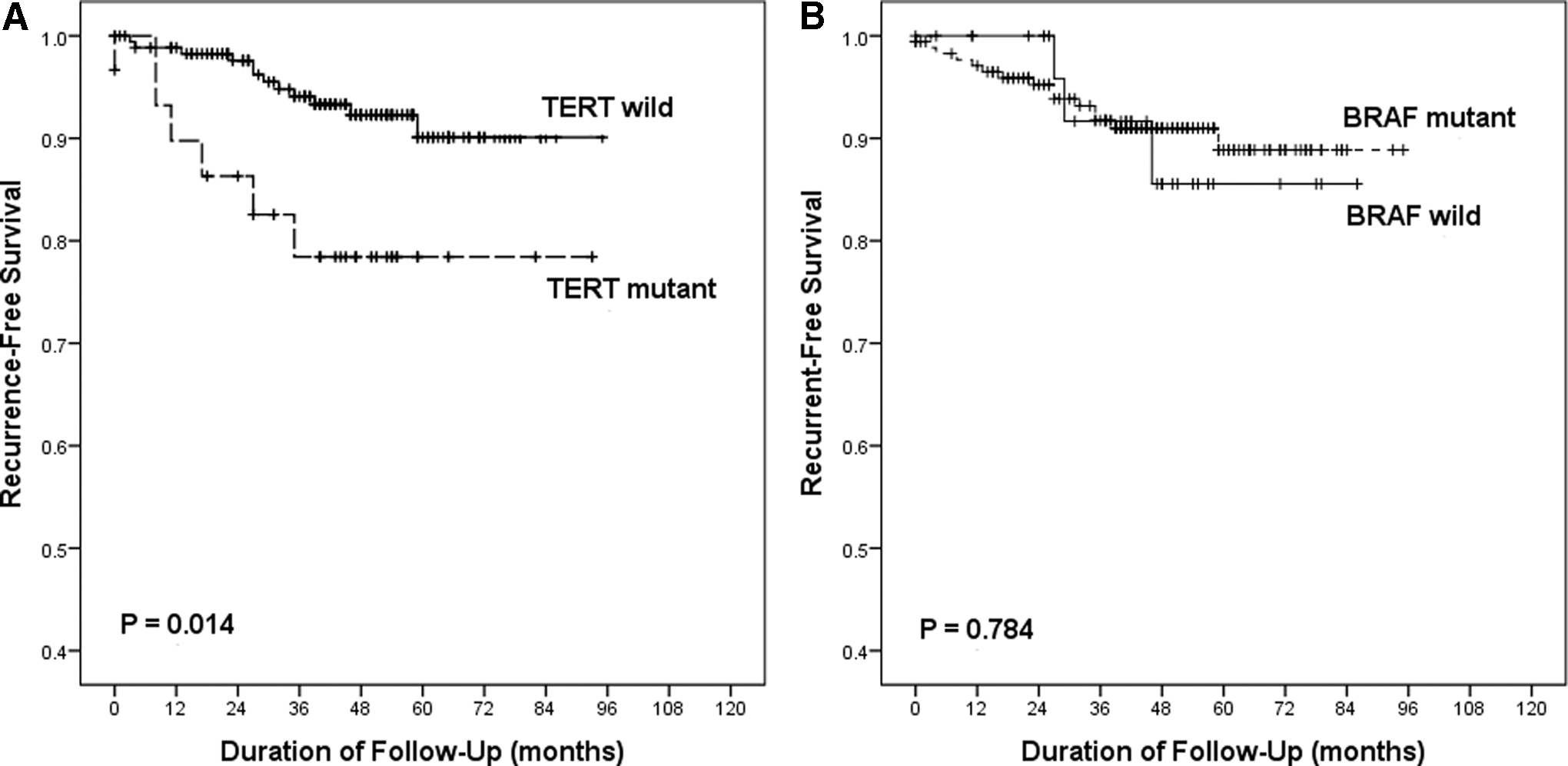
Kaplan–Meier survival curves with log-rank test of recurrence-free survival after classification into two groups based on the presence of a TERTC228T
mutation (
The prognostic relevance of clinicopathologic and biologic parameters on RFS of the patients with PTC was analyzed. RFS was significantly associated with tumor size (p = 0.001), ETE (p = 0.036), nodal stage (p = 0.004), and TERTC228T mutation status (p = 0.020) in univariate analysis. In multivariate analysis, tumor size (p = 0.019) and TERTC228T mutation status (p = 0.042) remained as an independent predictor of tumor recurrence when other clinicopathologic cofactors including BRAFV600E mutation were adjusted (Table 4).
Statistically significant values are shown in bold.
HR, hazard ratio; CI, confidence interval.
Discussion
The frequency of TERT promoter mutations was evaluated using 242 FNAB specimens of thyroid tumors. The frequency of TERT promoter mutations has been reported to vary between 7.5% and 25% in WD thyroid cancers, and it was found in up to 50% of oncocytic carcinomas, PD carcinomas, and ATCs (34 –36,40). In the present study, 14.5% (30/207) of PTCs, 26.7% (4/15) of FTCs, 50.0% (1/2) of PD carcinomas, and 60.0% (3/5) of ATCs harbored a TERTC228T mutation. Although the frequency of TERT promoter mutations in FTC was slightly higher than those in previous studies, this stepwise increase from differentiated to PD and ATC is in agreement with previous data (34 –37). The tall-cell variant of PTC (TVPTC) is known to be associated with a less favorable prognosis (49,50). Liu et al. (35) found that the prevalence of TERT mutations in TVPTC (30.8%) was higher than that in CPTC (35). In the present study, out of 33 PTCs containing at least 10% TCC, four (12.1%) cases harbored the TERTC228T mutation, which is lower than the prevalence reported in a previous study (35). However, Dettmer et al. recently identified that TERT mutations were found in 15.9% (7/44) of PTCs with a TCC component >10%, and the majority of TVPTCs with adverse outcome did not harbor TERT mutations (51). In the present study, the majority of patients with PTCs harboring a TCC component of >10% also did not develop recurrences. Because results on the prevalence of TERT mutations in Korean TVPTC cases are not available for comparison, a multicenter larger cohort study with PTCs harboring TCC needs to be performed. TERT promoter mutations were identified in 16.7% (1/6) of FAs. The identification of TERT promoter mutations in benign thyroid neoplasms was previously reported, and the authors suggested that TERT promoter mutations may occur as an early genetic event in thyroid follicular tumors (52).
Most of the TERT mutation analysis in thyroid neoplasm was performed with formalin-fixed paraffin-embedded (FFPE) specimens. One recent TERT promotor mutation analysis performed on thyroid FNAB revealed that 3.6% of the PTCs harbored a mutation, and the authors suggested that the lower observed prevalence might be attributed to the low sensitivity of the direct sequencing method on FNAB specimens due to sparse cancer cells (53). However, the prevalence of TERT promoter mutations in thyroid FNAB samples in the present study does not differ from that of the several recent studies performed on FFPE specimens (34 –38). Even though we did not compare the prevalence of TERT mutations between FNAB and matched FFPE specimens, BRAF mutation analysis using FNAB and matched FFPE specimens in the laboratory showed a 97.5% concordance rate (not published). Mutational analysis using FNAB specimens is more sensitive and specific when target cells are dissected properly. Moreover, FNAB specimens with alcohol fixation can preserve DNA better than FFPE specimens can.
Next, the relationships of TERT promoter and BRAFV600E mutation status and clinicopathologic factors in PTC specimens were evaluated. Among clinicopathologic factors, only recurrence rate was related with the presence of a TERTC228T mutation. The BRAFV600E mutation was not associated with recurrence, even though it was more frequently found in advanced stages. These findings are in agreement with most published studies (4,16,30 –33). As previously described, the prognostic significance of the BRAFV600E mutation remains controversial in Korea. One reason could be that prevalence of BRAF mutations in PTC is much higher in Korea compared with other countries and that the numbers for the remaining wild-type BRAF cases are not powered for analysis. The reason(s) for the higher prevalence of BRAF mutations in PTC of Korean patients remain elusive. A further reason for the controversy concerning the predictive value of a BRAF mutation could be that adverse patient outcomes with multiple tumor relapses and eventual death resulting from PTC are rare events (54).
Although a statistically significant association was not observed between the presence of TERT and BRAF mutations, the TERTC228T mutation was highly prevalent in tumors harboring the BRAFV600E mutation. The coexistence of a TERTC228T and a BRAFV600E mutation was found in 13.0% (27/207) of all PTCs, which is higher than the prevalence observed in previous studies (37,38). This may perhaps be explained by the higher prevalence of the BRAFV600E mutation in Korea. The coexistence of a TERTC228T and a BRAFV600E mutation was significantly associated with older age and advanced stage compared with the group negative for either mutation.
Patients with the TERTC228T mutation had significantly lower RFS than those with wild-type TERT did. This also remained an independent predictor of tumor recurrence when other clinicopathologic cofactors, including the BRAFV600E mutation, were adjusted. The findings concerning the risk factor associated with the presence of a TERT mutation are in line with the 2015 American Thyroid Association (ATA) Guidelines for Thyroid Nodules and Cancer that propose a number of hazard factors for persistence/recurrence of the tumor and death (55). For the risk categories provided, the presence of a TERT mutation is listed as placing patients at a high possibility of recurrence, regardless of the presence of a BRAFV600E mutation. Therefore, preoperative testing for TERT promoter mutations on FNAB samples could help in predicting the prognosis of PTC patients and triaging the patient to receive an appropriate treatment protocol at initial surgery.
The main limitation of this study is having a relatively small number of patients with short follow
In conclusion, among thyroid cancer patients in Korea, to the authors' knowledge, this is the first study performing a TERT promotor mutation analysis in combination with a BRAFV600E analysis on FNAB specimens. The prevalence of these mutations in various thyroid tumors and the prognostic impact of the TERTC228T mutation among patients where the BRAFV600E mutation is frequent were determined. The results provide evidence to adopt TERT promoter mutation analysis as a preoperative adjunctive diagnostic test, thereby providing a risk stratification tool to guide a tailored approach to patient treatment.
Footnotes
Acknowledgments
The authors thank Dr. Chan-Kwon Jung (Department of Pathology, College of Medicine, The Catholic University, Seoul, Korea) for reviewing thyroid tumor slides.
Author Disclosure Statement
The authors have nothing to disclose.