
Abstract
Background:
The extent of thyroidectomy for low-risk well-differentiated thyroid cancer (WDTC) remains controversial. Historically, total thyroidectomy (TT) has been recommended for WDTC ≥1 cm in size. However, recent National Comprehensive Cancer Network and American Thyroid Association guidelines recognize unilateral thyroid lobectomy as a viable alternative for 1–4 cm cancers due to their otherwise favorable prognosis, with TT remaining the preferred option for tumors with unfavorable pathological characteristics. This study sought to determine how often a completion TT would be recommended based on these guidelines if lobectomy was initially performed in patients with 1–4 cm WDTC without preoperatively known risk factors.
Methods:
Patients who underwent thyroidectomy for 1–4 cm WDTC (January 2000 to January 2010) were retrospectively reviewed. Patients with preoperatively known high-risk characteristics, including gross extrathyroidal extension (ETE) on preoperative imaging, clinically apparent lymph node metastases, distant metastases, history of radiation, and positive family history, were excluded. The pathology specimens from the cancer-containing lobe were evaluated for features that would lead to a recommendation for TT based on current guidelines, including aggressive histology, vascular invasion, microscopic ETE, positive margins, and any positive lymph nodes within the specimen.
Results:
Of 1000 consecutive patients operated for WDTC, 287 would have been eligible for lobectomy as the initial operation. The mean age in this cohort was 45 years, and 80% were women. Aggressive tall-cell variant histology was found in one patient (0.5%), angio-invasion in 34 (12%), ETE in 48 (17%), positive margins in 51 (18%), and positive lymph nodes in 49 (18%) patients. Completion TT would have been recommended in 122/287 (43%) patients. Even in those with 1–2 cm cancers, completion TT would have been recommended in 52/143 (36%) patients.
Conclusions:
Nearly half of the patients with 1–4 cm WDTC who are eligible for lobectomy under current guidelines would require completion TT based on pathological characteristics of the initial lobe. Surgeons, endocrinologists, and patients need to balance the relative benefits, risks, and costs of initial TT versus the possible need for reoperative completion TT.
Introduction
T
The other high-risk characteristics, however, are only apparent upon pathology examination in the postoperative setting. These include microscopic ETE, positive tumor margins, incidental positive lymph nodes in the specimen, vascular invasion, and an aggressive tumor subtype. Therefore, the subset of patients undergoing unilateral lobectomy that are subsequently found to have any of these features are recommended to undergo a completion TT—an additional operation. Although generally safe, particularly when performed at high-volume centers, completion TT adds cost and potential for complications. It is therefore important to determine the likelihood of finding high-risk pathological features that would lead to a second operation when deciding on the extent of initial operation (7). This study sought to determine how often a completion TT would be recommended based on these guidelines if lobectomy were the initial operation in patients who underwent thyroidectomy for 1–4 cm WDTC without preoperatively known high-risk characteristics.
Materials and Methods
Patients
A retrospective analysis was performed of patients at the University of California, San Francisco (UCSF) who underwent thyroid operations for WDTC 1–4 cm in size between January 2000 and January 2010. Patients were selected based on the final pathology using the UCSF cancer registry. Patients not eligible for initial lobectomy according to the National Comprehensive Cancer Network (NCCN) and American Thyroid Association (ATA) thyroid cancer management guidelines (5,6) were excluded. Thus, patients in the final analysis did not have any preoperatively known high-risk characteristics, including: (i) gross ETE on preoperative imaging or clinically evident intraoperatively, (ii) clinically apparent lymph node metastases (either preoperatively or intraoperatively), (iii) distant metastases, or (iv) a history of radiation or a positive family history. Bilateral nodularity was not used as exclusion criterion. However, a subgroup analysis was performed on the patients without contralateral nodules.
Indications for completion TT
The pathological characteristics of the thyroidectomy specimens were evaluated, focusing on the cancer-containing thyroid lobe. Specifically, the frequency of high-risk pathological features in the lobe that would have led to the recommendation for completion TT were evaluated. These high-risk characteristics included aggressive histology (tall-cell, diffuse sclerosing variant), lymphovascular invasion, microscopic ETE, positive margins, and any positive lymph nodes (N1) within the specimen. These characteristics can be found in recommendation 35 and table 12 of the 2015 ATA guidelines and on page 17 of the 2015 (version 1) NCCN guidelines (5,6). The specimens were also reviewed for the presence of additional tumor foci in the cancer-containing lobe (ipsilateral multifocality), as well as the presence of tumor foci in the contralateral lobe (contralateral multifocality), as these features also might direct clinicians to perform completion TT. A subset analysis was performed specifically for patients with 1–2 cm (T1b) tumors, who presumably would be at lowest risk.
Statistical analysis was performed using IBM SPSS Statistics for Windows v22 (IBM Corp, Armonk, NY). This study was approved by the UCSF Committee on Human Research, the university's Institutional Review Noard.
Results
Patient characteristics
One thousand patients who underwent thyroidectomy between January 2000 and January 2010 were analyzed. Of these, 287 (29%) would have been eligible for lobectomy according to the new guidelines by the NCCN and ATA (Fig. 1). The mean age of the cohort was 45 years (range 13–82 years), and 230 (80%) patients were women. The default recommended operation at UCSF was TT for all WDTC >1 cm in size, which was reflected by the 209/287 (73%) frequency of TT in this cohort. Lobectomy was performed in 78/287 (27%) of patients, of whom 70/78 (90%) underwent completion TT. Six of these patients also underwent central neck dissection as part of their second procedure. The mean size on pathology was 21 mm. Size on preoperative ultrasound was available in 206/287 (72%) patients, which was significantly larger, with a mean of 26 mm (p < 0.01; Table 1).
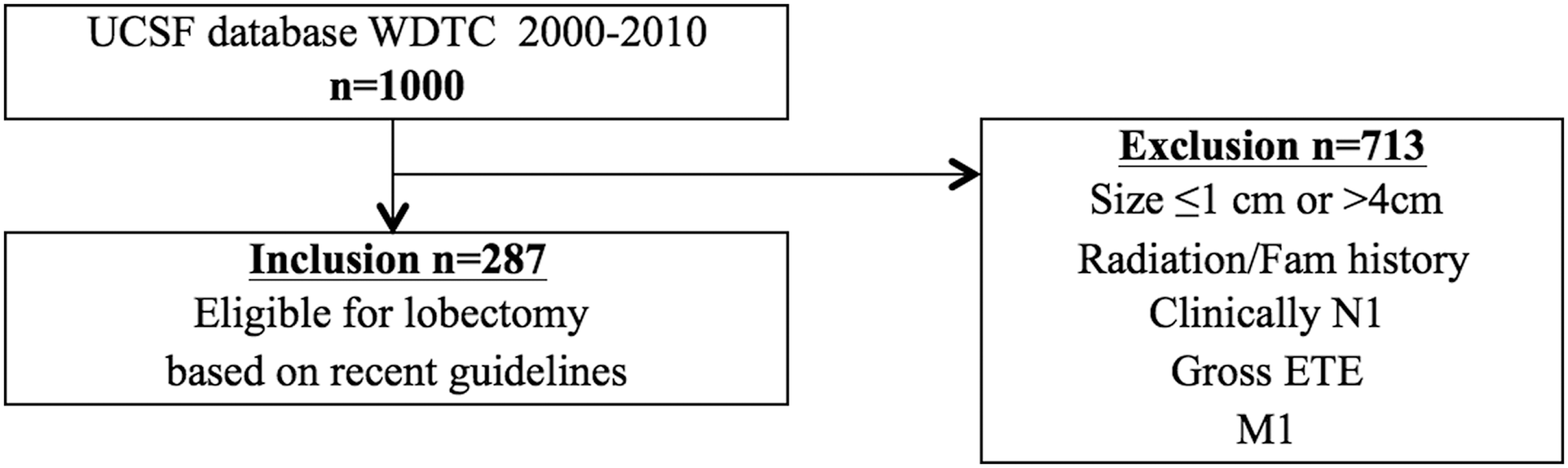
Flow chart of included patients.
WDTC, well-differentiated thyroid cancer; NCCN, National Comprehensive Cancer Network; ATA, American Thyroid Association; TT, total thyroidectomy.
Frequency of features leading to completion TT
On pathological examination of the cancer-containing lobe, 122 (43%) specimens had one or more high-risk characteristic that would be an indication for completion TT. Since indications for completion TT may vary per institution, Figure 2 allows clinicians to decide on the probability of needing a completion TT based on their own institutional practice. The most common reason for recommendation of completion TT was the presence of a microscopic positive margin (18%), followed by ETE (17%) and incidental positive lymph nodes in the central compartment (17%). Since those who underwent a formal neck node dissection were excluded, all nodes were found incidentally on pathology examination. None of the patients had more than five positive lymph nodes removed. The size of the metastatic lymph nodes was available in 10/49 patients, and in nine cases, they were >1 mm.

Individual and cumulative frequencies of selected high-risk characteristics that could lead to the recommendation of completion total thyroidectomy.
In addition, ipsilateral multifocality was found in 71 (25%) patients. Including ipsilateral multifocality as an indication for completion TT, 158 (55%) would have undergone an additional operation. Contralateral tumor foci were present in 73 (25%) of all patients, including in 42 (21%) of the patients who had no other high-risk characteristic in the initial lobe and would not otherwise have been recommended to undergo completion TT. A summary of these results can be found in Table 2.
FvPTC, follicular variant of papillary thyroid carcinoma; PTC, papillary thyroid carcinoma; FTC, follicular thyroid carcinoma.
Preoperative bilateral nodularity was seen on ultrasound in 108/287 (38%) patients. Subgroup analysis of the 179 patients without contralateral nodules revealed that 48% had one or more high-risk criteria for recommending a completion TT.
Of the total cohort, 143 (50%) patients had tumors 1–2 cm in size. The mean age of this group was 46 years, and 120 (84%) were women. Based on the same high-risk characteristics, completion TT would have been recommended in 52 (36%) patients in this group.
Discussion
This study found that 43% of patients undergoing thyroidectomy for preoperatively low risk 1–4 cm WDTC who would have been eligible for initial unilateral lobectomy under the current NCCN and ATA guidelines would have needed a completion TT after pathological analysis of the initial lobe. Even in patients with smaller tumors (1–2 cm), 36% would have required a completion TT.
The previous recommendation for routine TT for 1–4 cm WDTC was mainly based on a study by Bilmoria et al., which used data from the National Cancer Database to demonstrate longer disease-free survival and lower rate of local recurrence after TT than after unilateral lobectomy (2). Lobectomy was reserved only for cases of microcarcinomas (WDTC <1 cm) (1).
However, several recent studies showed no significant difference in either disease-free survival or recurrence rate in patients with WDTC >1 cm after lobectomy versus TT (4,8). A recent reanalysis of the National Cancer Database of 61,775 patients showed that the extent of surgery was not associated with survival (3). In contrast to the previous analysis of the National Cancer Database, Adam et al. adjusted their analysis for additional variables related to comorbidity and extensiveness of disease, which had caused the earlier difference in survival. Based on these studies, the most recent NCCN guidelines have been amended to support the option of unilateral thyroid lobectomy for patients without preoperatively known high-risk characteristics (5). The new ATA guidelines for the management of WDTC have echoed this shift in treatment recommendations for low-risk WDTC.
Thyroid lobectomy does have some advantages. First, lobectomy is inherently associated with lower operative risks than TT, particularly related to postoperative hypoparathyroidism, although both operations are quite safe, particularly in high-volume surgeon/center settings. Although extremely rare, the devastating risk of bilateral recurrent laryngeal nerve injury requiring tracheostomy is avoided with lobectomy (9). Having a remaining lobe may also obviate the need for thyroid hormone replacement in more than half of patients when thyrotropin suppression may not be necessary (10).
Despite these advantages, there are several reasons why TT has historically been the operative treatment of choice for WDTC >1 cm. TT allows for the use of radioactive iodine (RAI) in both postoperative treatment and surveillance. Therefore, the recommendation for TT is often tied to the recommendation for RAI. There has been a paradigm shift in the management of WDTC because recent data have not shown benefits of RAI in low-risk tumors, and an iodine scan is no longer the only surveillance modality. Ultrasound imaging technology and sensitivity of thyroglobulin measurements have improved greatly and have become the standard of care for surveillance. Although there is currently a trend toward more selective use of RAI in the treatment of WDTC, it is still unclear whether low- to intermediate-risk patients have similar outcomes without RAI treatment (11). In the present cohort, of 165 patients that did not have any concerning features on final pathology requiring completion TT, 77 (47%) still received RAI. This reflects the wide variation and lack of broad consensus among medical endocrinology practices and lack of clear guidelines, due to conflicting data, concerning the role of RAI. A possible explanation for this finding might be that these patients had other features that would have been an indication for additional treatment such as tumor multifocality. In the absence of a clear consensus, the decision on the extent of thyroidectomy and the role of RAI is always one that should be made between the patient, surgeon, and endocrinologist, as reflected in the present results.
About 30% of patients with low-risk WDTC harbor contralateral cancers (12,13). While the clinical relevance of these cancers is still unclear, these tumors may represent multicentricity or intrathyroidal spread (14,15). Often these are microcarcinomas that are not detected on preoperative imaging. In addition, some observational studies have shown very low progression rates (16). Nevertheless, it is important for clinicians to realize that after a lobectomy, 25% of these patients will have contralateral cancer foci.
Following patients with thyroid cancer after lobectomy may be more challenging. Thyroglobulin levels are easier to interpret after TT than after lobectomy, and detecting recurrent central lymph nodes using ultrasound is also more technically challenging with a remaining thyroid lobe (17).
Based on the present results, clinicians should be aware that nearly half of the patients who undergo unilateral thyroid lobectomy for seemingly low-risk WDTC 1–4 cm in size may eventually undergo completion TT. Unfortunately, not all high-risk characteristics can be determined preoperatively. For patients whose high-risk characteristics are only found on pathology, a second operation is needed. Whether this need for reoperation is reasonable depends on many factors, including how the patient perceives this risk. The complication rates of a two-stage thyroidectomy should be similar to upfront TT when performed by a high-volume surgeon, but a two-stage operation involves additional anesthesia, patient stress, and costs to both the system and patients (18). Cost-effectiveness analyses would be helpful to address the relative value of unilateral lobectomy versus TT, taking into account the likelihood of requiring a second operation after an initial lobectomy.
This study has several limitations. First, the percentage of patients requiring completion TT may be institution dependent, and the inherent potential for selection bias in reviewing patients from a high-volume tertiary-care academic center is acknowledged. Second, different definitions and determinations of high-risk features over time may also lead to varying needs for completion TT. For example, some of the presumed higher-risk characteristics, such as microscopic positive margins, do not have clearly delineated clinical significance. Third, any positive lymph nodes within the specimen were used as high-risk characteristic, whereas patients with five lymph nodes or fewer (<0.2 cm) are still considered ATA low risk. Since prophylactic neck dissections are not performed and all patients with clinically N1 were excluded, none of the patients had more than five lymph nodes removed. It is possible that of the 39 patients without available size of the lymph node metastasis, some contained micrometastatic (<0.2 cm) disease and would have been considered ATA low risk. Thus, the rates of completion TT in this study may be overestimated. Fourth, intrathyroidal, well-differentiated follicular cancer with fewer than four foci of vascular invasion are considered low risk. However, since the information on the number of vessels invaded was not available for every patient in this historical cohort, it was not possible adjust for this. Although only a small subset of patients had minimally invasive follicular carcinomas in this study (n = 42), this can potentially result in an overestimation of the rate of completion TT. Fifth, the BRAFV600E status was not taken into account, since mutational analysis was not routinely performed until 2010. A positive mutation classifies these patients as ATA intermediate risk. In the authors' center, up to 88% of patients with papillary thyroid cancer harbor a BRAFV600E mutation. Thus, including this variable will most likely increase the rate of completion TT substantially (19).
Lastly, there may not be complete concordance between the size of cancer on pathology exam and the size of the lesion on ultrasound. The size of tumors for inclusion was extracted from final pathology reports, as these were available for all patients. However, this size was significantly larger than the size on ultrasound (26 mm vs. 21 mm). Using ultrasound size for inclusion may have provided a more realistic sample. However, even when only smaller cancers of 1–2 cm were included, 36% of the patients still would have required TT.
The current trend in the management of WDTC has become more conservative. Unilateral lobectomy is now suggested as a viable alternative to TT for patients with WDTC 1–4 cm in size. Although overall prognosis seems to be excellent after lobectomy, many of these patients have high-risk characteristics that only become apparent at final pathology. It is important for the patient and clinician to understand and estimate the risks and benefits of lobectomy versus TT. This study provides some estimate for this possible need for completion TT after an initial lobectomy for these otherwise low-risk patients.
Footnotes
Acknowledgments
We thank Ann Griffin and Joseph McGuire for their help in identifying patients from the UCSF Cancer Registry Database.
Author Disclosure Statement
The authors have nothing to disclose.