
Abstract
Background:
Serum thyroid hormone concentration is regulated through the hypothalamic–pituitary–thyroid axis. This study aimed to clarify the relationships between thyroid hormone regulation and ultrasonographic findings in subjects with thyroid nodules detected during thyroid ultrasound examination for the Fukushima Health Management Survey.
Methods:
As of October 31, 2014, a total of 296,253 subjects, who had been living in Fukushima Prefecture at the time of the Fukushima nuclear power plant accident and were aged ≤18 years on March 11, 2011, participated in two concurrent screening programs. In the primary screening, thyroid nodules were detected in 2241 subjects. A secondary confirmatory thyroid ultrasound examination and blood sampling for thyroid function tests were performed on 2004 subjects. The subjects were reassessed and classified into disease-free subjects (Group 1), subjects with cysts only (Group 2), subjects with nodules (Group 3), and subjects with malignancy or suspected malignancy (Group 4). Serum concentrations of free triiodothyronine (fT3), free thyroxine (fT4), thyrotropin (TSH), thyroglobulin, and the fT3/fT4 ratio were classified according to the diagnoses.
Results:
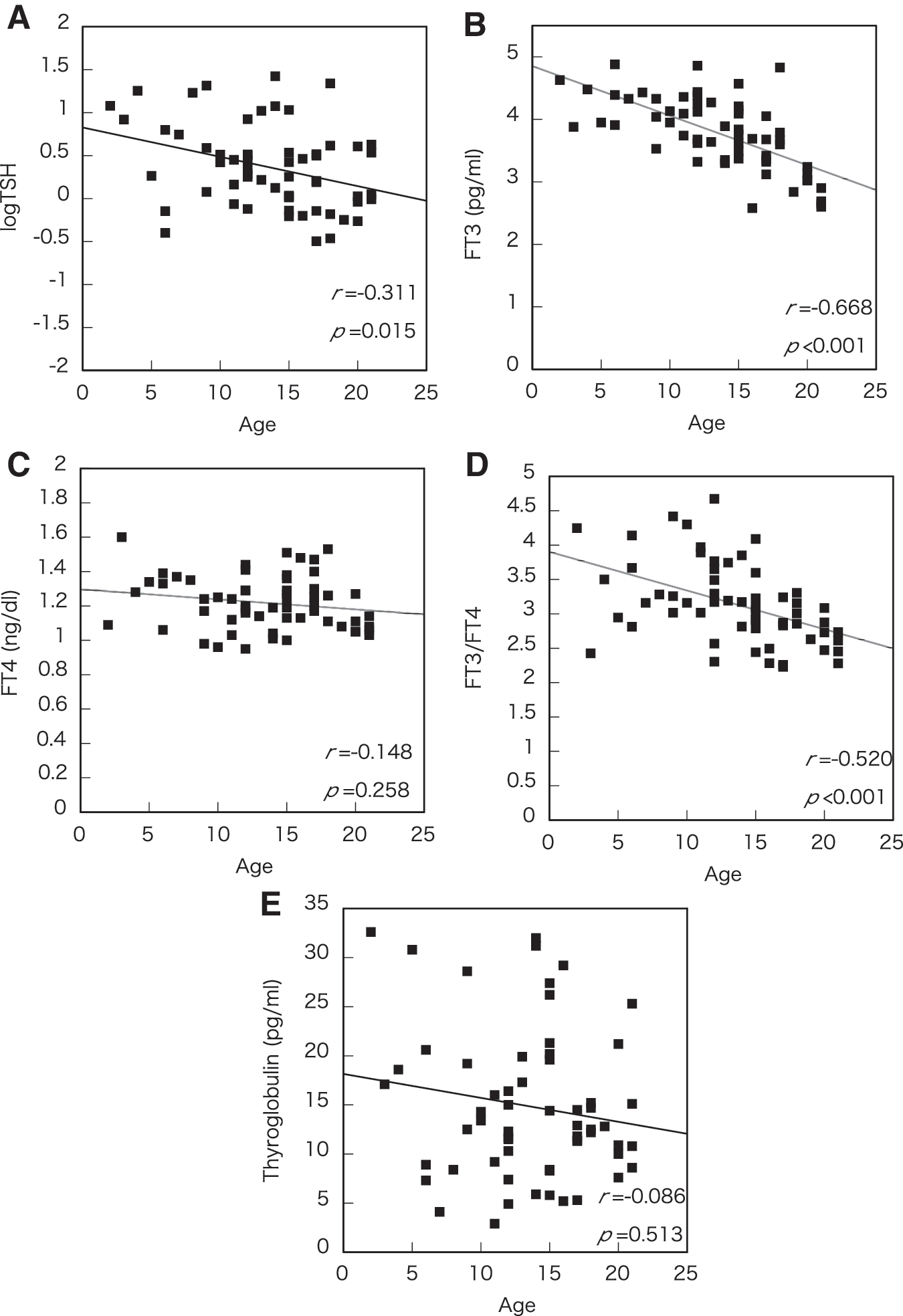
Inverse relationships between age and log TSH values (Spearman's correlation r = −0.311, p = 0.015), serum fT3 concentration (r = −0.688, p < 0.001), and the fT3/fT4 ratio (r = −0.520, p < 0.001) were observed in Group 1. When analysis of covariance with Bonferroni post hoc comparisons was used in the four groups, the log TSH values were significantly lower in both Group 3 and Group 4 compared with Group 1 and Group 2 after correcting for age (p < 0.001; Group 1 vs. Group 3, p = 0.016; Group 1 vs. Group 4, p = 0.022; Group 2 vs. Group 3, p = 0.001; Group 2 vs. Group 4, p = 0.008). However, no significant differences were observed between the four groups regarding levels of fT3, fT4, fT3/fT4 ratio, and thyroglobulin (p = 0.304, 0.340, 0.208, and 0.583, respectively).
Conclusion:
TSH suppression can be present in response to illness, including thyroid nodules, in young subjects. Low TSH levels may be associated with the finding of papillary thyroid cancer as well as with thyroid nodules in children and adolescents.
Introduction
A
In the current study, age dependency was assessed initially using data obtained from healthy subjects who had undergone the second screening. Serum concentrations of fT3, fT4, TSH, and thyroglobulin were evaluated in the group of patients with normal thyroid function following exclusion of subjects with autoimmune thyroid disease, apparently abnormal function tests, and thyroid nodules and cysts. Subsequently, the concentrations of thyroid hormone and TSH were assessed in those groups with nodules based on the results of the second screening. The different responses of thyroid hormone to TSH concentrations in the individuals with nodules, including those with thyroid cancer, were then evaluated.
Subjects and Methods
Thyroid ultrasound examination in the Fukushima Health Management Survey
The initial TUE of the Fukushima Health Management Survey included approximately 360,000 subjects who had been living in Fukushima Prefecture at the time of the accident and were aged ≤18 years on March 11, 2011 (1). The participation rate was 81.2% for ages 2–19 years as of December 31, 2014. The subjects were classified into three categories (A, B, and C) according to the results of the primary screening. Category A contained subjects without thyroid nodules or cysts (subcategory A1) and subjects with benign findings (≤5.0 mm nodules and/or ≤20.0 mm simple or colloid cysts) that did not require further confirmatory TUE (subcategory A2). Category B subjects had nodules ≥5.1 mm and/or cysts ≥20.1 mm, and were recommended to undergo a confirmatory TUE. Category C subjects had TUE findings that were of concern, such as a large tumor or tumors associated with either major extrathyroidal invasion or multiple, large lymph node metastases, and an immediate re-examination was recommended. Thus, a total of 2241 subjects from Categories B and C were entered into the confirmatory survey (Fig. 1).
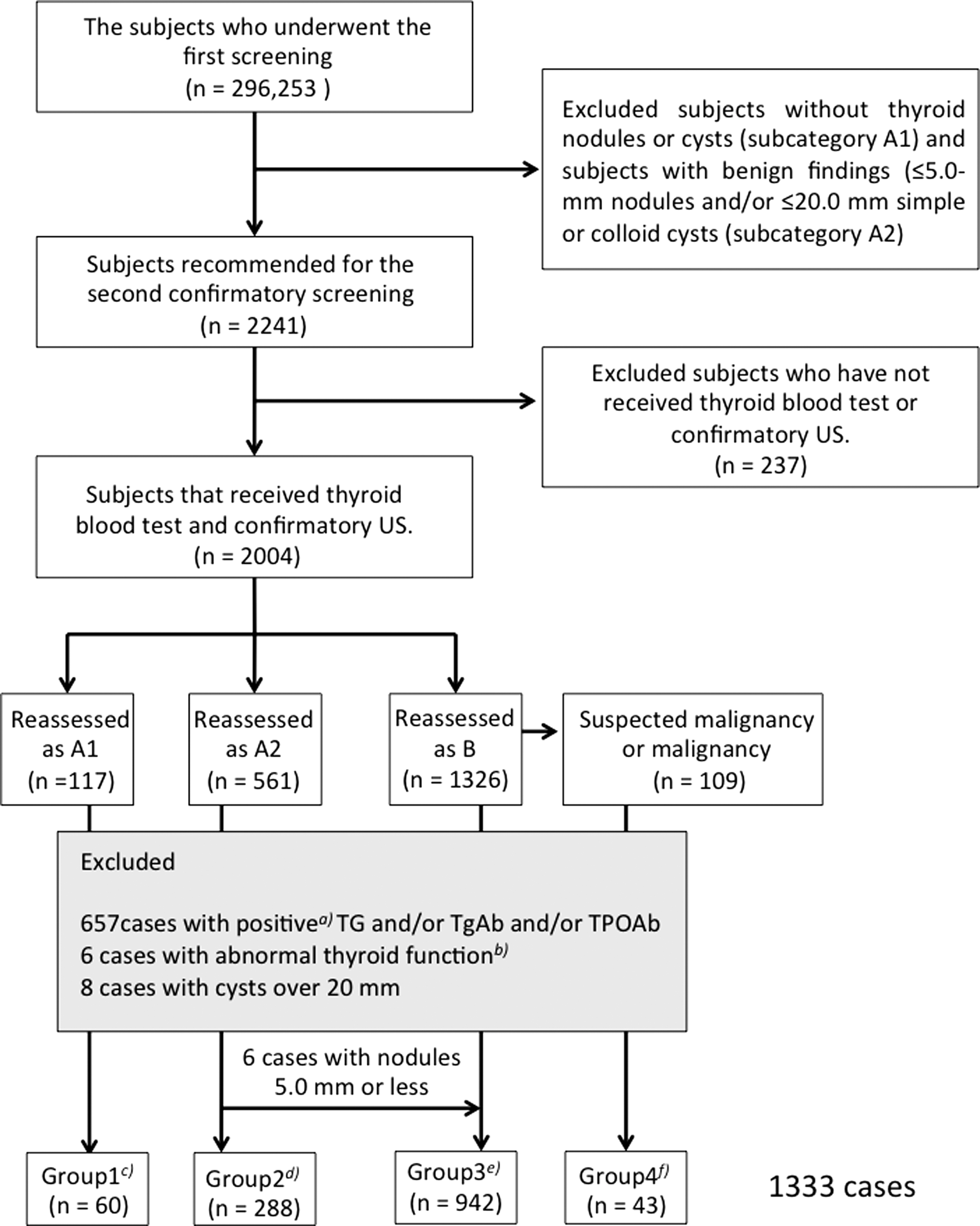
Flow chart of subject selection. A total of 2241 subjects were tentative cases with nodules >5.0 mm and/or cysts >20.0 mm after the first screening of 296,253 subjects as of October 31, 2014. Of these, 2004 subjects received either thyroid blood tests and confirmatory thyroid ultrasound examination. After reassessment of the category, a total of 671 cases were excluded, as shown in lower gray panel. Six cases with nodules of ≤5.0 mm were categorized in Group 3. Subjects with thyroglobulin (Tg) values of <32.7 ng/mL and/or antithyroglobulin antibody (TgAb) of ≤28.0 IU/mL and/or antithyroperoxidase antibody (TPOAb) of <16.0 IU/mL were excluded as positive. Subjects with concentration levels beyond the mean ±3SD (log thyrotropin [TSH] <–1.66 [TSH 0.19 mIU/L] and log TSH >1.94 [TSH 6.96 mIU/L]; free triiodothyronine [fT3] concentration [<2.0 pg/mL and >5.12 pg/mL]; free thyroxine [fT4] concentration [<0.757 ng/dL and >2.73 ng/dL]) were classified as having abnormal thyroid function and excluded. Group 1, cases with neither nodules nor cysts; Group 2, cases with only cysts; Group 3, cases with nodules; Group 4, cases with suspected or pathologically diagnosed papillary thyroid carcinomas (PTCs).
The confirmatory survey involved a precise ultrasound examination using the highest-resolution machine. Then, a final diagnosis was made by specialized physicians who were mostly board-certified medical doctors credentialed by various Japanese medical associations, namely the Japan Thyroid Association, the Japan Association of Endocrine Surgeons, the Japanese Society of Thyroid Surgery, the Japan Society of Ultrasonics in Medicine (JSUM; Seno-thyroidology and General), the Japanese Society of Pediatric Endocrinology, the Japanese Society of Sonographers (JSUM-registered Medical Sonographer, Seno-Thyroidology), and the Japan Association of Breast and Thyroid Sonology (JABTS). In addition, more detailed medical examinations, together with blood and urine analyses, were performed. In these examinations, fT3, fT4, TSH, and thyroglobulin concentrations, as well as TgAb and TPOAb, were measured. Ultrasound screening criteria were used to evaluate whether a thyroid lesion was more likely to be benign or malignant. If an assessment was not possible, the subject was reclassified as A1 or A2, and about one third of the subjects fell into these categories. In the absence of universal ultrasonography diagnostic guidelines for childhood thyroid cancer, the criteria used for adult patients was adapted (2). According to the consensus of the JABTS and the JSUM, fine-needle aspiration cytology is recommended for the following: nodules >5 mm in diameter if strongly suspicious for thyroid carcinoma; those >10 mm in diameter and suspicious for carcinoma; all nodules >20 mm in diameter; and all cystic lesions >20 mm in diameter. Subjects diagnosed with a benign or malignant tumor or suspected malignancy underwent follow-up or surgical treatment. This survey was approved by the ethics review committee of Fukushima Medical University (No. 1318). Written informed consent was obtained from the surveyed subjects' parents.
Study subjects
Among the total of 2051 subjects, 2004 individuals were fully studied to reach a final diagnosis based on thyroid findings and performed blood tests. From these cases, 884 ptients were excluded from Categories B and C for the following reasons: 383 subjects with elevated thyroglobulin (reference range <32.7 ng/mL); 288 subjects with positive TgAb (≤28.0 IU/mL); 205 subjects with positive anti-TPOAb (≤16.0 IU/mL); and eight cases with >20.0 mm thyroid cysts. Also excluded were six subjects with apparent thyroid function abnormalities, such as those with TSH, fT3, or fT4 concentration levels beyond the mean ± 3SD (log TSH <–1.66 [TSH 0.19 mIU/L] and log TSH >1.94 [TSH 6.96 mIU/L]; fT3 concentration <2.0 pg/mL and >5.12 pg/mL; fT4 concentration <0.757 ng/dL and >2.73 ng/dL). A total of 1333 subjects were assessed.
Measurements of serum concentrations of thyroid hormones, TSH, and thyroglobulin, as well as TgAb and TPOAb
fT3, fT4, TSH, and thyroglobulin levels were measured by electrochemiluminescence immunoassay using ECLusys FT3 (reference range 2.13–4.07 pg/mL), fT4 (reference range 0.95–1.74 ng/dL), TSH (reference range 0.340–3.880 IU/mL), and thyroglobulin (reference range <32.7 ng/mL; Roche Diagnostics GmbH, Mannheim, Germany). Radioimmunoassays were used to measure TgAb and TPOAb (Cosmic Co., Tokyo, Japan). The interassay coefficients of variation for the fT3, fT4, TSH, thyroglobulin, TgAb, and TPOAb assays were 4.0%, 6.0%, 4.0%, 2.0%, 4.4%, and 4.5%, respectively. The fT3 (pg/ml)/fT4 (ng/dL) ratio was calculated as an index for the conversion of T4 to T3.
Statistical analysis
IBM SPSS Statistics for Windows v19 (IBM Corp., Armonk, NY) was used for statistical analyses. The nonparametric Spearman's correlation matrix coefficient was estimated between a series of thyroid function tests and age (Fig. 2). Since TSH values were not parametric (Kolmogorov–Smirnov test; p < 0.001), the data were normalized by logarithmic transformation (Kolmogorov–Smirnov test; p = 0.374). Age, log TSH, fT3, fT4, fT3/fT4 ratio, and thyroglobulin levels were compared between the different groups using one-way analysis of variance (Table 1). Statistical methods including analysis of covariance (ANCOVA) to compare the clinical variables, and post hoc analyses were performed with the Bonferroni-corrected significance test, as shown in Figure 4 and Table 2. In the event that Bonferroni-corrected significance was attained, whether concentration differences were categorized in a nodule-dependent fashion was tested. ANCOVA was performed with age as a covariate. p-Values of ≤0.05 were considered statistically significant.
The relationships between age and log TSH (
p-Values of analysis of variance are shown.
Values in parentheses denote females.
Mean ± standard error is shown.
The values expressed in a natural logarithm.
BMI, body mass index; fT3, free triiodothyronine; fT4, free thyroxine; PTC, papillary thyroid carcinoma; TSH, thyrotropin.
Group 1, cases without nodules and cysts; Group 2, cases with cysts; Group 3, cases with nodules; Group 4, cases with papillary thyroid carcinoma.
p-Values refer to analysis of covariance, adjusted for age.
The values expressed in a natural logarithm.
Values in parentheses denote confidence interval.
The values in Group 4 were significantly lower than other three Groups, based on the results of the Bonferroni-corrected significance test as post hoc analyses.
Results
Characterization of thyroid function in subjects with neither nodules nor cysts
Among the subjects who underwent the confirmatory survey, approximately one third (678 cases) had their diagnosis changed. Of these, 60 subjects were eventually diagnosed as having normal thyroid findings. Retrospectively, subjects with intrathyroidal thymus, lymph nodes, ultrasound artifacts, and aberrant vessels were prone to misdiagnosis/overdiagnosis at the time of the first screening. There were inverse relationships between age and each marker (Fig. 2). Log TSH, fT3, and the fT3/fT4 ratio all showed significant age-dependent suppression.
Characterization of thyroid function in the subjects with nodules
Age, body mass index (BMI), serum concentrations of fT3, fT4, and thyroglobulin, the values of log TSH, and fT3/fT4 ratio were compared between the subjects with: no nodules (Group 1), cysts only (Group 2), nodules (Group 3), and suspected or pathologically diagnosed papillary thyroid cancers (PTCs; Group 4). Each mean ± standard deviation (SD) is shown in Table 1. There were significant differences between the four groups in terms of age, log TSH, fT3, and fT3/fT4 ratio. All studied biochemical parameters, except thyroglobulin, decreased as a function of age (Fig. 2). Thus, the focus was on the relationship between each thyroid function level and age in the four groups. As shown in Figure 3A–D, log TSH levels were suppressed age dependently in all four groups. ANCOVA was performed using age as a covariate. There were no interactions between age and group in all determinations studied. The mean ± standard error (SE) after correction and the p-values for the observed differences are shown in Figure 4. A significant difference was observed in log TSH. Figure 4A shows that there were no significant differences in the values of log TSH between Groups 1 and 2. Furthermore, the values in Group 3 were similar to those in Group 4. In contrast, there were apparent differences between Groups 1 and 2 and Groups 3 and 4. These differences were not observed for fT3, fT4, fT3/fT4 ratio, or thyroglobulin concentration.

The relationships between age and thyroid function tests in the groups categorized by ultrasonographic and cytopathological findings. The relationships between age and log TSH in the subjects without nodules and cysts (
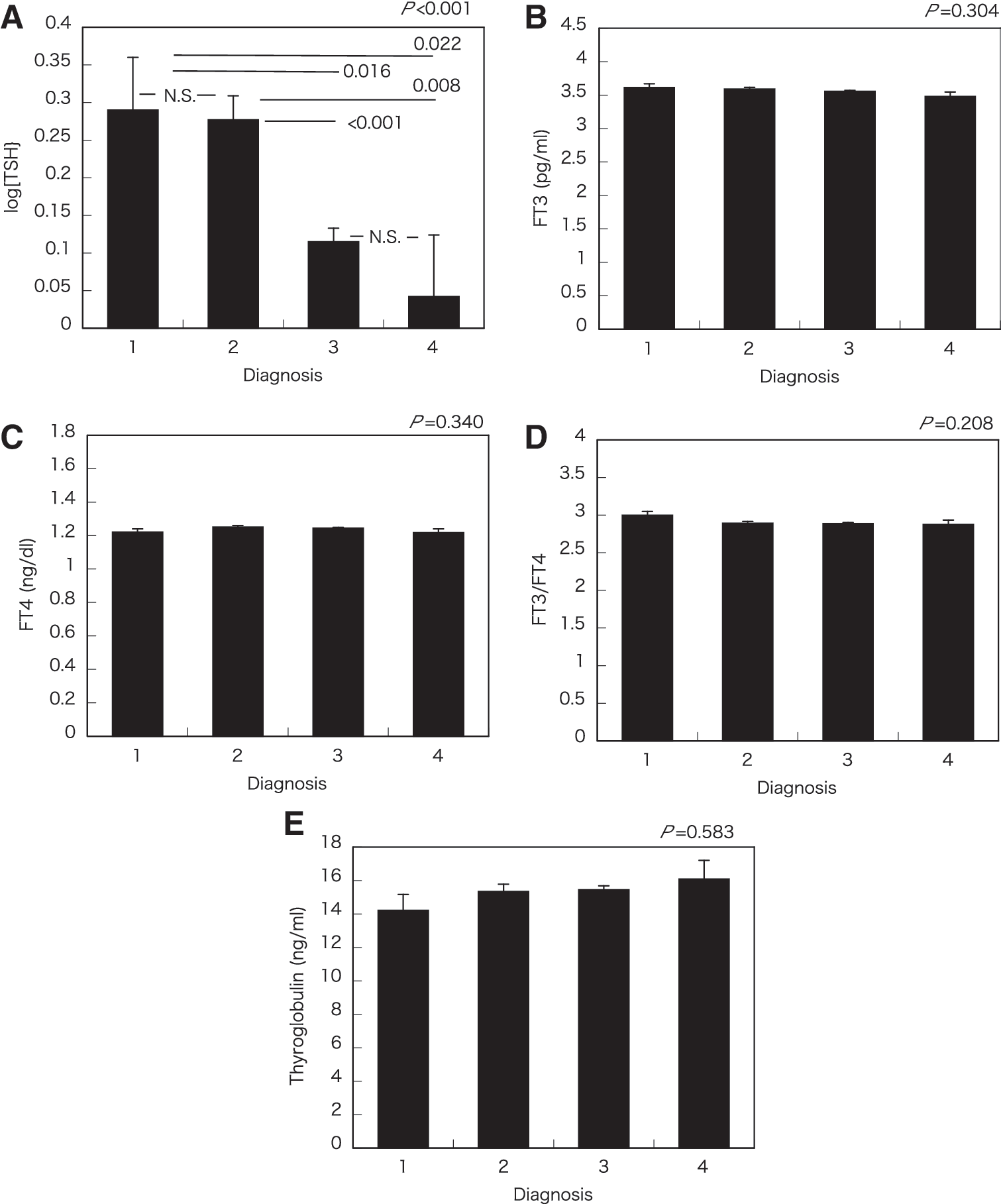
Thyroid function in the various categories. Means ± standard error of log TSH (
Log TSH values were most affected in females, but were not significantly affected in males (p = 0.067; Table 2). fT3 was significantly suppressed among females in Group 4. The values of fT4, fT3/fT4 ratio, and thyroglobulin levels were not affected in any of the categories in either sex.
Discussion
Although thyroid hormone is crucial for the development of the brain during childhood, thyroid function profiles on the laboratory examinations of children are not well known. Since the opportunity to measure thyroid hormone and TSH concentrations in healthy children is uncommon, the normal values have not been determined. In the Fukushima Health Management Survey, the main purpose was to detect nodules to screen for potential radiation-induced cancers in childhood. Approximately 2000 subjects were suspected to have nodules >5.0 mm and/or cysts >20.0 mm after the first screening. They underwent thyroid hormone and TSH concentration measurements, as well as examination of titers of thyroid-related antibodies and thyroglobulin combined with precise thyroid ultrasound examination in the confirmatory survey.
After the exclusion of subjects with positive thyroid-related antibodies, elevated thyroglobulin, apparent abnormal thyroid function, and reclassified diagnoses of nodules and cysts, 60 subjects were reclassified as having no nodules or cysts with normal serum thyroid function tests. All fT3, fT4, and TSH values decreased with age, although there was no significant relationship between fT4 and age (Fig. 2). Several studies have reported normal values of fT3, fT4, and TSH for childhood (3). All three values were suppressed with age in Japan as well as other countries with iodine-insufficient regions, indicating that the present results are consistent with the previously reported results (3).
TSH and thyroid hormone levels are relatively higher in childhood than in adulthood (3). The decrease of TSH without alteration of fT4 with age reported in previous studies suggests that the hypothalamus–pituitary–thyroid (HPT) set point may be altered by age. The ontogeny of the HPT axis, especially that of the negative feedback system, is not well known. However, reports suggest that a system of negative feedback regulation may be initiated at the time of birth in humans (4). The HPT set point may somehow converge at a certain point during childhood. This implies that suppressing TSH levels without alteration of fT4 is a process of maturation of the HPT axis from the immature fetal state. In the present study, fT3 was suppressed with age, resulting in the fT3/fT4 ratio also being suppressed with age. These findings suggest that the conversion of fT4 to fT3 may be suppressed by an age-dependent decrease in deiodinase activity (5).
Negative feedback is a fundamental physiological regulatory mechanism for maintaining hormonal homeostasis in vivo. The serum concentrations of thyroid hormone, fT3, and fT4 are regulated by TSH following stimulation with thyrotropin-releasing hormone; namely, negative feedback regulation in the HPT axis. It is well known that there is an almost linear relationship between the logarithmic TSH value and fT4 concentration in the normal pituitary–thyroid axis (6). In all healthy individuals, there is a unique HPT axis set point, which is mainly determined by various factors, including genetics, aging, sex, and environmental factors (7,8).
Impaired negative feedback mechanisms are occasionally observed in certain illnesses. Serum T3 concentrations decrease without an adaptive increase of TSH in critical illnesses; the so-called low T3 syndrome (9). Such phenomena are probably due to adaptation to critical illness (10). It remains unclear as to whether thyroid nodules affect the HPT axis set point or vice versa. It is believed that serum concentrations of thyroid hormone and TSH are not affected by thyroid nodules unless the nodule is functioning. The relationship between high TSH level and the development of PTC is controversial. Since elevation of TSH is one of the risk factors for developing thyroid cancer in adults, high TSH might predispose to the development of PTC (11 –16). However, one study has reported otherwise (17). In addition, epidemiological examinations have demonstrated elevated thyroglobulin and suppressed TSH levels in patients with PTC (18).
Sensitivity to thyroid hormone may be regulated in an age-dependent manner, since all three determinants (fT3, fT4, and TSH) have been reported to change with age in adults (19). In a previous study of approximately 4000 adult subjects with thyroid diseases, it was demonstrated that there may be sex- and age-dependent regulation of the TSH–thyroid axis (8). In that study, although the subjects were quite heterogeneous, the thyroid hormone response to TSH might have been altered by sex and/or age in the pituitary–thyroid axis. In the Fukushima Health Management Survey, the normal values of fT3, fT4, and TSH were determined based on the measurements of those values in subjects who had undergone the confirmatory examination after exclusion of thyroid autoimmunity. The subjects were those with nodules and/or cysts detected in the confirmatory examination, as previously shown (20).
After correcting for age, the mean log TSH levels in the subjects of the present study with no nodules and subjects with only cysts showed no significant differences. Thus, cysts may not be associated with TSH suppression. In addition, the mean log TSH in subjects with nodules was not significantly different from that of subjects with PTC or suspected PTC. There is a report on the relationship between low TSH levels and thyroid cancers based on an epidemiological study (18). In the present study, the nodules including thyroid cancer were associated with a TSH decrease in childhood. Taken together, these findings suggest that a TSH decrease is a feature associated with both benign nodules and thyroid cancer in childhood.
In the current study, a limited number of the subjects (60 individuals) were reclassified as having no nodules or cysts with normal serum thyroid function tests. This limited sex-specific analyses as well as further intragroup analyses. The log TSH values in each of the categories did not show any significant differences in males, although the p-value was low (p = 0.067), indicating that the number of male samples may not be sufficient to show any significant differences. fT3 levels were significantly suppressed in Group 4 for females only, implying that a low TSH level may induce low T3 in female patients with PTC. The results indicate that TSH suppression may not be due to the elevation of thyroid hormone concentration in at least female patients with nodules. The fT4 and fT3/fT4 ratio values, as well as the thyroglobulin levels, were not affected by any of the categories in either sex, as shown in Table 2.
A suppressed TSH with normal peripheral thyroid hormones defines the entity of subclinical hyperthyroidism, which has several distinct etiologies. It has been suggested that thyroid nodules may be more commonly associated with subclinical hyperfunction, rather than hypofunction, in childhood. Alternatively, nodules or perinodular lesions may leak subnormal amounts of thyroid hormone into the peripheral blood stream, inducing suppression of TSH as a result of subclinical hyperthyroidism. Another possibility is that anti-TSH receptor antibodies (TRAb), rather than TSH, may potentially induce tumor development and hyperfunction, since TRAb stimulate goiter formation. This possibility could not be eliminated, since TRAb levels were not available for the present study. The tumor size of PTC, however, was significantly larger in patients with normal titers of TRAb than in patients with elevated TRAb titers (21), indicating that TRAb may not induce subclinical hyperthyroidism in patients with nodules.
As mentioned above, subclinical hyperthyroidism is one of the interpretations of low TSH levels. fT3, however, was significantly suppressed in female patients with PTC or suspected PTC, indicating that low TSH may be related to hypothalamic–pituitary dysfunction. Numerous reports have suggested that TSH is one of the growth factors responsible for thyroid cancer development, and that TSH suppression therapy is one possible therapy for preventing the recurrence of differentiated thyroid cancer (12). Thus, the possibility that a low TSH without alterations of fT3 and fT4 levels could directly contribute to potential nodule growth appears less plausible. Alternatively, there is a possibility that low TSH and the developing nodules have a common cause, such as polymorphisms and environmental factors. Recent genome-wide association studies have demonstrated several single-nucleotide polymorphisms associated with both thyroid cancer and low serum TSH levels (22,23). These studies reached the conclusion that the gene variants associated with serum TSH concentrations can be divided into two groups: those that confer a risk of thyroid cancer and those that do not (22). Thus, in the present study, genetic background may have been one of the reasons for low TSH levels in the subjects with thyroid nodules.
In conclusion, TSH and fT3 concentrations were suppressed age dependently in childhood. The TSH decrease might be associated with nodule development, including PTC, without overt alterations of fT3 and fT4 concentrations. A nodule itself may play a part in the suppression of TSH, which is not an isolated specific feature of thyroid cancers in childhood. Further elucidation is required, especially with respect to the mechanisms of the relationship between thyroid nodules and the HPT axis.
Footnotes
Acknowledgments
We express our gratitude to all members participating in the Fukushima Health Management Survey. We would also like to thank Ms. Tazuko Kawasaki and Ms. Takako Takahashi for their excellent secretarial assistance.
The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of the Fukushima Prefectural Government.
This survey was conducted as part of Fukushima Prefecture's post-disaster recovery plans and was supported by the national “Health Fund for Children and Adults Affected by the Nuclear Incident.”
Other participating expert committee members, advisors, and staff in The Fukushima Health Management Survey: Kenji Kamiya, Seiji Yasumura, Kenneth E. Nollet, Kumiko Tsuboi, Shiro Matsui, Seisho Tanaka, Masaharu Maeda, Shigeatsu Hashimoto, Keiya Fujimori, Suguru Ishida, Hideto Takahashi, Testuo Ishikawa, Akira Sakai, Michio Murakami, Yuko Hino, Hiroshi Mizunuma, Keiichi Nakano, Hirokazu Okayama, Tomomi Hakoiwa, Chisato Takahashi, Yukari Sato, Ayako Sato, Nobuko Sakuma, Toshie Sakagami, Manabu Ohishi, Norikazu Abe, Masao Kuribara, Masahiko Henmi, Takao Yamahata, Mizuki Sekino, and Yuko Sato.
Author Disclosure Statement
The authors have nothing to disclose. There is no conflict of interest in this study. No competing financial interests exist.