
Abstract
Purpose:
The aim of this study was to determine the rate and significance of TERT promoter mutations that have been recently described in adult thyroid cancer (TC) but not yet in the uncommonly occurring pediatric TC. Furthermore, the role of the BRAFV600E mutation in the clinical outcome of pediatric TC is unknown.
Method:
The study included 55 pediatric (median age 16 years, range 9–18 years; 46 females) and 210 adult TC patients (median age 40 years, range 20–75 years; 155 females) seen during the same time period. DNA was isolated from TC tissues and subjected to direct sequencing. Genetic–clinicopathological correlations were analyzed.
Results:
Only one case of pediatric TC was found to harbor the C228T TERT promoter mutation (1.8%). The C250T mutation was not detected in any of the 55 pediatric TC. In contrast, there was a significantly higher rate of TERT promoter mutations in the adult patients (15.7%, 33/210) compared with the pediatric patients (p = 0.003). In addition, persistent/recurrent TC was seen in 8/12 (66.7%) pediatric patients harboring the BRAFV600E mutation versus 14/41 (34.1%) patients harboring the wild type BRAF (p = 0.05), and when only conventional papillary TC was examined, in 7/9 (77.8%) cases harboring BRAFV600E mutation versus 11/33 (33.3%) cases harboring wild type BRAF (p = 0.025).
Conclusions:
This is the first study on TERT promoter mutations in pediatric TC, which revealed an exceedingly low prevalence, suggesting a limited role of these mutations in pediatric TC. This study also for the first time demonstrates an association of the BRAFV600E mutation with TC recurrence in pediatric patients.
Introduction
D
Over the last decade, major progress in our understanding of the molecular pathogenesis of DTC has been achieved (16). The contribution of genetic mutations in the mitogen-activated protein kinase (MAPK) and PI3K-Akt pathways in the pathogenesis of DTC are now well established (16). BRAFV600E is the most common and well-characterized mutation in papillary thyroid cancer (PTC) (16 –18). Its incidence has been reported to be around 45% of cases on average (17). In the vast majority of studies, the BRAFV600E mutation has been found to be associated with aggressive histopathological features and worse long-term outcome of PTC (18 –21). Although some of those studies included small numbers of pediatric patients, the vast majority of patients were adults. A number of small studies on the genetic mutations were published on pediatric DTC patients. These studies reported a lower frequency of BRAFV600E and its lack of association with aggressive histopathological features and poor outcome of DTC in this age group (22 –25). Therefore, further studies are needed to clarify the frequency and role of BRAFV600E in the pathogenesis of pediatric DTC.
New pathways and genetic alterations are being discovered as additional drivers for the initiation and progression of follicular cell-derived thyroid cancer (TC). These include mutations in the TERT promoter (26,27). TERT is responsible for adding telomeres to the end of the chromosomes to maintain their length, which usually gradually shortens in the dividing somatic cells (28). TERT activity varies in different cells, but is frequently upregulated in many types of cancer cells. This seems to provide cancer cells with increasing survival advantage and contribute to their extended capability of division and longevity (28). There are many mechanisms by which TERT activity is increased in cancer cells (28). Although mutations in the coding regions of the TERT gene are rare, TERT promoter mutations (C288T and C250T) have been found recently to be common in many cancers, including follicular cell-derived TC (29,30). They were also found to be associated with more aggressive types of TC and BRAFV600E mutation (29 –37). These findings have been described exclusively in adult patients with TC. There are no previous studies that examined TERT promoter mutations in pediatric and adolescent TC. Such a study could further support or refute a true biological difference between pediatric and adult TC. This study investigated TERT promoter mutations in a large series of pediatric TC patients, with a comparative examination of adult TC from the same ethnic background. It also examined the BRAFV600E mutation and its relationship with TERT promoter mutations and its association with clinicopathological features and outcomes of TC.
Patients and Methods
Patients
Tumors from 55 non-selected pediatric TC patients were studied (Table 1; median age 16 years, range 9–18 years; 46 females). Nineteen patients were aged 9–13 years, and 36 patients were 14–18 years of age. A cutoff limit of ≤18 years was used to define pediatric TC in accordance with the recent American Thyroid Association Guidelines on the management of thyroid cancer in children (38). The tumors included 43 conventional PTC (CPTC), six follicular variant PTC (FVPTC), one tall-cell PTC (TC-PTC), one diffuse sclerosing PTC, two follicular thyroid cancer (FTC), and two poorly differentiated thyroid cancer (PDTC). Data were extracted from the medical and pathological reports of the patients and the study was approved by the Institutional Review Board. Informed consents were obtained when appropriate.
Some features were not reported for all patients so those numbers reflect the number of patients with available data on the characteristic.
Since BRAF V600E mutation does not occur in FTC and HCC, these subtypes were excluded from the calculations
TC, thyroid cancer; CPTC, conventional papillary thyroid cancer; FVPTC, follicular variant papillary thyroid cancer; TC-PTC, tall cell variant papillary thyroid cancer; HCC, Hürthle cell cancer; FTC, follicular thyroid cancer; DSC, diffuse sclerosing type papillary thyroid cancer; PDTC, poorly differentiated thyroid cancer.
All patients underwent near-total or total thyroidectomy. Central lymph node dissection was done in 16 patients (29%), and central and lateral neck dissection was performed in 35 patients (63.6%). Forty-nine patients (89%) received radioactive iodine ablation 6–12 weeks after thyroidectomy with a median dose of 128 mCi (range 53–210 mCi). They were then treated with L-thyroxine suppression and clinically followed regularly every 6–12 months. Forty-seven patients were in TNM stage I (85.5%), and eight patients had lung metastasis and were in stage II (15%). As a comparison group, TERT promoter and BRAFV600E mutations were also examined in DTC from 210 adult patients (155 females) with a median age of 40 years (range 20–75 years) seen at the same institution during the same period of time (January 2003 to October 2014). There was no difference between the pediatric and adult patients in tumor subtypes, size, multifocality, extrathyroidal extension, distant metastasis, remission rate at 6–12 months after radioactive iodine ablation or initial surgery, and recurrence rate at the last follow-up. However, there was a higher rate of lymph node metastasis in the pediatric group (82.4%) compared with the adult group (56.6%; p = 0.002). The following definitions were used in this study: remission, stimulated thyroglobulin (Tg) ≤1 ng/dL with negative Tg autoantibodies and with negative neck ultrasonography and other imaging studies (when done); persistence, any or a combination of the following findings—stimulated or unstimulated Tg >1 ng/dL, positive ultrasound (US)-guided fine-needle aspiration, suspicious lymph nodes on US, or positive radioactive iodine whole-body scan when done; recurrence, similar to persistence after a period of remission (39).
DNA isolation, polymerase chain reaction, and direct sequencing
The pathological tissue from each patient was examined by an experienced endocrine pathologist (H.A.), and the tumor tissue was carefully dissected from formalin-fixed, paraffin-embedded tissue. DNA was extracted using a commercial DNA extraction kit (QIAamp DNA FFPE Tissue Kit, QIAGEN; Catalog No. 56404) according to the manufacturer's instructions. DNA was quantified using a nanodrop2000 spectrophotometer (Thermo Scientific), and DNA purity was assured by the A260/280 ratio, with a ratio ≥1.8 indicating a good purity DNA. Polymerase chain reaction (PCR) and direct sequencing using Big Dye terminator v3.1 cycle sequencing reaction kit and an ABI PRISM 3730XL genetic analyzer (Applied Biosystems) were used to detect TERT promotor mutations using the same primers and PCR conditions as previously described (30). The presence of a BRAFV600E mutation was examined by amplifying and sequencing exon 15 of the BRAF gene using previously described primers and PCR protocol (30).
Statistical analysis
Continuous data were summarized as median and range or mean ± standard deviation (SD), and a t-test was used for significance analysis. Categorical data were expressed as numbers and percentages or ratios, and Fisher's exact and chi-square tests were used for significance analysis. In all statistical tests used, a two-tailed p-value of <0.05 was considered significant.
Results
Demographic and clinicopathological characteristics
The initial demographic and clinicopathological characteristics of the 55 pediatric and 210 adult patients with TC are summarized in Table 1. Other than the significantly younger age and higher prevalence of lymph node metastasis in the pediatric patients compared with the adult patients, there was no difference in other clinicopathological characteristics between the two groups (Table 1).
TERT promotor mutations
Of the 55 pediatric DTC (Table 1), only one case (Fig. 1A) with CPTC had a C228T TERT promoter mutation (1.8%). The patient was a 10-year-old boy with a 4 cm CPTC showing no evidence of multifocality or extrathyroidal invasion and no lymph node or distant metastasis. He was treated with total thyroidectomy and central neck dissection followed by radioiodine therapy with 58 mCi 131I. His postoperative 12-month evaluation showed complete remission, and he continued to be in remission over the next five years of follow up. All other 54 tumors were negative for this mutation. There were also no C250T TERT mutations in any of the 55 pediatric TC.
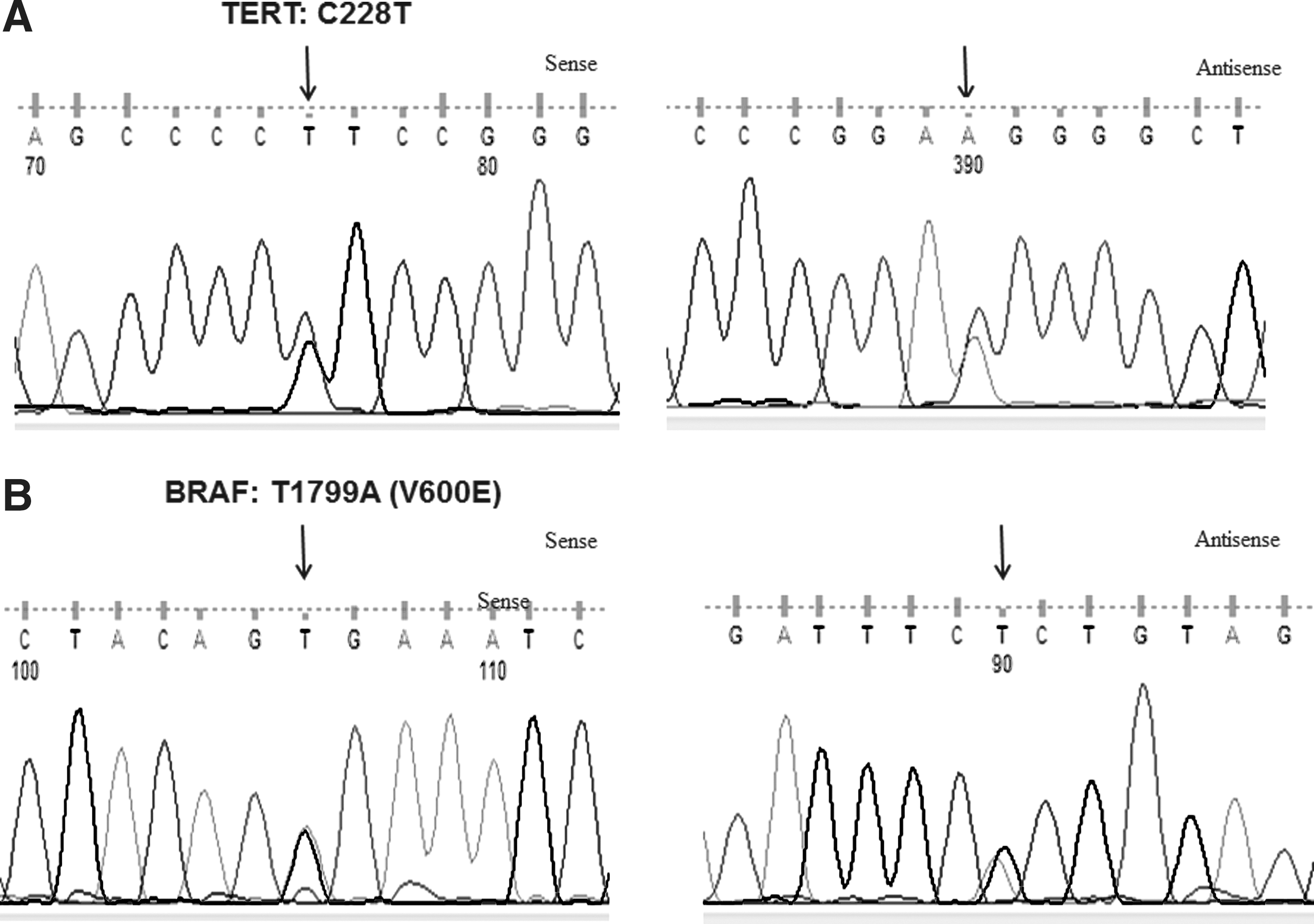
Chromatograms showing (
In the 210 adult patients (Table 1), the C250T TERT promoter mutation was detected in six patients (2.9%), the C228T TERT promoter mutation in 27 patients (12.9%), and the two TERT promoter mutations collectively in 33 patients (15.7%). This rate was significantly higher than that in the pediatric group (p = 0.003).
BRAFV600E mutation
Excluding cases of FTC and Hürthle cell cancer in which the BRAFV600E does not normally occur, a BRAFV600E mutation (Fig. 1B) was present in 12/53 pediatric TC (22.6%). The BRAFV600E -positive tumors were CPTC (11 cases) and a TC-PTC (one case). In the adult patients, a BRAFV600E mutation was detected in 98/204 tumors (48.0%), which was significantly more common compared with the pediatric group (p < 0.001; Table 1).
TERT and BRAFV600E mutations concurrently or exclusively occurring in TC
TERT and BRAFV600E mutations concurrently occurred in 20 cases (9.5%) of adult patients and in none of the patients in the pediatric groups (Table 1). Similarly, TERT or BRAFV600E mutations occurred in 111 cases of the adult group (52.9%) and in only 13 patients (23.6%) of the pediatric group (p < 0.001).
BRAFV600E mutation is associated with a high persistence/recurrence rate of pediatric TC
Comparing tumors harboring a BRAFV600E mutation with those with wild type BRAF in the 55 pediatric patients revealed no difference in tumor size, multifocality, extrathyroidal invasion, lymph node metastasis, distant metastasis, and rate of persistent disease at 6–12 months after primary surgery or radioactive iodine ablation (Table 2). However, there was a significant difference in the rate of persistent/recurrent disease between the two groups at the last follow-up (median follow-up period 6.7 years, range 1.5–11.7 years). Specifically, persistent/recurrent disease was seen in 8/12 (66.7%) patients harboring the BRAFV600E mutation versus 14/41 (34.1%) patients with wild type BRAF (p = 0.05; Table 2). This difference became even more significant (Table 2) when the analysis was limited to CPTC, in which BRAFV600E is a characteristic mutation, showing that persistent/recurrent disease occurred in 7/9 (77.8%) patients harboring a BRAFV600E mutation compared with 11/33 (33.3%) patients with wild type BRAF (0.025). Except for one TC-PTC, which was positive for a BRAFV600E mutation, all other cases harbored wild type BRAF, and therefore similar analysis for an association between BRAFV600E mutation and persistent/recurrent disease could not be performed.
Discussion
Despite an increasing incidence of TC in children, it remains a relatively rare cancer. This has contributed to the limited data on many aspects of this pediatric cancer. Although it has long been considered similar to TC in adults, several studies have demonstrated significantly different clinicopathological features and outcomes of pediatric TC compared with adults (6 –12). Many case series have suggested more aggressive features at the time of presentation, with an increased tendency for extrathyroidal invasion, lymph node and distant metastasis, and a higher propensity for persistent/recurrent disease (7,8,11 –13). The reasons for these differences in clinicopathological features between pediatric and adult TC might be due to factors extrinsic to the tumors themselves. For example, it is possible that the tumor microenvironment is different in pediatric patients compared with adults (40). Similarly, immunity might be more active in pediatric patients, and this may induce stronger interactions between the tumor and microenvironment with resultant aggressive features but might also lead to subsequent containment of the TC and result in better outcomes. Interestingly, despite these aggressive features at the time of diagnosis, disease-specific mortality is exceedingly rare (7,41). This suggests that pediatric TC might be different in its behavior from TC in adults, and this merits further studies, particularly in terms of elucidation of the molecular pathogenesis.
There are limited data on the molecular basis of pediatric TC. The BRAFV600E mutation is the most common mutation in adult PTC (16). However, its prevalence in pediatric PTC has been variable (22,23,42,43). In most studies, the frequency of this mutation is lower than that in adult patients. Penko et al. studied 14 sporadic cases of PTC in the 10–21-year age group, and none of them was found to have a BRAFV600E mutation (42). Kumagiai et al. examined PTC from Japanese pediatric patients without history of irradiation and 15 tumors from post-Chernobyl childhood PTC (43). A BRAFV600E mutation was found only in one (3.2%) PTC in the former group and in none of the latter group (43). Rosenbaum et al. studied 20 PTC from patients aged 10–17 years at the time of diagnosis and found mutations in only 20% of them (44). They noticed an increasing prevalence of the BRAFV600E mutation with increasing age (44). A much higher frequency of the BRAFV600E mutation has recently been reported by Henke et al. (24). Using restriction fragment length polymorphism (RFLP) analysis, they examined 27 PTC in patients <22 years of age and found a BRAFV600E mutation in 63% of their patients (24). It is noteworthy that the RFLP technique is not as accurate as the direct sequencing method, which is the gold standard, and this may have led to a falsely higher rate of BRAFV600E mutation. In another recent study, Givens et al. used a pyrosequencing method and detected the BRAFV600E mutation in 7/19 DTC (36.8%) examined from patients in the age range 2.8–18 years (23). The present study also found a lower rate of the BRAFV600E mutation in pediatric PTC (21.8%) compared with adults (43.4%). The fact that the frequency of the BRAFV600E mutation in adults in the current study is similar to the average BRAFV600E frequency in other studies suggests that this low prevalence of the BRAFV600E mutation in this pediatric patients is not due to ethnic differences and is consistent with the previously reported low prevalence of the BRAFV600E mutation in the pediatric population.
In most studies, BRAFV600E has been associated with more aggressive histopathological features and worse clinical outcomes in adult patients (17,19 –21). The present study found no significant association between the BRAFV600E mutation and tumor size, tumor multifocality, extrathyroidal invasion, lymph node and distant metastasis, and the TNM stage (Table 2). However, there was a borderline significant association between the BRAFV600E mutation and tumor persistence/recurrence at the last follow-up in this pediatric group of patients. This association became even more significant when the analysis was limited to CPTC in which BRAFV600E is a characteristic mutation (Table 2). The association of the BRAFV600E mutation with PTC recurrence in this pediatric patient cohort was interestingly most significant at the last follow-up visit. One explanation is that disease recurrence of PTC takes time and thus the manifestation of the effect of the BRAFV600E mutation on PTC recurrence can be seen only after certain time. In the present study, the last follow-up time provided the longest observation time to capture recurrent disease and thus the effect of a BRAFV600E mutation would be best seen at this point. This result is consistent with previous findings suggesting that the different recurrence rates between PTC with the BRAFV600E mutation and wild type BRAF in adult patients became progressively more pronounced as the follow up time was prolonged (45). Although specific supportive data are not available, the BRAFV600E mutation-induced impairment of radioiodine avidity, as initially shown in adult patients (18), is likely also a cause of the increased PTC recurrence in this pediatric cohort. This is the first such observation in pediatric PTC. Previous studies did not show such an association (23,24). It is possible that this lack of an association in previous studies is due to the small sample size in these studies.
TERT C288T and C250T promoter mutations have recently been reported to be common in TC in patients from North America and Europe, with a prevalence of 10–15% (26,29 –35,37). These mutations were more common in poorly differentiated and anaplastic thyroid cancers and were associated with more aggressive features of TC (29,30). Further studies showed a synergistic effect of these mutations with the BRAFV600E mutation in terms of poor clinicopathological outcomes of PTC (33,36,37).
No previous study has assessed the frequency of TERT promoter mutations in pediatric TC. The present study is the first to screen a relatively large number of pediatric TC for these mutations and found them to be exceedingly uncommon. To assess whether this low frequency of TERT promoter mutation is a feature of the current ethnic population or is specific to the pediatric TC, a large sample of adult patients from the same ethnic background was tested for TERT promoter mutations. In this adult group, the prevalence of TERT promoter mutations was found to be similar to those reported from North America and Europe, suggesting that the much lower frequency of TERT promoter mutations in the pediatric TC is a real pediatric-specific phenomenon. This conclusion is also supported by the observation of a significantly lower frequency of the BRAFV600E mutation in the pediatric patients compared with adults, which is similar to the findings in other ethnic populations as discussed above. The extremely low frequency of TERT promoter mutations in pediatric TC demonstrated in this study suggests a limited role of such mutations in pediatric TC. The low prevalence of TERT promoter mutations as well as the low prevalence of the BRAFV600E mutation is consistent with the known fact that pediatric TC is different from adult TC in clinicalopathological behaviors (9,10,12,46). The present finding of a low prevalence of TERT promoter mutations in the pediatric patients is in line with the reports that TERT promoter mutations are more common in older adult than younger adult TC patients (30,33 –35).
In summary, this is the first study on TERT promoter mutations in a pediatric cohort of TC. It revealed an exceedingly low prevalence of such mutations, in contrast to the relatively high prevalence of these mutations in adult TC, suggesting that TERT promoter mutations have a limited role in pediatric TC. This study, with its relatively large size, also demonstrates for the first time an association of the BRAFV600E mutation with disease recurrence of PTC in pediatric patients, suggesting a potential prognostic role of this mutation in pediatric TC as in adult TC.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.