
Abstract
Background:
Thyroid carcinoma is the most common endocrine malignancy and has an increasing incidence. High-frequency ultrasound (HFUS) has a spatial resolution of 30 μm, which is a property that has been exploited for thyroid visualization and analysis in mice. The aim of this study was to generate a novel orthotopic mouse model of human follicular thyroid carcinoma (FTC) using an HFUS-guided injection system.
Methods:
Twenty Balb/C nude mice were injected in the right lobe of the thyroid with 2 × 106 FTC-133 cells using the microinjection HFUS-guided system, and 20 mice, used as a control, underwent surgical orthotopic implantation of 2 × 106 FTC-133 cells in the right lobe of the thyroid. All mice underwent HFUS imaging two weeks after cell injection; HFUS examinations and tumor volume (TV) measurements were repeated weekly. Micro–computed tomography was performed at different time points to determine whether lung metastasis had occurred. TVs were compared between the two models (surgical vs. HFUS-guided) using the Mann–Whitney U-test, and the Mantel–Cox log-rank test was applied to evaluate the death hazard. Hematoxylin and eosin analysis of formalin-fixed, paraffin-embedded mouse tissue was performed to validate the in vivo imaging results.
Results:
Of the HFUS-guided injected mice, 9/18 survived up to 40 days after the injection of tumor cells. Mice injected surgically had 100% mortality at day 29. Of 38 mice, 29 (14/18 HFUS, 15/20 surgical) showed metastasis in the salivary glands and lymph nodes, and 13 (10/18 HFUS, 3/20 surgical) also showed metastasis in the lungs, which was confirmed by histological analysis. In the surgical group, there was an evident, frequent (12/20 mice) involvement of the contralateral lobe of the thyroid, whereas this feature was only detected in 1/18 mice in the HFUS group. Statistical analysis showed the same pattern of growth in the two groups, and a significant hazard in the mice in the surgical group (p = 0.03).
Conclusions:
This study demonstrated the technical feasibility of an HFUS-guided orthotopic mouse model of FTC. The HFUS-guided orthotopic model is easily reproducible and allows prolonged monitoring of the disease because the animals showed an increased survival rate.
Introduction
T
In recent years, considerable efforts have been made to develop genetically engineered xenograft and orthotopic mouse models of thyroid carcinoma in order to study the effectiveness of drugs (3,4,9). Subcutaneous xenograft models are technically simple, reproducible, and cost-effective. However, they differ in the original tumor microenvironment (4,10 –13). The use of genetically engineered mice in preclinical studies can be limited by the length of the time needed to develop tumors, the high costs of model establishment, and rare reproducible distant metastasis (14). Orthotopic tumor models are more cumbersome to develop, but they allow cell growth directly in the organ of origin and can recapitulate metastatic behavior with sufficient penetrance and reproducibility (4,10 –14).
High-frequency ultrasound (HFUS) is widely employed as a non-invasive method for imaging anatomic structures in mouse models of disease (15 –18). HFUS has the ability to detect structures as small as 30 μm, which is a property that has been exploited for thyroid visualization and analysis in mice (19). This study describes the use of HFUS to inject FTC-133 cells directly into the murine thyroid to develop a novel orthotopic model of FTC, and this method is compared to a surgical procedure.
Materials and Methods
Cell culture
The human FTC cell line FTC-133 was purchased from the European Collection of Cell Culture (Sigma-Aldrich, St. Louis, MO) and cultured in vitro at 37°C and 5% CO2 in a humidified incubator. FTC-133 cells were seeded at 1–5 × 10,000 cells/cm2 in a 10 cm diameter culture dish (Corning-Falcon, Corning, NY) and grown without antibiotics in Dulbecco's modified Eagle's medium (DMEM; Invitrogen, Carlsbad, CA) and high glucose, supplemented with 10% fetal bovine serum (FBS; Invitrogen) and 2% Glutamax (Gibco-Life Technologies, Waltham, MA). For in vivo inoculation, 2 × 106 cells (90–95% viability) were detached from each culture dish using a 2.5% Trypsin-EDTA solution (Sigma-Aldrich), and the cells were resuspended in DMEM without phenol red (Gibco-Life Technologies; Ref. 21063-029) and serum to obtain 2 × 106 cells in 20 μL. This concentration and volume were used to prevent cellular lysis that could interfere with the injection of cells, while DMEM without phenol red was used to avoid possible interference of the pigment in the histological analysis.
Tumor implantation
The animal protocols used in this work were evaluated and approved by the Animal Use and Ethic Committee (OBA) of CEINGE, Biotecnologie Avanzate (Naples, Italy; Protocol 15/2/14_n 3). They are in accordance with Federation of European Laboratory Animal Science Associations (FELASA) guidelines and the guidelines defined by the European Communities Council directive (2010/63/EU). Forty Balb/C nude six-week-old female mice were purchased from Charles River Laboratories International, Inc. (Wilmington, MA), and were allowed to acclimate for one week before beginning the experiments. All of the procedures described here were performed under general anesthesia with isoflurane in oxygen (induction phase: isoflurane 5% in oxygen 0.8 L/min; maintenance phase: isoflurane 1.5% in oxygen 0.8 L/min). From the 13th day after the injection of tumor cells, gel diet water (99% of water ionized 10 kGy) and gel diet energy (SAFE, Scientific Animal Food & Engineering, 2biological instruments, Besozzo, Italy) were left on the floor of the cages to avoid excessive weight loss in the mice. Furthermore, when an animal showed any sign of dehydration, sterile saline solution and/or 5% glucose solution (30 mL/kg body weight) were injected subcutaneously once per day. Mice that appeared to be cachectic (body weight reduction of 25%) were sacrificed.
HFUS-guided orthotopic thyroid injection
HFUS equipment, specifically Vevo 2100 (VisualSonics Inc., Toronto, Canada), with a multifrequency (22–55 MHz) probe (MicroScan™ MS550D, VisualSonics Inc.) was used in all procedures. Each mouse (n = 20) was positioned in dorsal recumbency on the handling table of the Vevo imaging station (Vevo Integrated Rail System III; VisualSonics Inc.), and a thick pad of warm gel was placed over the ventral aspect of the neck to provide a coupling medium for the transducer. Once the thyroid gland was identified (Fig. 1A) in the transverse plane, following the indications of Mancini et al. (19), the syringe (1 mL Norm-Ject®; Henke-Sass, Wolf GmbH, Tuttlingen, Germany), which was mounted on the injection mount of the Vevo Rail System, was slowly advanced until the needle tip entered the field of view, and its position was adjusted using the micro-manipulation mechanical controller. The syringe was prefilled with 2 × 106 cells in ∼20 μL DMEM without phenol red and without serum (Gibco-Life Technologies) and mounted on a 27G × ¾″ (20 mm) needle (NN-2719R, Terumo® Neolus®; Terumo Europa N.V., Leuven, Belgium). When the needle was in contact with the skin, the skin was gently stretched with non-traumatic dissecting forceps to allow needle advancement in the soft tissue surrounding the thyroid gland. The needle was further advanced using the micro-manipulation controls until the tip was within the thyroidal parenchyma; at this point, the cells were gently injected (Fig. 1B). Mice were left to recover from anesthesia, as previously described.
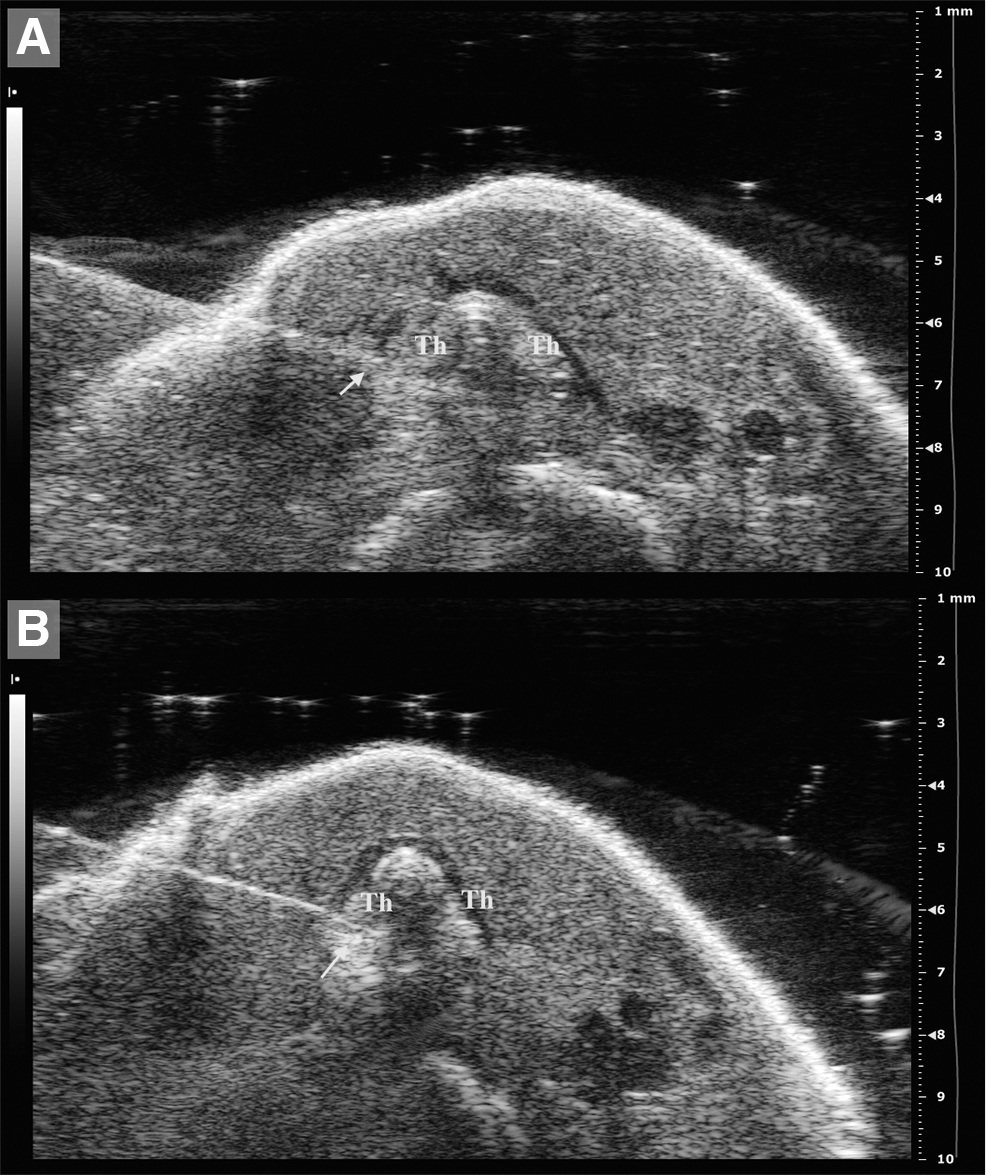
High-frequency ultrasound (HFUS)-guided injection methodology. (
Surgical orthotopic thyroid implantation
Twenty mice underwent surgical orthotopic implantation of thyroid tumor cells, as described in previous studies (4,9). Mice were given general anesthesia and were positioned under a dissecting microscope. After surgical preparation of the skin, a midline ventral cervical incision was made. The salivary glands were reflected laterally and held in position with mosquito forceps, the central component of the neck was exposed, and the overlying strap muscles were bluntly dissected to reveal the thyroid gland adjacent to both side of the trachea. Direct injection into the right thyroid gland was completed with 2 × 106 cells in ∼20 μL DMEM without phenol red (Gibco-Life Technologies) and without serum using a 0.5 mL syringe with an integrated 30G × 5/16″ needle (Omnican® 50; B. Braun Melsungen AG, OPM, Melsungen, Germany). Only the right lobe of the thyroid was injected; the left side of the thyroid was not manipulated and was used as a control. Following the injection, the salivary glands were repositioned over the anterior neck, and the incision was closed using 6-0 absorbable sutures (Coated Vicryl™; Johnson & Johnson Ethicon, LLC, Parma, Italy) in a simple continuous pattern. A double antibiotic ointment (Cicatrene®; Johnson & Johnson s.p.a., Rome, Italy) was applied over the surgical incision, and the mice were placed under a warming lamp during recovery from anesthesia.
The same operator, a veterinary doctor with >10 years of experience in micro-surgery and molecular imaging, performed the surgical and HFUS procedures. Mice were checked daily for signs of postoperative complications (hematoma, stridor, etc.).
HFUS imaging and data collection
Two weeks after injection (day 13), all mice underwent HFUS imaging. All tumors were scanned on both the transverse and the sagittal plane, and height, width, and length were recorded. Tumor volume (TV; mm3) was calculated according to the ellipsoid formula: height × width × length × π/6 at day 13, 22, and 27 after tumor cells injection. The HFUS examinations were repeated at different time points from day 4 to follow up tumor growth, invasiveness, and any other change in the morphology of the neck.
Micro–computed tomography
Each mouse (n = 40) was subjected to micro–computed tomography (micro-CT) imaging at day 22 and then at any time a mouse showed signs of suffering to assess whether lung metastasis occurred. Micro-CT was performed under general anesthesia, as previously described, with the scanner Explore Locus (GE Healthcare, Manchester, United Kingdom) using the following parameters: 80 K X-ray tube voltage, 450 μA X-ray tube current, scan technique 360°. A 20-minute scan with a spatial resolution of 45 μm was performed. Images were reconstructed using the Microview-software analysis of the Explore locus.
The resulting raw data were reconstructed to a final image volume of 875 × 875 × 465 slices at (93 μm3) voxel dimensions. The reconstructed slices were output in the CT manufacturer's raw format and were corrected to the Hounsfield units. The images were exported as DICOM and re-evaluated with OsiriX v.5.9 64-bit (Pixmeo Sàrl, Switzerland).
Histopathology
Tissue samples collected from all the mice were fixed for 48–72 hours in 10% neutral-buffered formalin. Samples were subjected to a light one-day standard decalcification procedure before being embedded in paraffin using a commercial electrolytic decalcifying solution, Biodec R (Bio-Optica, Milan, Italy). Fixed and decalcified mouse samples were trimmed with a cross-section of the trachea at the point where the thyroid and parathyroid glands meet and placed into cassettes for histologic processing. Histopathology evaluation was performed on hematoxylin and eosin (H&E) stained, 5 μm-thick tissue sections of the thyroid, regional lymph nodes, and lungs. H&E evaluation was performed using an Olympus BX 41 microscope. The sections of murine neck of both HFUS and surgical mice were examined by histology.
Statistical analysis
Statistical analysis was performed using commercially available computer programs (JMP® v8.0, SAS Institute, Inc., Cary, NC; Prism® v6.0, GraphPad Software, Inc., La Jolla, CA). Tumor volume data are reported as the mean ± standard error of the mean (SEM). Normality of data distribution was tested with Shapiro–Wilk's W-test. A multivariate analysis of variance (MANOVA) was applied to study the effect of time and the interaction between time and the type of technique on tumor growth. The TVs were compared between surgically and HFUS-guided injected mice, at any time point, using a Mann–Whitney's U-test. The Mantel–Cox log-rank test was used to compare the survival distributions of the two groups, and a Kaplan–Meier survival curve was created. For all tests, significance was set at p < 0.05.
Results
There were no anesthetic or procedural complications in any of the orthotopic FTC mice with either HFUS-guided implantation or the surgical procedure. Both procedures were well tolerated by the animals, and there was no post-procedure mortality.
The HFUS-guided procedure, including orthotopic cell injection and induction of and recovery from anesthesia, had a duration of approximately seven minutes, whereas the surgical procedure and the complete recovery of the mice from anesthesia had a mean duration of 13 minutes.
In the HFUS group, accurate placement of FTC-133 cells in the right thyroid lobe was evident in 18/20 (90%) mice. In 2/20 (10%) mice, the primary tumor developed in the salivary gland. These mice were excluded from TV analysis but were further analyzed for pulmonary metastasis assessment with a micro-CT scan. The contralateral lobe was not affected by any echostructural abnormality (Fig. 2A and B) in 17/18 (94%) mice, with only 1/18 (5.5%) of the mice showing bilateral involvement of the thyroid lobes. These findings were confirmed by H&E analysis (Fig. 2C). No ultrasound sign of thyroid inflammation, as free fluid around the injected lobe or hypo-anechoic foci within the gland, were seen at four days post-injection (data not shown).

(
In the surgical group, during the procedure, part of the inoculum escaped the right thyroid gland and was visible on the surgical field. All exceeding fluids were absorbed with a sterile cotton swab. No signs of infection or surgical complications were detected in any of the mice. Bilateral involvement of thyroid lobes was detected in 12/20 (60%) mice, whereas monolateral cancer development was recorded in 8/20 (40%) mice. H&E analysis showed obvious infiltrates in the strap muscles and salivary glands (Fig. 2F).
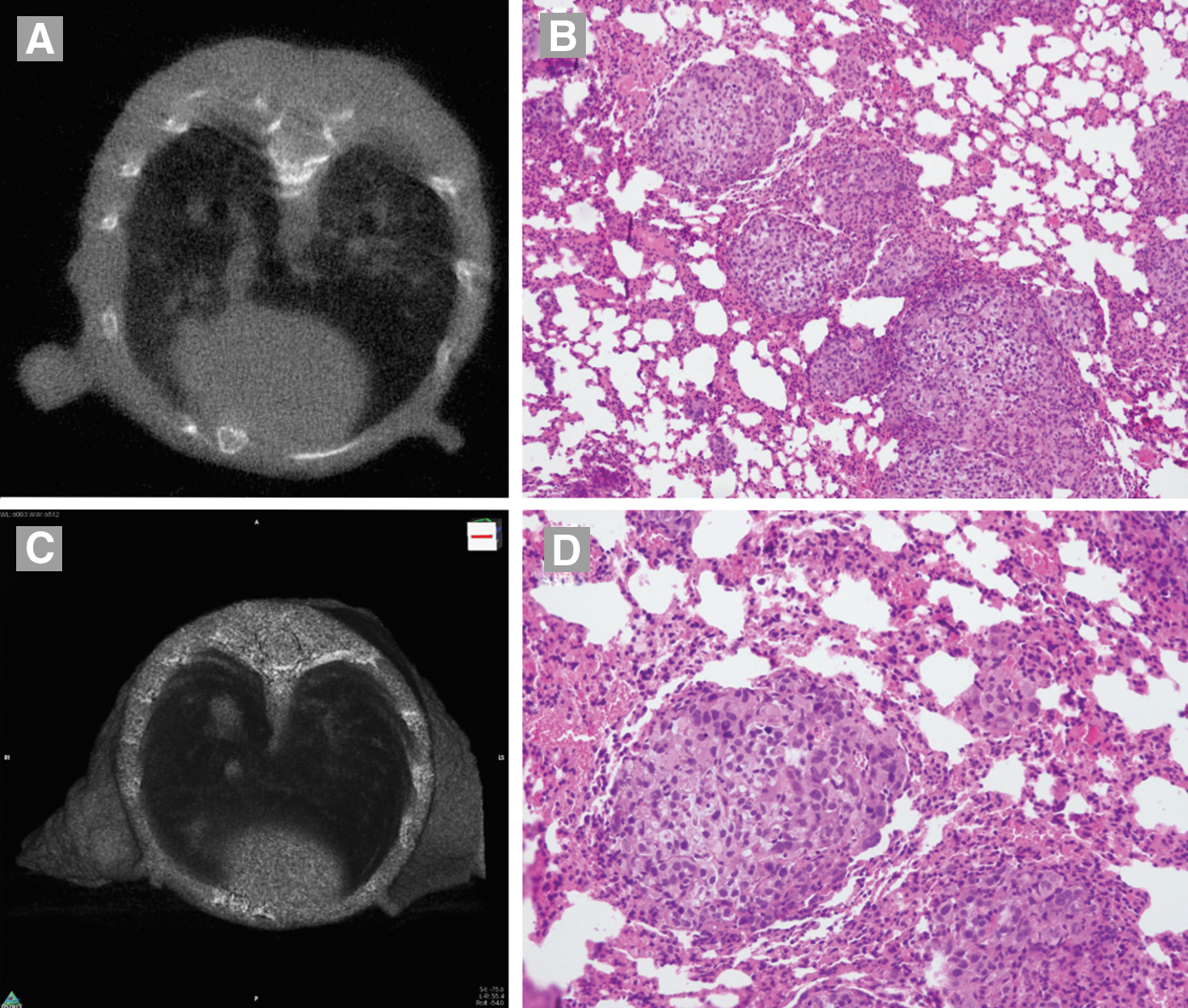
In the HFUS group, metastases in the salivary gland and regional lymph nodes were evident in 14/18 (78%) mice from day 13 after tumor cell injection. Pulmonary metastases were detectable in 10/18 (55%) mice at day 34. In particular, pulmonary metastases were found in 4/18 (22%) mice at day 29 and in an additional 6/18 (33%) mice at day 34 (Fig. 3A). Representative H&E staining of the lung showed multiple metastatic nodules with highly aggressive cancer cells characterized by the presence of high pleomorphism (Fig. 3B). High magnification images of the HFUS group of the primary tumor and pulmonary metastases are shown in Supplementary Figure S1 (Supplementary Data are available online at
(
In the surgical group, metastases in the salivary gland and regional lymph nodes were evident in 15/20 (75%) mice from day 13. Micro-CT analysis showed lung metastases in 3/20 (15%) mice at day 29 (Fig. 3C). These lung samples showed the same histopathological and micro-CT features described for the mice with HFUS-guided tumors (Fig. 3C and D). Mice in the surgery group began to show cachexia and poor health conditions at day 20; none survived after the 29th day after tumor cell injection.
Cachexia or at least poor health condition developed in all the mice included in the study, albeit at different time points, and ultimately required euthanasia in all cases. Pathological features detected in the HFUS and surgical group, as well as survival rates, are summarized in Table 1.
Bilateral involvement of thyroid lobes after two weeks.
Lung metastases after four weeks.
Lung metastases after five weeks.
HFUS, high-frequency ultrasound.
TVs recorded in the two groups are shown in Table 2. A small goiter was clearly visible in all mice in both groups at day 13. The MANOVA showed a significant effect of time on TVs (p = 0.002), whereas neither the effect of group nor the interaction of time on the group was significant (Fig. 4). This was confirmed by the comparison of mean TVs between groups (Table 2), which did not demonstrate a significant difference at any time point. The Mantel–Cox test showed a significant hazard for the surgical group compared with the HFUS-guided group (p = 0.03; Fig. 5).

Graphic representation of the growing rate of the two orthotopic models (MANOVA). The red line represents the mice injected by HFUS, and the blue line represents mice injected by surgery.
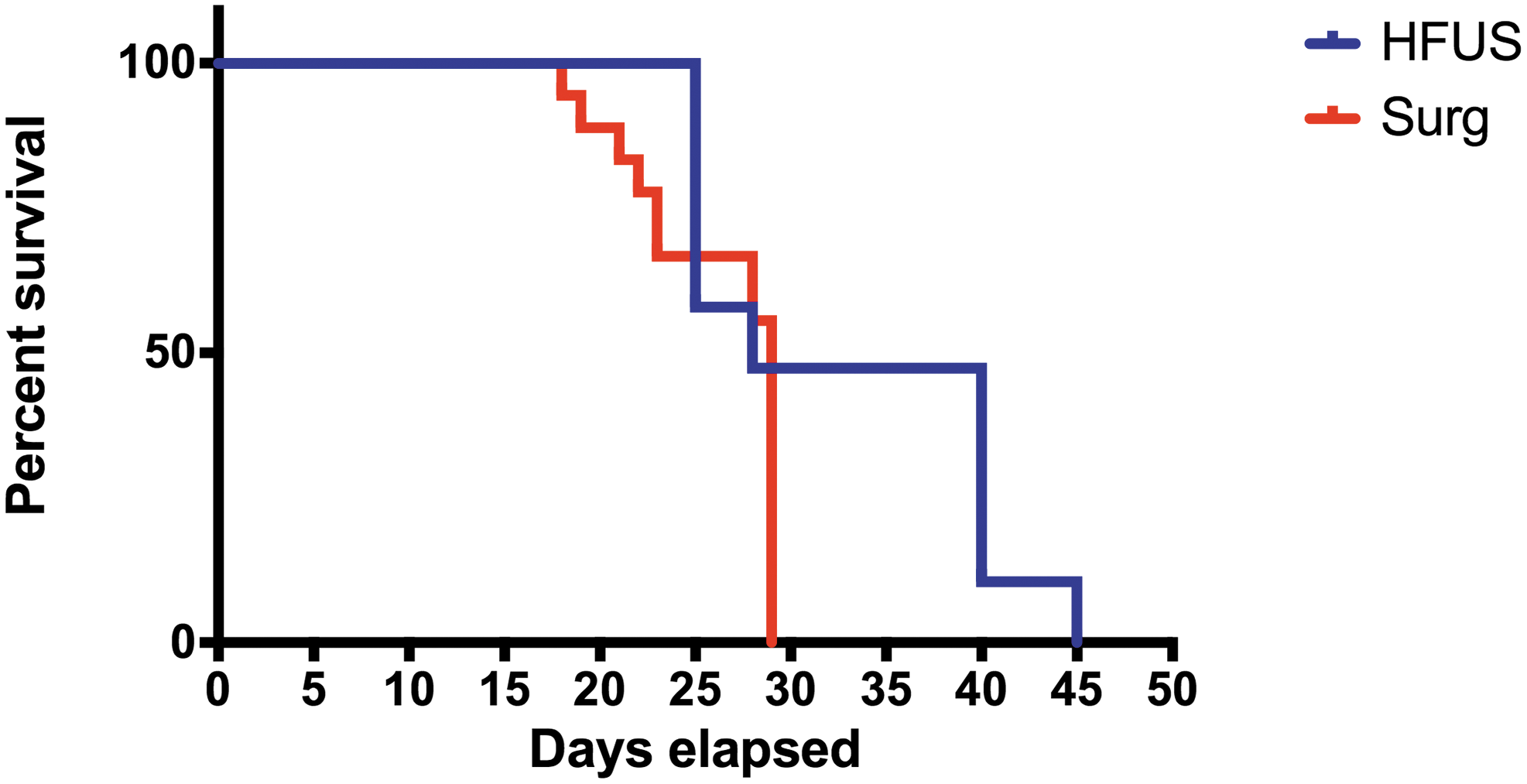
Graphic representation of the Kaplan–Meier survival curve. The blue line represents the mice injected by HFUS, and the red line represents mice injected by surgery.
Data are reported as mean ± SEM.
TVs, tumor volumes.
Discussion
Thyroid cancer is one of the few cancer types with increasing incidence, particularly among women (3). Surgery and/or radioiodine therapy are effective against local differentiated carcinomas, but the choices for successful treatment are limited for dedifferentiated, invasive, or metastatic thyroid cancers. FTC likely metastasizes via the vascular system to distant organs and is less likely to take up therapeutic radioactive iodide (5,7). Having a reliable and reproducible animal model of thyroid cancer is an important step in the testing and development of novel therapeutics. Most models for FTC were established based on the genetic alterations discovered in human tumors (20). Transgenic models are valid systems for preclinical tests to evaluate the feasibility, efficacy, and safety of new therapies against thyroid cancer, but one obstacle is the high costs related to transgenic mice compared with orthotopic models. Furthermore, the development of new drugs often requires a high number of animals for testing (21). There is also a widespread use of subcutaneous tumor models, especially in therapeutic screening studies. Although these xenograft models are easy to produce, and the progression of tumors can be easily monitored, increasing evidence indicates that the xenograft models might not be adequate for the prediction of a clinical response. As assessed by other authors, a more convenient and less expensive approach would be desirable to assess tumor formation (21). Orthotopic models of thyroid cancer are an important tool in developing novel therapeutics because they more closely reflect the biological and morphological features of cancer growth and metastasis in humans, and they will better predict potential clinical activity (4,14,22,23). Orthotopic model have been created for surgery, and a new, non-invasive, and more effective system using HFUS has been developed.
The modern focus in experimental research is to find alternatives to in vivo research and, if that is not possible, to make experimental techniques in laboratory animals as minimally invasive as possible according to the principles of the 3Rs: replacement, reduction, and refinement. Today, the 3Rs are increasingly seen as a framework for conducting high-quality science experiments in the academic and industrial sectors. The aim of the present study was to demonstrate the feasibility of HFUS-guided injection of thyroid cancer cells for the generation of a novel orthotopic mouse model. The results reported in this study show that the technique was successfully applicable, easy to reproduce, and non-invasive with regard to animal well-being.
Mice included in this study were followed longitudinally for at least 29 days, and HFUS allowed a non-invasive precise characterization of the thyroidal tumor evolution, as confirmed by histopathology analysis.
The HFUS-guided procedure was practical and feasible with a high degree of precision, indicated by the fact that only 2/20 mice had cells injected in the salivary glands and 1/20 of the mice had bilateral involvement of the thyroid lobes. The surgical procedure showed a higher degree of local aggressiveness, and bilateral invasion of the thyroid lobes was detected in 12/20 mice. The latter result might be explained by the fact that it was necessary to dissect the strap muscles to inject the tumor cells, which creates dead-space pockets that can lead to the diffusion of the cells in the contralateral thyroid lobe. This diffusion has to be attributed to the surgical procedure and not to a metastatic involvement of the contralateral thyroid lobe, as confirmed by the fact that the bilateral tumor was detected at the same moment in the two lobes as soon as HFUS imaging was performed. The present findings are similar to those in previous publications related to orthotopic thyroid carcinoma models. Furthermore, both the higher volume injected (20 μL in the present experiments vs. 10 μL in the others) and the different cell line and cell number need to be taken into consideration when evaluating the current results (4,9,23). FTC-133 are large fibroblastoid cells, and the minimum volume of medium needed for their survival was 20 μL. Thus, it is possible that the combination of the surgical dissection with the consequent creation of pockets and dead spaces, and the large volume of the inoculum, could explain the wider local invasion recorded in the surgical group.
The TVs were larger in the HFUS-guided procedure compared with the surgical one, but the difference did not reach statistical significance. Even if the power of the statistical test to detect this difference was far from 80%, it was not within the aims of the study to demonstrate any substantial disproportion in tumor growth between the two techniques. Nonetheless, the tumor only grew linearly in the HFUS group. This different trend might be due to the higher local spread of the tumor cells during the surgical implantation and to the large volume of the inoculum used.
Concerning the metastasis formation at four weeks, the surgical groups displayed 3/20 (15%) pulmonary metastases, whereas the HFUS group showed 4/18 mice with pulmonary metastasis (22%). This difference was not statistically significant (p = 0.67). However, it would be difficult to infer what would have happened if the mice in the surgical group had survived as long as the HFUS mice.
The HFUS-guided procedure has some advantages: it is faster, animals are not subjected to surgery and post-surgery stress, and a lower relative hazard was found with a longer time of survival and better health conditions of the mice for a longer period. Moreover, even though the HFUS-guided procedure does not require high surgical skill, it does require a period of training to acquire the technique, as well as a dedicated device.
In conclusion, this novel HFUS-guided orthotopic model is technically feasible and easily reproducible, and might serve as an effective tool in preclinical studies of novel anticancer therapies. It would also be desirable to use the same technique for the administration of drugs within the lesion in future experiments, and further studies will be conducted to assess the feasibility of an ultrasound-guided therapy approach.
Footnotes
Acknowledgments
This work was supported by grants from RRC-2014-2354542 Ricerca Corrente and GR-2010–2314003 Italian Ministry of Health (MoH).
Author Disclosure Statement
No competing financial interests exist.