
Abstract
Background:
Programs initiated to prevent iodine deficiency disorders (IDD) may not remain effective due to changes in government policies, commercial factors, and human behavior that may affect the efficacy of IDD prevention programs in unpredictable directions. Monitoring and outcome studies are needed to optimize the effectiveness of IDD prevention.
Summary:
Although the need for monitoring is compelling, the current reality in Europe is less than optimal. Regular and systematic monitoring surveys have only been established in a few countries, and comparability across the studies is hampered by the lack of centralized standardization procedures. In addition, data on outcomes and the cost of achieving them are needed in order to provide evidence of the beneficial effects of IDD prevention in countries with mild iodine deficiency.
Conclusion:
Monitoring studies can be optimized by including centralized standardization procedures that improve the comparison between studies. No study of iodine consumption can replace the direct measurement of health outcomes and the evaluation of the costs and benefits of the program. It is particularly important that health economic evaluation should be conducted in mildly iodine-deficient areas and that it should include populations from regions with different environmental, ethnic, and cultural backgrounds.
Iodine Deficiency Prevention Programs Have to Be Monitored
J
Although the need for monitoring is compelling, the current reality in Europe is less than optimal. In a recent review (5), Lazarus pointed out that in the previous two years, fewer than 50% of European countries had performed monitoring studies. Indeed, Europe is highly fragmented with respect to IDD prevention and monitoring programs and only a few countries regularly and systematically assess their IDD prevention programs (Fig. 1). In Latin America, only 4/22 countries regularly monitor their IDD prevention programs (4).
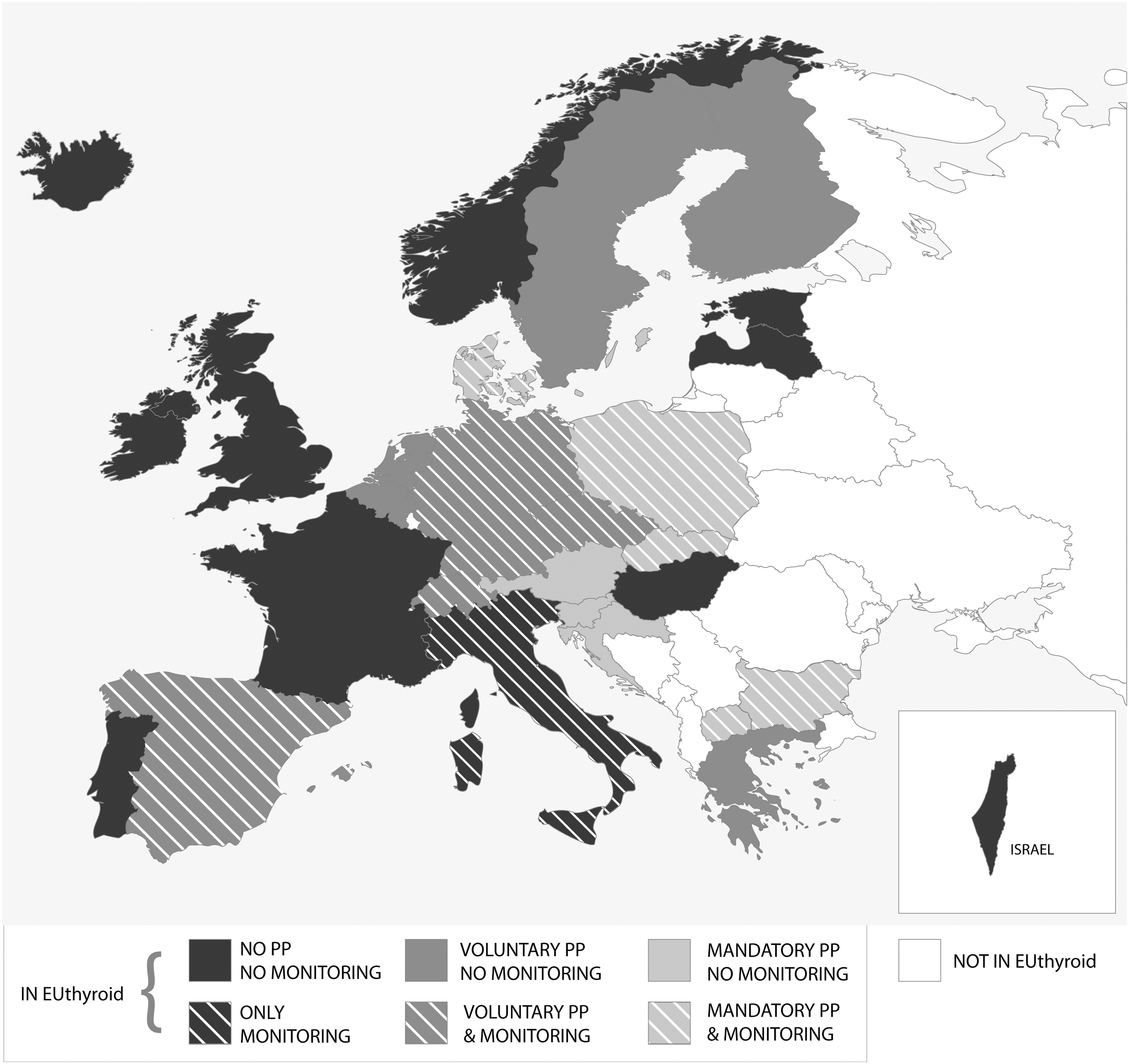
Heterogeneity in iodine deficiency disorders (IDD) prevention programs (PP) and monitoring in Europe.
As physicians, we know about the importance of monitoring treatment, especially in the therapy of chronic diseases. For example, we would call it medical malpractice not to monitor blood pressure after initiating antihypertensive therapy.
For IDD prevention programs, in some respects, the patient is effectively the population. Of course, we do not treat the population with iodine as a drug in the classical sense, as IDD prevention programs intervene in a careful way, to augment natural human nutrition.
As is the case in patients under treatment, IDD prevention programs have to be monitored in populations. The obvious intention of such programs is to improve the iodine supply to individuals in a population. The Iodine Global Network (IGN) recommends a mean daily iodine intake of 150 μg from 10 years of age, which equates to a target range of median urinary iodine concentration (UIC) of 100–199 μg/L (6).
The simplest method of assessing iodine intake is to ask individuals about their nutritional habits. Unfortunately, calculating the average iodine intake based on questionnaires gives only a rough estimate because of the recognized limitations of dietary-intake data. Furthermore, databases on the iodine content of foods (which varies from region to region) might be inadequate. Indeed, very few countries have national databases that include the iodine content of foods (7,8). Particular challenges arise from dairy products, which play an increasing role in iodine intake in many countries (9). Varying farming practices with respect to iodine feeding of dairy cows may lead to large and previously unregulated and even unnoticed shifts in iodine intake of populations that may be unobserved when only questionnaire-based studies monitor IDD prevention.
Studies that seek to measure UIC directly face another challenge: gold standard methods for measuring UIC levels such as inductively coupled plasma-mass spectroscopy are costly and highly sophisticated, resulting in their infeasibility for most studies (10). Some alternative methods show good correlation with the best (11), but results from different methods and laboratories may vary considerably. In general, UIC analysis is demanding, and it requires well-trained and experienced laboratory personnel. Participation in an external quality assessment program is helpful in making valid UIC measurements. Many laboratories performing iodine measurements participate in the Ensuring the Quality of Iodine Procedures (EQUIP) program of the U.S. Centers for Disease Control and Prevention (12).
For studies that assess iodine intake by self-reported dietary intake or through direct UIC measurements in a spot-urine sample, intra-individual variability because of day-to-day variation in intake and hydration status are factors that must be considered. Assuming a random variation, UIC measurements from spot samples can be relied upon for sufficiently large study populations. The examined group should include at least 100 study participants and should ideally use urinary creatinine to correct for hydration status (13). Alternatively, intra-individual variation can be addressed by repeated measurements in selected study participants (14).
In schoolchildren, the net effect of iodine consumption can be assessed by measuring the thyroid size. The mean thyroid volume and goiter prevalence will decrease over time if iodine supply becomes sufficient after an IDD prevention program has been established. Thus, repeated cross-sectional studies including thyroid ultrasound may indicate the beneficial effects of an improved iodine supply in populations.
How Valid Are International Maps of Iodine Status?
Numerous World Health Organization and IGN publications provide maps illustrating the current status of iodine supply across regions (15,16). Epidemiological researchers usually put much effort into the standardization of their data, leading to a good internal validity of single surveys or trend studies performed by single centers. However, external validity is sometimes hampered by using different nutritional questionnaires or protocols, applying different UIC measurement methods, and by the heterogeneity of ultrasound measurements, which may be unfavorably influenced by different devices, probes, or observers (17).
Mapping thyroid-related parameters across countries and regions requires highly comparable absolute values, but comparability may be severely limited by the aforementioned methodological issues and low external validity of single studies. Thus, a multinational iodine survey with centralized standardization and quality assurance would be very helpful in mapping regional disparities in iodine supply. For Europe, population studies such as the proposed European Health Examination Survey (18,19) may offer a good option for monitoring UIC levels, but neither thyroid examinations nor UIC measurements will be integrated.
For the analysis of regional differences in thyroid volume and goiter prevalence, further factors should be considered. Besides iodine supply, there are other important factors that may vary between regions and influence the individual goiter risk. For example, cigarette smokers, particularly those living in iodine-deficient regions, have a higher risk of goiter (20), and second-hand smoking may influence thyroid-related parameters in schoolchildren (21). The prevalence of tobacco consumption varies considerably between populations (22). Thus, the region-specific proportion of smokers and different smoking habits may modify the associations between iodine supply and the prevalence and incidence of thyroid diseases in different populations. When interpreting goiter maps, other common risk factors for thyroid disorders should also be considered, including socioeconomic (23), environmental (24,25), genetic (26,27), metabolic (28), and sex-specific factors (20,29). All may vary across populations, regions, ethnicities, religions, and cultures, and represent possible explanations for discrepancies between iodine status and goiter prevalence.
Monitoring Is Not Enough—Evaluation Is Needed
Some of the lessons given by Dunn and others have been learned by now. There are many iodine fortification and supplementation programs across the world, and epidemiological studies assess these programs in many countries (30). Some of these studies estimate the iodine intake by food questionnaires, while others directly measure UIC excretion in population samples. The aim is to see median UIC levels of between 100 and 200 μg/L, while the proportion of subjects presenting UIC levels <50 μg/L or >300 μg/L should be kept as low as possible; this will give reassurance that the IDD prevention program is adequate.
But is this conclusion correct?
One of the key lessons young physicians are taught in their clinical career is that they should never treat on the basis of laboratory values alone. Indeed, laboratory data may have been affected by pre-analytical circumstances or by the measurement method itself. A value outside a reference range does not necessarily mean that the patient is sick, and conventional reference values established from cross-sectional studies are of limited prognostic significance (31). Finally yet importantly, the focus of any treatment is on achieving a healthy outcome and lower risk for the patient.
With respect to hypertension, for example, physicians have to be aware that the ultimate aim of antihypertensive treatment is not to lower blood pressure. Rather, the major goal is to reduce the risk of hypertension-related cardiovascular outcomes; lowering the blood pressure is only the bridge to reach this goal. Of course, controlling the blood pressure under therapy is a useful tool for its high predictive value for cardiovascular risks, but it is only a surrogate of the major goal. Consequently, evaluation of the treatment goals is required. In hypertensive patients, evaluation of hypertension-related end-organ damage is recommended on a regular basis (32).
The major goals of IDD prevention programs in populations must be borne in mind, that is, reducing the prevalence and incidence of cretinism and adverse effects on neurocognitive function in children in addition to minimizing the risk of goiter, thyroid nodules, and thyroid dysfunction in adults. The increase of iodine nutrition in populations only serves as a bridge to this goal (Fig. 2).
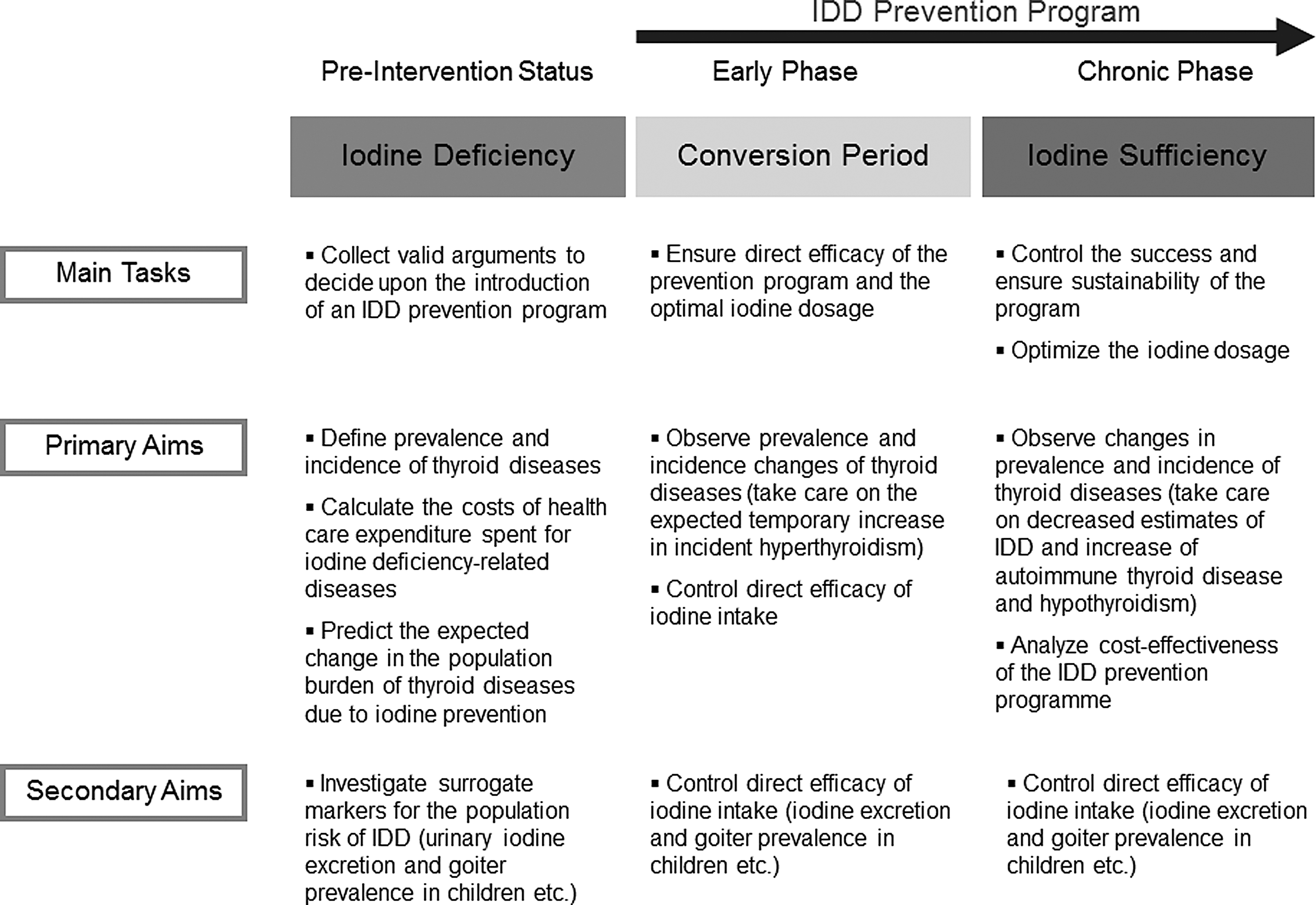
Primary and secondary aims of IDD PP and tasks for monitoring and outcome research.
A huge amount of research has provided strong evidence that improved iodine status in severely iodine-deficient regions will achieve this aim (33,34). As justifiably convincing as these benefits may be in general, it can be easy to forget that data are also needed from mildly-to-moderately iodine-deficient regions in order to provide evidence that IDD prevention is also effective in those regions. Indeed, little research has been published on outcomes, including changes in prevalence and incidence of clinical thyroid disease and treatment, following the implementation of iodine fortification programs in mildly iodine-deficient regions (35 –37).
Recent studies suggest that neurocognitive function in children may be impaired if pregnant women are exposed to even mild iodine deficiency (38). This finding needs to be further substantiated (39), since even only small changes in the mean population IQ may affect the economy and well-being of societies (40).
May Iodine Harm Populations?
Young internists learn early in their clinical career that the more effective the drug therapy, the more likely that unintended side effects will occur. As physicians, we are obliged to prevent harm in our patients. Thus, we have to be aware of potential side effects, especially when using highly effective therapies.
Increasing the iodine supply has beneficial effects on thyroid health, but does it have side effects? An increased incidence of hypothyroidism may be the price we have to pay for preventing IDD. An improved iodine supply is associated with increased median circulating thyrotropin (TSH), an increased incidence of hypothyroidism (41 –44), and an increased use of thyroid hormone replacement therapy within the population (45). But is this really a side effect of IDD prevention programs?
Although a number of studies (41 –43,45) indicate that the answer is “yes,” there are alternative physiological explanations (46). A higher iodine intake induces inhibitory effects on cellular processes involved in thyroid hormone synthesis and secretion (47 –49). Consequently, higher TSH levels are necessary to maintain normal thyroid hormone release, which can also be observed at the population level. In iodine-sufficient regions, median TSH levels are higher than are those in iodine-deficient regions (50). Since reference ranges strongly depend on the distribution of TSH levels in the general population, the TSH reference range is also shifted toward higher values after the iodine supply of a population has improved. Unfortunately, TSH reference ranges used to define thyroid dysfunction are rarely adjusted to the current level of iodine intake in populations. Therefore, applying the same reference ranges before and after introducing IDD prevention programs, which is often the case in clinical practice and epidemiological research, may result in an overestimation of the prevalence and incidence of hypothyroidism, which should not necessarily be interpreted as a side effect of IDD prevention programs.
These considerations may particularly explain findings from countries that have carefully increased iodine supply to median UIC excretion levels of around 100 μg/L. If median UIC reaches much higher levels (e.g. ≥300 μg/L), an increased incidence of hypothyroidism may indeed be related to an increasing population incidence of autoimmune thyroiditis due to iodine oversupply.
During antihypertensive therapy, we are sensitive to possible side effects of the drugs used. We know when to interrupt the therapy with a specific agent and to switch to another one if the first one appears to harm our patient. However, to assess an IDD prevention program as successful, we lack predefined criteria on the prevalence or incidence of hypothyroidism that is acceptable during IDD prevention. Likewise, no recommendations are available on the tolerable extent and duration of hyperthyroidism (33,36,51) that may be temporarily observable after initiation of an IDD prevention program.
Outcome Research Is Needed to Evaluate IDD Prevention Programs
Of note, in comparison to the huge number of UIC measurements in populations, there are very few studies available that compare the prevalence or incidence of hyper- and hypothyroidism in populations that have IDD prevention programs (52). The benchmark for this approach is the DanThyr project (45,53), which commendably combines repeated cross-sectional and cohort studies with analyses of registry data. More projects like DanThyr and disease-registry data are urgently needed to determine what outcomes can safely be tolerated under IDD prevention programs (Table 1).
IDD, iodine deficiency disorders.
Do Not Ignore the Costs
Prevention programs have to be beneficial for individuals and societies. To allocate limited resources efficiently in healthcare systems is one of the major aims of prevention. For example, for Germany, it was estimated that €1 billion was allocated annually to clinical practice for IDD management before the national IDD prevention program was established (54). Some studies of projected healthcare costs have estimated that IDD prevention programs can be highly beneficial and cost-effective (54,55).
Meanwhile, many IDD prevention programs have been established, but of particular note, there is currently no comprehensive analysis available that evaluates the cost-effectiveness of any of these programs. Not only must the benefits be considered but also the putative side effects of iodine fortification, both temporary and chronic, as well as the related need for monitoring. Such cost-effectiveness analyses will be essential for meaningful discussion with health authorities in countries that have remained mildly or moderately iodine deficient (30) or that are considering switching from voluntary to mandatory prevention programs.
Conclusions
To reiterate Dunn's assertion (1), “It is not enough to implement IDD prevention programs, it is also vital to stabilize such programs over time.” To this end, iodine intake and UIC levels, as determined by population representative studies, can be used as surrogate markers to monitor the effectiveness of IDD prevention programs. To the extent that we ensure quality control of the methodology over time, such studies are well suited to assess the effect of change in iodine supply in populations subjected to IDD prevention programs and to uncover unintended outcomes in the course of such programs.
But we can do better!
Monitoring studies can be optimized by including centralized standardization procedures to improve the comparability across studies. No study of iodine consumption can replace the direct measurement of health outcomes and evaluation of the program costs and benefits. Health economic evaluation should specifically be conducted in mildly iodine-deficient regions and should include populations from regions with different environmental, ethnic, and cultural backgrounds. Findings from outcome studies will help us fine-tune the right level of IDD prevention programs specific to each population that is subjected to such programs. Finally, outcome research at an international level will have been achieved. Such evidence is needed to motivate the remaining iodine-deficient countries to join the fight for eradication (30).
Footnotes
Acknowledgments
This work was supported by EUthyroid. The project has received funding from the European Union's Horizon 2020 research and innovation program under grant agreement number 634453.
Author Disclosure Statement
There are no conflicts of interest.