
Abstract
Background:
Thyroid nodules and cancers are rare in children compared with adults. However, after the 1986 Chernobyl Nuclear Power Plant accident, a rapid increase in childhood thyroid cancer was observed. To avoid any confusion and misunderstanding of data obtained in Fukushima after the 2011 nuclear accident, baseline prevalence of thyroid nodules and cancers should be carefully assessed with standardized criteria systematically, and comprehensively applied to the population perceived to be at risk.
Aims:
Under the official framework of the Fukushima Health Management Survey, the thyroids of children in Fukushima were examined using ultrasound, and the results collected in the first four years after the nuclear accident were analyzed in order to establish a baseline prevalence of childhood thyroid abnormalities, especially cancer.
Subjects and methods:
Of 367,685 people aged 18 years or younger as of April 1, 2011, who were living in Fukushima Prefecture at the time of the accident, 300,476 underwent thyroid ultrasound screening. Of those, 2108 subjects with thyroid nodules were further examined using an advanced ultrasound instrument, with standardized criteria applied to determine the need for fine-needle aspiration cytology (FNAC). FNAC results determined the need for surgery and histological confirmation of the cytological diagnosis.
Results:
Of the 2108 rescreened subjects, 543 underwent FNAC, of whom 113 were diagnosed with malignancy or suspected malignancy. Subsequently, 99 patients underwent surgical resection, revealing 95 cases of papillary thyroid cancer, three poorly differentiated cancers, and one benign nodule. The overall prevalence of childhood thyroid cancer in Fukushima was determined to be 37.3 per 100,000 with no significant differences between evacuated and non-evacuated areas. Thyroid cancer patients had external exposure estimates of <2.2 mSv during the first four months.
Conclusions:
The high prevalence of childhood thyroid cancer detected in this four-year study in Fukushima can be attributed to mass screening. It clearly exceeds what is found incidentally anywhere else. Direct comparisons with any other results, even those from cancer registries, are not meaningful because of differences in methodology.
Introduction
T
Since then, it has become the focus of public and professional attention whether the FDNPP accident would cause radiation-associated cancers, especially thyroid carcinomas, among exposed young individuals. Mass screening using thyroid ultrasonography and aspiration cytology has been performed on children and adolescents, even in the absence of symptoms, as part of the Fukushima Health Management Survey, in order to establish a baseline childhood thyroid cancer prevalence, to be followed by lifetime surveillance (2,3).
A comprehensive review by the United Nations Scientific Committee on the Effects of Atomic Radiation conducted on the 20th anniversary of the Chernobyl NPP accident indicated that the main adverse health effect of radiation involved a substantial rise in thyroid cancer incidence among exposed young people, starting at four to five years after exposure (4,5). By 1995, 10 years after the event, the incidence of childhood thyroid cancer reached 4/100,000 per year, approximately 80- to 130-fold higher than the prior rate of 0.03–0.05 cases per 100,000 per year in Belarus. A latency of about three to four years was followed by a linear increase for at least six years (6). However, meaningful comparisons are often complicated by differences in diagnostic criteria and instrumentation, such as cancer registry surveillance versus deliberate mass screening. It is therefore essential to understand that the annual incidence of thyroid cancer among Japanese adults without screening is 2.4–4.5 males and 8.5–12.4 females per 100,000 person-years (7), but comprehensive screening of children and adolescents using advanced ultrasound technology is not comparable, as such mass screening has no precedent. It cannot be said that the clinical characteristics of childhood thyroid cancers detected by mass screening (asymptomatic) are the same as those of symptomatic cases diagnosed in other healthcare settings. However, it is known that children often have a better prognosis, even in cases of invasive tumors, and a higher frequency of extrathyroidal spread and higher recurrence rate than those found in adults (8). Thus, although screening without clinical indication is controversial for adult thyroid cancer, it was implemented for children to address fear and anxiety about an increased risk of thyroid cancer among Fukushima residents, whose excessive radiation exposure was deemed to be much lower than that of comparable populations affected by the Chernobyl NPP accident.
This study reports the first round of thyroid ultrasound examination survey results obtained over four years following the FDNPP accident, in order to establish a baseline prevalence of childhood and adolescent thyroid pathology in Fukushima.
Subjects and Methods
Study design
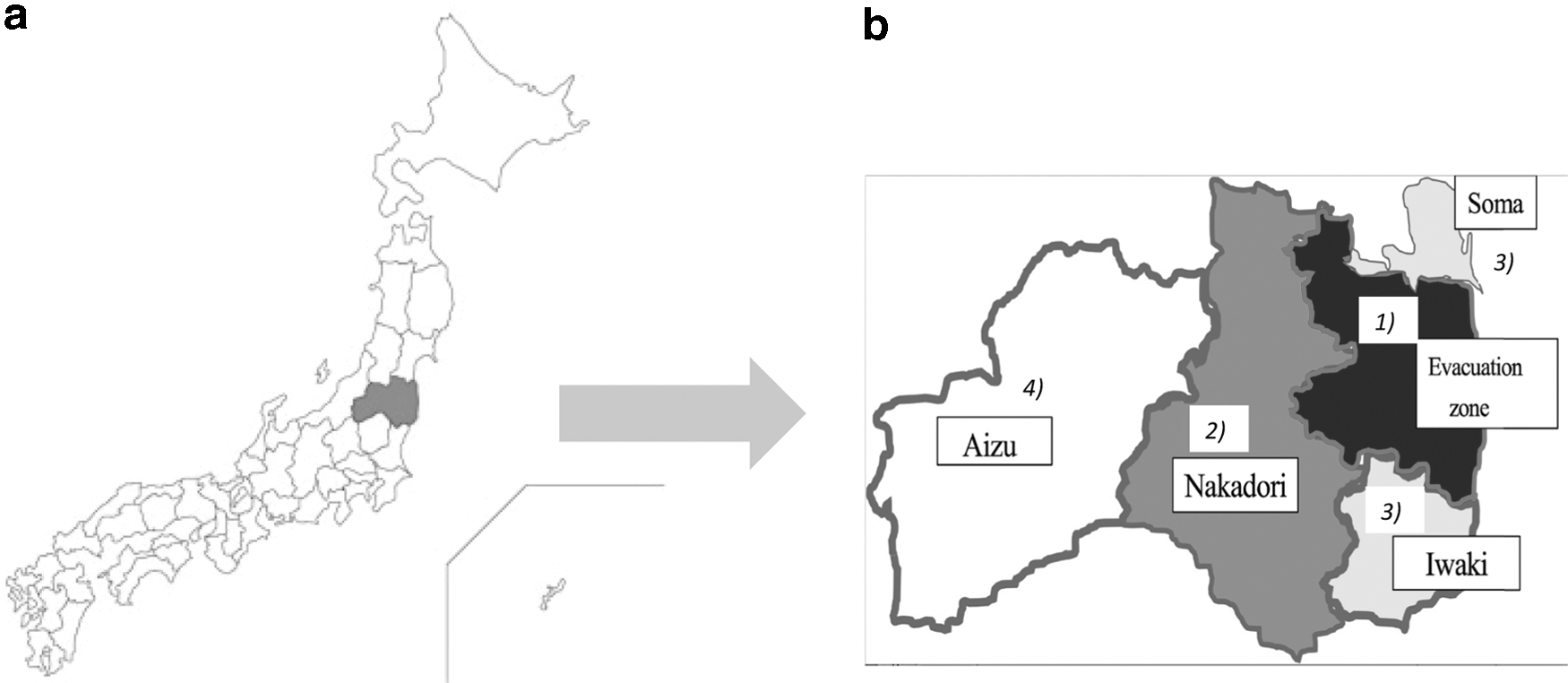
The present investigation was designed as a cohort study, in which screening was performed over the first four years as a baseline, with post-putative-latency surveys (Full-Scale Thyroid Screening) to continue every two years until participants reach 20 years of age, and every five years thereafter. To increase the number of opportunities to participate in the initial examination, these examinations were continued until notice of the Full-Scale Thyroid Screening program was sent to the residents. Primary baseline screening was completed as of June 30, 2015. Baseline screening began in 13 evacuation zone municipalities, from which 10–100% of residents were evacuated, followed by Nakadori (central Fukushima), Iwaki and Soma (on the Pacific coast below and above the evacuation zone, respectively), and finally Aizu (inland), as shown in Figure 1.
(
Screening population
Japan's civil registry system identified 367,686 people aged 18 years or younger as of April 1, 2011, living in Fukushima Prefecture at the time of the accident.
Thyroid ultrasonography screening program
Physicians and technicians credentialed by the Japan Thyroid Association, Japanese Society of Thyroid Surgery (JSTS), Japan Society of Ultrasonics in Medicine (JSUM), Japanese Society for Paediatric Endocrinology, Japanese Society of Sonographers, or Japan Association of Breast and Thyroid Sonology (JABTS) performed screening using advanced instrumentation (9 –11). Thyroid volume, nodules, cysts, echogenicity, and other findings, such as diffuse goiter, swelling of lymph nodes or parathyroid glands, congenital defects, ectopic thymus, and ultimobranchial bodies, were recorded. In cases with cysts, multifocality, location, and the greatest dimension were also documented. For nodules, quantity (single or multiple), location of the largest nodule, and its greatest dimension were assessed. Questionable findings were referred to an expert panel.
Fine-needle aspiration cytology
In the absence of universal ultrasonography diagnostic guidelines for childhood thyroid cancer, criteria used for adult patients were adapted (9,10). According to the consensus of JABTS and JSUM, fine-needle aspiration cytology (FNAC) is recommended for nodules >5 mm in diameter if thyroid carcinoma is strongly suspected, those >10 mm in diameter if carcinoma is suspected, all nodules >20 mm in diameter, and all cystic lesions >20 mm in diameter. These guidelines were made to avoid unnecessary FNAC, especially for nodules between 5 and 10 mm.
Histologic diagnosis of thyroid specimens
Aspirated or resected specimens were diagnosed locally, most often at the Department of Pathology, Fukushima Medical University (FMU), and sent to an expert panel for confirmation.
Thyroid cancer treatment
Confirmed results were discussed in detail with patients and guardian(s), who could then elect surveillance or surgery. Surgery was performed mainly at FMU by JSTS-certified specialists. Cases were reviewed by a panel of thyroid experts preoperatively and postoperatively. Clinicopathologic data, such as tumor size, presence of extrathyroidal extension (ETE), and lymph node metastases, were retrieved from the relevant medical records at FMU and other participating medical facilities. ETE was defined as invasion of adjacent organs or skeletal muscle outside the isthmus (12). TNM stage was assessed according to the 7th edition of the tumor, node, and metastasis classification system proposed by the American Joint Committee on Cancer.
External radiation dose estimation
To establish the radiation doses of individuals, questionnaires about their location and activity from March 11 to July 11, 2011, were separately mailed to around 2.06 million inhabitants of all ages within the framework of the Fukushima Health Management Survey (basic survey). Responses were received from 553,418 people as of October 31, 2014. The four-month effective (external exposure) doses due to the accident for 531,691 inhabitants were estimated by superimposing their “record of movements and activities” on time-dependent gamma ray dose rate maps using software from the National Institute of Radiological Sciences (13,14). Although efforts have been made to estimate internal exposure due to radioiodine, individual estimates of internal dose are challenging due to limited information on dosimetric parameters for radioiodine. Control of the food chain was, however, more immediate and more effective than that of rural areas around Chernobyl. Thus, the four-month external doses were used to assess radiation exposure levels by region or group. Details regarding prophylactic potassium iodide intake after the accident were not available.
Thyroid cancer prevalence in Fukushima Prefecture
The prevalence of diagnosed or suspected thyroid cancer was estimated in four geographic areas: the evacuation zone (where the majority of subjects were evacuated, and where 1.1% were exposed to ≥5 mSv), Nakadori (central Fukushima, the most densely populated area, where 0.007% had such exposure), Iwaki and Soma (coastal regions not evacuated, where 0.004% had such exposure), and Aizu (inland Fukushima, where 0% had such exposure).
Statistical analysis
A logistic regression model adjusted for age and sex was applied to compare thyroid cancer prevalence of different areas (the evacuation zone, Nakadori, and Iwaki and Soma) with that of Aizu as the reference. Calculations excluding patients with a possible genetic predisposition (n = 4), and those with a history of whole-body irradiation including the neck (n = 1) from the regression were also done. All statistical tests were two-tailed, with a p-value of <0.05 being considered statistically significant. SAS v9.3 (SAS Institute, Cary, NC) was used for the analysis.
Study ethics
This study received approval (#1318) from the FMU Ethics Committee, which is guided by local policy, national law, and the World Medical Association Declaration of Helsinki. Informed consent was obtained from parents or guardians, and documented in writing. Methods used were carried out in accordance with the approved guidelines.
Results
Thyroid ultrasound examination
Primary screening was performed on 300,476 (81.7%) of 367,685 eligible children and adolescents between October 2011 and June 2015. From 300,476 completed results, there were 2275 (0.8%) with nodule(s) >5 mm and 1715 with nodule(s) ≤5 mm; 12 had cyst(s) measuring >20 mm and 143,901 (47.9%) had cysts ≤20.0 mm. The 2294 cases with nodules >5 mm and/or cysts >20.0 mm were recommended to undergo secondary screening (confirmatory examinations). Investigations of 2108 (91.9%) of these cases included 537 (39.6%) with cytological assessment, 700 (34.0%) with lesions found to be smaller in size than in the threshold criteria, and 1356 (66.0%) were recommended to undergo re-evaluation after six months to a year in the absence of clear indications for a biopsy (Fig. 2).
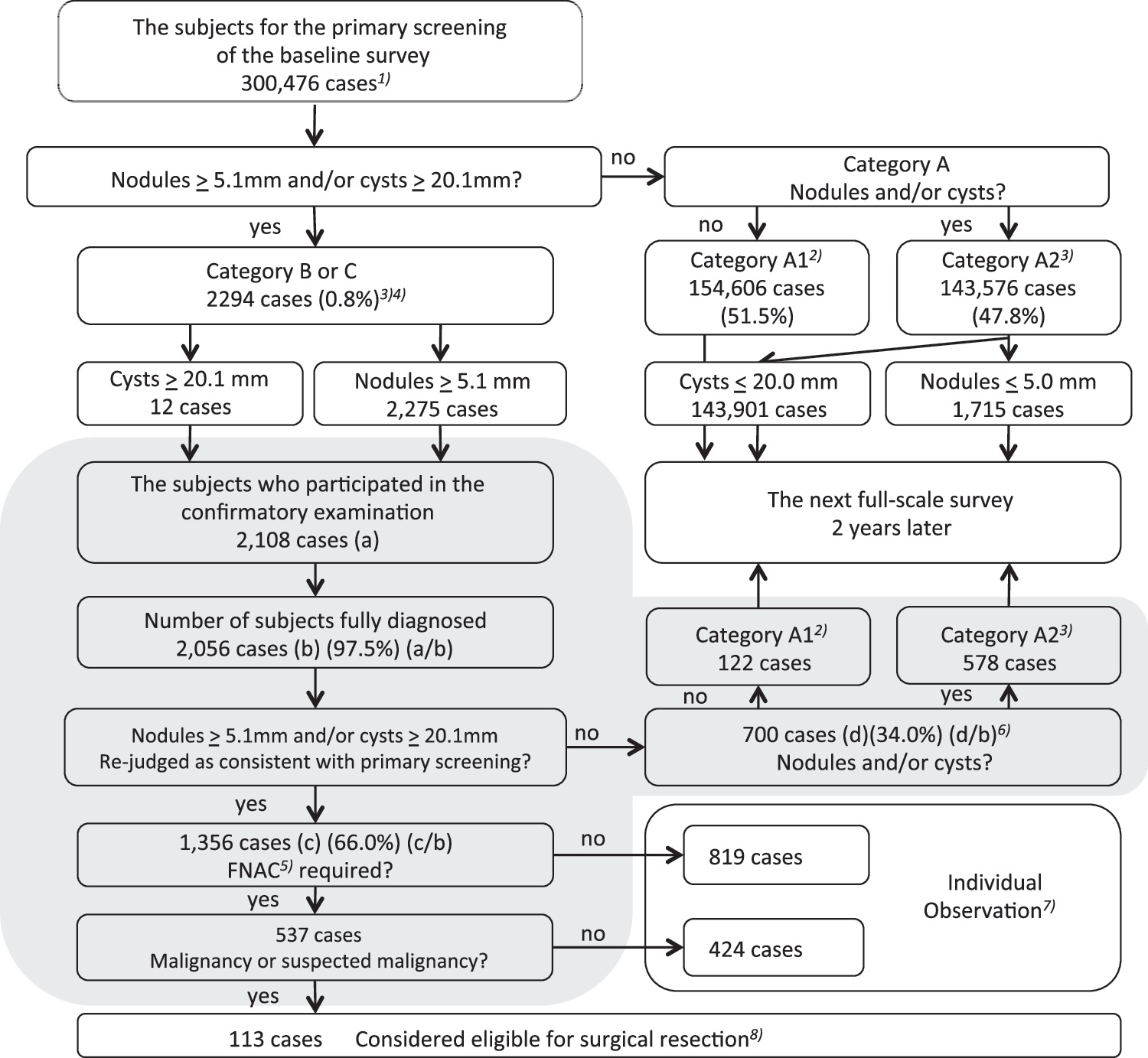
Flow chart of primary screening in the baseline survey from October 9, 2011, to June 30, 2015. Gray area denotes the confirmatory survey.
FNAC
Of the 537 patients referred for FNAC, surgery was not indicated for 424 because of the lack of evidence of any malignancy. The cytological diagnoses of the 424 cases were “nondiagnostic,” “benign,” “atypia of undetermined significance,” “follicular lesion of undetermined significance,” “follicular neoplasm,” and so on, based on the Bethesda System for Reporting Thyroid Cytopathology (15). The other 113 cases (38 male) were diagnosed as, or strongly suspected to be, thyroid carcinoma as per expert consensus. The age of these carcinoma patients ranged from 6 to 18 years at the time of the accident (Fig. 3). No carcinoma was observed among children younger than six years of age at the time of the accident.
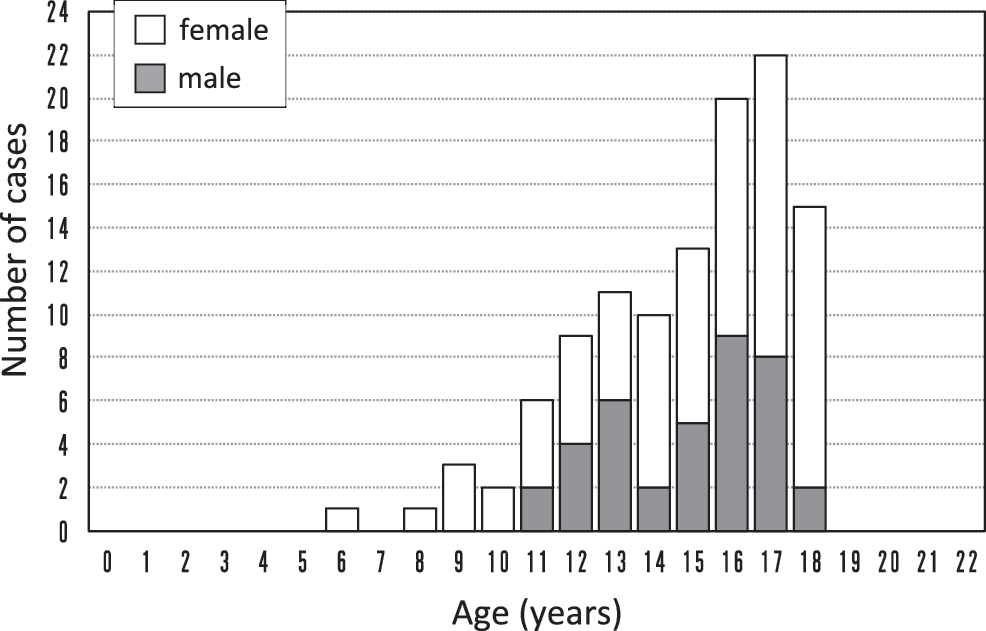
Age distribution of patients diagnosed with or suspected for thyroid carcinoma (n = 113; 38 males) at the time of the accident. No patients younger than six years of age had lesions, whereas more adolescents did, with a peak at 17 years of age (n = 22).
Surgery
Of the 113 patients diagnosed with or suspected of having cancer, 99 patients had undergone surgery at FMU or other hospitals as of June 30, 2015. Pathological examination revealed 95 cases of papillary thyroid carcinoma (PTC), three poorly differentiated thyroid carcinomas, and one histologically benign lesion. Among the 94 operated patients with cancer, a total 54 cases as of November 11, 2014, have been reported to a public committee subgroup that is tasked with overseeing the thyroid examination program. At FMU, 54 patients (23 male) aged between 6 and 18 years (M ± standard deviation [SD] = 14.8 ± 2.7) at the time of the accident, and between 9 and 21 years (M ± SD = 17.4 ± 2.8) at diagnosis had undergone surgery as of December 2014. Regarding their descriptive characteristics, the mean tumor size was 14.5 mm (range 5–53 mm), 59% had T1 lesions, 37% had positive ETE, 74% were found to have lymph node metastasis, and all cases except two (poorly differentiated thyroid carcinomas) were histologically classical PTC. There were no solid variant PTCs. Notably, two cases (4%) had distant metastases in the lung.
Thyroid cancer prevalence and external radiation exposure dose in Fukushima Prefecture
Based on the above results, the overall prevalence of children and adolescent thyroid cancer was calculated as 37.3/100,000 in Fukushima (Table 1). When the region of Fukushima Prefecture was divided into four areas according to the estimated fallout, no significant differences in thyroid cancer prevalence were found between the evacuation zone (33.5/100,000), Iwaki and Soma (43.0/100,000), Nakadori (37.2/100,000), and the reference area of Aizu (32.6/100,000), which had the lowest radiation levels. Compared with Aizu, the age- and sex-adjusted odds ratios of thyroid cancer for the evacuation zone, Iwaki and Soma, and Nakadori areas were 1.223 [confidence interval (CI) 0.554–2.699], 1.189 [CI 0.582–2.429], and 1.212 [CI 0.638–2.300], respectively. Girls had a higher prevalence of thyroid cancer than boys, and the adjusted odds ratio was 1.871 ([CI 1.261–2.775]; p < 0.01). In addition, the four-month cumulative external radiation dose was estimated for 63 confirmed or suspected cancer patients who provided their location and behavior details to the Fukushima Health Management Survey. A total of 45 (71.4%) of those patients were exposed to <1.0 mSv, and none were exposed to >2.2 mSv (Fig. 4). No higher cumulative dose was observed among the patients compared to young and adolescent residents analyzed separately (14).

Distribution of the estimated four-month (March 11 to July 11, 2011) cumulative effective dose in children and adolescents from 0 to 18 years of age at the time of the accident. The numbers in parentheses indicate those with records of residence/action for less than four months. Of the 63 patients diagnosed with or suspected for carcinoma, 45 (71.4%), including five whose record of residence/action did not extend to four months, were exposed to a cumulative effective dose of <1 mSv.
The baseline survey for thyroid screening was performed in two and half years from October 2011 to March 2014 in four different areas as follows: October 2011 to March 2012 in the evacuation area, April 2012 to March 2013 in 83% of Nakadori and April 2013 to March 2014 in the remaining 17% of Nakadori, and April 2013 to June 2014 in Iwaki and Soma, and Aizu.
External radiation doses (effective dose) individually estimated for respondents to the Basic Survey. Background (natural) radiation dose was subtracted in the estimation (14).
Number of diagnosed or suspected cancer cases by fine-needle aspiration cytology/number of children screened × 100,000.
Excluding one patient with benign tumor confirmed after surgery.
Discussion
The present study found a high overall thyroid cancer prevalence of 37.3/100,000 (0.037%), along with a high prevalence of cysts (47.8%) and nodules (1.4%) in children and adolescents. This clearly exceeds the thyroid cancer rates in young populations reported elsewhere. However, direct comparisons with other results, including those of cancer registries, cannot be made because of methodological differences and the absence of a rigorously defined control group outside Fukushima with any excess radiation exposure.
On the other hand, an independent study implemented the same screening protocol in three other Japanese prefectures (Aomori to the North, Yamanashi in central Japan, and Nagasaki to the West). Among 4365 children aged 3–18 years, cysts, nodules, and carcinomas were found in 56.9%, 1.7%, and 0.02% (n = 1), respectively (16), and such proportions were not statistically different from those in Fukushima. Considering that not all positive examinees in these prefectures accepted confirmatory testing, their actual prevalence of thyroid pathologies might be higher. Nevertheless, baseline results of mass screening in Fukushima have provoked concern and fear because a larger-than-expected number of cancers or suspicious lesions were detected (17). The Japan Public Health Centre-based Prospective Study (n = 52,679; age 40–69 years), with a mean follow-up of 14.5 years, identified 134 new thyroid cancer cases with an overall prevalence of 254.4/100,000, or 17.5/100,000 per year (18). They showed a positive association between seaweed consumption and the risk of thyroid cancer, especially for PTC in postmenopausal women. Further analyses did not indicate any association between seaweed intake and the risk of thyroid cancer after statistically adjusting for potential confounding variables, as well as on stratification by menopausal status (19). This remains to be further clarified, and it is worth noting that other risk factors besides radiation exposure could influence the prevalence of thyroid cancer in Fukushima.
Although a high thyroid cancer prevalence was revealed in Fukushima Prefecture for the first time within the putative latent period for radiation-related cancers, the relationship between such a high prevalence of thyroid cancer and exposure of radioiodine and other fallout caused by the nuclear plant accident is thought to be very unlikely for the following reasons.
First, there is a striking discrepancy in age distribution of cancer patients in Fukushima within the first three years following the accident versus similar data in the Ukraine after a latency period, where those younger than five years of age had the highest risk for thyroid cancer (20). Post-Chernobyl thyroid carcinomas were diagnosed in patients younger than 15 years of age. In contrast, the incidence of thyroid cancers post-Chernobyl in Italy and France increased with age, and most (57%) were diagnosed after the age of 14 years (21). The Italian and French data are consistent with the present study results, where half of the cancer cases were diagnosed in adolescents older than 15 years of age.
Second, the present study is the largest survey of baseline thyroid pathology for children with few or no symptoms. Concerning the thyroid equivalent dose received by children in Fukushima, especially those from the evacuation zones, available information on internal exposure due to 131I is limited. However, according to direct measurements of 131I activity in the thyroids of 62 evacuees from heavily contaminated areas such as Namie Town, the median thyroid equivalent dose due to internal exposure was 4.2 mSv for children (maximum 23 mSv) and 3.5 mSv for adults (maximum 33 mSv) (22). These doses were much smaller than those of the Chernobyl evacuees.
Third, concerning the relationship between the prevalence of thyroid cancer and regional differences within Fukushima Prefecture, the Aizu area (32.6/100,000), with minimal radiation exposure and no residents receiving >5 mSv during the first four months, was used as the reference. There were no significant differences between the evacuation zone (33.5/100,000) and the other two areas, Iwaki and Soma (43.0/100,000) and Nakadori (37.2/100,000).
Fourth, the distribution of individual estimated doses among patients is similar to that of young residents overall (i.e., all those <19 years old at the time of the accident), for example <1 mSv, 62.2% versus 71.4%; 1–2 mSv, 27.0% versus 30.2%; 2–5 mSv, 1.6% versus 7.5%; and >5 mSv, 0% versus 0.04% (13). Thus, we do not anticipate any future increase of thyroid cancer risk because the reference dose of radiation at which thyroid cancer risk is thought to increase is >100 mSv from the standpoint of known dose–response relationships (23 –28).
In addition to the above reasons, a higher dose of dietary iodine intake contributes to lower radioiodine uptake in the thyroid. It is well-known that iodine deficiency in conjunction with radiation exposure increases the risk of thyroid carcinoma (1). Although information regarding dietary iodine in Ukraine and Belarus during the 1980s is unclear, the prevalence of small goiters among children suggested iodine deficiency, and urinary iodine measurements from 1990 support this conjecture (29). Characterization of childhood thyroid carcinomas in areas of Belarus, Ukraine, and the Russian Federation affected by the Chernobyl accident, compared with that of England, Wales, and pre-FDNPP accident Japan, suggests that dietary iodine is a significant modulator of radiation-induced thyroid carcinogenesis, such that iodine deficiency could increase incidence, reduce latency, and influence tumor morphology and aggressiveness (30). In contrast, although data concerning iodine intake in Fukushima Prefecture were not available, it is reported that iodine intake (mainly from seaweed) in Japan is 1–3 mg/day, or 10–31 times that of Americans (31), suggesting a lower possibility of increased risk of radioactive iodine uptake into thyroid glands.
Gupta et al. reported that after 300 children were referred for evaluation of suspected nodules, a total of 125 children met the criteria for FNAC at a medical institute in the United States, where 28 children were diagnosed with thyroid cancer—a rate of 22% (32). In Fukushima, 113/537 cases with FNAC were diagnosed as having malignant lesions, and the rate of cancer was 21.0%, indicating that the discovery rate of thyroid cancers from nodules by FNAC in children is comparable.
The high prevalence of childhood and adolescent thyroid cancers detected in Fukushima can therefore be attributed to mass screening effects, even though we have implemented a relatively conservative diagnostic protocol of ultrasound examination to avoid overdiagnosis (9 –11). Thyroid cancer diagnoses have been increasing worldwide for the last three decades, especially in Korea, where it is the leading cancer among women, accounting for 30.1% of total cancer cases in 2010. The age-standardized incidence for thyroid cancer in women was 88.6/100,000 in 2012, four times greater than that of the United States and 13 times that of Japan (31). In the period 1992–1995, half of the overall increase in PTC came from very small (< 10 mm) lesions. This rise in microcarcinomas detected by ultrasonography may also be attributed to screening effects; as a larger population is screened, a greater apparent incidence of thyroid cancer is observed (33). There has been a levelheaded debate concerning the gap between the rapidly rising numbers of PTC diagnoses and the stable cancer-related death rate of 0.5/100,000 Americans between 1979 and 2009 (34).
Taking into consideration the critical debate on adult thyroid cancer screening, treatments should be carefully evaluated for children and adolescents (32) because their prognosis is better than that of adults, even with a higher frequency of extrathyroidal spread and higher recurrence rates (8). Davies et al. reported that small thyroid carcinomas (49% <1 cm; 87% <2 cm) increased in the United States between 1988 and 2002 (35). In the present study, the majority had small tumors, with 59% T1 cases (28% <1 cm, 59% <2 cm). Although 37% had ETE and 74% were node positive in this series, the frequencies of lymph node metastasis and ETE of the current cases were the same as those in other reports (36,37). In addition, the finding of pulmonary metastasis observed around Chernobyl and in the present cases in Fukushima is lower than that of a previous Japanese pediatric thyroid cancer study, which was reported before the introduction of thyroid ultrasound screening (36). Taken together, the subjects underwent surgery at early rather than advanced stages because of the accurate diagnosis by FNAC together with the uniform diagnostic criteria of sophisticated ultrasound screening. The potential for overdiagnosis of thyroid lesions should be carefully examined in the ongoing secondary evaluation and future surveys.
As all of the malignant cases were diagnosed as PTC or suspected PTC in the present study, cases with follicular thyroid cancer (FTC) should be potentially found with regard to the high discovery rate of malignancy. It is difficult to make a diagnosis of FTC in the early stage of screening because it is not possible based on cytology. In these cases, the nodules will be followed up as a follicular thyroid tumor, and FTC may be found after longitudinal follow-up. For this reason, the patients with a follicular tumor are being carefully followed. One patient among the cases with malignancy or suspected malignancy had a suspected FTC based on the cytology results, but the postoperative pathological diagnosis was poorly differentiated thyroid cancer.
Finally, not only radioiodine-related but also sporadic childhood thyroid cancers are shown to be highly linked to a specific genetic rearrangement resulting in slow incremental changes after a latency period, followed by rapid growth after gene rearrangement on another chromosome (38). Although there is no specific signature gene of radiation-induced thyroid carcinogenesis, the genetic analysis of these patients using surgically resected samples clearly demonstrated different oncogenic profiles from Chernobyl, suggesting non-radiogenic etiology of these cancers (39).
In conclusion, considering that there was a substantial rise in childhood thyroid cancer incidence observed at around four to five years after exposure around Chernobyl, this current large-scale survey was undertaken covering the first four years in Fukushima to establish a baseline prevalence of childhood and adolescent thyroid cancers, which serves as the reference for subsequent investigations related to the FDNPP accident. It must be emphasized that the rather high cancer prevalence observed among older children and adolescents is probably a consequence of mass screening with advanced ultrasonography. However, the second- and third-round surveys should be continued and analyzed carefully and then be compared to the baseline data. Future cumulative data are expected to clarify the natural history and risk factors of childhood and adolescent thyroid cancers, and also the risk–benefit relationship of thyroid ultrasound screening itself in Fukushima Prefecture.
Footnotes
Acknowledgments
We express our gratitude to all members participating in the Fukushima Health Management Survey. We also wish to thank Tazuko Kawasaki and Takako Takahashi for their excellent secretary assistance. In addition, we thank the many physicians, medical technologists, and other professionals from Fukushima and throughout Japan for their dedicated efforts. We are deeply indebted to Professor Emeritus Teizo Fujita for his critical review of the manuscript.
The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of Fukushima Prefectural Government.
This survey was conducted as part of Fukushima Prefecture's post-disaster recovery plans and was supported by the national “Health Fund for Children and Adults Affected by the Nuclear Incident.”
Participating other expert committee members, advisors, and staff in the Fukushima Health Management Survey: Kumiko Tsuboi, Shiro Matsui, Seisho Tanaka, Masaharu Maeda, Shigeatsu Hashimoto, Keiya Fujimori, Suguru Ishida, Yuko Hino, Hiroshi Mizunuma, Keiichi Nakano, Hirokazu Okayama, Chiyo Ohkouchi, Tomomi Hakoiwa, Chisato Takahashi, Yukari Sato, Ayako Sato, Nobuko Sakuma, Toshie Sakagami, Manabu Ohishi, Norikazu Abe, Masao Kuribara, Masahiko Henmi, Takao Yamahata, Mizuki Sekino, and Yuko Sato.
Author Disclosure Statement
The authors have nothing to disclose. There is no conflict of interest in this study.